Social Dialogue and Psychosocial Risk Management: Added Value of Manager and Employee Representative Agreement in Risk Perception and Awareness

 ,
,  , and
, and
Abstract
:1. Introduction
2. Stakeholder Perceptions and Psychosocial Risk Management
3. Materials and Methods
3.1. Design
3.2. Study Population
3.3. Psychosocial Risk Perception and Awareness
3.4. General Occupational Safety and Health Risk Perception and Awareness
3.5. Psychosocial Risk Management
3.6. General Measures for Traditional OSH Management
3.7. Data Analysis
4. Results
4.1. Degree of Agreement and Discrepancies in Risk Perception and Awareness
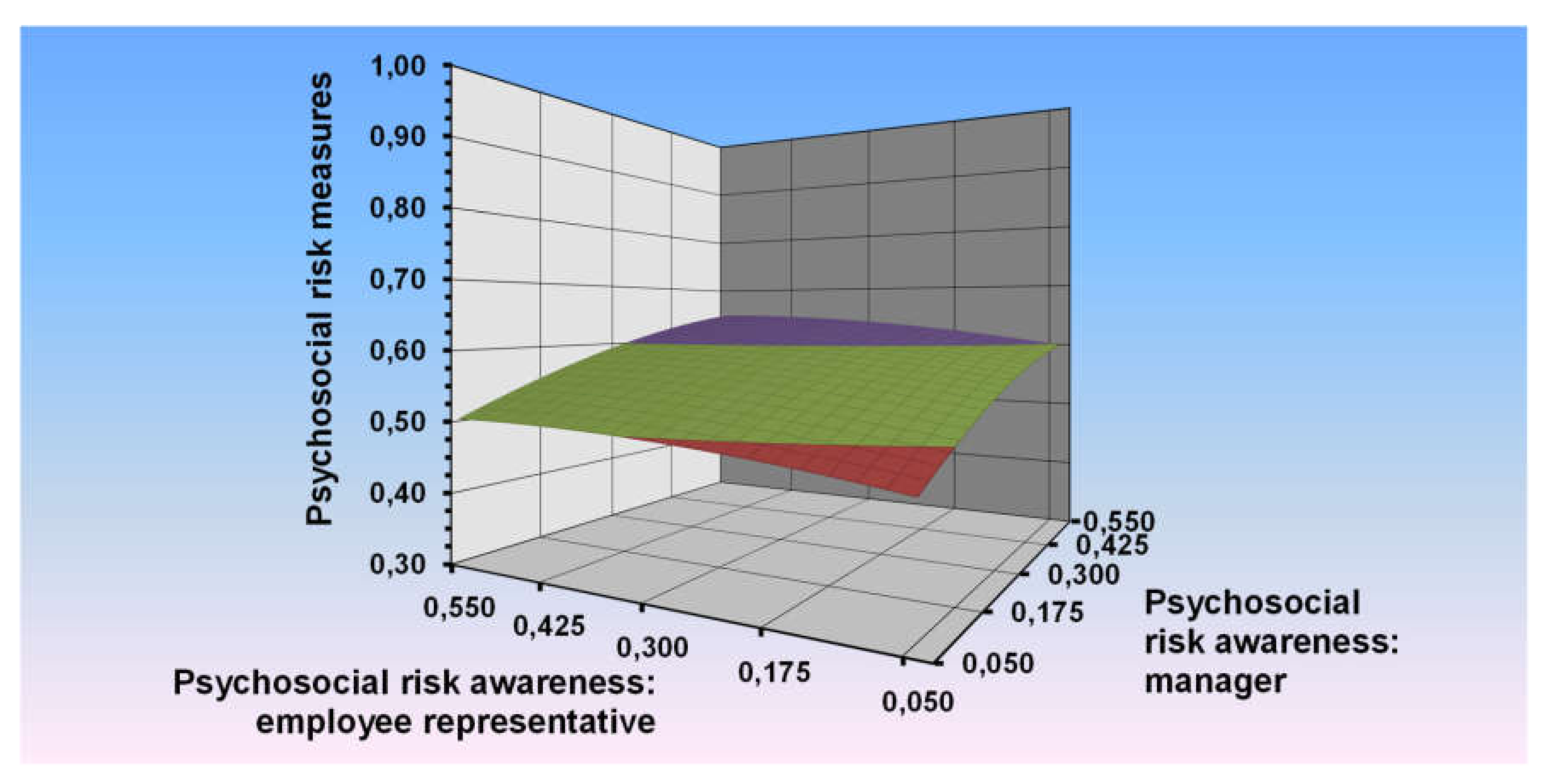
4.2. Psychosocial Risk Perception and Awareness Explaining Psychosocial Risk Management
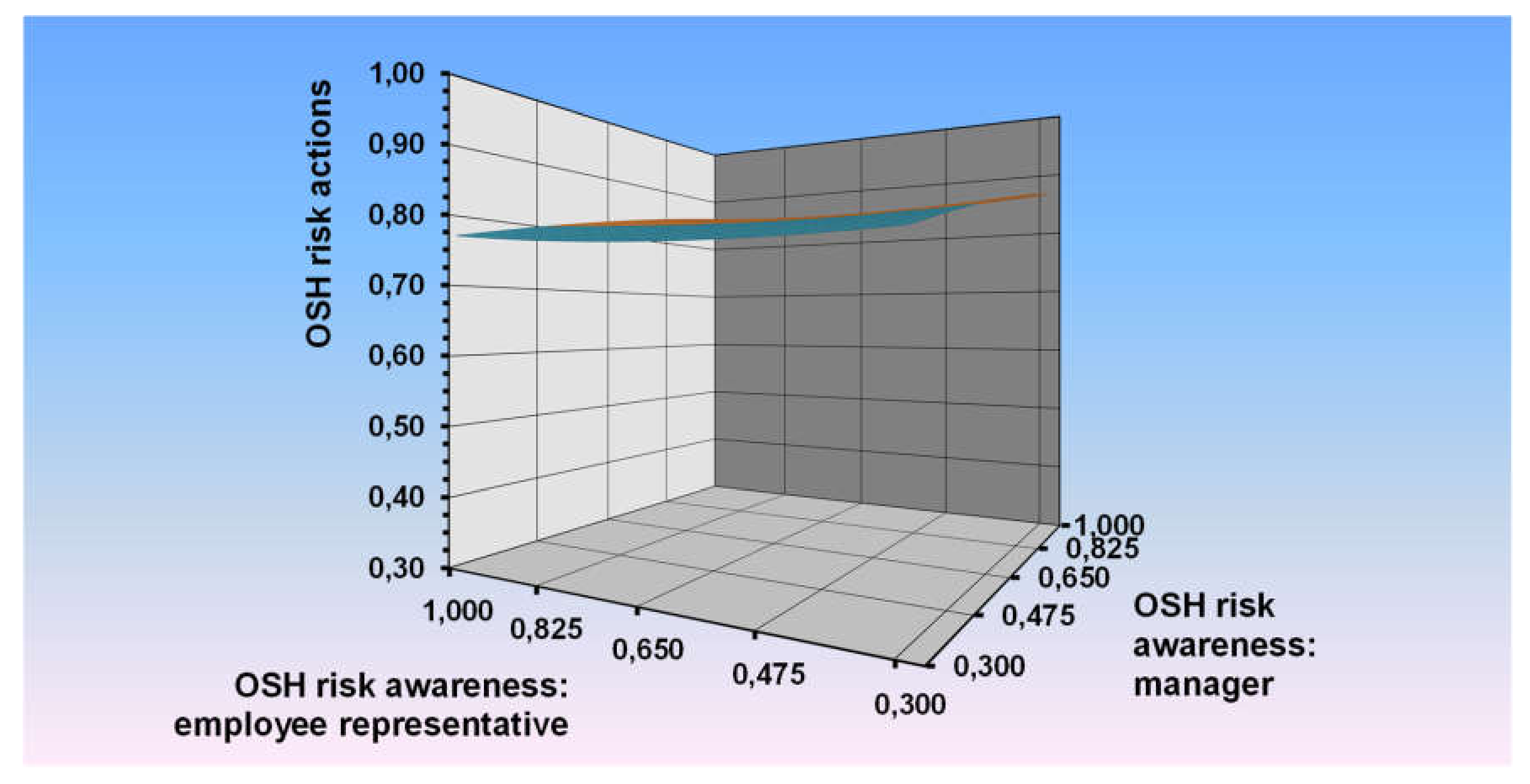
4.3. Perception and Awareness of Traditional OSH Risks and Traditional Risk Management
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Labour Organization. Work Related Stress: A Collective Challenge; International Labour Office: Geneva, Switzerland, 2016. [Google Scholar]
- Davies, R.; Jones, P. Trends and Context to Rates of Workplace Injury; HSE Books: Sudbury, UK, 2005. [Google Scholar]
- Eurofound—European Foundation for the Improvement of Living and Working Conditions. Working Conditions and Workers’ Health; European Foundation for the improvement of living and working conditions: Dublin, Ireland, 2019. [Google Scholar]
- Eurofound & EU-OSHA. Psychosocial Risks in Europe: Prevalence and Strategies for Prevention; Publications Office of the European Union: Brussels, Belgium, 2014. [Google Scholar]
- Leka, S.; Jain, A. Health impact of Psychosocial Hazards at Work: An Overview; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- European Agency for Safety and Health at Work. European Risk Observatory Report: Expert Forecast on Emerging Psychosocial Risks Related to Occupational Safety and health; Publications Office of the European Union: Brussels, Belgium, 2007. [Google Scholar]
- European Agency for Safety and Health at Work. European Survey of Enterprises on New and Emerging Risks: Managing safety and Health at Work; Publications Office of the European Union: Brussels, Belgium, 2010. [Google Scholar]
- European Agency for Safety and Health at Work. Second European Survey of Enterprises on New and Emerging Risks (ESENER-2); Publications Office of the European Union: Brussels, Belgium, 2016. [Google Scholar]
- European Agency for Safety and Health at Work. Management of Psychosocial Risks in European Workplaces: Evidence from the Second European Survey of Enterprises on New and Emerging Risks (ESENER-2); Publications Office of the European Union: Brussels, Belgium, 2018. [Google Scholar]
