Model for Taking Care of Patients with Early Childhood Caries during the SARS-Cov-2 Pandemic



Abstract
:1. Introduction
1.1. The SARS-CoV-2 Pandemic and Its Social Consequences
1.2. Peculiarities of the SARS-CoV-2 Infection in Children
1.3. Transmission of SARS-CoV-2
1.4. Urgent and Emergency Dental Interventions
1.5. Early Childhood Caries (ECC)
2. Methods
2.1. Study Design
2.2. Studies Selection and Data Extraction
2.3. Inclusion and Exclusion Criteria
2.4. Outcomes
2.5. Statistical Analysis
2.6. Results Section Structuration
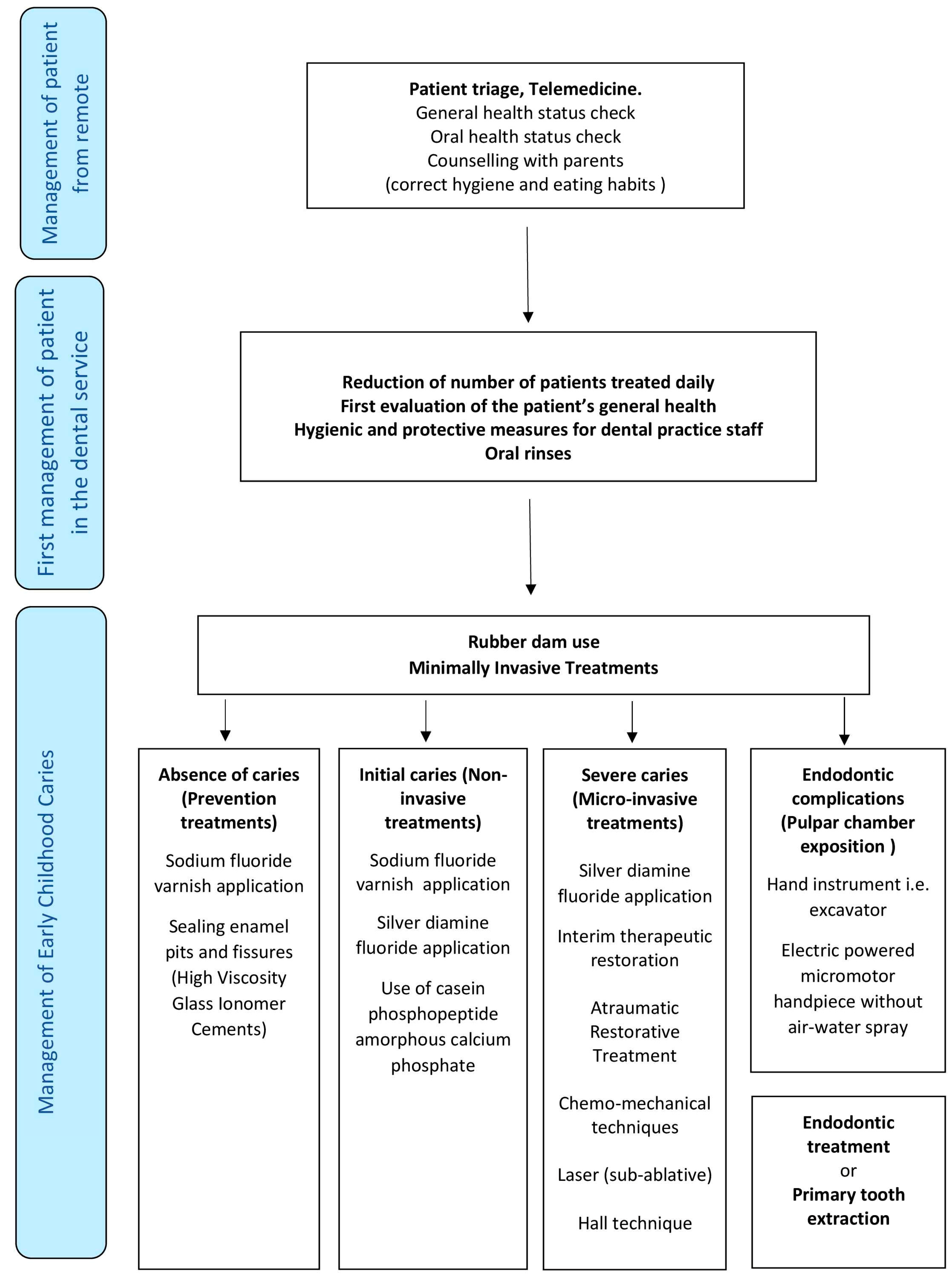
3. Results (Protocol for ECC Management during the SARS-CoV-2 Pandemic)
3.1. “General Safety Criteria” for Avoiding SARS-CoV-2 Contamination from Saliva Droplets
3.1.1. Reduction of Number of Patients Treated Daily
3.1.2. First Evaluation of the Patient’s General Health
3.1.3. Hygienic and Protective Measures for Dental Practice Staff
3.1.4. Work Surface Management
3.1.5. Oral Rinses
3.1.6. Rubber Dam Use
3.1.7. High Speed Drills
3.2. “Specific Safety Criteria” for Avoiding SARS-CoV-2 Contamination From the Use of Air-Water Sprays
3.2.1. Minimally Invasive Treatments (MITs)
3.2.2. Classification of Minimally Invasive Treatments (MITs)
3.2.3. Non-Invasive Treatments
Use of Fluoride Varnishes
Use of Silver Diamine Fluoride (SDF)
Use of Casein Phosphopeptide—Amorphous Calcium Phosphate (CPP-ACP) Products
Use of High Viscosity Glass Ionomer Cements (HVGIC) in the Prevention of Carious Lesions
3.2.4. Micro-Invasive Treatments
Interim Therapeutic Restoration (ITR)
Atraumatic Restorative Treatment (ART)
Chemo-Mechanical Techniques
Use of Sub-Ablative Energy Lasers
Use of Preformed Crown (Hall Technique)
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sohrabi, C.; Alsafi, Z.; O’Neil, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Lewnard, J.A.; Lo, N.C. Scientific and ethical basis for social- distancing interventions against COVID-19. Lancet Infect. Dis. 2020, 23. [Google Scholar] [CrossRef] [Green Version]
- Koo, J.R.; Cookm, A.R.; Park, M.; Sun, H.; Lim, J.T.; Tam, C.; Dickens, B.L. Interventions to mitigate early spread of SARS-CoV-2 in Singapore: A modelling study. Lancet. Infect. Dis. 2020, 23. [Google Scholar] [CrossRef] [Green Version]
- Riley, P.; Worthington, H.V.; Clarkson, J.E.; Beirne, P.V. Recall intervals for oral health in primary care patients. Cochrane Database Syst. Rev. 2013, 19, CD004346. [Google Scholar] [CrossRef]
- Dondi, A.; Piccinno, V.; Morigi, F.; Sureshkumar, S.; Gori, D.; Lanari, M. Food Insecurity and Major Diet-Related Morbidities in Migrating Children: A Systematic Review. Nutrients 2020, 31, E379. [Google Scholar] [CrossRef] [Green Version]
- Cianetti, S.; Lombardo, G.; Lupatelli, E.; Rossi, G.; Abraha, I.; Pagano, S.; Paglia, L. Dental caries, parents educational level, family income and dental service attendance among children in Italy. Eur. J. Paediatr. Dent. 2017, 18, 15–18. [Google Scholar]
- Nielsen, F. Inequality and inequity. Soc. Sci. Res. 2017, 62, 29–35. [Google Scholar] [CrossRef]
