Gender Differences in Cognitive Impairment among Rural Elderly in China

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
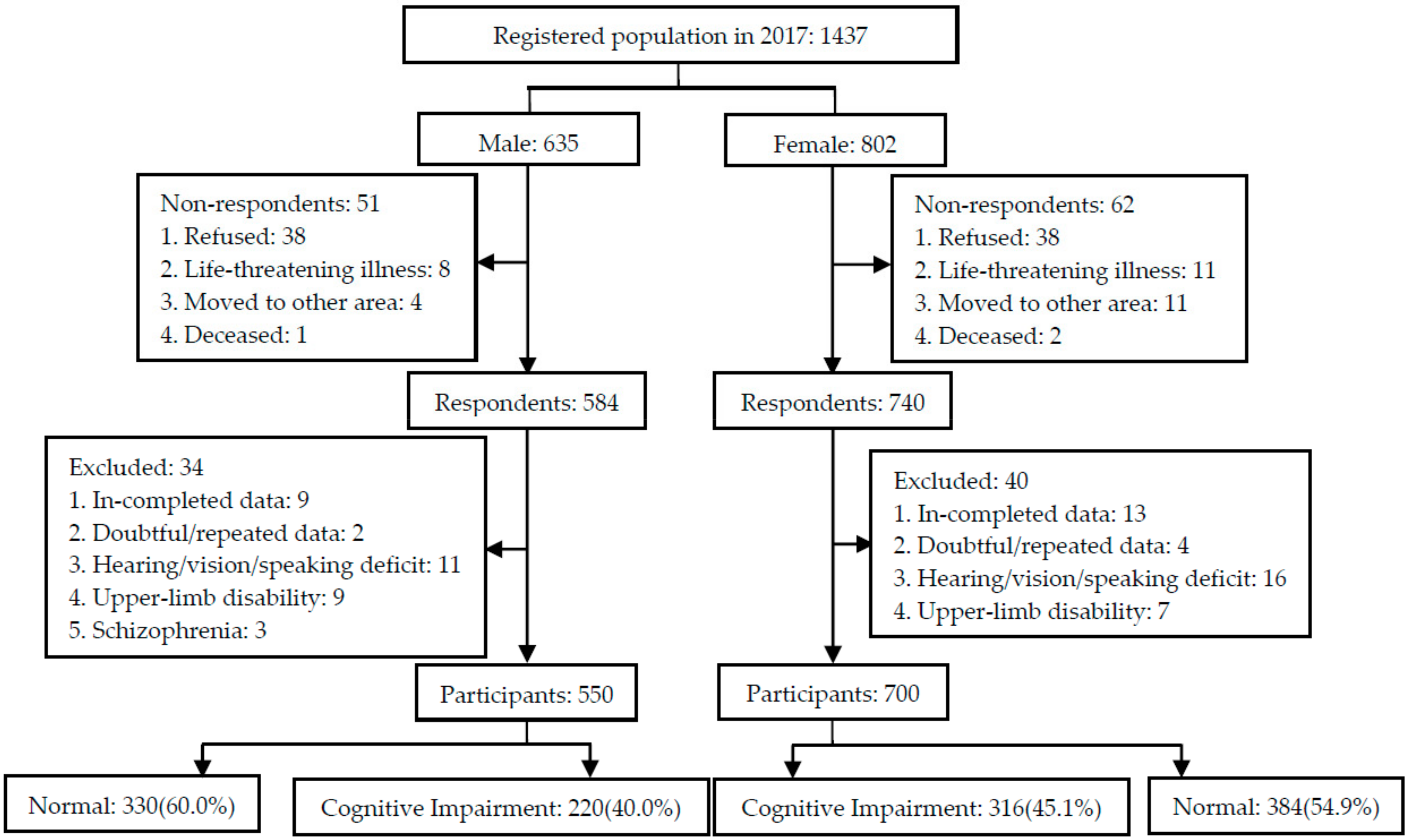
2.2. Setting and Participants
2.3. Data Collection
2.3.1. Demographic Information
2.3.2. Cognitive Function
2.3.3. Lifestyle Factors
2.3.4. Psychosocial Factors
2.3.5. Health-Related Factors
2.4. Data Analysis
3. Results
3.1. Demographic, Lifestyle, and Psychosocial Information
3.2. Health-Related Information
3.3. Cognitive Impairment inMales and Females
3.4. Univariate Analysis of Factors Associated withCognitive Impairment
3.5. Multivariate Analysis of Factors Associated withCognitive Impairment
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Dementia: A Public Health Priority; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Alzheimer’s Disease International. World Alzheimer Report 2018: The State of the Art of Dementia Research; Alzheimer’s Disease International: London, UK, 2018. [Google Scholar]
- Baumgart, M.; Snyder, H.M.; Carrillo, M.C.; Fazio, S.; Kim, H.; Johns, H. Summary of the evidence on modifiable risk factors for cognitive decline and dementia: A population-based perspective. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2015, 11, 718–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deckers, K.; van Boxtel, M.P.; Schiepers, O.J.; de Vugt, M.; Munoz Sanchez, J.L.; Anstey, K.J.; Brayne, C.; Dartigues, J.F.; Engedal, K.; Kivipelto, M.; et al. Target risk factors for dementia prevention: A systematic review and Delphi consensus study on the evidence from observational studies. Int. J. Geriatr. Psychiatry 2015, 30, 234–246. [Google Scholar] [CrossRef] [PubMed]
- Kivipelto, M.; Mangialasche, F.; Ngandu, T. Lifestyle interventions to prevent cognitive impairment, dementia and Alzheimer disease. Nat. Rev. Neurol. 2018, 14, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Disease International. World Alzheimer Report 2014: Dementia and Risk Reduction; Alzheimer’s Disease International: London, UK, 2014. [Google Scholar]
- Heward, J.; Stone, L.; Paddick, S.M.; Mkenda, S.; Gray, W.K.; Dotchin, C.L.; Kissima, J.; Collingwood, C.; Swai, B.; Walker, R.W. A longitudinal study of cognitive decline in rural Tanzania: Rates and potentially modifiable risk factors. Int. Psychogeriatr. IPA 2018, 30, 1333–1343. [Google Scholar] [CrossRef]
- Jia, L.; Quan, M.; Fu, Y.; Zhao, T.; Li, Y.; Wei, C.; Tang, Y.; Qin, Q.; Wang, F.; Qiao, Y.; et al. Dementia in China: Epidemiology, clinical management, and research advances. Lancet Neurol. 2020, 19, 81–92. [Google Scholar] [CrossRef]
- Au, B.; Dale-McGrath, S.; Tierney, M.C. Sex differences in the prevalence and incidence of mild cognitive impairment: A meta-analysis. Ageing Res. Rev. 2017, 35, 176–199. [Google Scholar] [CrossRef]
- Gannon, O.J.; Robison, L.S.; Custozzo, A.J.; Zuloaga, K.L. Sex differences in risk factors for vascular contributions to cognitive impairment & dementia. Neurochem. Int. 2019, 127, 38–55. [Google Scholar] [CrossRef]
