An Italian Network of Population-Based Birth Cohorts to Evaluate Social and Environmental Risk Factors on Pregnancy Outcomes: The LEAP Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cohorts
2.2. Socioeconomic, Demographic and Obstetric Characteristics
2.3. Air Pollution Exposure Assessment
2.3.1. Standard Models
2.3.2. Back-Extrapolated Models
- We calculated the “annual” average concentration for the background monitoring sites during the measurement period used to build standard models (MLUR).
- For each day from 2007–2013, we calculated the ratio between the daily concentration (DC) and the annual average covering the LUR-models measurement period: Ratio = DC/MLUR.
- For each day, we calculated the extrapolated concentration by multiplying the modelled LUR concentration attributed to each subject (CLEAP) with the Ratio: C extrapolated = CLEAP × Ratio.
- We calculated both an average exposure during pregnancy, using extrapolated temporally adjusted exposures, and trimester specific exposures.
- In order to account for the nine months of pregnancy, we attributed these back-extrapolated exposures only to births occurred from 2008 to 2013.
2.3.3. Additional Exposure Models
3. Results
3.1. Cohorts’ Selection and Description
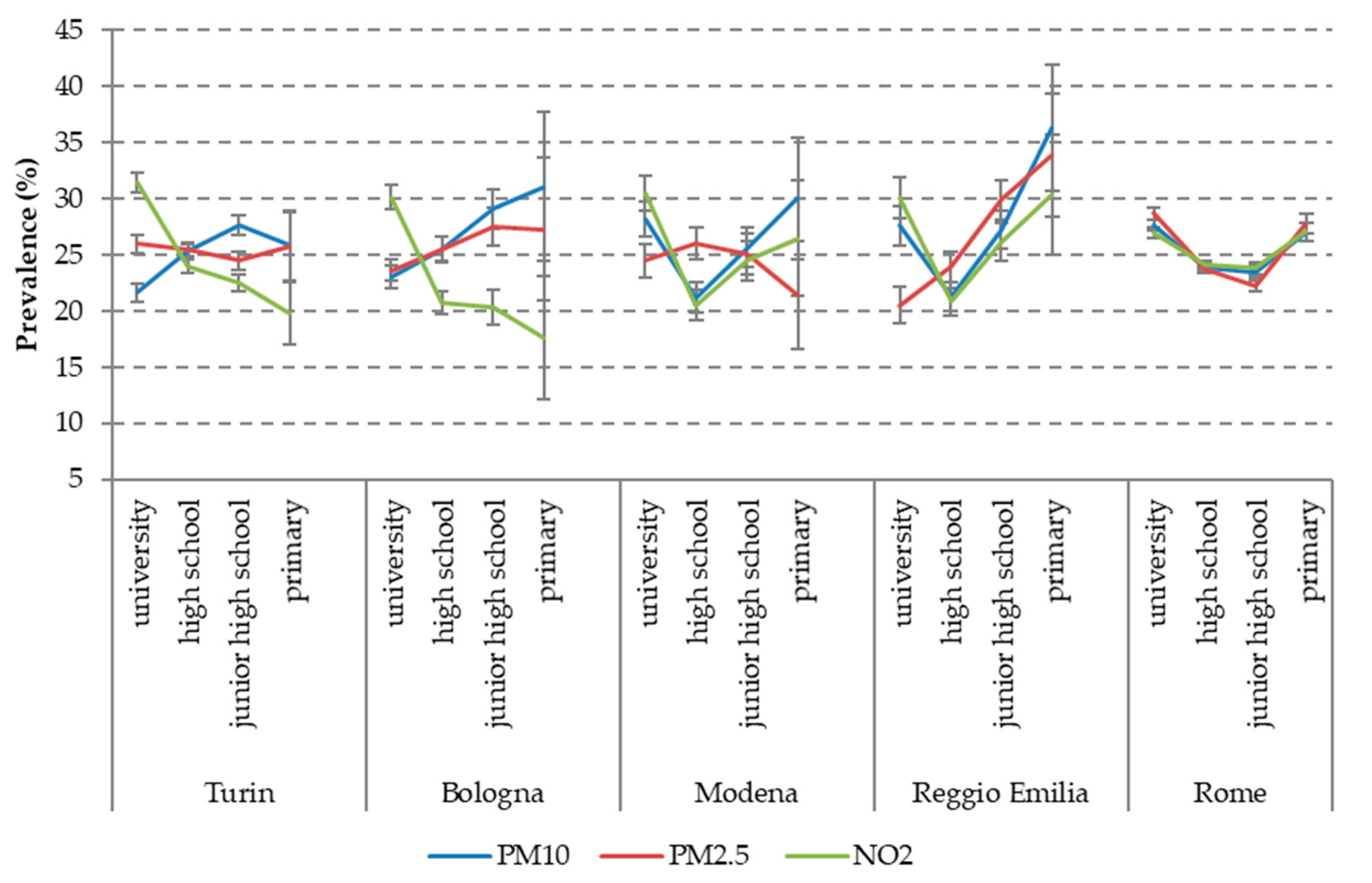
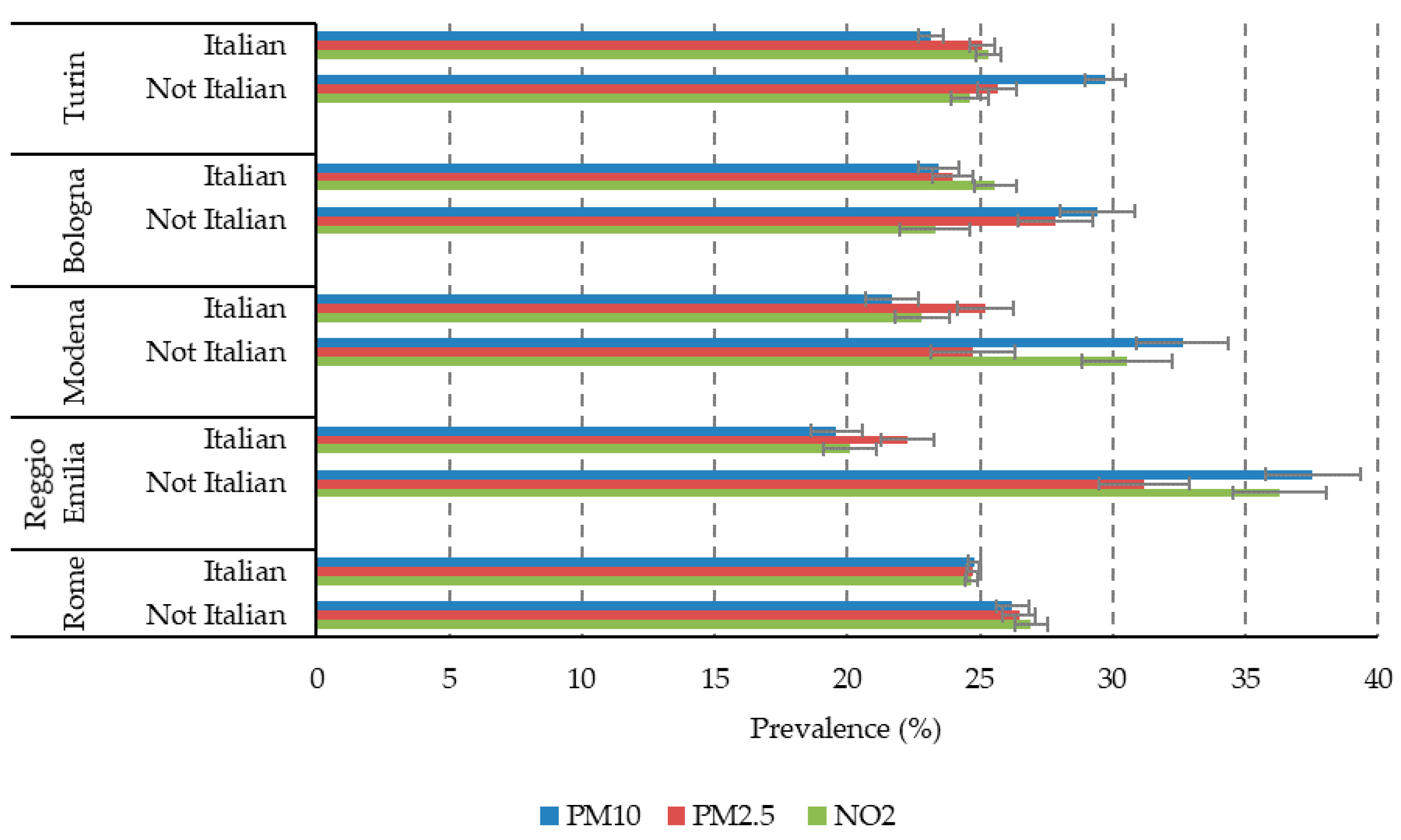
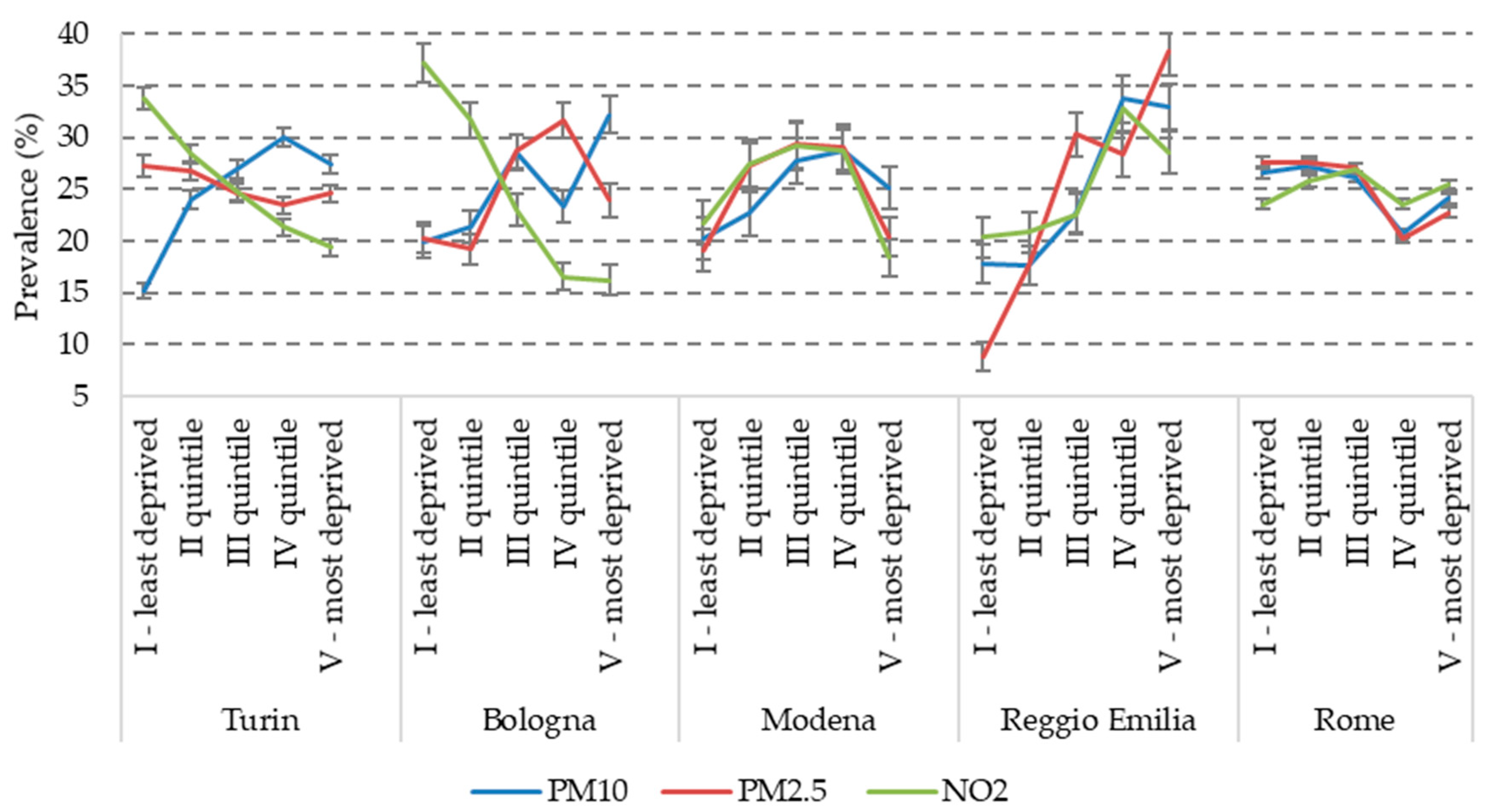
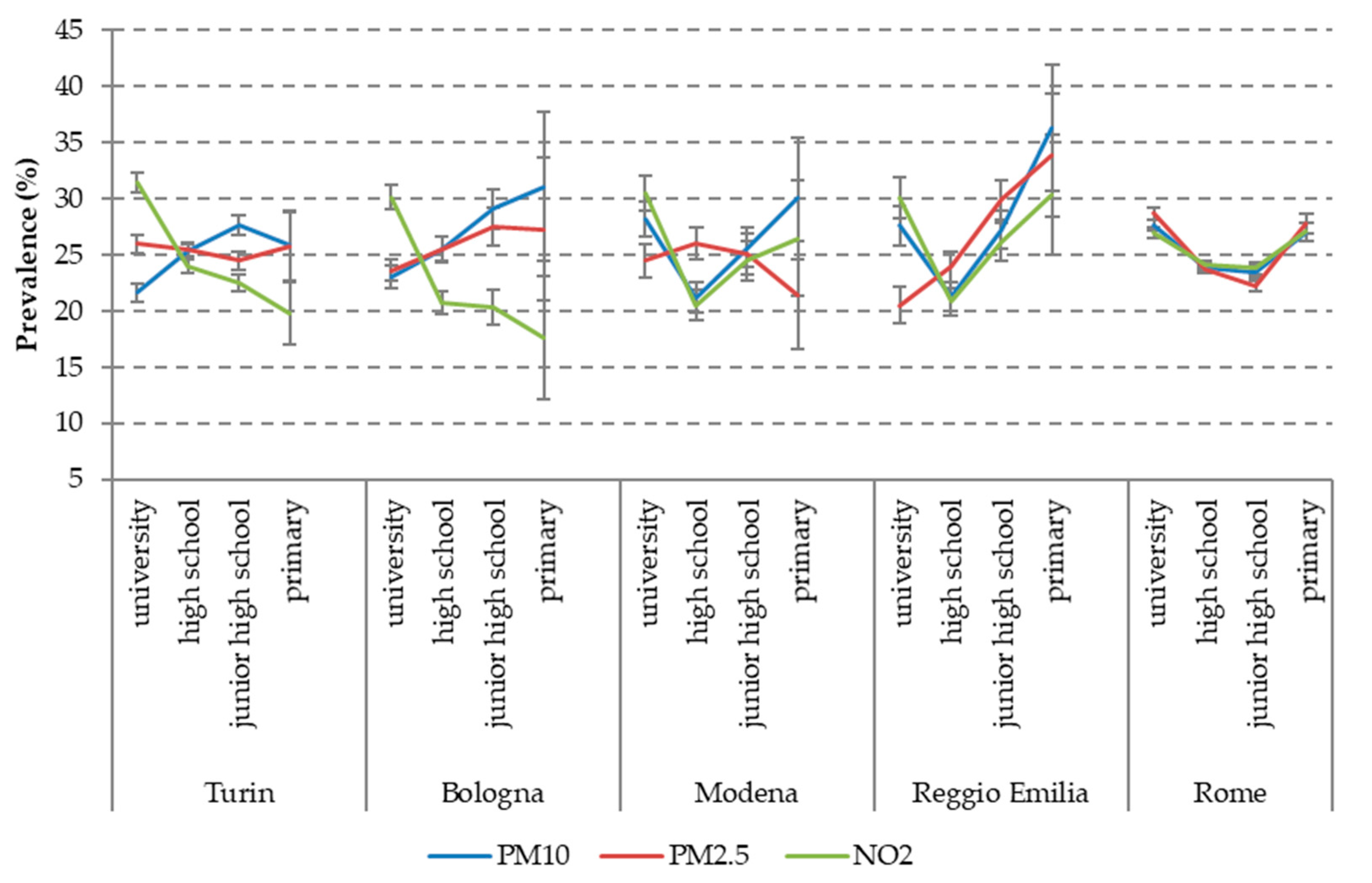
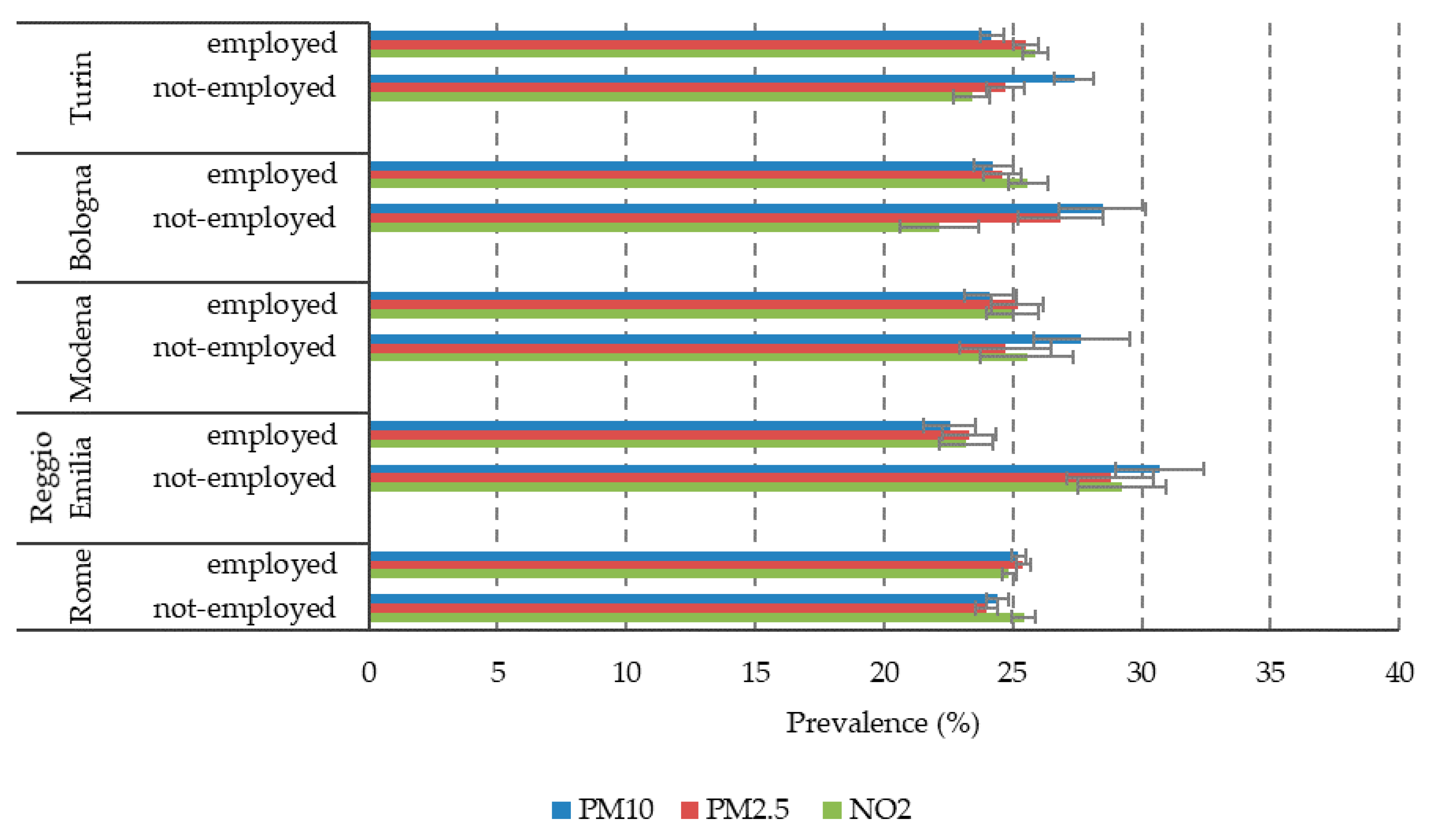
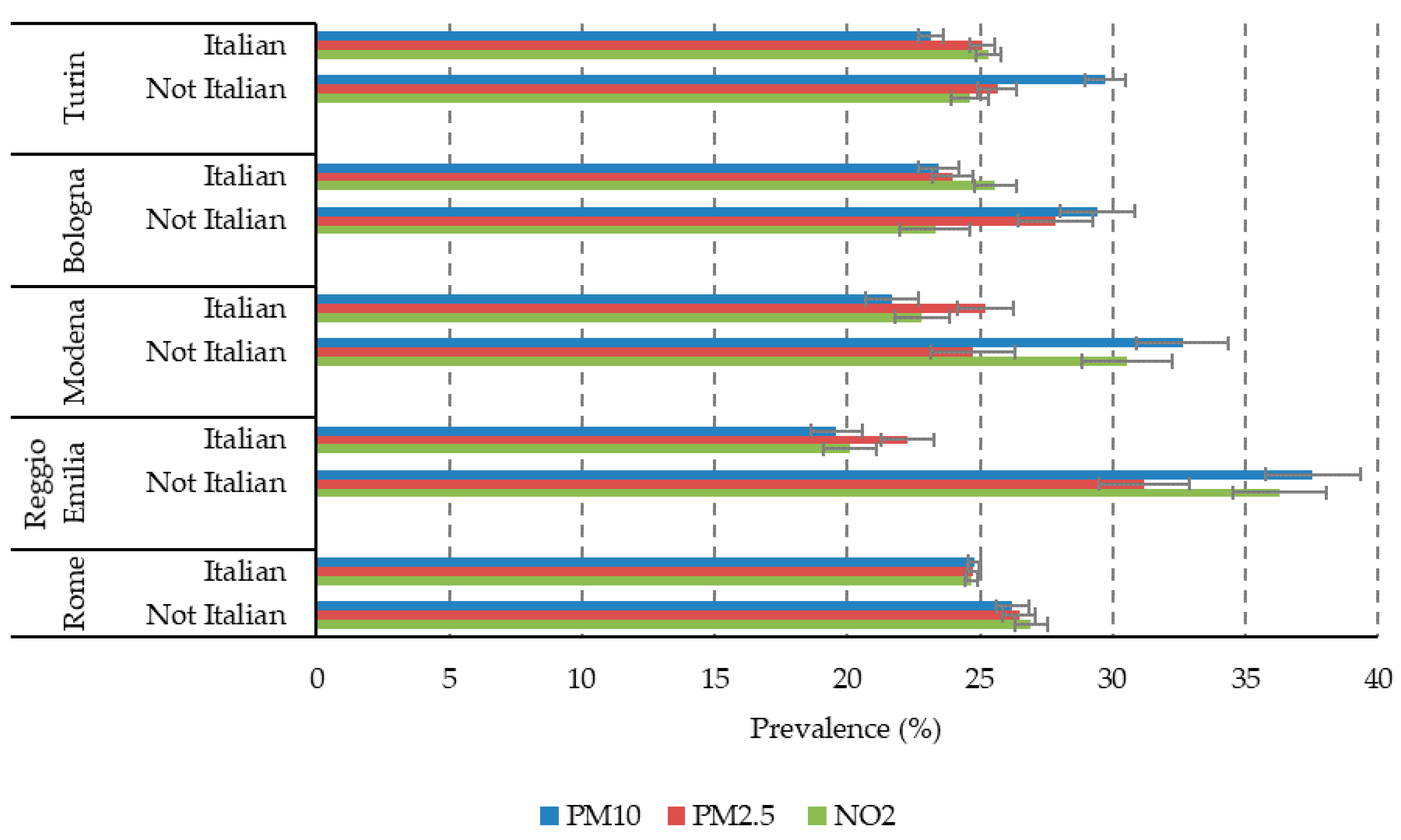
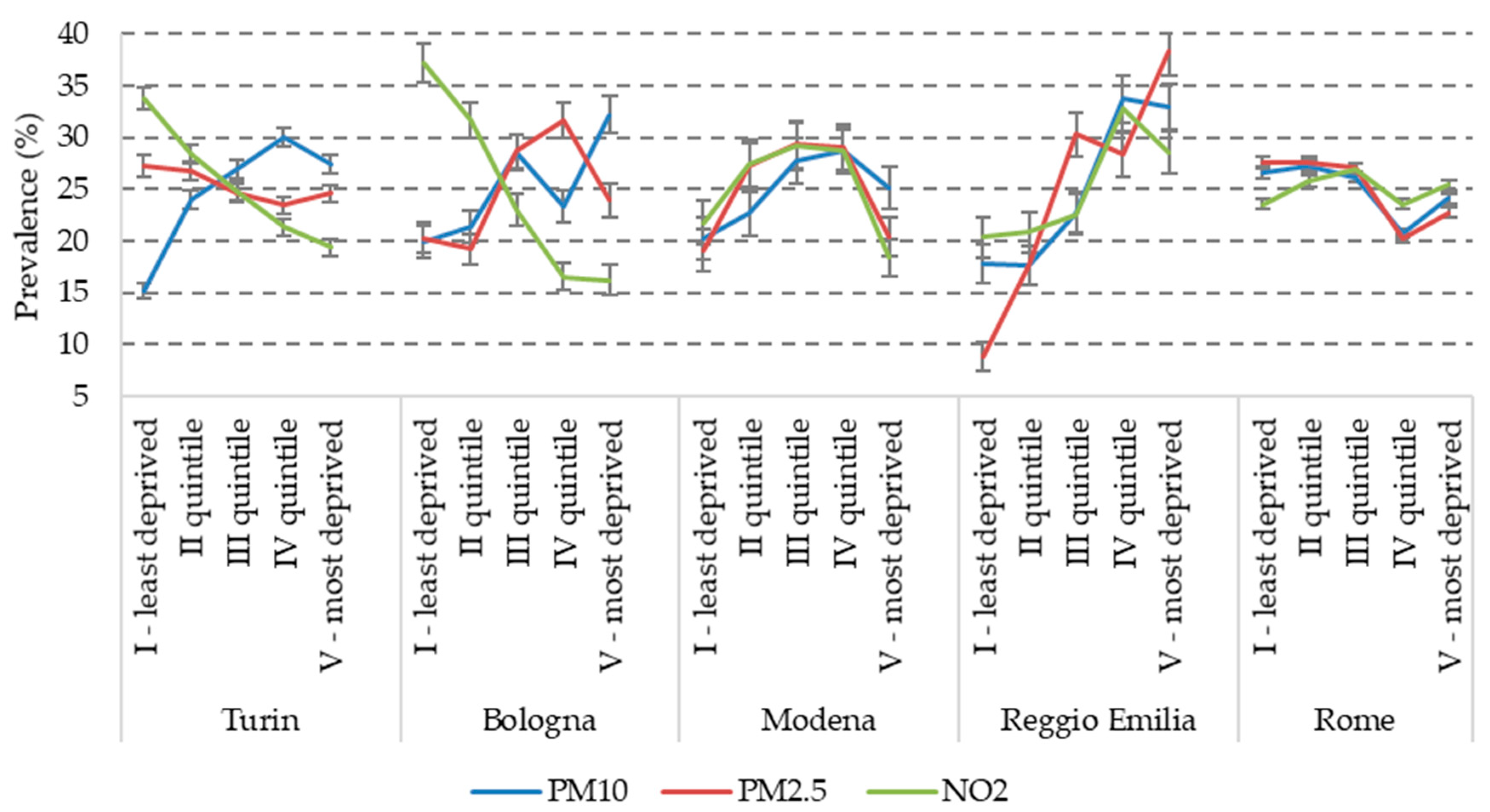
3.2. Air Pollution Exposure
3.3. Outcomes
3.4. Interactions between Determinants
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kramer, M.S.; Séguin, L.; Lydon, J.; Goulet, L. Socio-economic disparities in pregnancy outcomes: Why do the poor fare so poorly? Paediatr. Perinat. Epidemiol. 2000, 14, 194–210. [Google Scholar] [CrossRef] [PubMed]
- Blumenshine, P.; Egerter, S.; Barclay, C.J.; Cubbin, C.; Braveman, P.A. Socioeconomic disparities in adverse birth outcomes: A systematic review. Am. J. Prev. Med. 2010, 39, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, A.; Lail, P.; Ghali, W.A.; Sauve, R.S. The