- European Agency for Safety and Health at Work. Third European Survey of Enterprises on New and Emerging Risks (ESENER 3)–First Findings; Publications Office of the European Union: Brussels, Belgium, 2019. [Google Scholar]
- Bonde, J.P.E. Psychosocial factors at work and risk of depression: A systematic review of the epidemiological evidence. Occup. Environ. Med. 2008, 65, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Madsen, I.E.; Nyberg, S.T.; Hanson, L.M.; Ferrie, J.E.; Ahola, K.; Alfredsson, L.; Batty, G.D.; Bjorner, J.B.; Borritz, M.; Burr, H.; et al. Job strain as a risk factor for clinical depression: Systematic review and meta-analysis with additional individual participant data. Psychol. Med. 2017, 47, 1342–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Netterstrøm, B.; Conrad, N.; Bech, P.; Fink, P.; Olsen, O.; Rugulies, R.; Stansfeld, S. The relation between work-related psychosocial factors and the development of depression. Epidemiol. Rev. 2008, 30, 118–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eller, N.H.; Netterstrøm, B.; Gyntelberg, F.; Kristensen, T.S.; Nielsen, F.; Steptoe, A.; Theorell, T. Work-related psychosocial factors and the development of ischemic heart disease: A systematic review. Cardiol. Rev. 2009, 17, 83–97. [Google Scholar] [CrossRef]
- Kivimaki, M.; Nyberg, S.T.; Batty, G.D.; Fransson, E.I.; Heikkila, K.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Steptoe, A.P.A.; Theorell, T. Job strain as a risk factor for future coronary heart disease: Collaborative meta-analysis of 2358 events in 197,473 men and women. Lancet 2012, 380, 1491–1497. [Google Scholar]
- Briggs, A.M.; Bragge, P.; Smith, A.; Govil, D.; Straker, L.M. Prevalence and Associated Factors for Thoracic Spine Pain in the Adult Working Population: A Literature Review. J. Occup. Health 2009, 51, 177–192. [Google Scholar] [CrossRef] [Green Version]
- Da Costa, B.E.; Vieira, E.R. Risk factors for work-related musculoskeletal disorders: A systematic review of recent longitudinal studies. Am. J. Ind. Med. 2010, 53, 285–323. [Google Scholar] [CrossRef]
- Dekkers-Sánchez, P.M.; Hoving, J.L.; Sluiter, J.K.; Frings-Dresen, M.H.W. Factors associated with long-term sick leave in sick-listed employees: A systematic review. Occup. Environ. Med. 2008, 65, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Duijts, S.F.A.; Kant, I.J.; Swaen, G.M.H.; Brandt, P.A.v.d.; Zeegers, M.P.A. Meta-analysis of observational studies identifies predictors of sickness absence. J. Clin. Epidemiol. 2007, 60, 1105–1115. [Google Scholar] [CrossRef]
- Leka, S.; Jain, A.; Iavicoli, S.; Vartia, M.; Ertel, M. The role of policy for the management of psychosocial risks at the workplace in the European Union. Saf. Sci. 2011, 49, 558–564. [Google Scholar] [CrossRef]
