Reporting Guidelines for Community-Based Participatory Research Did Not Improve the Reporting Quality of Published Studies: A Systematic Review of Studies on Smoking Cessation

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Types of Articles Included
2.2. Search Strategy
2.3. Study Selection
2.4. Definition of Community-Based Participatory Research (CBPR)
2.5. Data Extraction and Assessment of Reporting Quality
2.6. Data Analysis
3. Results
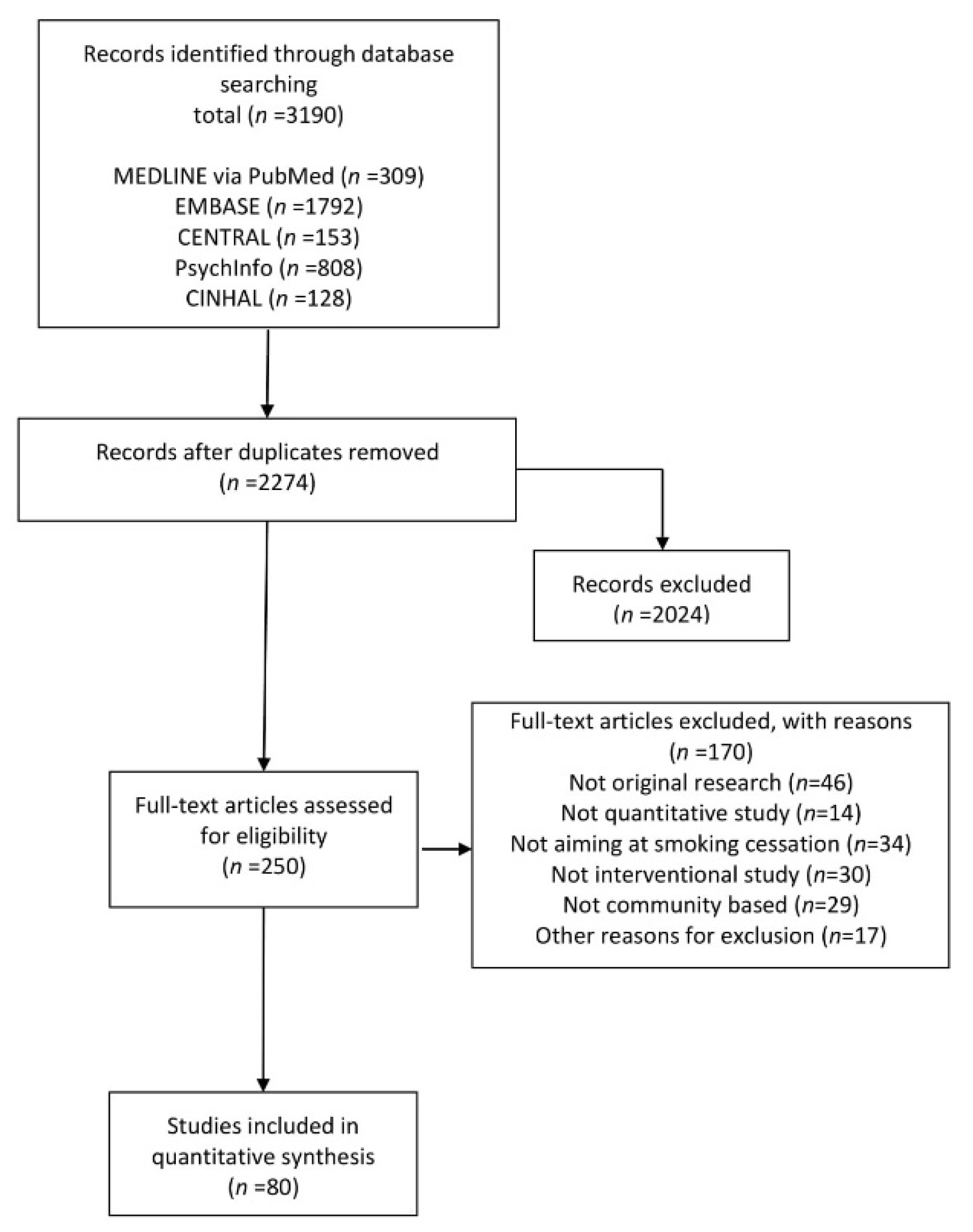
3.1. Search Results and Characteristics of the Articles Included
3.2. Conformity with the CBPR Reporting Guidelines
3.3. Factors Associated with the Total Reporting Score
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tam, W.W.S.; Lo, K.K.H.; Khalechelvam, P. Endorsement of PRISMA statement and quality of systematic reviews and meta-analyses published in nursing journals: A cross-sectional study. BMJ Open 2017, 7, e013905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panic, N.; Leoncini, E.; de Belvis, G.; Ricciardi, W.; Boccia, S. Evaluation of the endorsement of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement on the quality of published systematic review and meta-analyses. PLoS ONE 2013, 8, e83138. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; The CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Jones, A.; Lepage, L.; CONSORT Group (Consolidated Standards for Reporting of Trials). Use of the CONSORT statement and quality of reports of randomized trials: A comparative before-and-after evaluation. JAMA 2001, 285, 1992–1995. [Google Scholar] [CrossRef]
- Plint, A.C.; Moher, D.; Morrison, A.; Schulz, K.; Altman, D.G.; Hill, C.; Isabelle Gaboury, I. Does the CONSORT checklist improve the quality of reports of randomised controlled trials? A systematic review. Med. J. Aust. 2006, 185, 263–267. [Google Scholar] [CrossRef]
- Turner, L.; Shamseer, L.; Altman, D.G.; Schulz, K.F.; Moher, D. Does use of the CONSORT Statement impact the completeness of reporting of randomised controlled trials published in medical journals? A Cochrane Review. Syst. Rev. 2012, 1, 60. [Google Scholar] [CrossRef] [Green Version]
- Israel, B.A.; Eng, E.; Schulz, A.J.; Parker, E.A. Methods in Community-Based Participatory Research for Health, 2nd ed.; Jossey-Bass: San Francisco, CA, USA, 2012; ISBN 978-1-118-02186-6. [Google Scholar]
- Minkler, M.; Wallerstein, N. Community-Based Participatory Research for Health: From Process to Outcomes, 2nd ed.; Jossey-Bass: San Francisco, CA, USA, 2008; ISBN 978-04-7026-043-2. [Google Scholar]
- Smith, L.; Rosenzweig, L.; Schmidt, M. Best practices in the reporting of participatory action research: Embracing both the forest and the trees. Couns. Psychol. 2010, 38, 1115–1138. [Google Scholar] [CrossRef]
- Andrews, J.O.; Newman, S.D.; Heath, J.; Williams, L.B.; Tingen, M.S. Community-based participatory research and smoking cessation interventions: A review of the evidence. Nurs. Clin. N. Am. 2012, 47, 81–96. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Eckhardt, J. The looming threat of Asian tobacco companies to global health. Lancet 2017, 389, 1958–1960. [Google Scholar] [CrossRef] [Green Version]