- Singhal, T. A Review of Coronavirus Disease-2019 (COVID-19). IndianJ. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Tu, M.; Wang, S.; Chen, S.; Zhou, L.; Wang, M.; Zhao, Y.; Zeng, W.; Huang, Q.; Xu, H.; et al. Clinical characteristics of laboratory confirmed positive cases of SARS-CoV-2 infection in Wuhan, China: A retrospective single center analysis. Travel. Med. Infect. Dis. 2020, 101606. [Google Scholar] [CrossRef]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, Z. Epidemiological Characteristics of 2143 Pediatric Patients with 2019 Coronavirus Disease in China. Pediatrics 2020, 16, e20200702. [Google Scholar] [CrossRef] [Green Version]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral. Sci. 2020, 12, 9. [Google Scholar] [CrossRef]
- Bagga, B.S.; Murphy, R.A.; Anderson, A.W.; Punwani, I. Contamination of dental unit cooling water with oral microorganisms and its prevention. J. Am. Dent. Assoc. 1984, 109, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pung, R.; Chiw, C.J.; Young, B.E.; Chin, S.; Chen, M.I.; Clapham, H.E.; Cook, A.R.; Maurer-Stroh, S.; Toh, M.P.H.S.; Poh, C.; et al. Singapore 2019 Novel Coronavirus Outbreak Research Team. Investigation of three clusters of COVID-19 in Singapore: Implications for surveillance and response measures. Lancet 2020, 395, 1039–1046. [Google Scholar] [CrossRef]
- Lai, T.H.T.; Tang, E.W.H.; Fung, K.S.C.; Li, K.K.W. Reply to “Does hand hygiene reduceSARS-CoV-2 transmission?”. Graefes. Arch. Clin. Exp. Ophthalmol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Volgenant, C.M.C.; de Soet, J.J. Cross-transmission in the Dental Office: Does This Make You Ill? Curr. Oral. Health Rep. 2018, 5, 221–228. [Google Scholar] [CrossRef] [Green Version]
- Seto, W.H.; Tsang, D.; Yung, R.W.; Ching, T.Y.; Ng, T.K.; Ho, L.M.; Peiris, J.S. Effectiveness of precautions against droplets and contact in prevention of nosocomial transmission of severe acute respiratory syndrome (SARS). Lancet 2003, 36, 1519–1520. [Google Scholar] [CrossRef] [Green Version]
- Peres, M.A.; Daly, B.; Guarnizo-Herreno, C.C.; Benzian, H.; Watt, R.G. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Kagihara, L.E.; Niederhauser, V.P.; Stark, M. Assessment, management, and prevention of early childhood caries. J. Am. Acad. Nurse Pr. 2009, 21, 1–10. [Google Scholar] [CrossRef]
- Mansoori, S.; Mehta, A.; Ansari, M.I. Factors associated with Oral Health Related Quality of Life of children with severe-Early Childhood Caries. J. Oral. Biol. Craniofac. Res. 2019, 9, 222–225. [Google Scholar] [CrossRef]
- Sheikhtaheri, A.; Kermani, F. Telemedicine in Diagnosis, Treatment and Management of Diseases in Children. Stud. Health Technol. Inf. 2018, 248, 148–155. [Google Scholar]
- Neville, P.; van der Zande, M.M. Dentistry, e-health and digitalisation: A critical narrative review of the dental literature on digital technologies with insights from health and technology studies. Community Dent. Health 2020, 37, 51–58. [Google Scholar] [PubMed]
- Riggs, E.; Kilpatrick, N.; Slack-Smith, L.; Chadwick, B.; Yelland, J.; Muthu, M.S.; Gomersall, J.C. Interventions with pregnant women, new mothers and other primary caregivers for preventing early childhood caries. Cochrane Database Syst. Rev. 2019, 11, 14651858. [Google Scholar] [CrossRef] [PubMed]
