A Lifestyle (Dietary) Intervention Reduces Tiredness in Children with Subclinical Hypothyroidism, a Randomized Controlled Trial

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Population
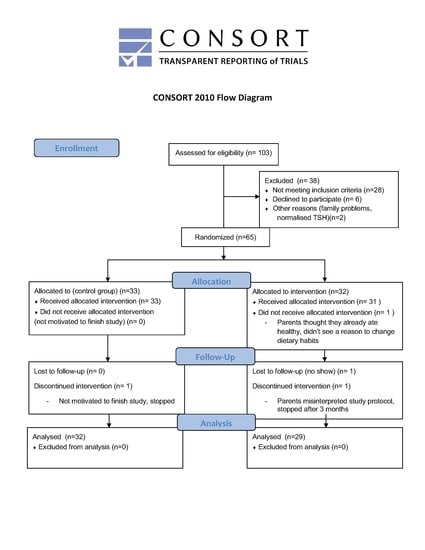
2.2. Recruitment and Randomization
2.3. Study Protocol
2.4. Intervention
2.5. Measurements
2.6. Questionnaires
2.7. Statistical Analysis
2.8. Outcomes
3. Results
3.1. Patient Descriptives
3.2. Outcomes
3.3. Tiredness
3.4. Growth
3.5. Lipid Profile
3.6. Adherence to the Diet
4. Discussion
4.1. Limitations and Future Directions
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Surks, M.I.; Ortiz, E.; Daniels, G.H.; Sawin, C.T.; Col, N.F.; Cobin, R.H.; Franklyn, J.A.; Hershman, J.M.; Burman, K.D.; Denke, M.A.; et al. Subclinical thyroid disease: Scientific review and guidelines for diagnosis and management. JAMA 2004, 291, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Flowers, J.W.; Tudiver, F.; Wilson, J.L.; Punyasavatsut, N. Subclinical thyroid disorders and cognitive performance among adolescents in the United States. BMC Pediatr. 2006, 6, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paoli-Valeri, M.; Maman-Alvarado, D.; Jimenez-Lopez, V.; Arias-Ferreira, A.; Bianchi, G.; Arata-Bellabarba, G. Frequency of subclinical hypothyroidism among healthy children and those with neurological conditions in the state of Merida, Venezuela. Investig. Clin. 2003, 44, 209–218. [Google Scholar]
- Lazar, L.; Frumkin, R.B.; Battat, E.; Lebenthal, Y.; Phillip, M.; Meyerovitch, J. Natural history of thyroid function tests over 5 years in a large pediatric cohort. J. Clin. Endocrinol. Metab. 2009, 94, 1678–1682. [Google Scholar] [CrossRef]
- Canaris, G.J.; Manowitz, N.R.; Mayor, G.; Ridgway, E.C. The Colorado thyroid disease prevalence study. Arch. Intern. Med. 2000, 160, 526–534. [Google Scholar] [CrossRef] [Green Version]
- Papi, G.; Uberti, E.D.; Betterle, C.; Carani, C.; Pearce, E.N.; Braverman, L.E.; Roti, E. Subclinical hypothyroidism. Curr. Opin. Endocrinol. Diabetes Obes. 2007, 14, 197–208. [Google Scholar] [CrossRef] [Green Version]
- Shriraam, M.; Sridhar, M. Subclinical hypothyroidism in children. Indian Pediatr. 2014, 51, 889–895. [Google Scholar] [CrossRef]
- Aijaz, N.J.; Flaherty, E.M.; Preston, T.; Bracken, S.S.; Lane, A.H.; Wilson, T.A. Neurocognitive function in children with compensated hypothyroidism: Lack of short term effects on or off thyroxin. BMC Endocr. Disord. 2006, 6, 2. [Google Scholar] [CrossRef] [Green Version]
- Gawlik, A.; Such, K.; Dejner, A.; Zachurzok, A.; Antosz, A.; Malecka-Tendera, E. Subclinical hypothyroidism in children and adolescents: Is it clinically relevant? Int. J. Endocrinol. 2015, 2015, 691071. [Google Scholar] [CrossRef]
- Ergur, A.T.; Taner, Y.; Ata, E.; Melek, E.; Bakar, E.E.; Sancak, T. Neurocognitive functions in children and adolescents with subclinical hypothyroidism. J. Clin. Res. Pediatr. Endocrinol. 2012, 4, 21–24. [Google Scholar] [CrossRef]