- Iavicoli, S.; Natali, E.; Deitinger, P.; Rondinone, B.M.; Ertel, M.; Jain, A.; Leka, S. Occupational health and safety policy and psychosocial risks in Europe: The role of stakeholders’ perceptions. Health Policy 2011, 101, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Ertel, M.; Stilijanow, U.; Iavicoli, S.; Natali, E.; Jain, A.; Leka, S. European social dialogue on psychosocial risks at work: Benefits and challenges. Eur. J. Ind. 2010, 16, 169–183. [Google Scholar] [CrossRef]
- European Agency for Safety and Health at Work. Worker Representation and Consultation on Health and Safety—An Analysis of the Findings of the European Survey of Enterprises on New and Emerging Risks (ESENER); Publications Office of the European Union: Brussels, Belgium, 2012. [Google Scholar]
- International Labour Organization. ILO Introductory Report: Global Trends and Challenges on Occupational Safety and Health; International Labour Office: Geneva, Switzerland, 2011. [Google Scholar]
- Pandit, B.; Albert, A.; Patil, Y.; Al-Bayati, A.J. Impact of safety climate on hazard recognition and safety risk perception. Saf. Sci. 2019, 113, 44–53. [Google Scholar] [CrossRef]
- International Standardization Organization. ISO 45001:2018-Occupational Health and Safety Management Systems: Requirements with Guidance for Use; ISO: Geneva, Switzerland, 2018. [Google Scholar]
- European Agency for Safety and Health at Work. Drivers and Barriers for Psychosocial Risk Management—An Analysis of the Findings of the European Survey of Enterprises on New and Emerging Risks (ESENER); Publications Office of the European Union: Brussels, Belgium, 2012. [Google Scholar]
- European Agency for Safety and Health at Work. Joint analysis of ESENER-2, the LFS 2013 ad hoc Module on Accidents at Work and Other Work-Related Health Problems and the 6th EWCS; Publications Office of the European Union: Brussels, Belgium, 2017. [Google Scholar]
- Knispel, A.; Voordouw, I.; Onrust, S. Implementatie van groepsinterventies in de preventieve GGZ. TSG 2011, 89, 35–42. [Google Scholar] [CrossRef]
- Koppelaar, E.; Knibbe, J.J.; Miedema, H.S.; Burdorf, A. Determinants of implementation of primary preventive interventions on patient handling in healthcare: A systematic review. Occup. Environ. Med. 2009, 66, 353–360. [Google Scholar] [CrossRef] [Green Version]
- Rundmo, T. Associations between risk perception and safety. Saf. Sci. 1996, 24, 197–209. [Google Scholar] [CrossRef]
- Aven, T.; Renn, O. Risk Management and Governance: Concepts, Guidelines and Applications; Springer Science & Business Media: Singapore, 2010. [Google Scholar]