association between neighbourhoods and adverser birth outcomes: A systematic review and meta-analysis of multi-level studies. Paediatr. Perinat. Epidemiol. 2011, 25, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.S. Socioeconomic disparities in preterm births. Paediatr. Perinat. Epidemiol. 2015, 29, 169–171. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, G.; Strandberg-Larsen, K.; Mortensen, L.; Barros, H.; Cordier, S.; Correia, S.; Danileviciute, A.; van Eijsden, M.; Fernández-Somoano, A.; Gehring, U.; et al. Exploring educational disparities in risk of preterm delivery: A comparative study of 12 European birth cohorts. Paediatr. Perinat. Epidemiol. 2015, 29, 172–183. [Google Scholar] [CrossRef]
- Ruckerl, R.; Schneider, A.; Breitner, S.; Cyrys, J.; Peters, A. Health effects of particulate air pollution: A review of epidemiological evidence. Inhal. Toxico. 2011, 23, 555–592. [Google Scholar] [CrossRef]
- Klepac, P.; Locatelli, I.; Korošec, S.; Künzli, N.; Kukec, A. Ambient air pollution and pregnancy outcomes: A comprehensive review and identification of environmental public health challenges. Environ. Res. 2018, 167, 144–159. [Google Scholar] [CrossRef]
- Erickson, A.C.; Ostry, A.; Chan, H.M.; Arbour, L. Air pollution, neighbourhood and maternal-level factors modify the effect of smoking on birth weight: A multilevel analysis in British Columbia, Canada. BMC Public Health. 2016, 16, 585–596. [Google Scholar] [CrossRef] [Green Version]
- Shah, P.S.; Balkhair, T. Knowledge Synthesis Group on Determinants of Preterm/LBW births. Air pollution and birth outcomes: A systematic review. Environ. Int. 2010, 37, 498–516. [Google Scholar] [CrossRef]
- Stieb, D.M.; Chen, L.; Eshoul, M.; Judek, S. Ambient air pollution, birth weight and preterm birth: A systematic review and meta-analysis. Environ. Res. 2012, 117, 100–111. [Google Scholar] [CrossRef]
- Caranci, N.; Di Girolamo, C.; Rossi, P.G.; Spadea, T.; Pacelli, B.; Broccoli, S.; Ballotari, P.; Costa, G.; Zengarini, N.; Agabiti, N.; et al. Cohort profile: The Italian Network of Longitudinal Metropolitan Studies (IN-LiMeS), a multicentre cohort for socioeconomic inequalities in health monitoring. BMJ Open 2018, 8, e020572. [Google Scholar] [CrossRef] [PubMed]
- Caranci, N.; Biggeri, A.; Grisotto, L.; Pacelli, B.; Spadea, T.; Costa, G. L’indice di deprivazione italiano a livello di sezione di censimento: Definizione, descrizione e associazione con la mortalità. [The Italian deprivation index at census block level: Definition, description and association with general mortality]. Epidemiol. Prev. 2010, 34, 167–176. [Google Scholar] [PubMed]
- Rosano, A.; Caranci, N.; Zengarini, N.; Pacelli, B.; Cislaghi, C.; Costa, G. La Misura della Deprivazione nelle Province Italiane Declinata al Femminile: Mortalità Evitabile e Deprivazione nelle donne Italiane. [The Measure of Deprivation in the Italian Provinces in a Female Perspective: Avoidable Mortality and Deprivation in Italian Women]. 2017. Available online: https://assr.regione.emilia-romagna.it/pubblicazioni/corsi-convegni/espanet2017-caranci/@@download/publicationFile/espanet2017_caranci.pdf (accessed on 26 March 2020).
