Are Services Inclusive? A Review of the Experiences of Older GSD Women in Accessing Health, Social and Aged Care Services

 , ,
, , 
Abstract
:1. Background
2. Methods
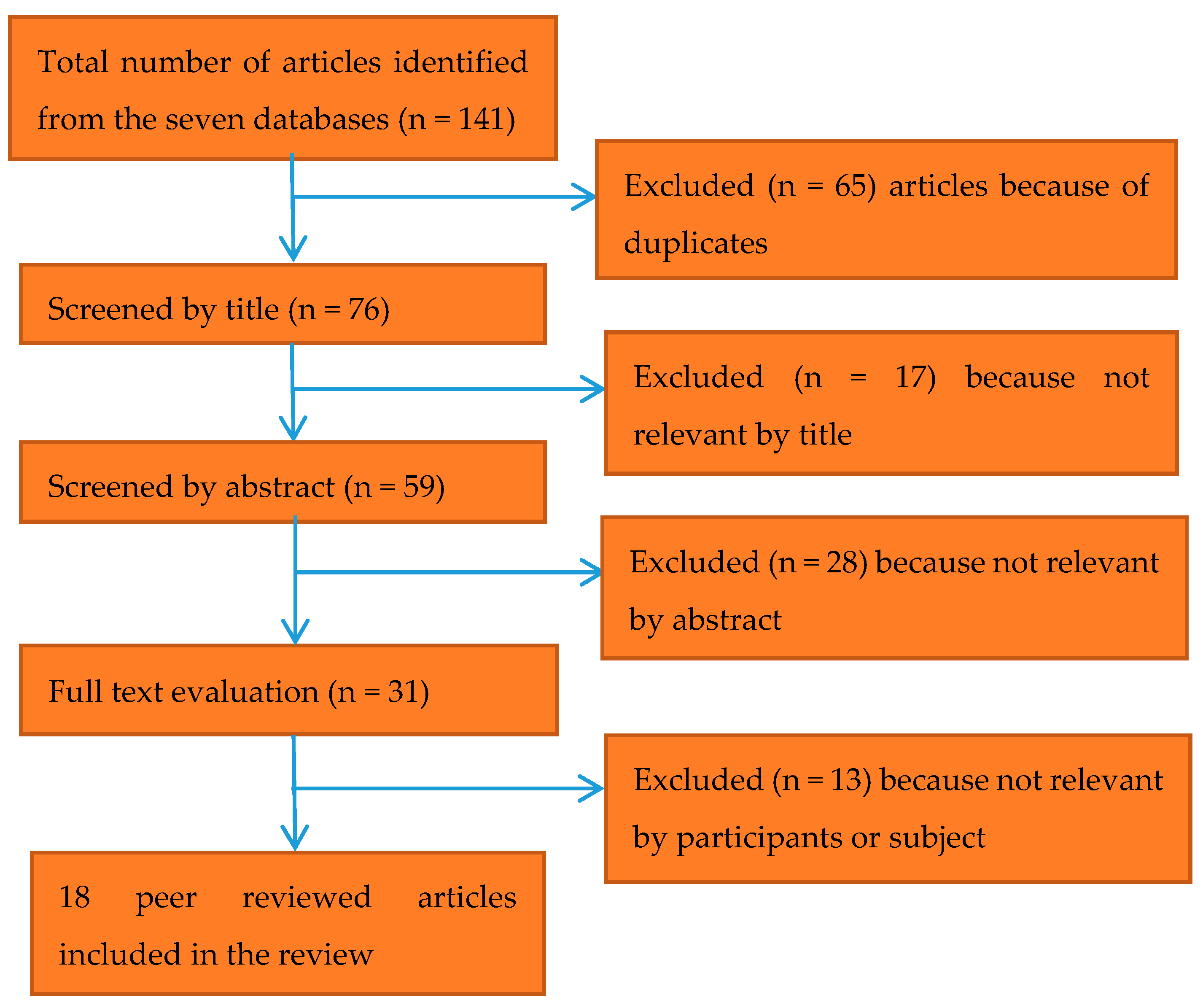
2.1. Research Design and Search Strategy
2.2. Quality Assessment
2.3. Data synthesis and Reporting
3. Results
3.1. Basic Characteristic of the Included Studies
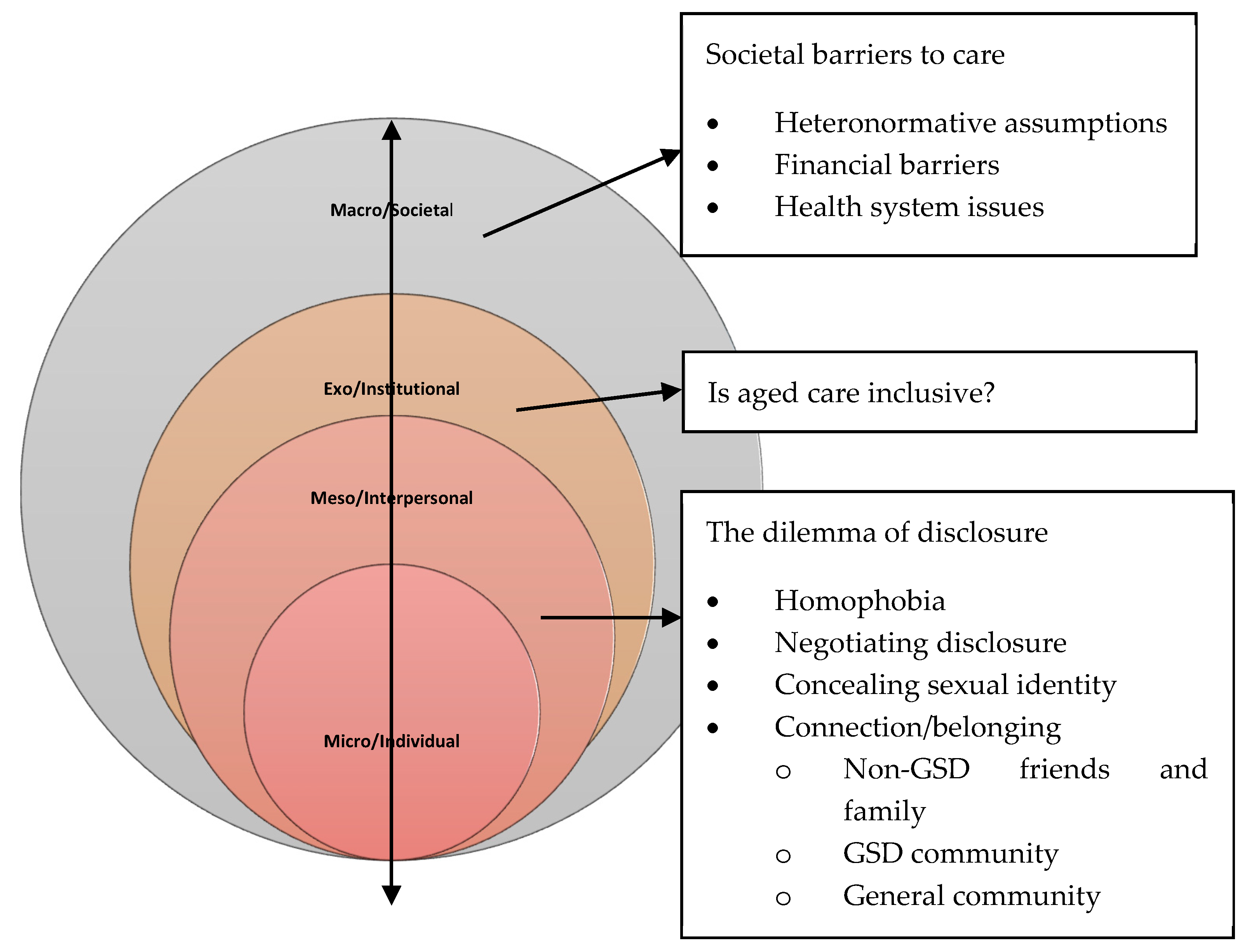
3.2. Interpersonal Level: The Dilemma of Disclosure
3.2.1. Homophobia
3.2.2. Negotiating Disclosure
3.2.3. Concealing Sexual Identity
3.2.4. Connection/Belonging and Support-Seeking Behaviour
3.2.5. Non-GSD Friends and Family
3.2.6. GSD Community
3.2.7. General Community
3.3. Institutional: Is Aged Care Inclusive?
3.4. Societal Barriers to Care
3.4.1. Heteronormative Assumptions
3.4.2. Financial Barriers
3.4.3. Health System Issues
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Phillips, J.; Marks, G. Ageing Lesbians: Marginalising Discourses and Social Exclusion in the Aged Care Industry. J. Gay Lesbian Soc. Serv. 2007, 20, 187–202. [Google Scholar] [CrossRef]
- United Nations Government Survey 2016. In E-Government in Support Of Sustainable Development; United Nations: New York, NY, USA, 2016.