- Buckley, R.F.; Mormino, E.C.; Amariglio, R.E.; Properzi, M.J.; Rabin, J.S.; Lim, Y.Y.; Papp, K.V.; Jacobs, H.I.L.; Burnham, S.; Hanseeuw, B.J.; et al. Sex, amyloid, and APOE epsilon4 and risk of cognitive decline in preclinical Alzheimer’s disease: Findings from three well-characterized cohorts. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2018, 14, 1193–1203. [Google Scholar] [CrossRef]
- Sohn, D.; Shpanskaya, K.; Lucas, J.E.; Petrella, J.R.; Saykin, A.J.; Tanzi, R.E.; Samatova, N.F.; Doraiswamy, P.M. Sex Differences in Cognitive Decline in Subjects with High Likelihood of Mild Cognitive Impairment due to Alzheimer’s disease. Sci. Rep. 2018, 8, 7490. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.; Jin, Y.; Lee, I.; Hong, H.; Kim, D.; Park, S.; Kang, H. Physical inactivity and cognitive impairment in Korean older adults: Gender differences in potential covariates. Ann. Hum. Boil. 2017, 44, 729–737. [Google Scholar] [CrossRef]
- Chen, C.; Zissimopoulos, J.M. Racial and ethnic differences in trends in dementia prevalence and risk factors in the United States. Alzheimer’s Dement. (N. Y.) 2018, 4, 510–520. [Google Scholar] [CrossRef]
- Dominguez, J.; Fe de Guzman, M.; Reandelar, M.; Thi Phung, T.K. Prevalence of Dementia and Associated Risk Factors: A Population-Based Study in the Philippines. J. Alzheimer’s Dis. JAD 2018, 63, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.; Wang, F.; Wei, C.; Zhou, A.; Jia, X.; Li, F.; Tang, M.; Chu, L.; Zhou, Y.; Zhou, C.; et al. The prevalence of dementia in urban and rural areas of China. Alzheimer’s Dement. 2014, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Miyawaki, C.E.; Liu, M. Gender differences in cognitive impairment among the old and the oldest-old in China. Geriatr. Gerontol. Int. 2019, 19, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Yang, Y.; Xiao, L.D.; Deng, L.; Wang, Y.; Li, M.; Ullah, S. Nurse-led cognitive screening model for older adults in primary care. Geriatr. Gerontol. Int. 2015, 15, 721–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Liu, J.; Qin, J.; Lan, C.; Yang, H.; Yang, L. Mental Health Status and Coping Behaviors of the Guangxi Baiku Yao Population in Response to Life Events. Med Sci. Monit. 2017, 23, 580–587. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Yaffe, K.; Hoang, T.D.; Byers, A.L.; Barnes, D.E.; Friedl, K.E. Lifestyle and health-related risk factors and risk of cognitive aging among older veterans. Alzheimer’s Dement. J Alzheimer’s Assoc. 2014, 10, S111–S121. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Guan, Y.; Shi, Z.; Yue, W.; Liu, S.; Liu, S.; Lu, H.; Zhao, L.; Zhang, Y.; Su, W.; et al. Sex Differences in the Prevalence of and Risk Factors for Cognitive Impairment No Dementia among the Elderly in a Rural Area of Northern China: A Population-Based Cross-Sectional Study. Neuroepidemiology 2019, 52, 25–31. [Google Scholar] [CrossRef]