- Bertino, E.; Spada, E.; Occhi, L.; Coscia, A.; Giuliani, F.; Gagliardi, L.; Gilli, G.; Bona, G.; Fabris, C.; De Curtis, M.; et al. Neonatal Anthropometric Charts: The Italian neonatal study compared with other European studies. JPGN 2010, 51, 353–361. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/20601901 (accessed on 20 May 2020). [CrossRef] [Green Version]
- Eeftens, M.; Beelen, R.; de Hoogh, K.; Bellander, T.; Cesaroni, G.; Cirach, M.; Declercq, C.; Dedele, A.; Dons, E.; de Nazelle, A.; et al. Development of land use regression models for pm2.5, pm2.5 absorbance, pm10 and pmcoarse in 20 european study areas; results of the ESCAPE project. Environ. Sci. Technol. 2012, 46, 11195–11205. [Google Scholar] [CrossRef] [PubMed]
- Beelen, R.; Hoek, G.; Vienneau, D.; Eeftens, M.; Dimakopoulou, K.; Pedeli, X.; Tsai, M.; Künzli, N.; Schikowski, T.; Marcon, A. Development of NO2 and NOx land use regression models for estimating air pollution exposure in 36 study areas in Europe—The ESCAPE project. Atmos. Environ. 2013, 72, 10–23. [Google Scholar] [CrossRef]
- Vienneau, D.; de Hoogh, K.; Bechle, M.J.; Beelen, R.; van Donkelaar, A.; Martin, R.V.; Millet, D.B.; Hoek, G.; Marshall, J.D. Western European land use regression incorporating satellite- and ground-based measurements of NO2 and PM10. Environ. Sci. Technol. 2013, 47, 13555–13564. [Google Scholar] [CrossRef]
- de Hoogh, K.; Gulliver, J.; van Donkelaar, A.; Martin, R.V.; Marshall, J.D.; Bechle, M.J.; Cesaroni, G.; Pradas, M.C.; Dedele, A.; Eeftens, M.; et al. Development of West-European PM(2.5) and NO(2) land use regression models incorporating satellite-derived and chemical transport modelling data. Environ. Res. 2016, 151, 1–10. [Google Scholar] [CrossRef] [Green Version]
- ESCAPE (European Study of Cohorts for Air Pollution Effects). Procedure for Extrapolation Back in Time, Version 25 January 2012; Available online: http://www.escapeproject.eu/manuals/Procedure_for_extrapolation_back_in_time.pdf (accessed on 16 March 2020).
- de Hoogh, K.; Wang, M.; Adam, M.; Badaloni, C.; Beelen, R.; Birk, M.; Cesaroni, G.; Cirachm, M.; Declercq, C.; Dėdelė, A.; et al. Development of land use regression models for particle composition in twenty study areas in Europe. Environ. Sci. Technol. 2013, 47, 5778–5786. [Google Scholar] [CrossRef]
- Nording, E.; Berglind, N.; Melén, E.; Emenius, G.; Hallberg, J.; Nyberg, F.; Pershagen, G.; Svartengren, M.; Wickman, M.; Bellander, T. Traffic-related air pollution and childhood respiratory symptoms, function and allergies. Epidemiology 2008, 19, 401–408. [Google Scholar] [CrossRef]
- Tanner, J.P.; Salemi, J.L.; Stuart, A.L.; Yu, H.; Jordan, M.M.; DuClos, C.; Cavicchia, P.; Correia, J.A.; Watkins, S.M.; Kirby, R.S. Uncertainty in maternal exposures to ambient PM2.5 and benzene during pregnancy: Sensitivity to exposure estimation decisions. Spat. Spatio-Temporal Epidemiol. 2016, 17, 117–129. [Google Scholar] [CrossRef]
- Doidge, J.C.; Harron, K.L. Reflections on modern methods: Linkage error bias. Int. J. Epidemiol. 2019, 48, 2050–2060. [Google Scholar] [CrossRef] [PubMed]
- Cesaroni, G.; Porta, D.; Badaloni, C.; Stafoggia, M.; Eeftens, M.; Meliefste, K.; Forastiere, F. Nitrogen dioxide levels estimated from land use regression models several years apart and association with mortality in a large cohort study. Environ. Health. 2012, 11, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eeftens, M.; Beelen, R.; Fischer, P.; Brunekreef, B.; Meliefste, K.; Hoek, G. Stability of measured and modelled spatial contrasts in NO2 over time. Occup. Environ. Med. 2011, 68, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Henderson, S.B.; Sbihi, H.; Allen, R.W.; Brauer, M. Temporal stability of land use regression models for traffic-related air pollution. Atmos. Environ. 2013, 64, 312–319. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Selection | Turin | Bologna | Modena | Reggio Emilia | Rome | Total |
|---|---|---|---|---|---|---|
| N singleton livebirths | 46,376 | 16,817 | 9502 | 10,188 | 144,614 | 227,497 |
| Exclusions | ||||||
| missing geocoding | 502 (1.1%) | 524 (.1%) | 16 (0.2%) | 704 (6.9%) | 6182 (4.3%) | 7928 (3.5%) |
| missing exposure | 195 (0.4%) | 157 (0.9%) | 14 (0.1%) | 140 (1.4%) | 3724 (2.6%) | 4230 (1.9%) |