- ILO; UNCTAD; UNDESA; WTO. Macroeconomic stability, inclusive growth and employment. In UN System Task Team on the Post; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Richters, J.; Altman, D.; Badcock, P.B.; Smith, A.M.; de Visser, R.O.; Grulich, A.E.; Rissel, C.; Simpson, J.M. Sexual identity, sexual attraction and sexual experience: The Second Australian Study of Health and Relationships. Sex. Health 2014, 11, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Blando, J. Twice hidden: Older gay and lesbian couples, friends, and intimacy. Generations 2001, 25, 87–89. [Google Scholar]
- Hinrichs, K.L.; Vacha-Haase, T. Staff perceptions of same-gender sexual contacts in long-term care facilities. J. Homosex. 2010, 57, 776–789. [Google Scholar] [PubMed]
- Metlife Mature Market Institute. The Lesbian Gay Aging Issues Network of the American Society on Aging. Out and aging: The MetLife study of lesbian and gay baby boomers. J. GLBT Fam. Stud. 2010, 6, 40–57. [Google Scholar]
- Koh, C.S.; Kang, M.; Usherwood, T. ‘I demand to be treated as the person I am’: Experiences of accessing primary health care for Australian adults who identify as gay, lesbian, bisexual, transgender or queer. Sex. Health 2014, 11, 258–264. [Google Scholar] [CrossRef]
- Khan, A.; Plummer, D.; Hussain, R.; Minichiello, V. Does physician bias affect the quality of care they deliver? Evidence in the care of sexually transmitted infections. Sex. Transm. Infect. 2008, 84, 150–151. [Google Scholar] [CrossRef]
- Johnson, M.J.; Jackson, N.C.; Arnette, J.K.; Koffman, S.D. Gay and lesbian perceptions of discrimination in retirement care facilities. J. Homosex. 2005, 49, 83–102. [Google Scholar] [CrossRef]
- Villar, F.; Serrat, R.; Fabà, J.; Celdrán, M. As long as they keep away from me: Attitudes toward non-heterosexual sexual orientation among residents living in Spanish residential aged care facilities. Gerontologist 2015, 55, 1006–1014. [Google Scholar] [CrossRef] [Green Version]
- Horner, B.; McManus, A.; Comfort, J.; Freijah, R.; Lovelock, G.; Hunter, M.; Tavener, M. How prepared is the retirement and residential aged care sector in Western Australia for older non-heterosexual people? Qual. Prim. Care 2012, 20, 263–274. [Google Scholar] [PubMed]
- Barrett, C.; Whyte, C.; Comfort, J.; Lyons, A.; Crameri, P. Social connection, relationships and older lesbian and gay people(1). Sex. Relatsh. Ther. 2015, 30, 131–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, M. Lesbian and gay people’s concerns about ageing and accessing services. Aust. Soc. Work 2009, 62, 186–201. [Google Scholar] [CrossRef] [Green Version]
- Duffy, F.; Healy, J.P. A social work practice reflection on issues arising for LGBTI older people interfacing with health and residential care: Rights, decision making and end-of-life care. Soc. Work. Health Care 2014, 53, 568–583. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.K.; Harold, R.D.; Boyer, J.M. Awareness of LGBT aging issues among aging services network providers. J. Gerontol. Soc. Work 2011, 54, 659–677, Epub 5 October 2011. [Google Scholar] [CrossRef] [PubMed]
- Addis, S.; Davies, M.; Greene, G.; MacBride-Stewart, S.; Shepherd, M. The health, social care and housing needs of lesbian, gay, bisexual and transgender older people: A review of the literature. Health Soc. Care Community 2009, 17, 647–658. [Google Scholar] [CrossRef]
- Albuquerque, G.A.; Garcia, C.D.L.; Quirino, G.D.S.; Alves, M.J.H.; Belém, J.M.; Figueiredo, F.W.D.S.; Paiva, L.D.S.; Nascimento, V.B.D.; Maciel, E.D.S.; Valenti, V.E.; et al. Access to health services by lesbian, gay, bisexual, and transgender persons: Systematic literature review. BMC Int. Health Hum. Rights. 2016, 16, 2. [Google Scholar] [CrossRef] [Green Version]
- Brotman, S.; Ryan, B.; Cormier, R. The Health and Social Service Needs of Gay and Lesbian Elders and Their Families in Canada. Gerontologist 2003, 43, 192–202. [Google Scholar] [CrossRef] [Green Version]
- Deevey, S. Older lesbian women an invisible minority. J. Gerontol. Nurs. 1990, 16, 35–39. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, K.M.; Koenka, A.C.; Sanchez, C.E.; Moshontz, H.; Cooper, H. Reporting standards for literature searches and report inclusion criteria: Making research syntheses more transparent and easy to replicate. Res. Synth. Methods 2015, 6, 87–95. [Google Scholar] [CrossRef]