- Cerbone, M.; Capalbo, D.; Wasniewska, M.; Mattace Raso, G.; Alfano, S.; Meli, R.; De Luca, F.; Salerno, M. Cardiovascular risk factors in children with long-standing untreated idiopathic subclinical hypothyroidism. J. Clin. Endocrinol. Metab. 2014, 99, 2697–2703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ittermann, T.; Thamm, M.; Wallaschofski, H.; Rettig, R.; Volzke, H. Serum thyroid-stimulating hormone levels are associated with blood pressure in children and adolescents. J. Clin. Endocrinol. Metab. 2012, 97, 828–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Althaus, B.U.; Staub, J.J.; Ryff-De Leche, A.; Oberhansli, A.; Stahelin, H.B. LDL/HDL-changes in subclinical hypothyroidism: Possible risk factors for coronary heart disease. Clin. Endocrinol. (Oxf.) 1988, 28, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Kvetny, J.; Heldgaard, P.E.; Bladbjerg, E.M.; Gram, J. Subclinical hypothyroidism is associated with a low-grade inflammation, increased triglyceride levels and predicts cardiovascular disease in males below 50 years. Clin. Endocrinol. (Oxf.) 2004, 61, 232–238. [Google Scholar] [CrossRef]
- Crisafulli, G.; Aversa, T.; Zirilli, G.; Pajno, G.B.; Corica, D.; De Luca, F.; Wasniewska, M. Subclinical Hypothyroidism in Children: When a Replacement Hormonal Treatment Might Be Advisable. Front. Endocrinol. (Lausanne) 2019, 10, 109. [Google Scholar] [CrossRef] [Green Version]
- Vigone, M.C.; Capalbo, D.; Weber, G.; Salerno, M. Mild Hypothyroidism in Childhood: Who, When, and How Should Be Treated? J. Endocr. Soc. 2018, 2, 1024–1039. [Google Scholar] [CrossRef]
- Feller, M.; Snel, M.; Moutzouri, E.; Bauer, D.C.; de Montmollin, M.; Aujesky, D.; Ford, I.; Gussekloo, J.; Kearney, P.M.; Mooijaart, S.; et al. Association of Thyroid Hormone Therapy With Quality of Life and Thyroid-Related Symptoms in Patients With Subclinical Hypothyroidism: A Systematic Review and Meta-analysis. JAMA 2018, 320, 1349–1359. [Google Scholar] [CrossRef]
- Andrade, G.R.G.; Gorgulho, B.; Lotufo, P.A.; Bensenor, I.M.; Marchioni, D.M. Dietary Selenium Intake and Subclinical Hypothyroidism: A Cross-Sectional Analysis of the ELSA-Brasil Study. Nutrients 2018, 10, 693. [Google Scholar] [CrossRef] [Green Version]
- Winther, K.H.; Wichman, J.E.; Bonnema, S.J.; Hegedus, L. Insufficient documentation for clinical efficacy of selenium supplementation in chronic autoimmune thyroiditis, based on a systematic review and meta-analysis. Endocrine 2017, 55, 376–385. [Google Scholar] [CrossRef] [Green Version]
- NEVO Tables. Dutch Food Composition Database. Available online: https://nevo-online.rivm.nl/ (accessed on 15 April 2015).
- Kuiper, M.W.J.; van der Gaag, E.J. Subclinical Hypothyroidism in Children Can Normalize after Changes in Dietary Intake. Food Nutr. Sci. 2012, 3, 411–416. [Google Scholar] [CrossRef] [Green Version]
- The Netherlands Nutrition Centre. Example Diet for Young Children. Voedingscentrum. Available online: https://www.voedingscentrum.nl/nl/mijn-kind-en-ik/dreumes-en-peuter/voorbeelddagmenu-voor-dreumes-en-peuter.aspx (accessed on 20 June 2019).
