Noncommunicable Diseases, Park Prescriptions, and Urban Green Space Use Patterns in a Global South Context: The Case of Dhaka, Bangladesh


Abstract
:1. Introduction
2. Materials and Methods
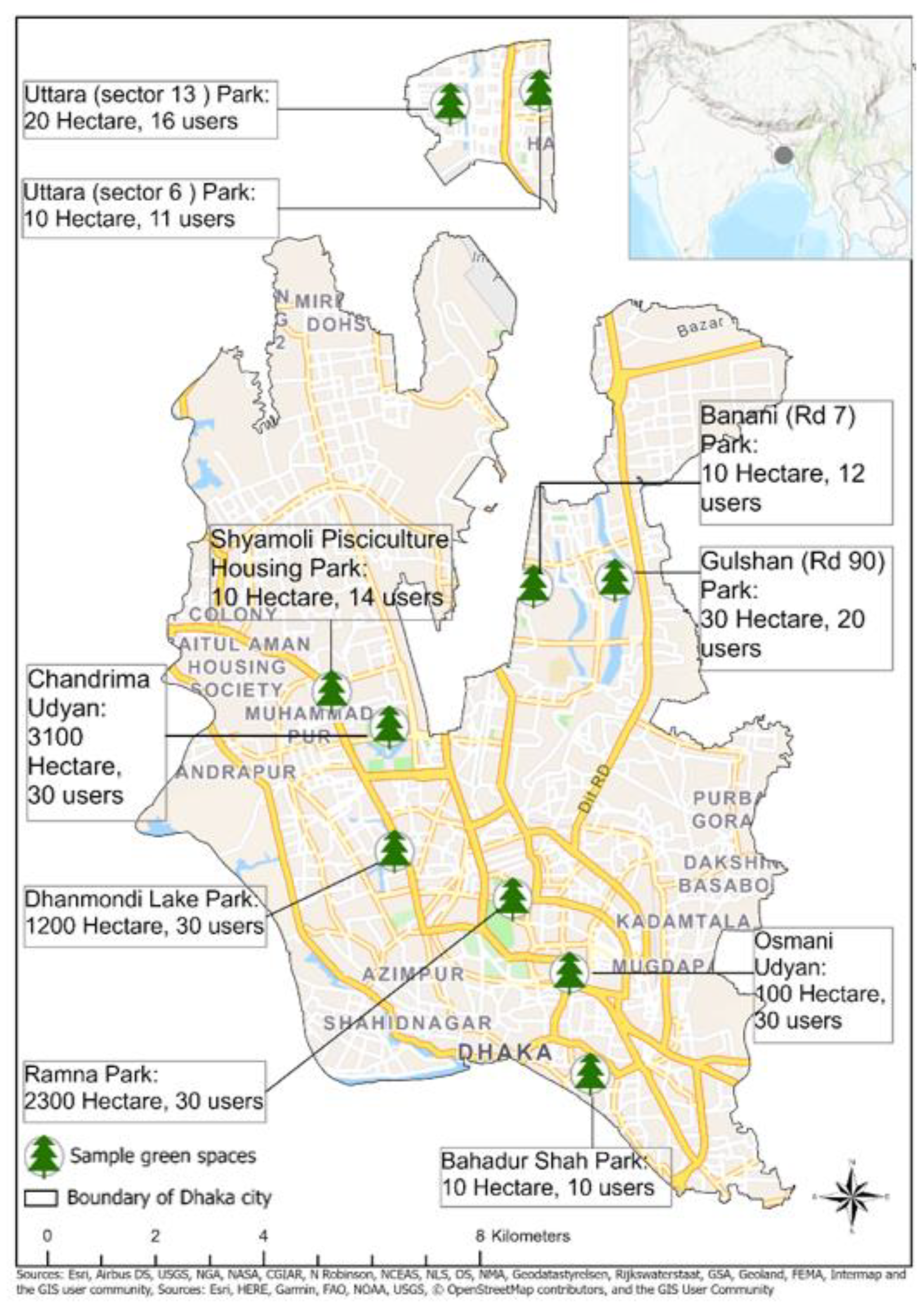
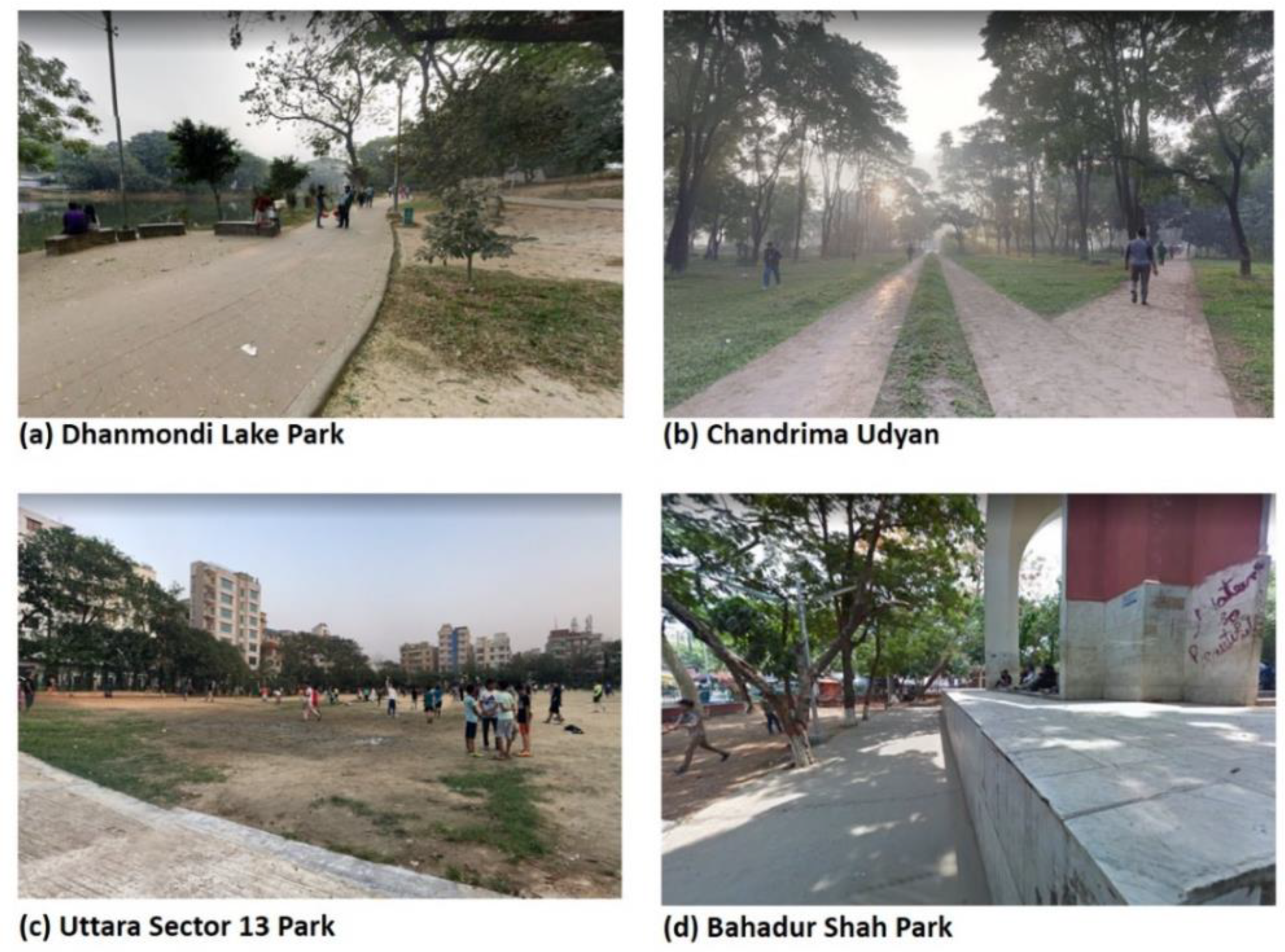
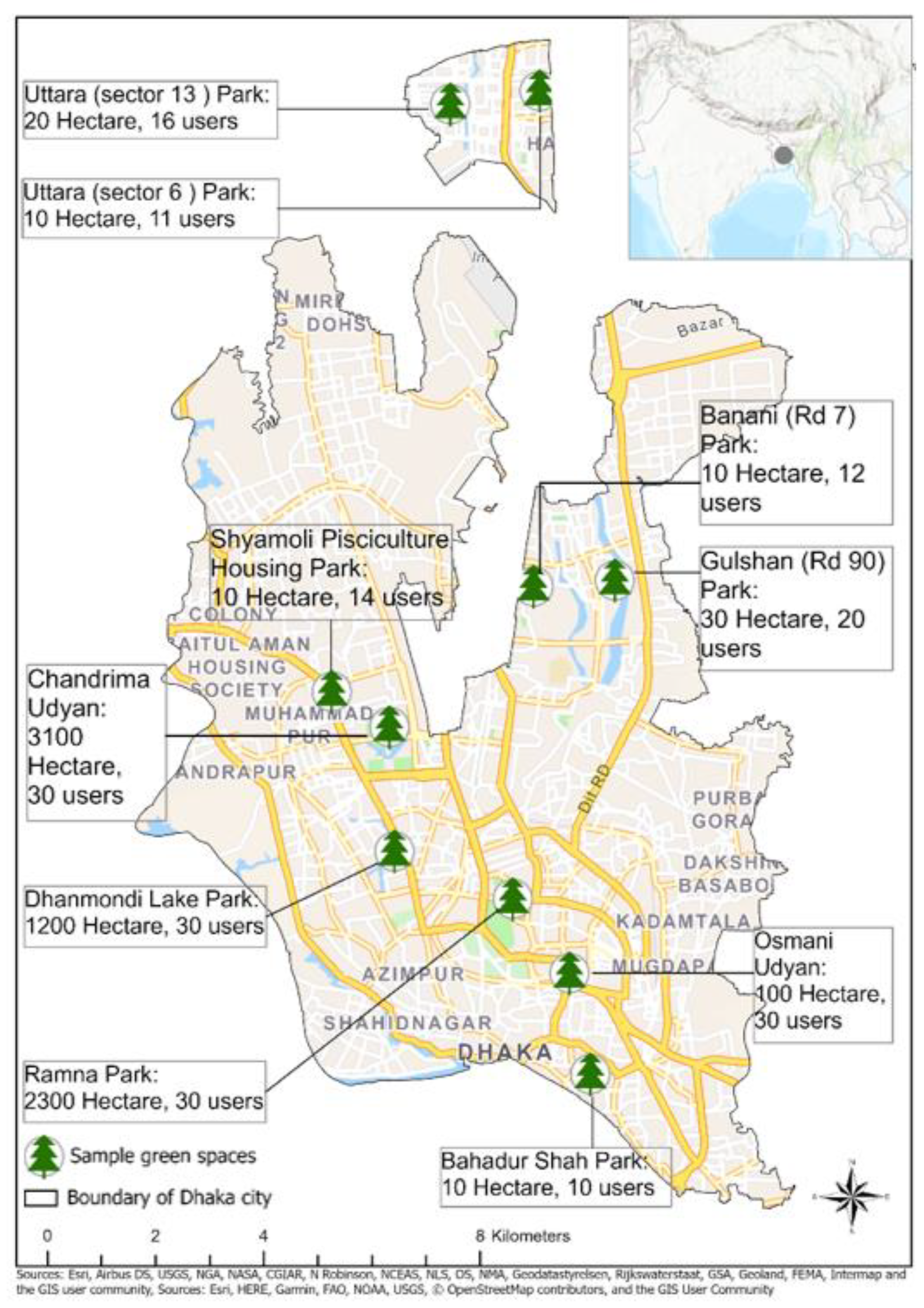
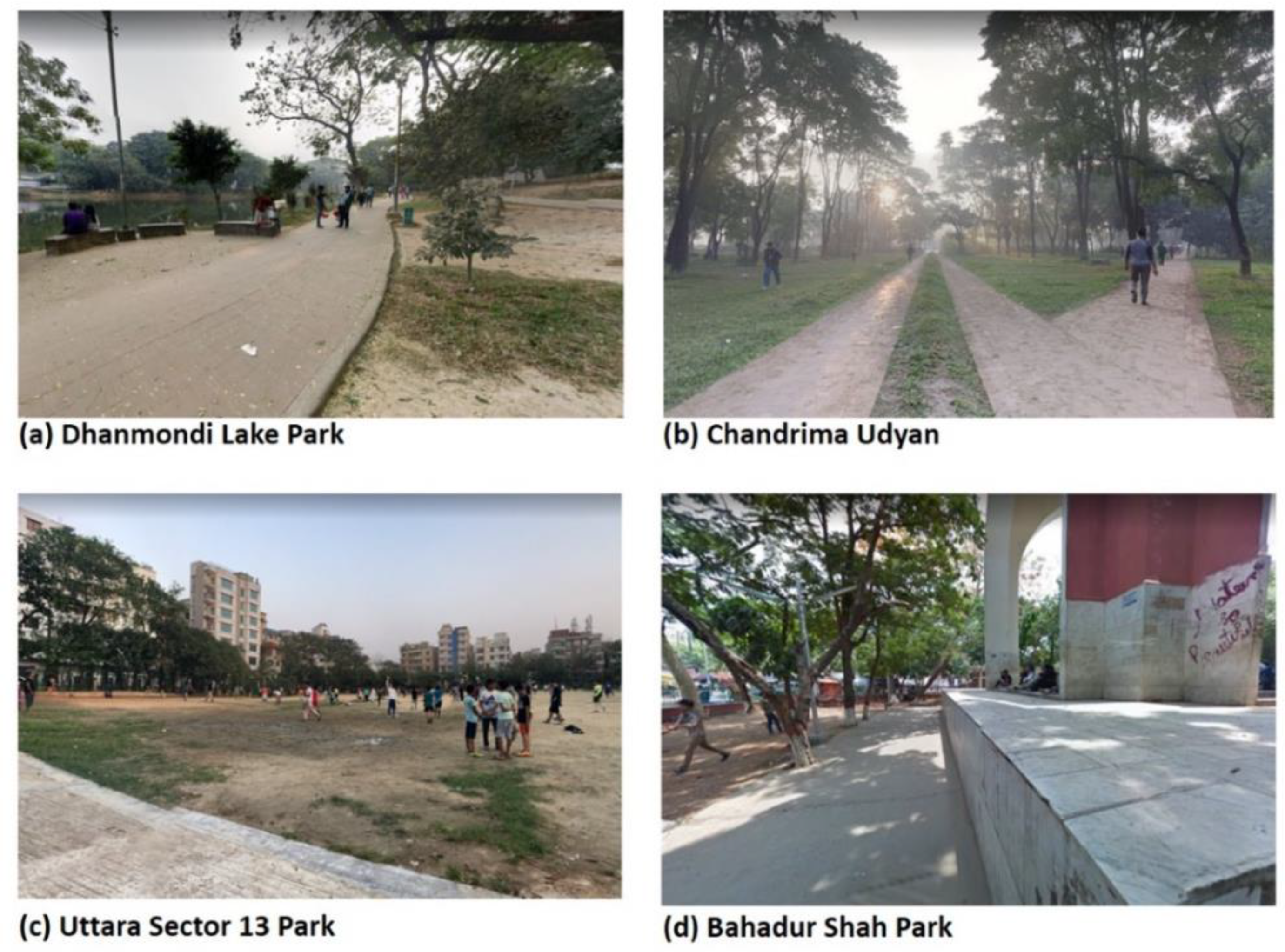
2.1. Case Study Area