- Sandelowski, M. “To be of use”: Enhancing the utility of qualitative research. Nurs. Outlook 1997, 45, 125–132. [Google Scholar] [CrossRef]
- Robinson, L.; Spilsbury, K. Systematic review of the perceptions and experiences of accessing health services by adult victims of domestic violence. Health Soc. Care Community 2008, 16, 16–30. [Google Scholar] [CrossRef] [PubMed]
- National Academies Press. The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Pruitt, S.D.; Epping-Jordan, J.E. Preparing the 21st century global healthcare workforce. BMJ 2005, 330, 637–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The ecology of human development: Experiments by nature and design. Am. Psychol. 1979, 32, 513–531. [Google Scholar] [CrossRef]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef] [Green Version]
- Anderson, L.; Healy, T.; Herringer, B.; Isaac, B.; Perry, T. Out in the Cold The Context of Lesbian Health in Northern British Columbia; British Columbia Centre of Excellence for Women’s Health: Vancouver, BC, USA, 2001. [Google Scholar]
- Averett, P.; Yoon, I.; Jenkins, C.L. Older lesbians: Experiences of aging, discrimination and resilience. J. Women Aging 2011, 23, 216–232. [Google Scholar] [CrossRef]
- Barbara, A.M.; Quandt, S.A.; Anderson, R.T. Experiences of Lesbians in the Health Care Environment. Women Health 2001, 34, 45–62. [Google Scholar] [CrossRef]
- Bjorkman, M.; Malterud, K. Lesbian women’s experiences with health care: A qualitative study. Scand. J. Prim. Health Care 2009, 27, 238–243. [Google Scholar] [CrossRef]
- Grigorovich, A. Negotiating sexuality in home care settings: Older lesbians and bisexual women’s experiences. Cult. Health Sex. 2015, 17, 947–961. [Google Scholar] [CrossRef]
- Grigorovich, A. Restricted Access: Older Lesbian and Bisexual Women’s Experiences with Home Care Services. Res. Aging 2015, 37, 763–783. [Google Scholar] [CrossRef] [PubMed]
- Grigorovich, A. The meaning of quality of care in home care settings: Older lesbian and bisexual women’s perspectives. Scand. J. Caring Sci. 2016, 30, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Hash, K.M.; Netting, F.E. It Takes a Community: Older Lesbians Meeting Social and Care Needs. J. Gay Lesbian Soc. Serv. 2009, 21, 326–342. [Google Scholar] [CrossRef]
- Hughes, M.; Kentlyn, S. Older Lesbians and Work in the Australian Health and Aged Care Sector. J. Lesbian Stud. 2015, 19, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, S.; Samdahl, D.M. Leisure in the lives of old lesbians: Experiences with and responses to discrimination. J. Leis. Res. 1998, 30, 233. [Google Scholar]
- Rowan, N.L.; Butler, S.S. Resilience in Attaining and Sustaining Sobriety among Older Lesbians with Alcoholism. J. Gerontol. Soc. Work. 2014, 57, 176–197. [Google Scholar] [CrossRef]
- Phillips, J.; Marks, G. Coming Out, Coming In: How do dominant discourses around aged care facilities take into account the identity and needs of ageing lesbians? Gay Lesbian Issues Psychol. Rev. 2006, 2, 67–77. [Google Scholar]
- Quam, J.K. The Story of Carrie and Anne. J. Gay Lesbian Soc. Serv. 1997, 6, 97–99. [Google Scholar] [CrossRef]
- Richard, C.A.; Brown, A.H. Configurations of Informal Social Support among Older Lesbians. J. Women Aging 2006, 18, 49–65. [Google Scholar] [CrossRef]
- Rowan, N.L.; Giunta, N. Lessons on social and health disparities from older lesbians with alcoholism and the role of interventions to promote culturally competent services. J. Human Behav. Soc. Environ. 2015, 26, 210–216. [Google Scholar] [CrossRef]
- Sinding, C.; Grassau, P.; Barnoff, L. Community Support, Community Values: The Experiences of Lesbians Diagnosed with Cancer. Women Health 2007, 44, 59–79. [Google Scholar] [CrossRef] [PubMed]
- Sinding, C.; Barnoff, L.; Grassau, P. Homophobia and Heterosexism in Cancer Care: The Experiences of Lesbians. CJNR (Can. J. Nurs. Res.) 2004, 36, 170–188. [Google Scholar] [PubMed]
- QIP. Rainbow Tick Standards. 2018. Available online: http://www.qip.com.au/standards/rainbow-tick-standards/ (accessed on 25 February 2020).