- Lobo, A.; Launer, L.J.; Fratiglioni, L.; Andersen, K.; Di Carlo, A.; Breteler, M.M.; Copeland, J.R.; Dartigues, J.F.; Jagger, C.; Martinez-Lage, J.; et al. Prevalence of dementia and major subtypes in Europe: A collaborative study of population-based cohorts. Neurologic Diseases in the Elderly Research Group. Neurology 2000, 54, S4–S9. [Google Scholar] [PubMed]
- Crimmins, E.M.; Saito, Y.; Kim, J.K.; Zhang, Y.S.; Sasson, I.; Hayward, M.D. Educational Differences in the Prevalence of Dementia and Life Expectancy with Dementia: Changes from 2000 to 2010. J. Gerontol. B Psychol. Sci. Soc. Sci. 2018, 73, S20–S28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipnicki, D.M.; Crawford, J.D.; Dutta, R.; Thalamuthu, A.; Kochan, N.A.; Andrews, G.; Lima-Costa, M.F.; Castro-Costa, E.; Brayne, C.; Matthews, F.E.; et al. Age-related cognitive decline and associations with sex, education and apolipoprotein E genotype across ethnocultural groups and geographic regions: A collaborative cohort study. PLoSMed. 2017, 14, e1002261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocca, W.A.; Mielke, M.M.; Vemuri, P.; Miller, V.M. Sex and gender differences in the causes of dementia: A narrative review. Maturitas 2014, 79, 196–201. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Education of the People’s Republic of China. 9-year Compulsory Education. Available online: http://www.china.org.cn/english/education/184879.htm (accessed on 20 May 2020).
- Xinhua. China Improves Compulsory Education in Rural Areas. Available online: http://www.xinhuanet.com/english/2018–08/16/c_137395895.htm (accessed on 20 May 2020).
- Gu, Y.J.; He, C.H.; Li, S.; Zhang, S.Y.; Duan, S.Y.; Sun, H.P.; Shen, Y.P.; Xu, Y.; Yin, J.Y.; Pan, C.W. Tea consumption is associated with cognitive impairment in older Chinese adults. Aging Ment. Health 2018, 22, 1232–1238. [Google Scholar] [CrossRef]
- Kakutani, S.; Watanabe, H.; Murayama, N. Green Tea Intake and Risks for Dementia, Alzheimer’s Disease, Mild Cognitive Impairment, and Cognitive Impairment: A Systematic Review. Nutrients 2019, 11, 1165. [Google Scholar] [CrossRef] [Green Version]
- Feng, L.; Gwee, X.; Kua, E.H.; Ng, T.P. Cognitive function and tea consumption in community dwelling older Chinese in Singapore. J. Nutr. Heal. Aging 2010, 14, 433–438. [Google Scholar] [CrossRef]
- Polito, C.A.; Cai, Z.Y.; Shi, Y.L.; Li, X.M.; Yang, R.; Shi, M.; Li, Q.S.; Ma, S.C.; Xiang, L.P.; Wang, K.R.; et al. Association of Tea Consumption with Risk of Alzheimer’s Disease and Anti-Beta-Amyloid Effects of Tea. Nutrients 2018, 10, 655. [Google Scholar] [CrossRef] [Green Version]
- Loughrey, D.G.; Kelly, M.E.; Kelley, G.A.; Brennan, S.; Lawlor, B.A. Association of Age-Related Hearing Loss With Cognitive Function, Cognitive Impairment, and Dementia: A Systematic Review and Meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 115–126. [Google Scholar] [CrossRef]