- Han, S.; Saba, F.; Lee, S.; Mohamed, Y.; Peña-Mora, F. Toward an understanding of the impact of production pressure on safety performance in construction operations. Accid. Anal. Prev. 2014, 68, 106–116. [Google Scholar] [CrossRef]
- Huang, Y.H.; Verma, S.K.; Chang, W.R.; Courtney, T.K.; Lombardi, D.A.; Brennan, M.J.; Perry, M.J. Management commitment to safety vs. employee perceived safety training and association with future injury. Accid. Anal. Prev. 2012, 47, 94–101. [Google Scholar] [CrossRef]
- Huang, Y.H.; Robertson, M.M.; Lee, J.; Rineer, J.; Murphy, L.A.; Garabet, A.; Dainoff, M.J. Supervisory interpretation of safety climate versus employee safety climate perception: Association with safety behavior and outcomes for lone workers. Transp. Res. Part F Traffic Psychol. Behav. 2014, 26, 348–360. [Google Scholar] [CrossRef] [Green Version]
- Gittleman, J.L.; Gardner, P.C.; Haile, E.; Sampson, J.M.; Cigularov, K.P.; Ermann, E.D.; Stafford, P.; Chen, P.Y. CityCenter and Cosmopolitan Construction Projects, Las Vegas, Nevada: Lessons learned from the use of multiple sources and mixed methods in a safety needs assessment. J. Saf. Res. 2010, 41, 263–281. [Google Scholar] [CrossRef]
- Marín, L.S.; Lipscomb, H.; Cifuentes, M.; Punnett, L. Perceptions of safety climate across construction personnel: Associations with injury rates. Saf. Sci. 2019, 118, 487–496. [Google Scholar] [CrossRef]
- Gormley, D.K. Are we on the same page? Staff nurse and manager perceptions of work environment, quality of care and anticipated nurse turnover. J. Nurs. Manag. 2011, 19, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Houtman, I.L.D.; van der Ploeg, K.; de Vroome, E.; Ramaekers, M. Core figures. In Arbobalans; Douwes, M., Hooftman, W., Eds.; TNO: Leiden, The Netherlands, 2019; pp. 65–73. (in Dutch) [Google Scholar]
- Houtman, I.L.D.; Goudswaard, A.; Dhondt, S.; van der Grinten, M.P.; Hildebrandt, V.H.; Poel, E.G.T. Dutch monitor on stress and physical load: Risk factors, consequences, and preventive action. Occup. Environ. Med. 1998, 55, 73–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houtman, I.L.D. Monitor stress en lichamelijke belasting: Werkgevers en werknemers over risico’s, gevolgen en maatregelen. Gedrag en Organ. 1999, 12, 364–383. [Google Scholar]
- Mathisen, G.E.; Brønnick, K.; Arntzen, K.J.; Bergh, L.I.V. Identifying and managing psychosocial risks during organizational restructuring: It’s what you do and how you do it. Saf. Sci. 2017, 100, 20–29. [Google Scholar] [CrossRef]
- International Labour Organization. Social Dialogue Interventions: What Works and Why? Lessons Learned from a Synthesis Review 2013–2016; International Labour Office: Geneva, Switzerland, 2017. [Google Scholar]