- WHO Report on the Global Tobacco Epidemic 2017; World Health Organization: Geneva, Switzerland, 2017.
- Goodchild, M.; Nargis, N.; Tursan d′Espaignet, E. Global economic cost of smoking-attributable diseases. Tob. Control 2018, 27, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Minkler, M. Ethical challenges for the ‘outside’ researcher in community-based participatory research. Health Educ. Behav. 2004, 31, 684–697. [Google Scholar] [CrossRef] [PubMed]
- Oetzel, J.G.; Wallerstein, N.; Duran, B.; Sanchez-Youngman, S.; Nguyen, T.; Woo, K.; Wang, J.; Schulz, A.; Keawe’aimoku Kaholokula, J.; Israel, B.; et al. Impact of participatory health research: A test of the community-based participatory research conceptual model. BioMed. Res. Int. 2018, 2018, 7281405. [Google Scholar] [CrossRef]
- Hicks, S.; Duran, B.; Wallerstein, N.; Avila, M.; Belone, L.; Lucero, J.; Magarati, M.; Mainer, E.; Martin, D.; Muhammad, M.; et al. Evaluating community-based participatory research to improve community-partnered science and community health. Prog. Community Health Partnersh. 2012, 6, 289–299. [Google Scholar] [CrossRef]
- Rothman, J.; Erlich, J.; Tropman, J. Strategies of Community Intervention: Macro Practice, 6th ed.; FE Peacock Publishers: Itasca, IL, USA, 2001; ISBN 978-08-7581-436-0. [Google Scholar]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Darity, W.A.; Chen, T.T.L.; Tuthill, R.W.; Buchanan, D.R.; Winder, A.E.; Stanek, E.; Cernada, G.P.; Pastides, H. A multi-city community-based smoking research intervention project in the African-American population. Int. Q. Community Health Educ. 2007, 26, 323–336. [Google Scholar] [CrossRef]
- Prendergast, M.L.; McCollister, K.; Warda, U. A randomized study of the use of screening, brief intervention, and referral to treatment (SBIRT) for drug and alcohol use with jail inmates. J. Subst. Abuse Treat. 2017, 74, 54–64. [Google Scholar] [CrossRef] [Green Version]
- Little, J.; Higgins, J.P.T.; Ioannidis, J.P.A.; Moher, D.; Gagnon, F.; von Elm, E.; Khoury, M.J.; Cohen, B.; Davey-Smith, G.; Grimshaw, J.; et al. STrengthening the REporting of Genetic Association Studies (STREGA)-an extension of the STROBE statement. Genet. Epidemiol. 2009, 33, 581–598. [Google Scholar] [CrossRef]
- Delgado-Rodríguez, M.; Llorca, J. Bias. J. Epidemiol. Community Health 2004, 58, 635–641. [Google Scholar] [CrossRef] [Green Version]
- Rosenthal, R.; Jacobson, L. Pygmalion in the classroom. Urban Rev. 1968, 3, 16–20. [Google Scholar] [CrossRef]
- Banno, M.; Tsujimoto, Y.; Kataoka, Y. The majority of reporting guidelines are not developed with the Delphi method: A systematic review of reporting guidelines. J. Clin. Epidemiol. 2020, 124, 50–57. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All Studies (N = 80) | Studies Pre-Guideline (n = 38) | Studies Post-Guideline (n = 42) | ||||
|---|---|---|---|---|---|---|
| Item | n | % | N | % | n | % |
| 1. Structure of the article | ||||||
| q1: Organizational structure | 80 | 100% | 38 | 100% | 42 | 100% |
| 2. Key elements of the project | ||||||
| q2.1: Initiation | 62 | 78% | 27 | 71% | 35 | 83% |
| q2.2: Timeframe | 75 | 94% | 36 | 95% | 39 | 93% |