- Guthrie, D.M.; Davidson, J.G.S.; Williams, N.; Campos, J.; Hunter, K.; Mick, P.; Orange, J.B.; Pichora-Fuller, M.K.; Phillips, N.A.; Savundranayagam, M.Y.; et al. Combined impairments in vision, hearing and cognition are associated with greater levels of functional and communication difficulties than cognitive impairment alone: Analysis of interRAI data for home care and long-term care recipients in Ontario. PLoS ONE 2018, 13, e0192971. [Google Scholar] [CrossRef]
- Whitson, H.E.; Cronin-Golomb, A.; Cruickshanks, K.J.; Gilmore, G.C.; Owsley, C.; Peelle, J.E.; Recanzone, G.; Sharma, A.; Swenor, B.; Yaffe, K.; et al. American Geriatrics Society and National Institute on Aging Bench-to-Bedside Conference: Sensory Impairment and Cognitive Decline in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 2052–2058. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; Quaranta, N.; Logroscino, G. Sensory Changes and the Hearing Loss-Cognition Link: The Cognitive Ear. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 127–128. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Peters, S.A.; Woodward, M.; Mejia Arango, S.; Batty, G.D.; Beckett, N.; Beiser, A.; Borenstein, A.R.; Crane, P.K.; Haan, M.; et al. Type 2 Diabetes as a Risk Factor for Dementia in Women Compared With Men: A Pooled Analysis of 2.3 Million People Comprising More Than 100,000 Cases of Dementia. Diabetes Care 2016, 39, 300–307. [Google Scholar] [CrossRef] [Green Version]
- Podcasy, J.L.; Epperson, C.N. Considering sex and gender in Alzheimer disease and other dementias. Dialogues Clin.Neurosci. 2016, 18, 437–446. [Google Scholar]
- Lee, K.H.; Jung, E.S.; Choi, Y.Y. Association of oral health and activities of daily living with cognitive impairment. Gerodontology 2020, 37, 38–45. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Male (n = 550), n (%) | Female (n = 700), n (%) | p | |
|---|---|---|---|---|
| Demographics | ||||
| Age (years) | 65~ | 197(35.8) | 236(33.7) | 0.744 |
| 70~ | 175(31.8) | 218(31.1) | ||
| 75~ | 108(19.6) | 153(21.9) | ||
| 80~ | 70(12.7) | 93(13.3) | ||
| Marital status | Married | 444(80.7) | 417(59.6) | 0.000 |
| Divorced/Widowed | 106(19.3) | 283(40.4) | ||
| Education | Illiteracy | 27(4.9) | 108(15.4) | 0.000 |
| Primary school | 222(40.4) | 392(56.0) | ||
| ≥ Secondary school | 301(54.7) | 200(28.6) | ||
| Income | Subsidies § | 219(39.8) | 412(58.9) | 0.000 |
| Poverty | 115(20.9) | 145(20.7) | ||
| Non-poverty | 216(39.3) | 143(20.4) | ||
| Living situation | Alone | 46(8.4) | 93(13.3) | 0.000 |
| With spouse | 243(44.2) | 212(30.3) | ||
| 2 generations | 33(6.0) | 61(8.7) | ||
| ≥3 generations | 228(41.5) | 334(47.7) | ||
| Lifestyle | ||||
| Regular house/farm work | No | 227(41.3) | 137(19.6) | 0.000 |
| Yes | 323(58.7) | 563(80.4) | ||
| Smoking | Never | 290(52.7) | 693(99.0) | 0.000 |
| Ex-smoker | 33(6.0) | 6(0.9) | ||
| Smoker | 227(41.3) | 1(0.1) | ||