- Jain, A.; Leka, S. Social Dialogue in Occupational Safety and Health. OSH-Wiki: Online Encyclopaedia of the European Agency for Safety and Health at Work. 2013. Available online: https://oshwiki.eu/wiki/Social_dialogue_in_occupational_safety_and_health (accessed on 14 May 2020).
- European Social Partners. Framework Agreement on Work-Related Stress; European social partners-ETUC, UNICE(BUSINESSEUROPE), UEAPME and CEEP: Brussels, Belgium, 2004. [Google Scholar]
- European Social Partners. Framework Agreement on Harassment and Violence at Work; Social partners-ETUC, BUSINESSEUROPE, UEAPME and CEEP: Brussels, Belgium, 2007. [Google Scholar]
- European Foundation for the Improvement of Living and Working Conditions. Working Conditions and Social Dialogue; European Foundation for the improvement of living and working conditions: Dublin, Ireland, 2011. [Google Scholar]
- Jespersen, A.H.; Halse, P.; Nielsen, K.T. The wicked character of psychosocial risks: Implications for regulation. NJWLS 2016, 6, 23–42. [Google Scholar] [CrossRef] [Green Version]
- European Agency for Safety and Health at Work. Calculating the Costs of Work-Related Stress and Psychosocial Risks—A Literature Review; Publications Office of the European Union: Brussels, Belgium, 2014. [Google Scholar]
- Riedmann, A.; Pfister, M. European Survey on New and Emerging Risks–Psychosocial Risks (ESENER-PSR 2009). Technical Report: Methodology, Questionnaire Development and Fieldwork; TNS Infratest: Munich, Germany, 2009. [Google Scholar]
- Fleenor, J.W.; McCauley, C.D.; Brutus, S. Self-other rating agreement and leader effectiveness. Leadersh. Q. 1996, 7, 487–506. [Google Scholar] [CrossRef]
- Edwards, J.R. The study of congruence in organizational behavior research: Critique and proposed alternative. Organ. Behav. Hum. Decis. Process 1994, 58, 51–100. [Google Scholar] [CrossRef] [Green Version]
- Aiken, L.S.; West, S.G. Multiple Regression: Testing and Interpreting Interactions; Sage: Newbury Park, CA, USA, 1991. [Google Scholar]
- Edwards, J.R.; Parry, M.E. On the use of polynomial regressions equations as an alternative to difference scores in organizational research. Acad. Manag. J. 1993, 36, 1577–1613. [Google Scholar]
- Shanock, L.R.; Baran, B.E.; Gentry, W.A.; Pattison, S.C.; Heggestad, E.D. Polynomial regression with response surface analysis: A powerful approach for examining moderation and overcoming limitations of difference scores. J. Bus. Psychol. 2010, 25, 543–554. [Google Scholar] [CrossRef]
- Edwards, J.R. Alternatives to difference scores: Polynomial regression analysis and response surface methodology. In Advances in Measurement and Data Analysis; Drasgow, F., Schmitt, N.W., Eds.; Jossey-Bass: San Francisco, CA, USA, 2002; pp. 350–400. [Google Scholar]