- Zimmermann, M.B. Interactions of vitamin A and iodine deficiencies: Effects on the pituitary-thyroid axis. Int. J. Vitam. Nutr. Res. 2007, 77, 236–240. [Google Scholar] [CrossRef]
- Kandhro, G.A.; Kazi, T.G.; Afridi, H.I.; Kazi, N.; Arain, M.B.; Sarfraz, R.A.; Sirajuddin; Syed, N.; Baig, J.A.; Shah, A.Q. Evaluation of iron in serum and urine and their relation with thyroid function in female goitrous patients. Biol. Trace Elem. Res. 2008, 125, 203–212. [Google Scholar] [CrossRef]
- Wasniewska, M.; Salerno, M.; Cassio, A.; Corrias, A.; Aversa, T.; Zirilli, G.; Capalbo, D.; Bal, M.; Mussa, A.; De Luca, F. Prospective evaluation of the natural course of idiopathic subclinical hypothyroidism in childhood and adolescence. Eur. J. Endocrinol. 2009, 160, 417–421. [Google Scholar] [CrossRef] [Green Version]
- Matusik, P.; Gawlik, A.; Januszek-Trzciakowska, A.; Malecka-Tendera, E. Isolated Subclinical Hyperthyrotropinemia in Obese Children: Does Levothyroxine (LT4) Improve Weight Reduction during Combined Behavioral Therapy? Int. J. Endocrinol. 2015, 2015, 792509. [Google Scholar] [CrossRef] [Green Version]
- Stott, D.J.; Rodondi, N.; Bauer, D.C.; Group, T.S. Thyroid Hormone Therapy for Older Adults with Subclinical Hypothyroidism. N. Engl. J. Med. 2017, 377, e20. [Google Scholar] [CrossRef] [PubMed]
- Steenbruggen, T.G.; Hoekstra, S.J.; van der Gaag, E.J. Could a change in diet revitalize children who suffer from unresolved fatigue? Nutrients 2015, 7, 1965–1977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, M.E.; DeCesare, K.N.; Johnson, A.; Kress, K.S.; Inman, C.L.; Weiss, E.P. Short-Term Mediterranean Diet Improves Endurance Exercise Performance: A Randomized-Sequence Crossover Trial. J. Am. Coll. Nutr. 2019, 38, 597–605. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, L.E.; Biberstine, S.L.; Paddon-Jones, D.; Schwichtenberg, A.J.; Campbell, W.W. Adopting a Mediterranean-Style Eating Pattern with Different Amounts of Lean Unprocessed Red Meat Does Not Influence Short-Term Subjective Personal Well-Being in Adults with Overweight or Obesity. J. Nutr. 2018, 148, 1917–1923. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, K.; Konomi, A. Iron deficiency without anaemia is a potential cause of fatigue: Meta-analyses of randomised controlled trials and cross-sectional studies. Br. J. Nutr. 2017, 117, 1422–1431. [Google Scholar] [CrossRef]
- Hock, A.D. Review: Vitamin D3 deficiency results in dysfunctions of immunity with severe fatigue and depression in a variety of diseases. In Vivo 2014, 28, 133–145. [Google Scholar]
- Apostolova, N.; Victor, V.M. Molecular strategies for targeting antioxidants to mitochondria: Therapeutic implications. Antioxid. Redox Signal. 2015, 22, 686–729. [Google Scholar] [CrossRef] [PubMed]
- Filler, K.; Lyon, D.; Bennett, J.; McCain, N.; Elswick, R.; Lukkahatai, N.; Saligan, L.N. Association of Mitochondrial Dysfunction and Fatigue: A Review of the Literature. BBA Clin. 2014, 1, 12–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Boit, M.; Hunter, A.M.; Gray, S.R. Fit with good fat? The role of n-3 polyunsaturated fatty acids on exercise performance. Metabolism 2017, 66, 45–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Xi, Q.; Zhang, H.; Song, B.; Liu, X.; Mao, X.; Li, J.; Shen, H.; Tang, W.; Zhang, J.; et al. Investigation of thyroid function and blood pressure in school-aged subjects without overt thyroid disease. Endocrine 2012, 41, 122–129. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Intervention Group | Control Group | p-Value | |
|---|---|---|---|
| n = 29 | n = 32 | ||
| Male:female | 15:14 | 16:16 | 0.89 |
| Age in years (SD) | 7.7 (3.1) | 8.1 (3.3) | 0.67 |
| 2-Parents family | 27 (51%) | 26 (49%) | 0.23 |
| Parental education (only primary or high school) | 6 (20.6%) | 1 (3.3%) | 0.32 |
| Tiredness (according to parents) | 23 (79%) | 22 (73%) | 0.59 |