| Alcohol consumption | Never | 449(81.6) | 699(99.9) | 0.000 |
| Sometimes | 79(14.4) | 1(0.1) | ||
| Often | 22(4.0) | 0(0.0) | ||
| Tea consumption | No | 386(70.2) | 659(94.1) | 0.000 |
| Yes | 164(29.8) | 41(5.9) | ||
| Psychosocial factors | ||||
| Sleep quality | Good | 391(71.1) | 400(57.1) | 0.000 |
| Moderate | 103(18.7) | 203(29.0) | ||
| Poor | 56(10.2) | 97(13.9) | ||
| Memory complaint | No | 120(21.8) | 96(13.7) | 0.000 |
| Yes | 430(78.2) | 604(86.3) | ||
| Social interactions in | Good | 172(31.3) | 239(34.1) | 0.513 |
| neighborhood | Satisfactory | 361(65.6) | 443(63.3) | |
| Poor | 17(3.1) | 18(2.6) | ||
| Coping | Negative | 50(9.1) | 75(10.7) | 0.342 |
| Positive | 500(90.9) | 625(89.3) | ||
| Characteristics | Male (n = 550), n (%) | Female (n = 700), n (%) | p | |
|---|---|---|---|---|
| BMI (kg/m2) | Underweight | 44 (8.0) | 46 (6.6) | 0.188 |
| Normal | 277 (50.4) | 328 (46.9) | ||
| Overweight | 229 (41.6) | 326 (46.6) | ||
| Waistline (cm) | Normal | 265 (48.2) | 244 (34.9) | 0.000 |
| High | 285 (51.8) | 456 (65.1) | ||
| Hearing | Poor | 171 (31.1) | 223 (31.9) | 0.780 |
| Moderate | 219 (39.8) | 286 (40.9) | ||
| Good | 160 (29.1) | 191 (27.3) | ||
| Vision | Normal | 510 (92.7) | 635 (90.7) | 0.203 |
| Weak | 40 (7.3) | 65 (9.3) | ||
| Chronic disease | 0 | 151 (27.5) | 139 (19.9) | 0.005 |
| 1 | 204 (37.1) | 260 (37.1) | ||
| 2 | 130 (23.6) | 188 (26.9) | ||
| ≥3 | 65 (11.8) | 113 (16.1) | ||
| Hypertension | No | 302 (54.9) | 335 (47.9) | 0.013 |
| Yes | 248 (45.1) | 365 (52.1) | ||
| Diabetes | No | 516 (93.8) | 629 (89.9) | 0.012 |
| Yes | 34 (6.2) | 71 (10.1) | ||
| Cerebrovascular disease | No | 501 (91.1) | 655 (93.6) | 0.099 |
| Yes | 49 (8.9) | 45 (6.4) | ||
| Heart disease | No | 407 (74.0) | 516 (73.7) | 0.909 |
| Yes | 143 (26.0) | 184 (26.3) | ||
| Hyperlipidemia | No | 522 (94.9) | 588 (84.0) | 0.000 |
| Yes | 28 (5.1) | 112 (16.0) | ||
| Renal disease | No | 521 (94.7) | 682 (97.4) | 0.013 |
| Yes | 29 (5.3) | 18 (2.6) | ||
| Traumatic brain injury | No | 496 (90.2) | 657 (93.9) | 0.016 |
| Yes | 54 (9.8) | 43 (6.1) | ||
| ADL dependence | No | 515 (93.6) | 646 (92.3) | 0.357 |
| Yes | 35 (6.4) | 54 (7.7) | ||
| Physical ADL dependence | No | 304 (55.3) | 241 (34.4) | 0.000 |
| Yes | 246 (44.7) | 459 (65.6) | ||
| IADL dependence | No | 392 (71.3) | 449 (64.1) | 0.008 |
| Yes | 158 (28.7) | 251 (35.9) | ||
| Subgroup | Male (n = 550) | Female (n = 700) | p | ||
|---|---|---|---|---|---|
| Individuals, N | Cases, n (%) | Individuals, N | Cases, n (%) | ||
| Overall | 550 | 220 (40.0) | 700 | 316 (45.1) | 0.068 |
| Age(years) | |||||
| 65~ | 197 | 70 (35.5) | 236 | 70 (29.7) | 0.193 |
| 70~ | 175 | 61 (34.9) | 218 | 84 (38.5) | 0.453 |
| 75~ | 108 | 49 (45.4) | 153 | 96 (62.7) | 0.005 |
| 80~ | 70 | 40 (57.1) | 93 | 66 (71.0) | 0.067 |
| Education | |||||
| Illiteracy | 27 | 13 (48.1) | 108 | 80 (74.1) | 0.009 |
| Primary school | 222 | 66 (29.7) | 392 | 139 (35.5) | 0.148 |