- de Silva, A.M. WITHDRAWN: Community-based population-level interventions for promoting child oral health. Cochrane Database Syst. Rev. 2016, 12, CD009837. [Google Scholar]
- Fung, I.C.; Cairncross, S. How often do you wash your hands? A review of studies of hand-washing practices in the community during and after the SARS outbreak in 2003. Int. J. Environ. Health Res. 2007, 17, 161–183. [Google Scholar] [CrossRef]
- Verbeek, J.H.; Rajamaki, B.; Ijaz, S.; Tikka, C.; Ruotsalainen, J.H.; Edmond, M.B.; Sauni, R.; Kilinc Balci, F.S. Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff. Cochrane Database Syst. Rev. 2019, 7, CD01162. [Google Scholar] [CrossRef]
- Carrouel, F.; Viennot, S.; Ottolenghi, L.; Gaillard, C.; Bourgeois, D. Nanoparticles as Anti-Microbial, Anti-Inflammatory, and Remineralizing Agents in Oral Care Cosmetics: A Review of the Current Situation. Nanomater. Nanomater. (Basel) 2020, 10, 140. [Google Scholar] [CrossRef] [Green Version]
- Carrouel, F.; Conte, M.P.; Fisher, J.; Gonçalves, L.S.; Dussart, C.; Llodra, J.C.; Bourgeois, D. COVID-19: A Recommendation to Examine the Effect of Mouthrinses with β-Cyclodextrin Combined with Citrox in Preventing Infection and Progression. J. Clin. Med. 2020, 9, E1126. [Google Scholar] [CrossRef] [Green Version]
- Shulman, J.D.; Wells, L.M. Acute ethanol toxicity from ingesting mouthwash in children younger than 6-years of age. Pediatr. Dent 1997, 19, 404–408. [Google Scholar]
- Hitz Lindenmüller, I.; Lambrecht, J.T. Oral care. Curr. Probl. Derm. 2011, 40, 107–115. [Google Scholar]
- Yhim, H.B.; Yoon, S.H.; Jang, Y.E.; Lee, J.H.; Kim, E.H.; Kim, J.T.; Kim, H.S. Effects ofbenzydamine hydrochloride on postoperative sore throat after extubation in children: A randomized controlled trial. BMC Anesth. 2020, 20, 77. [Google Scholar] [CrossRef] [PubMed]
- Samaranayake, L.P.; Reid, J.; Evans, D. The efficacy of rubber dam isolation in reducing atmospheric bacterial contamination. Asdc J. Dent. Child. 1989, 56, 442–444. [Google Scholar] [PubMed]
- Montedori, A.; Abraha, I.; Orso, M.; D’Errico, P.G.; Pagano, S.; Lombardo, G. Lasers for caries removal in deciduous and permanent teeth. Cochrane Database Syst. Rev. 2016, 9, CD010229. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, G.; Pagano, S.; Cianetti, S.; Capobianco, B.; Orso, M.; Negri, P.; Paglia, M.; Friuli, S.; Paglia, L.; Gatto, R.; et al. Sub-ablative laser irradiation to prevent acid demineralisation of dental enamel. A systematic review of literature reporting in vitro studies. Eur. J. Paediatr. Dent. 2019, 20, 295–301. [Google Scholar] [PubMed]
- Corrêa-Faria, P.; Viana, K.A.; Raggio, D.P.; Hosey, M.T.; Costa, L.R. Recommended procedures for the management of early childhood caries lesions—A scoping review by the Children Experiencing Dental Anxiety: Collaboration on Research and Education (CEDACORE). BMC Oral. Health 2020, 20, 75. [Google Scholar] [CrossRef]
- Duangthip, D.; Chen, K.J.; Gao, S.S.; Lo, E.C.M.; Chu, C.H. Managing Early Childhood Caries with Atraumatic Restorative Treatment and Topical Silver and Fluoride Agents. Int. J. Environ. Res. Public Health 2017, 14, E1204. [Google Scholar] [CrossRef] [Green Version]