- European Agency for Safety and Health at Work. Worker Participation in the Management of Occupational Safety and Health: Qualitative Evidence from ESENER-2; Publications Office of the European Union: Brussels, Belgium, 2017. [Google Scholar]
- Westgaard, R.H.; Winkel, J. Occupational musculoskeletal and mental health: Significance of rationalization and opportunities to create sustainable production systems—A systematic review. Appl. Ergon. 2011, 42, 261–296. [Google Scholar] [CrossRef] [PubMed]
- Houtman, I.L.D.; Kraan, K. Absence policy during years of recession: The employer perspective. In Restricted in Function: Trend Report on Sickness Absence, Work Disability and Labour Participation of People with Chronic Health Problems; Versantvoort, M., van Echtelt, P., Eds.; SCP: Hague, The Netherlands, 2016; Chapter 5; pp. 99–129. (In Dutch) [Google Scholar]
- European Social Partners. Implementation of the European Autonomous Framework Agreement on Work-Related Stress; Report adopted by the European Social Partners–Adopted at the Social Dialogue Committee on 18 June 2008; European social partners-ETUC, BUSINESSEUROPE, UEAPME and CEEP: Brussels, Belgium, 2008. [Google Scholar]
- European Social Partners. Implementation of the European Autonomous Framework Agreement on Harassment and Violence at Work; Report adopted by the European Social Partners–Adopted at the Social Dialogue Committee on 24 October 2011; European social partners-ETUC, BUSINESSEUROPE, UEAPME and CEEP: Brussels, Belgium, 2011. [Google Scholar]
- European Commission. Report on the Implementation of the European Social Partners-Framework Agreement on Work-Related Stress; SEC(2011) 241 Final, Commission Staff Working Paper; European Commission: Brussels, Belgium, 2011. [Google Scholar]
- European Commission. Study on the Implementation of the Autonomous Framework Agreement on Harassment and Violence at Work; Publications Office of the European Union: Brussels, Belgium, 2016. [Google Scholar]
- Joint Action on Mental Health and Well-being. Mental Health at the Workplace: Situation Analysis and Recommendations for Action. 2015. Available online: https://www.mentalhealthandwellbeing.eu/publications/ (accessed on 14 May 2020).
- European Commission. EU Strategic Framework on Health and Safety at Work 2014–2020. COM(2014) 332 Final. 2014. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:52014DC0332 (accessed on 14 May 2020).
- Leka, S.; Jain, A. Mental Health in the Workplace in the European Union: Consensus Paper. EU Compass for Action on Mental Health & Well-Being. European Commission. 2017. Available online: https://ec.europa.eu/health/sites/health/files/mental_health/docs/compass_2017workplace_en.pdf (accessed on 14 May 2020).