- Dwan, K.; Gamble, C.; Williamson, P.R.; Kirkham, J.J. Systematic review of the empirical evidence of study publication bias and outcome reporting bias—An updated review. PLoS ONE 2013, 8, e66844. [Google Scholar]



{kind=link}
{kind=link}
| Parameters | Inclusion | Exclusion | Key Words/Steps |
|---|---|---|---|
| Context | International | None | N/A |
| Language | Written in English | Other languages | Select for English only |
| Time | 1990 | Before 1989 | Select from 1990 onwards |
| Population | Studies which include older lesbian, transgender, bisexual, intersex and queer population | Studies which only focus on young LGBTQI population | Older OR ageing OR aged OR elder * title OR aging (title) and Title (lesbian * OR transgender OR transsexual OR bisexual OR intersex OR queer OR homosexual * OR ‘same sex attracted’ OR ‘non-heterosexual’ OR ‘sexual minorities’ OR ‘gender diverse’ OR ‘sexually diverse’ OR two-spirit) |
| Interest | Studies concerned with the participants’ experiences (i.e., views and perceptions including facilitators and barriers) of accessing health, social and aged care services | Not concerned with health, social and aged care | (Title) AND ‘health need’ (title) OR ‘health access’ (title) OR ‘health care’ (title) OR ‘health services accessibility’ (title) OR ‘social service’ (title) OR ‘aged care ‘(title) OR retirement (title) ‘residential care’ (title) OR ‘nursing home’ (title) OR ‘home care’ (title) OR ‘community membership’ (title) OR belonging (title) |
| Study type | Primary research including qualitative, quantitative and mixed method designs | Studies which DO NOT include qualitative, quantitative and mixed methods of data collection and analysis | NA |
| Grey literature (unpublished documents) | Book reviews, letters to the editor, editorials, opinion pieces, literature reviews, policy documents | NA |
| No | Authors/Year | Country | Participants | Sample Size | Age Range | Services Referred | Research Design | Data Collection | Theoretical Approach | Main Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Anderson et al., 2001 [30] | Canada | Lesbian | 40 | 18+ | Health care | Qualitative | Focus group discussions | - | Homophobic responses from health care providers and heterosexism discouraged lesbian women from accessing health care. |
| 2 | Averett et al., 2011 [31] | USA | Lesbian | 456 | 51–86 | Social and health care | Quantitative | Online survey | - | Older lesbians underutilised health and social services because of homophobia and ageism. |
| 3 | Barbara et al., 2001 [32] | USA | Lesbian | 32 | 18 to 55+ | Health care | Qualitative | Focus group discussions | - | Lesbian women have anxiety and concern related to self-disclosure of sexual orientation; non-disclosure of sexual orientation; seeking out gay-positive physicians; frustration with assumptions of heterosexuality; treatment of lesbian partners. |
| 4 | Bjorkman et al., 2009 [33] | Norway | Lesbian | 121 | 18+ | Health care | Qualitative | Written answers to a web-based open questionnaire | Heteronormativity | Health care professionals should facilitate the disclosure of a lesbian orientation; display a positive attitude towards homosexuality; and acknowledge and respect the lesbian orientation in providing care to gender and sexually diverse (GSD) women. |
| 5 | Grigorovich, 2015 [34] | Canada | Lesbian and bisexual | 16 | 55–72 | Home care | Qualitative | In-depth interviews | - | Reveling sexual identity to home care workers involved a complex decision-making process and was done on a case-by-case basis. |
| 6 | Grigorovich, 2015 [35] | Canada | Lesbian and bisexual | 16 | 55–72 | Home care | Qualitative | Semi-structured interviews | Feminist political economy framework | Chronic illness, limited functional status and homophobia influenced older lesbian women’s ability to access support and care. |
| 7 | Grigorovich, 2016 [36] | Canada | Lesbian and bisexual | 16 | 55–72 | Home care | Qualitative | Semi-structured interviews | Feminist ethic of care | Quality of care was enabled when providers were attentive and responsive to lesbian and bisexual women’s needs, demonstrated appropriate competencies and actively enabled recipients’ comfort. |