- Frencken, J.E. Atraumatic restorative treatment and minimal intervention dentistry. Br. Dent. J. 2017, 223, 183–189. [Google Scholar] [CrossRef]
- Molina, G.F.; Faulks, D.; Frencken, J. Acceptability, feasibility and perceived satisfaction of the use of the Atraumatic Restorative Treatment approach for people with disability. Braz. Oral. Res. 2015, 29. [Google Scholar] [CrossRef] [Green Version]
- Marinho, V.C.; Worthington, H.V.; Walsh, T.; Clarkson, J.E. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst. Rev. 2013, 7, CD002279. [Google Scholar] [CrossRef]
- Gao, S.S.; Zhang, S.; Mei, M.L.; Lo, E.C.; Chu, C.H. Caries remineralisation and arresting effect in children by professionally applied fluoride treatment—a systematic review. BMC Oral. Health 2016, 16, 12. [Google Scholar] [CrossRef] [Green Version]
- Schmoeckel, J.; Gorseta, K.; Splieth, C.H.; Juric, H. How to Intervene in the Caries Process: Early Childhood Caries—A Systematic Review. Caries Res. 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.S.; Zhao, I.S.; Duffin, S.; Duangthip, D.; Lo, E.C.M.; Chu, C.H. Revitalising Silver Nitrate for Caries Management. Int. J. Environ. Res. Public Health 2018, 15, E80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, I.S.; Gao, S.S.; Hiraishi, N.; Burrow, M.F.; Duangthip, D.; Mei, M.L.; Lo, E.C.; Chu, C.H. Mechanisms of silver diamine fluoride on arresting caries: A literature review. Int. Dent. J. 2018, 68, 67–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, X.; Lin, X.; Zhong, T.; Xie, F. Evaluation of the efficacy of casein phosphopeptide-amorphous calcium phosphate on remineralization of white spot lesions in vitro and clinical research: A systematic review and meta-analysis. BMC Oral. Health 2019, 19, 295. [Google Scholar] [CrossRef] [Green Version]
- Tao, S.; Zhu, Y.; Yuan, H.; Tao, S.; Cheng, Y.; Li, J.; He, L. Efficacy of fluorides and CPP-ACP vs fluorides monotherapy on early caries lesions: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0196660. [Google Scholar] [CrossRef] [Green Version]
- Mickenautsch, S.; Yengopal, V. Caries-Preventive Effect of High-Viscosity Glass Ionomer and Resin-Based Fissure Sealants on Permanent Teeth: A Systematic Review of Clinical Trials. PLoS ONE 2016, 11, e0146512. [Google Scholar] [CrossRef]
- Ahovuo-Saloranta, A.; Forss, H.; Walsh, T.; Nordblad, A.; Makela, M.; Worthington, H.V. Pit and fissure sealants for preventing dental decay in permanent teeth. Cochrane Database Syst. Rev. 2017, 7, CD001830. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.N.; Kiang, L.; Manohara, R.; Tong, H.J.; Nair, R.; Hong, C.; Hu, S. Interim therapeutic restoration approach versus treatment under general anaesthesia approach. Int. J. Paediatr. Dent. 2017, 27, 551–555. [Google Scholar] [CrossRef]
- Dorri, M.; Martinez-Zapata, M.J.; Walsh, T.; Marinho, V.C.; Sheiham Deceased, A.; Zaror, C. Atraumatic restorative treatment versus conventional restorative treatment for managing dental caries. Cochrane Database Syst. Rev. 2017, 12, CD008072. [Google Scholar] [CrossRef] [Green Version]
- Phonghanyudh, A.; Phantumvanit, P.; Songpaisan, Y.; Petersen, P.E. Clinical evaluation of three caries removal approaches in primary teeth: A randomised controlled trial. Community Dent. Health 2012, 29, 173–178. [Google Scholar]