| ≥Secondary school | 301 | 141 (46.8) | 200 | 97 (48.5) | 0.716 |
| Marital status | |||||
| Married | 444 | 171 (38.5) | 417 | 160 (38.4) | 0.965 |
| Divorced/Widowed | 106 | 49 (46.2) | 283 | 156 (55.1) | 0.118 |
| Income | |||||
| Subsidies § | 219 | 100 (45.7) | 412 | 209 (50.7) | 0.226 |
| Poverty | 115 | 39 (33.9) | 145 | 51 (35.2) | 0.832 |
| Non-poverty | 216 | 81 (37.5) | 143 | 56 (39.2) | 0.751 |
| Living alone | |||||
| Yes | 46 | 19 (41.3) | 93 | 51 (54.8) | 0.133 |
| No | 504 | 201 (39.9) | 607 | 265 (43.7) | 0.204 |
| Variables | Male (n = 550) | Female (n = 700) | |||
|---|---|---|---|---|---|
| Prevalence (95%CI) | OR (95%CI) | Prevalence (95%CI) | OR (95%CI) | ||
| Total | 40.0 (35.9–44.1) | - | 45.1 (41.4–48.8) | - | |
| Age (years) | 65~ (ref.) | 35.5 (28.8–42.3) | 29.7 (23.8–35.5) | ||
| 70~ | 34.9 (27.7–42.0) | 0.971 (0.634–1.487) | 38.5 (32.0–45.0) | 1.487 (1.006–2.197) | |
| 75~ | 45.4 (35.8–54.9) | 1.507 (0.934–2.431) | 62.7 (55.0–70.5) | 3.994 (2.597–6.144) | |
| 80~ | 57.1 (45.3–60.0) | 2.419 (1.387–4.218) | 71.0 (61.6–80.4) | 5.797 (3.420–9.826) | |
| Marital status | Married (ref.) | 38.5 (34.0–43.1) | 38.4 (33.7–43.1) | ||
| Divorced/Widowed | 46.2 (36.6–55.9) | 1.372 (0.895–2.103) | 55.1 (49.3–61.0) | 1.973 (1.452–2.680) | |
| Education | Illiteracy (ref.) | 48.1 (28.0–68.3) | 74.1 (65.7–82.5) | ||
| Primary school | 29.7 (23.7–35.8) | 0.456 (0.203–1.022) | 35.5 (30.7–40.2) | 0.192 (0.119–0.310) | |
| ≥ Secondary school | 46.8 (41.2–52.5) | 0.949 (0.432–2.087) | 48.5 (41.5–55.5) | 0.330 (0.198–0.550) | |
| Income | Subsidies§(ref.) | 45.7 (39.0–52.3) | 50.7 (45.9–55.6) | ||
| Poverty | 33.9 (25.1–42.7) | 0.611 (0.382–0.976) | 35.2 (27.3–43.0) | 0.527 (0.356–0.780) | |
| Non-poverty | 37.5 (31.0–44.0) | 0.714 (0.487–1.047) | 39.2 (31.1–47.3) | 0.625 (0.424–0.921) | |
| Regular house/farm work | No (ref.) | 48.0 (41.5–54.6) | 63.5 (55.3–71.7) | ||
| Yes | 34.4 (29.2–39.6) | 0.567 (0.401–0.802) | 40.7 (36.6–44.7) | 0.394 (0.268–0.580) | |
| Smoking | Never (ref.) | 42.8 (37.0–48.5) | 45.0 (41.3–48.7) | ||
| Ex-smoker | 42.4 (24.6–60.2) | 0.986 (0.476–2.044) | 66.7 (12.5–120.9) | 2.442 (0.444–13.422) | |
| Smoker | 36.1 (29.8–42.4) | 0.757 (0.530–1.082) | 0.0 | 0.000 | |
| Alcohol consumption | Never (ref.) | 42.8 (38.2–47.4) | 45.2 (41.5–48.9) | ||
| Sometimes | 27.8 (17.7–38.0) | 0.517 (0.305–0.874) | 0.0 | 0.000 | |
| Often | 27.3 (7.1–47.5) | 0.502 (0.193–1.307) | - | - | |
| Tea consumption | No (ref.) | 43.3 (38.3–48.2) | 45.4 (41.6–49.2) | ||
| Yes | 32.3 (25.1–39.6) | 0.626 (0.426–0.919) | 41.5 (25.7–57.2) | 0.853 (0.450–1.617) | |
| Sleep quality | Good (ref.) | 39.6 (34.8–44.5) | 42.3 (37.4–47.1) | ||
| Moderate | 41.7 (32.1–51.4) | 1.091 (0.702–1.696) | 50.7 (43.8–57.7) | 1.408 (1.003–1.976) | |
| Poor | 39.3 (26.1–52.5) | 0.985 (0.555–1.748) | 45.4 (35.3–55.4) | 1.135 (0.726–1.773) | |
| Memory complaint | No (ref.) | 35.8 (27.1–44.5) | 29.2 (19.9–38.4) | ||