| Positive family history for thyroid diseases (%) | 16 (55%) | 15 (52%) | 0.55 |
| TSH start (mIU/L) (SD) | 6.14 (1.4) | 5.69 (1.4) | 0.15 |
| FT4 start (pmol/L) (SD) | 16.6 (2.1) | 15.7 (1.6) | 0.06 |
| Anti-TPO positive (%) start | 2 (7%) | 4 (12%) | 0.46 |
| Total Cholesterol (mmol/L) (median, IQR) | 4.2 (3.7–4.6) | 4.3 (3.8–4.9) | 0.28 |
| HDL-C (mmol/L) (median, IQR) | 1.4 (1.2–1.8) | 1.4 (1.2–1.8) | 0.80 |
| Cholesterol/HDL ratio (mmol/L) (median, IQR) | 3.0 (2.3–3.5) | 3.1 (2.4–4.0) | 0.61 |
| TG (mmol/L) (median, IQR) | 0.9 (0.7–1.3) | 1.0 (0.6–1.4) | 0.88 |
| LDL-C (mmol/L) (median, IQR) | 2.2 (1.8–2.4) | 2.4 (1.7–3.0) | 0.37 |
| Height (cm) (median, IQR) | 127 (113–139) | 132 (115–148) | 0.25 |
| Weigth (kg) (median, IQR) | 24.9 (21–34) | 31.1 (20–46) | 0.16 |
| BMI (kg/m2) (median, IQR) | 16.0 (15–17) | 17.0 (16–20) | 0.05 |
| Intervention Group | Control Group | p-Value | |||||
|---|---|---|---|---|---|---|---|
| t = 0 | t = 3 | t = 6 | t = 0 | t = 3 | t = 6 | ||
| TSH (mIU/L) | 6.1 (5.6–6.6) | 5.5 (4.8–6.1) | 5.2 (4.5–6.0) | 5.7 (5.2–6.2) | 5.0 (4.3–5.6) | 4.8 (4.1–5.5) | 0.98 |
| FT4 (pmol/L) | 16.6 (16–17) | 17.1 (16–18) | 16.6 (16–17) | 15.7 (15–16) | 16.0 (15–17) | 15.4 (15–16) | 0.51 |
| PedQL total | 61.8 (55–68) | 67.9 (61–75) | 74.1 (67–81) | 70.9 (65–77) | 70.5 (64–77) | 72.8 (66–80) | 0.04 |
| PedQl general | 59.4 (51–67) | 65.6 (57–74) | 72.9 (65–81) | 67.2 (60–75) | 67.9 (60–76) | 72.4 (65–80) | 0.14 |
| PedQl sleep | 62.5 (55–69) | 69.9 (63–77) | 77.8 (71–84) | 72.5 (66–79) | 73.1 (66–79) | 75.9 (70–82) | 0.03 |
| PedQl cognitive | 62.9 (53–73) | 67.1 (57–76) | 70.4 (60–81) | 73.9 (65–83) | 71.4 (62–80) | 71.1 (61–81) | 0.19 |
| Intervention Group | Control Group | p-Value | |||||
|---|---|---|---|---|---|---|---|
| t = 0 | t = 3 | t = 6 | t = 0 | t = 3 | t = 6 | ||
| SD height | −0.28 (−0.6–0.1) | −0.29 (−0.6–0.1) | −0.21 (−0.6–0.2) | 0.1 (−0.2–0.2) | 0.16 (−0.2–0.5) | 0.11 (−0.2–0.5) | 0.18 |
| SD weight | 0.18 (−0.3–0.7) | 0.2 (0.3–0.7) | 0.28 (−0.3–0.8) | 0.78 (0.3–1.2) | 0.83 (0.4–1.3) | 0.8 (0.3–1.3) | 0.24 |
| SD BMI | 0.34 (−0.1–0.8) | 0.37 (−0.1–0.9) | 0.4 (−0.1–0.9) | 0.83 (0.4–1.3) | 0.84 (0.4–1.3) | 0.84 (0.3–1.3) | 0.89 |
| TC (mmol/L) | 4.23 (4.0–4.5) | 4.33 (4.1–4.6) | 4.34 (4.1–4.6) | 4.29 (4.1–4.5) | 4.19 (4.0–4.4) | 4.22 (4.0–4.4) | 0.16 |
| HDL (mmol/L) | 1.4 (1.3–1.6) | 1.44 (1.3–1.6) | 1.52 (1.4–1.7) | 1.47 (1.3–1.6) | 1.43 (1.3–1.6) | 1.46 (1.3–1.6) | 0.20 |
| cholesterol/HDL ratio | 3.21 (2.8–3.6) | 3.15 (2.8–3.5) | 2.99 (2.7–3.3) | 3.19 (2.8–3.5) | 3.14 (2.8–3.4) | 3.09 (2.8–3.3) | 0.78 |
| TG (mmol/L) | 1.14 (0.8–1.4) | 1.32 (0.9–1.3) | 0.91 (0.7–1.1) | 1.15 (0.9–1.4) | 0.98 (0.8–1.2) | 0.98 (0.8–1.2) | 0.35 |
| LDL (mmol/L) | 2.31 (2.1–2.5) | 2.38 (2.–2.6) | 2.42 (2.2–2.6) | 2.3 (2.1–2.5) | 2.31 (2.1–2.5) | 2.3 (2.1–2.5) | 0.57 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Gaag, E.; van der Palen, J.; Schaap, P.; van Voorthuizen, M.; Hummel, T. A Lifestyle (Dietary) Intervention Reduces Tiredness in Children with Subclinical Hypothyroidism, a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 3689. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103689
van der Gaag E, van der Palen J, Schaap P, van Voorthuizen M, Hummel T. A Lifestyle (Dietary) Intervention Reduces Tiredness in Children with Subclinical Hypothyroidism, a Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2020; 17(10):3689. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103689
Chicago/Turabian Stylevan der Gaag, Ellen, Job van der Palen, Pim Schaap, Mirthe van Voorthuizen, and Thalia Hummel. 2020. "A Lifestyle (Dietary) Intervention Reduces Tiredness in Children with Subclinical Hypothyroidism, a Randomized Controlled Trial" International Journal of Environmental Research and Public Health 17, no. 10: 3689. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103689