- Chieruzzi, M.; Pagano, S.; Lombardo, G.; Cianetti, S. Effect of nanohydroxyapatite, antibiotic, and mucosal defensive agent on the mechanical and thermal properties of glass ionomer cements for special needs patients. J. Mater. Res. 2018, 33, 638–649. [Google Scholar] [CrossRef]
- Maragakis, G.M.; Hahn, P.; Hellwig, E. Chemomechanical caries removal: A comprehensive review of the literature. Int. Dent. J. 2001, 51, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Lai, G.; Lara Capi, C.; Cocco, F.; Cagetti, M.G.; Lingstrom, P.; Almhojd, U.; Campus, G. Comparison of Carisolv system vs traditional rotating instruments for cariesremoval in the primary dentition: A systematic review and meta-analysis. Acta Odontol. Scand. 2015, 73, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Steiner-Oliveira, C.; Longo, P.L.; Aranha, A.C.; Ramalho, K.M.; Mayer, M.P.; de Paula Eduardo, C. Randomized in vivo evaluation of photodynamic antimicrobialchemotherapy on deciduous carious dentin. J. Biomed. Opt. 2015, 20, 108003. [Google Scholar] [CrossRef] [Green Version]
- Innes, N.P.; Ricketts, D.; Ching, L.Y.; Keightley, A.J.; Lamont, T.; Santamaria, R.M. Preformed crowns for decayed primary molar teeth. Cochrane Database Syst. Rev. 2015, 12, CD005512. [Google Scholar] [CrossRef]
- Law, C.S. Management of premature primary tooth loss in the child patient. J. Calif. Dent. Assoc. 2013, 41, 612–618. [Google Scholar]
- Mathus-Vliegen, E.M.; Nikkel, D.; Brand, H.S. Oral aspects of obesity. Int. Dent. J. 2007, 57, 249–256. [Google Scholar] [CrossRef]
- Anthonappa, R.P.; Ashley, P.F.; Bonetti, D.L.; Lombardo, G.; Riley, P. Non-pharmacological interventions for managing dental anxiety in children. Cochrane Database Syst. Rev. 2017, 6, CD012676. [Google Scholar] [CrossRef] [Green Version]
- Alharbi, A.; Alharbi, S.; Alqaidi, S. Guidelines for dental care provision during the COVID-19 pandemic. Saudi Dent. J. 2020, 32, 181–186. [Google Scholar] [CrossRef]
- Spagnuolo, G.; De Vito, D.; Rengo, S.; Tatullo, M. COVID-19 Outbreak: An Overview on Dentistry. Int. J. Environ. Res. Public Health. 2020, 17, E2094. [Google Scholar] [CrossRef] [Green Version]
- Abramovitz, I.; Palmon, A.; Levy, D.; Karabucak, B.; Kot-Limon, N.; Shay, B.; Kolokythas, A.; Almoznino, G. Dental care during the coronavirus disease 2019 (COVID-19) outbreak: Operatory considerations and clinical aspects. Quintessence Int. 2020, 51, 418–429. [Google Scholar] [PubMed]
- 62. French Society of Stomatology, Maxillo-Facial Surgery and Oral Surgery (SFSCMFCO). Practitioners specialized in oral health and coronavirus disease 2019: Professional guidelines from the French society of stomatology, maxillofacial surgery and oral surgery, to form a common front against the infectious risk. J. Stomatol Oral. Maxillofac Surg. 2020, 121, 155–158.
- Prati, C.; Pelliccioni, G.A.; Sambri, V.; Chersoni, S.; Gandolfi, M.G. COVID-19: Its impact on dental schools in taly, clinical problems in endodontic therapy and general considerations. Int. Endod. J. 2020, 53, 723–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verbeek, J.H.; Rajamaki, B.; Ijaz, S.; Sauni, R.; Toomey, E.; Blackwood, B.; Tikka, C.; Ruotsalainen, J.H.; Kilinc Balci, F.S. Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff. Cochrane Database Syst. Rev. 2020, 15, CD011621. [Google Scholar]