| q2.3: Characteristics of participants and co-researchers | 59 | 74% | 28 | 74% | 31 | 74% |
| q2.4: Role of participants and co-researchers | 57 | 71% | 26 | 68% | 31 | 74% |
| q2.5: Process/methodology of the project | 80 | 100% | 38 | 100% | 42 | 100% |
| q2.6: Outcomes/emergent actions | 80 | 100% | 38 | 100% | 42 | 100% |
| q2.7: Future orientation | 72 | 90% | 33 | 87% | 39 | 93% |
| q2.8: Graphics of the project design | 30 | 38% | 8 | 21% | 22 | 52% |
| 3. Role of the researchers described | ||||||
| q3.1: Who wrote the article | 17 | 21% | 6 | 16% | 11 | 26% |
| q3.2: Who did not write the article | 31 | 39% | 17 | 45% | 14 | 33% |
| q3.3: Personal outcomes | 18 | 23% | 9 | 24% | 9 | 21% |
| 4. Challenges, pitfalls, and limitations of the project | ||||||
| q4.1: Their characteristics | 74 | 93% | 33 | 87% | 41 | 98% |
| q4.2: Their management | 38 | 48% | 17 | 45% | 21 | 50% |
| Studies Pre-Guideline (n = 29) | Studies Post-Guideline (n = 38) | |||
|---|---|---|---|---|
| Characteristics | Mean | 95% CI * | Mean | 95% CI * |
| Reporting score | 9.97 | 1.02, 1.98 | 9.32 | 1.39, 2.67 |
| Effect size | 0.11 | 0.12, 0.26 | 0.08 | 0.08, 0.16 |
| Characteristics | n | % | n | % |
| Evaluation of the project | ||||
| No | 13 | 45% | 17 | 45% |
| Study design | ||||
| Individual randomized CT | 4 | 14% | 11 | 29% |
| Cluster-randomized CT | 10 | 34% | 5 | 13% |
| Quasi-experimental | 15 | 52% | 22 | 58% |
| Characteristics | Beta Coefficient | 95% CI * |
|---|---|---|
| Period | ||
| Pre-guideline | ref | — |
| Post-guideline | −0.83 | −1.75, 0.10 |
| Effect size | −2.90 | −5.77, 0.04 |
| Evaluation of the project | ||
| No | ref | — |
| Yes | −0.04 | −0.95, 0.88 |
| Study design | ||
| Individually randomized CT | ref | — |
| Cluster-randomized CT | −0.61 | −2.01, 0.79 |
| Quasi-experimental | −0.89 | −2.01, 0.23 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kato, D.; Kataoka, Y.; Suwangto, E.G.; Kaneko, M.; Wakabayashi, H.; Son, D.; Kawachi, I. Reporting Guidelines for Community-Based Participatory Research Did Not Improve the Reporting Quality of Published Studies: A Systematic Review of Studies on Smoking Cessation. Int. J. Environ. Res. Public Health 2020, 17, 3898. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113898
Kato D, Kataoka Y, Suwangto EG, Kaneko M, Wakabayashi H, Son D, Kawachi I. Reporting Guidelines for Community-Based Participatory Research Did Not Improve the Reporting Quality of Published Studies: A Systematic Review of Studies on Smoking Cessation. International Journal of Environmental Research and Public Health. 2020; 17(11):3898. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113898
Chicago/Turabian StyleKato, Daisuke, Yuki Kataoka, Erfen Gustiawan Suwangto, Makoto Kaneko, Hideki Wakabayashi, Daisuke Son, and Ichiro Kawachi. 2020. "Reporting Guidelines for Community-Based Participatory Research Did Not Improve the Reporting Quality of Published Studies: A Systematic Review of Studies on Smoking Cessation" International Journal of Environmental Research and Public Health 17, no. 11: 3898. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113898