{kind=link}
{kind=link}
| Enterprise Characteristics | Interview with Both Management and Employee Representative (%) | Only Management Interview (%) | Total (%) | |
|---|---|---|---|---|
| Company size | 10–19 | 13.7 ▼ | 29.6 ▲ | 25.6 |
| 20–49 | 22.3 ▼ | 29.1 ▲ | 27.4 | |
| 50–99 | 16.3 ▲ | 14.6 ▼ | 15.1 | |
| 100+ | 47.7 ▲ | 26.7 ▼ | 32.0 | |
| Establishment founded 1 | Before 1990 | 61.6 ▲ | 51.5 ▼ | 53.6 |
| Between 1990 and 2005 | 33.9 ▼ | 43.3 ▲ | 41.1 | |
| After 2005 | 3.9 ▼ | 4.6 ▲ | 4.5 | |
| Does this establishment belong to the public sector? 1 | Yes | 26.3 ▲ | 20.1 ▼ | 21.7 |
| No | 73.3 ▼ | 79.5 ▲ | 77.9 | |
| Sector (NACE) | ||||
| C—Mining and quarrying | 0.6 | 0.7 | 0.7 | |
| D—Manufacturing | 32.7 ▲ | 28.6 ▼ | 29.6 | |
| E—Electricity, gas and water supply | 2.0 ▲ | 1.0 ▼ | 1.2 | |
| F—Construction | 8.0 ▼ | 10.2 ▲ | 9.6 | |
| G—Wholesale and retail trade; repair of motor vehicles, motorcycles and personal and household goods | 11.1 ▼ | 15.9 ▲ | 14.7 | |
| H—Hotels and restaurants | 1.9 ▼ | 3.8 ▲ | 3.3 | |
| I—Transport, storage & communication | 4.6 | 4.6 | 4.6 | |
| J—Financial intermediation | 2.4 | 2.5 | 2.5 | |
| K—Real estate, renting & business act. | 8.5 ▼ | 9.8 ▲ | 9.5 | |
| L—Public administration and defence; compulsory social security | 6.1 ▲ | 5.0 ▼ | 5.3 | |
| M—Education | 7.9 | 7.4 | 7.6 | |
| N—Health and social work | 9.8 ▲ | 6.7 ▼ | 7.5 | |
| O—Other community, social and personal service activities | 4.6 ▲ | 3.8 ▼ | 4.0 | |
| Country | ||||
| BE | 3.2 ▼ | 3.9 ▲ | 3.7 | |
| DK | 7.2 ▲ | 2.3 ▼ | 3.5 | |
| DE | 6.9 ▲ | 4.7 ▼ | 5.3 | |
| EL | 1.8 ▼ | 4.1 ▲ | 3.5 | |
| ES | 5.2 | 5.6 | 5.5 | |
| FI | 9.5 ▲ | 1.5 ▼ | 3.5 | |
| FR | 5.4 | 5.2 | 5.2 | |
| IE | 2.3 ▲ | 1.6 ▼ | 1.8 | |
| IT | 6.7 ▲ | 4.8 ▼ | 5.2 | |
| LU | 1.5 | 1.8 | 1.7 | |
| NL | 2.9 ▼ | 3.7 ▲ | 3.5 | |
| AT | 2.3 ▼ | 4.0 ▲ | 3.6 | |
| PT | 0.7 ▼ | 4.5 ▲ | 3.5 | |
| SE | 7.2 ▲ | 2.2 ▼ | 3.5 | |
| UK | 4.2 ▼ | 5.6 ▲ | 5.2 | |
| BG | 3.2 ▲ | 1.3 ▼ | 1.7 | |
| CY | 0.7 ▼ | 2.1 ▲ | 1.8 | |
| CZ | 2.5 ▼ | 3.9 ▲ | 3.5 | |
| EE | 2.7 ▲ | 1.4 ▼ | 1.7 | |
| HU | 2.9 ▼ | 3.8 ▲ | 3.6 | |
| LV | 1.7 | 1.8 | 1.8 | |
| LT | 1.1 ▼ | 2.0 ▲ | 1.8 | |
| MT | 0.8 ▼ | 1.3 ▲ | 1.2 | |
| PL | 5.0 | 5.3 | 5.2 | |
| RO | 1.8 | 1.8 | 1.8 | |
| SK | 0.9 ▼ | 2.1 ▲ | 1.8 | |
| SI | 1.1▼ | 2.1 ▲ | 1.8 | |
| TR | 1.8 ▼ | 6.4 ▲ | 5.2 | |
| HR | 1.7 | 1.7 | 1.7 | |
| CH | 1.8 ▼ | 4.2 ▲ | 3.6 | |
| NO | 3.4 | 3.3 | 3.3 | |
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|---|---|
| 1. | Psychosocial risk perception and awareness, employee representative | 0.34 | 0.25 | - | ||||
| 2. | Psychosocial risk perception and awareness, manager | 0.31 | 0.23 | 0.21 ** | - | |||
| 3. | Occupational safety and health perception and awareness, employee representative | 0.70 | 0.36 | 0.16 ** | 0.08 ** | - | ||
| 4. | Occupational safety and health perception and awareness, manager | 0.72 | 0.35 | 0.07 ** | 0.18 ** | 0.43 ** | - | |
| 5. | Psychosocial risk measures, manager | 0.47 | 0.31 | 0.15 ** | 0.27 ** | 0.06 ** | 0.09 ** | - |
| 6. | Occupational safety and health measures, manager | 0.61 | 0.35 | 0.03 ** | 0.00 | 0.06 ** | 0.09 ** | 0.17 ** |