| % success at linkage | 98.5 | 96.0 | 99.7 | 91.7 | 93.1 | 94.6 |
| malformations at birth | 803 (1.7%) | 145 (0.9%) | 46 (0.5%) | 90 (0.9%) | 2251 (1.6%) | 3335 (1.5%) |
| missing outcomes * | 32 (0.1%) | 110 (0.7%) | 5 (0.1%) | 2 (0.0%) | 2 (0.0%) | 151 (0.1%) |
| N births analysed | 44,844 | 15,881 | 9421 | 9252 | 132,455 | 211,853 |
| % of initial dataset | 96.7 | 94.4 | 99.1 | 90.8 | 91.6 | 93.1 |
| Year of delivery | ||||||
| 2007 | 6421 | 2129 | 1364 | 1341 | 19,124 | 30,379 |
| 2008 | 6626 | 2127 | 1340 | 1280 | 18,590 | 29,963 |
| 2009 | 6649 | 2255 | 1359 | 1384 | 18,457 | 30,104 |
| 2010 | 6449 | 2288 | 1326 | 1364 | 19,978 | 31,405 |
| 2011 | 6429 | 2350 | 1367 | 1373 | 19,383 | 30,902 |
| 2012 | 6313 | 2349 | 1390 | 1270 | 19,011 | 30,333 |
| 2013 | 5957 | 2383 | 1275 | 1240 | 17,912 | 28,767 |
| Characteristics | Turin | Bologna | Modena | Reggio Emilia | Rome | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (N = 44,844) | (N = 15,881) | (N = 9421) | (N = 9252) | (N = 132,455) | (N = 211,853) | |||||||
| Maternal age, years m (SD) | 32.3 (5.3) | 33.2 (5.2) | 32.5 (5.3) | 31.6 (5.4) | 33.3 (5.2) | 33.0 (5.2) | ||||||
| N | % | N | % | N | % | N | % | N | % | N | % | |
| Maternal education | ||||||||||||
| university | 9782 | 23.0 | 7404 | 46.6 | 3324 | 35.3 | 2422 | 26.2 | 34,133 | 25.8 | 57,065 | 27.3 |
| high school | 20,674 | 48.6 | 5741 | 36.1 | 3564 | 37.8 | 3976 | 43.0 | 63,501 | 48.0 | 97,456 | 46.5 |
| junior high school | 11,296 | 26.6 | 2549 | 16.1 | 2253 | 23.9 | 2570 | 27.8 | 24,188 | 18.3 | 42,856 | 20.5 |
| primary | 752 | 1.8 | 187 | 1.2 | 280 | 3.0 | 284 | 3.0 | 10,445 | 7.9 | 11,948 | 5.7 |
| Maternal occupational status | ||||||||||||
| employed | 30,501 | 69.1 | 12,775 | 80.7 | 7021 | 74.8 | 6326 | 68.4 | 92,764 | 70.1 | 149,387 | 70.8 |
| unemployed | 3471 | 7.9 | 497 | 3.1 | 310 | 3.3 | 429 | 4.6 | 12,884 | 9.7 | 17,591 | 8.3 |
| looking for the 1st job | 413 | 0.9 | 5 | 0.0 | 6 | 0.1 | 10 | 0.1 | 1393 | 1.1 | 1827 | 0.9 |
| student | 390 | 0.9 | 205 | 1.3 | 123 | 1.3 | 163 | 1.8 | 2124 | 1.6 | 3005 | 1.4 |
| housewife | 9163 | 20.7 | 2329 | 14.7 | 1919 | 20.4 | 2310 | 25.0 | 22,590 | 17.1 | 38,311 | 18.2 |
| other | 222 | 0.5 | 12 | 0.1 | 7 | 0.1 | 11 | 0.1 | 533 | 0.4 | 785 | 0.4 |
| Marital status | ||||||||||||
| married | 30,077 | 68.1 | 9913 | 63.4 | 6737 | 71.6 | 6589 | 71.4 | 86,773 | 65.5 | 140,089 | 66.4 |
| not married | 12,111 | 27.4 | 5534 | 35.4 | 2441 | 25.9 | 2448 | 26.5 | 42,194 | 31.9 | 64,728 | 30.7 |
| separated | 1185 | 2.7 | 90 | 0.6 | 135 | 1.4 | 107 | 1.1 | 2144 | 1.6 | 3661 | 1.7 |
| divorced | 689 | 1.6 | 69 | 0.4 | 88 | 0.9 | 81 | 0.9 | 1194 | 0.9 | 2121 | 1.0 |
| widowed | 70 | 0.2 | 21 | 0.1 | 9 | 0.1 | 6 | 0.1 | 149 | 0.1 | 255 | 0.1 |
| Citizenship | ||||||||||||
| Italian | 31,001 | 69.1 | 11,844 | 74.6 | 6603 | 70.1 | 6436 | 69.6 | 112,923 | 85.3 | 168,807 | 79.7 |
| foreigner | 13,843 | 30.9 | 4037 | 25.4 | 2818 | 29.9 | 2816 | 30.4 | 19,529 | 14.7 | 43,043 | 20.3 |
| Parity | ||||||||||||
| first child | 23,648 | 52.7 | 8788 | 55.3 | 4516 | 47.9 | 4307 | 46.6 | 74,063 | 55.9 | 115,322 | 54.4 |
| second child | 16,234 | 36.2 | 5517 | 34.7 | 3501 | 37.2 | 3674 | 39.7 | 45,979 | 34.7 | 74,905 | 35.4 |
| >2nd child | 4962 | 11.1 | 1576 | 9.9 | 1404 | 14.9 | 1271 | 13.7 | 12,413 | 9.4 | 21,626 | 10.2 |
| Type of delivery | ||||||||||||
| natural unassisted childbirth | 29,178 | 65.1 | 10,484 | 66.0 | 6551 | 69.5 | 6317 | 68.3 | 70,897 | 53.5 | 123,427 | 58.3 |
| caesarean section | 13,823 | 30.8 | 4708 | 29.6 | 2628 | 27.9 | 2559 | 27.7 | 56,976 | 43.0 | 80,694 | 38.1 |
| assisted childbirth | 1829 | 4.1 | 689 | 4.3 | 242 | 2.6 | 376 | 4.1 | 4458 | 3.4 | 7594 | 3.6 |
| other | 14 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 123 | 0.1 | 137 | 0.1 |
| Infant sex | ||||||||||||
| boys | 23,021 | 51.3 | 8214 | 51.7 | 4880 | 51.8 | 4764 | 51.5 | 68,207 | 51.5 | 109,086 | 51.5 |
| girls | 21,823 | 48.7 | 7667 | 48.3 | 4541 | 48.2 | 4488 | 48.5 | 64,248 | 48.5 | 102,767 | 48.5 |
| Pollutant | Turin | Bologna | Modena | Reggio Emilia | Rome |
|---|---|---|---|---|---|
| PM10 (µg/m3) | 46.7 (4.5) | 35.8 (2.3) | 38.7 (2.6) | 37.2 (3.0) | 36.3 (4.9) |
| PM2.5–10 (µg/m3) | 16.6 (3.0) | 16.4 (2.0) | 17.1 (2.3) | 15.6 (2.5) | 16.5 (3.3) |
| PM2.5 (µg/m3) | 26.3 (1.3) | 19.3 (0.7) | 21.6 (0.6) | 21.7 (0.8) | 19.4 (1.8) |