| Yes | 41.2 (36.5–45.8) | 1.253 (0.823–1.906) | 47.7 (43.7–51.7) | 2.213 (1.386–3.535) | |
| Living situation | Alone (ref.) | 41.3 (26.5–56.1) | 54.8 (44.5–65.1) | ||
| With spouse | 37.9 (31.7–44.0) | 0.866 (0.456–1.645) | 38.2 (31.6–44.8) | 0.509 (0.311–0.834) | |
| 2 generations | 24.2 (8.8–39.7) | 0.455 (0.169–1.223) | 44.3 (31.4–57.1) | 0.654 (0.342–1.252) | |
| ≥3 generations | 44.3 (37.8–50.8) | 1.130 (0.594–2.149) | 47.0 (41.6–52.4) | 0.730 (0.460–1.159) | |
| Social interactions in neighborhood | Good (ref.) | 40.1 (32.7–47.5) | 43.9 (37.6–50.3) | ||
| Satisfactory | 38.2 (33.2–43.3) | 0.924 (0.637–1.339) | 45.6 (40.9–50.3) | 1.070 (0.779–1.468) | |
| Poor | 76.5 (54.0–99.0) | 4.851 (1.519–15.497) | 50.0 (24.4–75.6) | 1.276 (0.489–3.328) | |
| Coping | Negative (ref.) | 48.0 (33.7–62.3) | 58.7 (47.3–70.1) | ||
| Positive | 39.2 (34.9–43.5) | 0.698 (0.390–1.251) | 43.5 (39.6–47.4) | 0.543 (0.334–0.883) | |
| Variables | Male (n = 550) | Female (n = 700) | |||
|---|---|---|---|---|---|
| Prevalence (95%CI) | OR (95%CI) | Prevalence (95%CI) | OR (95%CI) | ||
| BMI (kg/m2) | Underweight | 50.0 (34.6–65.4) | 60.9 (46.2–75.5) | ||
| Normal | 40.1 (34.3–45.9) | 0.669 (0.353–1.266) | 45.7 (40.3–51.2) | 0.542 (0.288–1.018) | |
| Overweight | 38.0 (31.7–44.3) | 0.613 (0.320–1.172) | 42.3 (36.9–47.7) | 0.472 (0.251–0.887) | |
| Waistline (cm) | Normal | 40.8 (34.8–46.7) | 46.3 (40.0–52.6) | ||
| High | 39.3 (33.6–45.0) | 0.941 (0.669–1.324) | 44.5 (39.9–49.1) | 0.930 (0.681–1.271) | |
| Hearing | Poor (ref.) | 36.3 (28.7–43.8) | 34.6 (27.7–41.4) | ||
| Moderate | 31.5 (25.3–37.7) | 0.477 (0.307–0.741) | 38.8 (33.1–44.5) | 0.319 (0.213–0.477) | |
| Good | 54.4 (46.8–61.9) | 0.386 (0.255–0.584) | 62.3 (55.9–68.7) | 0.383 (0.267–0.550) | |
| Vision | Normal | 38.4 (34.2–42.7) | 42.2 (38.4–46.1) | ||
| Weak | 60.0 (44.1–75.9) | 2.403 (1.245–4.637) | 73.8 (62.9–84.8) | 3.867 (2.175–6.872) | |
| Chronic disease | 0 (ref.) | 35.1 (27.4–42.8) | 36.0 (27.9–44.0) | ||
| 1 | 40.7 (33.9–47.5) | 1.268 (0.821–1.961) | 48.1 (42.0–54.2) | 1.648 (1.079–2.517) | |
| 2 | 39.2 (30.7–47.7) | 1.194 (0.735–1.940) | 47.3 (40.1–54.5) | 1.600 (1.021–2.508) | |
| ≥ 3 | 50.8 (38.3–63.3) | 1.907 (1.057–3.440) | 46.0 (36.7–55.3) | 1.517 (0.914–2.519) | |
| Hypertension | No (ref.) | 39.4 (33.9–44.9) | 41.8 (36.5–47.1) | ||
| Yes | 40.7 (34.6–46.9) | 1.057 (0.750–1.488) | 48.2 (43.1–53.4) | 1.297 (0.962–1.749) | |
| Diabetes | No (ref.) | 39.0 (34.7–43.2) | 44.7 (40.8–48.6) | ||
| Yes | 55.9 (38.3–73.5) | 1.985 (0.986–3.996) | 49.3 (37.4–61.2) | 1.204 (0.737–1.968) | |
| Cerebrovascular disease | No (ref.) | 38.9 (34.6–43.2) | 44.6 (40.8–48.4) | ||
| Yes | 51.0 (36.5–65.5) | 1.635 (0.908–2.944) | 53.3 (38.2–68.5) | 1.421 (0.775–2.603) | |
| Heart disease | No (ref.) | 39.6 (34.8–44.3) | 43.8 (39.5–48.1) | ||
| Yes | 41.3 (33.1–49.4) | 1.073 (0.728–1.581) | 48.9 (41.6–56.2) | 1.229 (0.877–1.721) | |