| Agreement Groups | Psychosocial Risk Perception & Awareness (%) | OSH Risk Perception & Awareness (%) |
|---|---|---|
| Manager perception and awareness and employee representative perception and awareness in agreement | 36 | 49 |
| Employee representative perception and awareness higher than manager perception and awareness | 32 | 24 |
| Manager perception and awareness higher than employee representative perception and awareness | 32 | 27 |
| Psychosocial Risk Measures | |
|---|---|
| Variable | b (SE) |
| 1. Perception & awareness manager | 0.28 (0.02) *** |
| 2. Perception & awareness employee representative | 0.09 (0.02) *** |
| 3. Perception & awareness manager squared | −0.32 (0.05) *** |
| 4. Perception & awareness manager × Perception & awareness employee representative | 0.04 (0.06) |
| 5. Perception & awareness employee representative squared | −0.20 (0.05) *** |
| R2 (explained variance) | 9.0% |
| Surface tests | |
| a1 (the linear slope of the line of perfect agreement) | 0.37 *** |
| a2 (the curvature of the line of perfect agreement) | −0.48 *** |
| a3 (the linear slope of the line of disagreement) | 0.19 *** |
| a4 (the curvature of the line of disagreement) | −0.56 *** |
| ‘Perceived Impact of General Occupational Safety and Health Policy’ | |
|---|---|
| Variable | b (SE) |
| 1. Perception & awareness manager | 0.15 (0.02) *** |
| 2. Perception & awareness employee representative | 0.01 (0.02) |
| 3. Perception and awareness manager squared | −0.07 (0.05) |
| 4. Perception & awareness manager × Perception & awareness employee representative | −0.05 (0.04) |
| 5. Perception & awareness employee representative squared | 0.10 (0.05) * |
| R2 (explained variance) | 2.0% |
| Surface tests | |
| a1 (the linear slope of the line of perfect agreement) | 0.16 *** |
| a2 (the curvature of the line of perfect agreement) | −0.02 |
| a3 (the linear slope of the line of disagreement) | 0.14 *** |
| a4 (the curvature of the line of disagreement) | 0.09 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Houtman, I.; van Zwieten, M.; Leka, S.; Jain, A.; de Vroome, E. Social Dialogue and Psychosocial Risk Management: Added Value of Manager and Employee Representative Agreement in Risk Perception and Awareness. Int. J. Environ. Res. Public Health 2020, 17, 3672. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103672
Houtman I, van Zwieten M, Leka S, Jain A, de Vroome E. Social Dialogue and Psychosocial Risk Management: Added Value of Manager and Employee Representative Agreement in Risk Perception and Awareness. International Journal of Environmental Research and Public Health. 2020; 17(10):3672. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103672
Chicago/Turabian StyleHoutman, Irene, Marianne van Zwieten, Stavroula Leka, Aditya Jain, and Ernest de Vroome. 2020. "Social Dialogue and Psychosocial Risk Management: Added Value of Manager and Employee Representative Agreement in Risk Perception and Awareness" International Journal of Environmental Research and Public Health 17, no. 10: 3672. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103672