| NO2 (µg/m3) | 52.3 (9.1) | 39.7 (6.4) | 39.7 (7.3) | 33.9 (9.1) | 40.7 (10.7) |
| Outcomes | Turin | Bologna | Modena | Reggio Emilia | Rome | Total | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (N = 44,844) | (N = 15,881) | (N = 9421) | (N = 9252) | (N = 132,455) | (N = 211,853) | |||||||||||||
| Gestational age, weeks | ||||||||||||||||||
| m (SD) | 39.0 (1.8) | 39.0 (1.9) | 39.0 (1.8) | 39.0 (1.8) | 38.9 (1.7) | 38.9 (1.8) | ||||||||||||
| Birthweight in grams | ||||||||||||||||||
| m (SD) | 3256 (496) | 3288 (510) | 3307 (517) | 3322 (523) | 3252 (485) | 3261 (493) | ||||||||||||
| Length in cm | ||||||||||||||||||
| m (SD) | 49.4 (2.6) | 50.0 (2.6) | 50.1 (2.5) | 50.3 (2.8) | 50.0 (2.4) | 49.9 (2.5) | ||||||||||||
| Cranial circumference in cm | ||||||||||||||||||
| m (SD) | 34.0 (2.9) | 34.3 (1.8) | 34.2 (1.6) | 34.4 (2.3) | 34.3 (1.7) | 34.2 (2.1) | ||||||||||||
| Outcomes | N | % | (95% CI) | N | % | (95% CI) | N | % | (95% CI) | N | % | (95% CI) | N | % | (95% CI) | N | % | (95% CI) |
| Preterm birth | ||||||||||||||||||
| no | 41,994 | 93.6 | (93.4–93.9) | 14,879 | 93.7 | (93.3–94.1) | 8804 | 93.5 | (92.9–94.0) | 8655 | 93.5 | (93.0–94.1) | 124,834 | 94.2 | (94.1–94.4) | 199,166 | 94.0 | (93.9–94.1) |
| yes | 2850 | 6.4 | (5.5-7.3) | 1002 | 6.3 | (4.8-7.8) | 617 | 6.5 | (4.6-8.5) | 597 | 6.5 | (4.5-8.4) | 7621 | 5.8 | (5.2-6.3) | 12,687 | 6.0 | (5.9–6.4) |
| On term low birthweight | ||||||||||||||||||
| no | 40,961 | 97.5 | (97.4–97.7) | 14,595 | 98.1 | (97.9–98.3) | 8643 | 98.2 | (97.9–98.5) | 8469 | 97.9 | (97.5–98.2) | 122,067 | 97.8 | (97.7–97.9) | 194,705 | 97.8 | (97.7–97.8) |
| yes | 1033 | 2.5 | (1.5-3.4) | 284 | 1.9 | (0.3-3.5) | 161 | 1.8 | (0.0-3.9) | 186 | 2.1 | (0.1-4.2) | 2767 | 2.2 | (1.7–2.8) | 4431 | 2.2 | (1.8–2.7) |
| Weight for gestational age | ||||||||||||||||||
| appropriate | 36,183 | 80.7 | (80.3–81.1) | 12,862 | 81.0 | (80.3–81.7) | 7614 | 80.8 | (79.9–81.7) | 7429 | 80.3 | (79.4–81.2) | 108,540 | 81.9 | (81.7–82.2) | 172,628 | 81.5 | (81.3–81.7) |
| small | 4257 | 9.5 | (8.6–10.4) | 1237 | 7.8 | (6.3–9.3) | 698 | 7.4 | (5.5-9.4) | 680 | 7.3 | (5.4-9.3) | 11,246 | 8.5 | (8.0–9.0) | 18,118 | 8.6 | (8.1–9.0) |
| large | 4404 | 9.8 | (8.9–10.7) | 1782 | 11.2 | (9.8–12.7) | 1109 | 11.8 | (9.9-13.7) | 1143 | 12.4 | (10.4-14.3) | 12,669 | 9.6 | (9.1–10.1) | 21,107 | 10.0 | (9.6–10.4) |
| Apgar score | ||||||||||||||||||
| 7–10 (normal) | 43,663 | 99.3 | (99.3–99.4) | 15,766 | 99.5 | (99.4–99.6) | 9330 | 99.0 | (98.9–99.3) | 9204 | 99.5 | (99.3–99.6) | 129,724 | 99.6 | (99.6–99.6) | 207,687 | 99.5 | (99.5–99.5) |
| 4–6 (needs assistance) | 237 | 0.5 | (0.0-1.5) | 62 | 0.4 | (0.0–1.9) | 81 | 0.9 | (0.0–2.9) | 45 | 0.5 | (0.0–2.5) | 348 | 0.3 | (0.0–0.8) | 773 | 0.4 | (0.0–0.8) |
| 1–3 (needs resuscitation) | 56 | 0.1 | (0.0–1.1) | 14 | 0.1 | (0.0–1.6) | 8 | 0.1 | (0.0–2.1) | 3 | 0.0 | (0.0–2.1) | 167 | 0.1 | (0.0–0.7) | 248 | 0.1 | (0.0–0.5) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spadea, T.; Pacelli, B.; Ranzi, A.; Galassi, C.; Rusciani, R.; Demaria, M.; Caranci, N.; Michelozzi, P.; Cerza, F.; Davoli, M.; et al. An Italian Network of Population-Based Birth Cohorts to Evaluate Social and Environmental Risk Factors on Pregnancy Outcomes: The LEAP Study. Int. J. Environ. Res. Public Health 2020, 17, 3614. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103614
Spadea T, Pacelli B, Ranzi A, Galassi C, Rusciani R, Demaria M, Caranci N, Michelozzi P, Cerza F, Davoli M, et al. An Italian Network of Population-Based Birth Cohorts to Evaluate Social and Environmental Risk Factors on Pregnancy Outcomes: The LEAP Study. International Journal of Environmental Research and Public Health. 2020; 17(10):3614. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103614
Chicago/Turabian StyleSpadea, Teresa, Barbara Pacelli, Andrea Ranzi, Claudia Galassi, Raffaella Rusciani, Moreno Demaria, Nicola Caranci, Paola Michelozzi, Francesco Cerza, Marina Davoli, and et al. 2020. "An Italian Network of Population-Based Birth Cohorts to Evaluate Social and Environmental Risk Factors on Pregnancy Outcomes: The LEAP Study" International Journal of Environmental Research and Public Health 17, no. 10: 3614. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103614