- Maret, D.; Peters, O.A.; Vaysse, F.; Vigarios, E. Integration of telemedicine into the public health response to COVID-19 must include dentists. Int. Endod. J. 2020. [Google Scholar] [CrossRef]
- Machado, R.A.; de Souza, N.L.; Oliveira, R.M.; Martelli Júnior, H.; Bonan, P.R.F. Social media and telemedicine for oral diagnosis and counselling in the COVID-19 era. Oral. Oncol. 2020. [Google Scholar] [CrossRef]
- Caprioglio, A.; Pizzetti, G.B.; Zecca, P.A.; Fastuca, R.; Maino, G.; Nanda, R. Management of orthodontic emergencies during 2019-NCOV. Prog. Orthod. 2020, 21, 10. [Google Scholar] [CrossRef] [Green Version]
- Guo, J.; Xie, H.; Liang, M.; Wu, H. COVID-19: A novel coronavirus and a novel challenge for oral healthcare. Clin. Oral. Investig. 2020. [Google Scholar] [CrossRef]
- Li, Y.; Ren, B.; Peng, X.; Hu, T.; Li, J.; Gong, T.; Tang, B.; Xu, X.; Zhou, X. Saliva is a non-negligible factor in the spread of COVID-19. Mol. Oral. Microbiol. 2020. [Google Scholar] [CrossRef]
- Casamassimo, P.S.; Townsend, J.A.; Litch, C.S. Pediatric Dentistry During and After COVID-19. Pediatr. Dent. 2020, 42, 87–90. [Google Scholar]
- Mallineni, S.K.; Innes, N.P.; Raggio, D.P.; Araujo, M.P.; Robertson, M.D.; Jayaraman, J. Coronavirus disease (COVID-19): Characteristics in children and considerations for dentists providing their care. Int. J. Paediatr. Dent. 2020, 30, 245–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volgenant, C.M.C.; Persoon, I.F.; de Ruijter, R.A.G.; de Soet, J.J. Infection control in dental health care during and after the SARS-CoV-2 outbreak. Oral. Dis. 2020, 13408. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Dental Emergencies |
|---|
| Trauma involving facial bones |
| Tooth or mandibular fracture |
| Pericoronitis or third molar pain |
| Incomplete tooth extractions |
| Surgical post-operative osteitis |
| Uncontrolled bleeding |
| Dental treatment required prior to critical medical procedures |
| Abscess |
| Infection with intra-oral or extra-oral swelling that potentially compromise airway patient |
| Severe resistant dental pain from pulp inflammation |
| Cellulitis or a diffuse soft tissue bacterial infection |
| Additional urgent dental treatments |
| Extensive dental caries or defective tooth development |
| Restorations causing pain |
| Suture removal |
| Denture adjustment on radiation/oncology patients or when function impeded |
| Replacing temporary filling |
| Endodontic treatment for patients experiencing pain |
| Biopsy of abnormal tissue |
| Hierarchy of Procedures | Type of Procedures | Description of Procedures | |
|---|---|---|---|
| From remote | Telemedicine | Child has to be visited by dentist from remotely through the use of a phone video camera. The child’s general health status has to be evaluated as well. In this step, the dentist decides if a visit with the patient in the dental office is indicated or if the patient can be managed remotely. | |