| Hyperlipidemia | No (ref.) | 40.0 (35.8–44.3) | 46.3 (42.2–50.3) | ||
| Yes | 39.3 (20.0–58.6) | 0.969 (0.445–2.110) | 39.3 (30.1–48.5) | 0.752 (0.498–1.135) | |
| Renal disease | No (ref.) | 39.9 (35.7–44.1) | 44.7 (41.0–48.5) | ||
| Yes | 41.4 (22.3–60.4) | 1.062 (0.497–2.270) | 61.1 (36.2–86.1) | 1.942 (0.744–5.071) | |
| Traumatic brain injury | No (ref.) | 38.7 (34.4–43.0) | 44.4 (40.6–48.3) | ||
| Yes | 51.9 (38.1–65.6) | 1.705 (0.971–2.996) | 55.8 (40.3–71.3) | 1.579 (0.848–2.939) | |
| ADL dependence | No (ref.) | 38.1 (33.9–42.3) | 42.7 (38.9–46.5) | ||
| Yes | 68.6 (52.4–84.8) | 3.551 (1.702–7.409) | 74.1 (62.0–86.1) | 3.830 (2.043–7.179) | |
| Physical ADL dependence | No (ref.) | 34.5 (29.2–39.9) | 33.2 (27.2–39.2) | ||
| Yes | 46.7 (40.5–53.0) | 1.664 (1.179–2.348) | 51.4 (46.8–56.0) | 2.130 (1.539–2.947) | |
| IADL dependence | No (ref.) | 35.7 (31.0–40.5) | 39.4 (34.9–44.0) | ||
| Yes | 50.6 (42.8–58.5) | 1.846 (1.270–2.684) | 55.4 (49.2–61.6) | 1.907 (1.395–2.607) | |
| Variables | Male (n-550) | Female (n = 700) | |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | ||
| Age (years) | 65~(ref.) | ||
| 70~ | 0.894 (0.559–1.430) | 1.133 (0.739–1.736) | |
| 75~ | 1.179 (0.690–2.014) | 2.793 (1.729–4.511) | |
| 80~ | 2.357 (1.255–4.428) | 2.070 (1.061–4.036) | |
| Education | Illiteracy (ref.) | ||
| Primary school | 0.754 (0.304–1.866) | 0.352 (0.199–0.623) | |
| ≥ Secondary school | 2.156 (0.868–5.355) | 0.851 (0.454–1.597) | |
| Tea consumption | No (ref.) | - | |
| Yes | 0.656 (0.431–0.999) | ||
| Social interactions in neighborhood | Good (ref.) | - | |
| Satisfactory | 0.942 (0.625–1.422) | ||
| Poor | 4.860 (1.424–16.583) | ||
| Hearing | Good (ref.) | ||
| Moderate | 0.830 (0.516–1.334) | 0.903 (0.589–1.382) | |
| Poor | 2.027 (1.211–3.393) | 2.110 (1.321–3.369) | |
| Vision | Normal (ref.) | - | |
| Weak | 2.024 (1.051–3.897) | ||
| Diabetes | No (ref.) | ||
| Yes | 2.344 (1.083–5.076) | - | |
| ADL dependence | No (ref.) | ||
| Yes | 3.267 (1.459–7.314) | 2.041 (0.976–4.270) | |
| Physical ADL dependence | No (ref.) | - | |
| Yes | 1.613 (1.121–2.322) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Xiao, L.D.; Wang, K.; Luo, Y.; Li, X. Gender Differences in Cognitive Impairment among Rural Elderly in China. Int. J. Environ. Res. Public Health 2020, 17, 3724. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103724
Wang J, Xiao LD, Wang K, Luo Y, Li X. Gender Differences in Cognitive Impairment among Rural Elderly in China. International Journal of Environmental Research and Public Health. 2020; 17(10):3724. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103724
Chicago/Turabian StyleWang, Jing, Lily Dongxia Xiao, Kai Wang, Yan Luo, and Xiaomei Li. 2020. "Gender Differences in Cognitive Impairment among Rural Elderly in China" International Journal of Environmental Research and Public Health 17, no. 10: 3724. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103724