| 8 | Hash et al., 2009 [37] | USA | Lesbian | 2 | 69 and 77 | Social care | Qualitative | Case studies | Psychological contracting | Older lesbian women experience isolation which impacted their access to support. |
| 9 | Huges et al., 2015 [38] | Australia | Lesbian | 4 | 59–72 | Health and aged care | Qualitative | Case stories/Narrative research | Socio-linguistic | Older lesbian women have diverse perspectives about disclosing sexual identity, socialising with lesbian groups and accessing aged care. |
| 10 | Jacobson et al., 1998 [39] | USA | Lesbian | 16 | 60+ | Discrimination and leisure | Qualitative | Written responses to leisure questions and in-depth interviews | Ecological perspective | Discrimination and stigma influenced older lesbian’s leisure. |
| 11 | Rowan et al., 2014 [40] | USA | Lesbian | 20 | 50+ | Health care | Qualitative | Interviews | Phenomenology | Close connections with family members and involvement in lesbian oriented groups are vital to accessing support. |
| 12 | Phillips et al., 2007 [1] | Australia | Lesbian | 6 | 45–69 | Aged care | Qualitative | FGDs and advertisement brochures | Feminist poststructuralism | Provision of services for older lesbians is structured in such a way that lead to exclusion and aged care advertising materials exclude non-heterosexual relationships. |
| 13 | Phillips et al., 2006 [41] | Australia | Lesbian | 6 | 45–69 | Aged care | Qualitative | Focus group discussions | Feminist poststructuralism | Aged care spaces are constructed to serve a normative understanding of identities and relationships by not meeting the needs of ageing lesbians. |
| 14 | Quam, 1997 [42] | USA | Lesbian | 2 | 81 and 77 | Home care | Qualitative | Case studies | - | Older lesbian women socialise little and have no interest in attending activities for older GSD people. |
| 15 | Richard et al., 2006 [43] | USA | Lesbian | 25 | 55+ | Social services | Qualitative | In-depth interviews | - | Ageing lesbians have financial and housing concerns and are less likely to access social services due to perception of bias within the service and lack of connections with service users. |
| 16 | Rowan et al., 2015 [44] | USA | Lesbian | - | 52+ | Health care | Qualitative | In-depth interviews | Intersectionality | Older lesbians experience discrimination at work and public spaces because of their sexual identities. |
| 17 | Sinding et al., 2007 [45] | Canada | Lesbian | 26 | 36–72 | Cancer care | Qualitative | Semi-structured interviews | Grounded theory | Older lesbians experience isolation and disconnection and receive support mainly from lesbian partners and friends. |
| 18 | Sinding et al., 2004 [46] | USA | Lesbian | 26 | 36–72 | Cancer care | Qualitative | Interviews | - | Heterosexism and homophobia impacted lesbian women’s access to standard care. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dune, T.; Ullman, J.; Ferfolja, T.; Thepsourinthone, J.; Garga, S.; Mengesha, Z. Are Services Inclusive? A Review of the Experiences of Older GSD Women in Accessing Health, Social and Aged Care Services. Int. J. Environ. Res. Public Health 2020, 17, 3861. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113861
Dune T, Ullman J, Ferfolja T, Thepsourinthone J, Garga S, Mengesha Z. Are Services Inclusive? A Review of the Experiences of Older GSD Women in Accessing Health, Social and Aged Care Services. International Journal of Environmental Research and Public Health. 2020; 17(11):3861. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113861
Chicago/Turabian StyleDune, Tinashe, Jacqueline Ullman, Tania Ferfolja, Jack Thepsourinthone, Shirali Garga, and Zelalem Mengesha. 2020. "Are Services Inclusive? A Review of the Experiences of Older GSD Women in Accessing Health, Social and Aged Care Services" International Journal of Environmental Research and Public Health 17, no. 11: 3861. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113861