| Scheduling dental office appointments | It is necessary to avoid crowding in the waiting room. Therefore, the number of appointments must be reduced to allow the sanitization of the working environments and the disinfection/sterilization of the dental instruments between two consecutive patients. | ||
| Dental office: waiting and service rooms | Before visiting the patient | The dental office staff has to be completely protected with gowns, disposable gloves and mask, and powered air-purifying respirators. The eyes should be protected with goggles or total face protectors. Before donning protective gloves, it is necessary to wash one’s hands twice, and after their use, three times again. | |
| Triage of patient and parents | As a first step in the dental office, the temperature of both child and his parent/caregiver must be taken and must measure lower than 37.3 °; a questionnaire about their general health status in relation to the SARS-CoV-2 pandemic must be filled out. | ||
| Dental office: dental chair room | Oral cavity disinfection | At the beginning of the visit, the patient must rinse for one minute with a solution of 0.5–1% oxygen peroxide or with iodine-povidone diluted 0.23% for at least 15 s. | |
| Teeth isolation | Rubber dam can be used to prevent the spread of saliva droplets from the patient’s mouth. | ||
| Minimally Invasive Treatments | Caries prevention | Educative intervention on correct oral health habits. Use of sodium fluoride varnishes or High Viscosity Glass Ionomer cements (HVGIC) sealants for prophylactic interventions. | |
| Enamel caries | Use of sodium fluoride gels/vanishes or silver diamine fluoride (SDF), or prescription of casein phosphopeptide—amorphous calcium phosphate for home use. | ||
| Dentine caries | Use of silver diamine fluoride (SDF), atraumatic restorative treatment (ART), interim therapeutic treatment (ITR), Chemo-mechanical techniques, sub-ablative laser, or Hall technique. | ||
| Dental complication treatments | Pulpits or abscesses | Opening primary tooth pulpal chamber with excavator or with burs powered by electric micromotor without water-air spray. In addition, endodontic treatment or primary tooth extraction. | |
| Dental office: after the visit | Sterilization, disinfection, and sanitation |
| |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cianetti, S.; Pagano, S.; Nardone, M.; Lombardo, G. Model for Taking Care of Patients with Early Childhood Caries during the SARS-Cov-2 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 3751. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113751
Cianetti S, Pagano S, Nardone M, Lombardo G. Model for Taking Care of Patients with Early Childhood Caries during the SARS-Cov-2 Pandemic. International Journal of Environmental Research and Public Health. 2020; 17(11):3751. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113751
Chicago/Turabian StyleCianetti, Stefano, Stefano Pagano, Michele Nardone, and Guido Lombardo. 2020. "Model for Taking Care of Patients with Early Childhood Caries during the SARS-Cov-2 Pandemic" International Journal of Environmental Research and Public Health 17, no. 11: 3751. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113751