2.2. Sample and Data Collection
Data Collection Sites
2.3. Measures
2.3.1. Green Space Use Patterns
2.3.2. Green Space Characteristics
2.3.3. Green Space Attachment
2.3.4. Green Space Availability
2.3.5. Health Condition and ParkRx
2.3.6. Confounders
2.4. Analyses
2.4.1. Main Analyses
2.4.2. Mediation Analyses
3. Results
3.1. Sample Characteristics
3.2. Green Space Characteristics and Use Patterns
3.3. Predictors of Green Space Use Patterns
3.3.1. Influence of Health Condition and ParkRx on Green Space ‘Use Intensity’
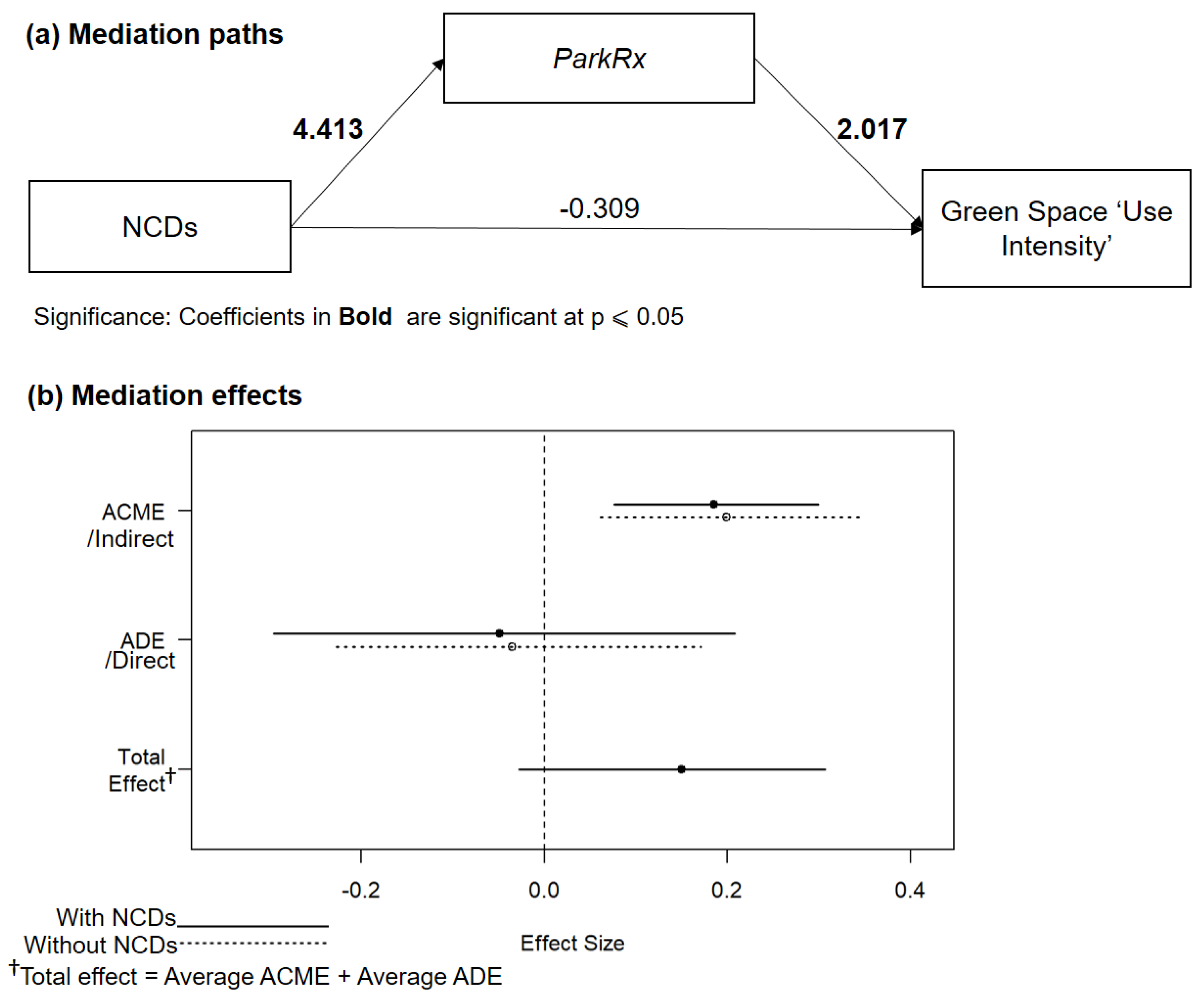
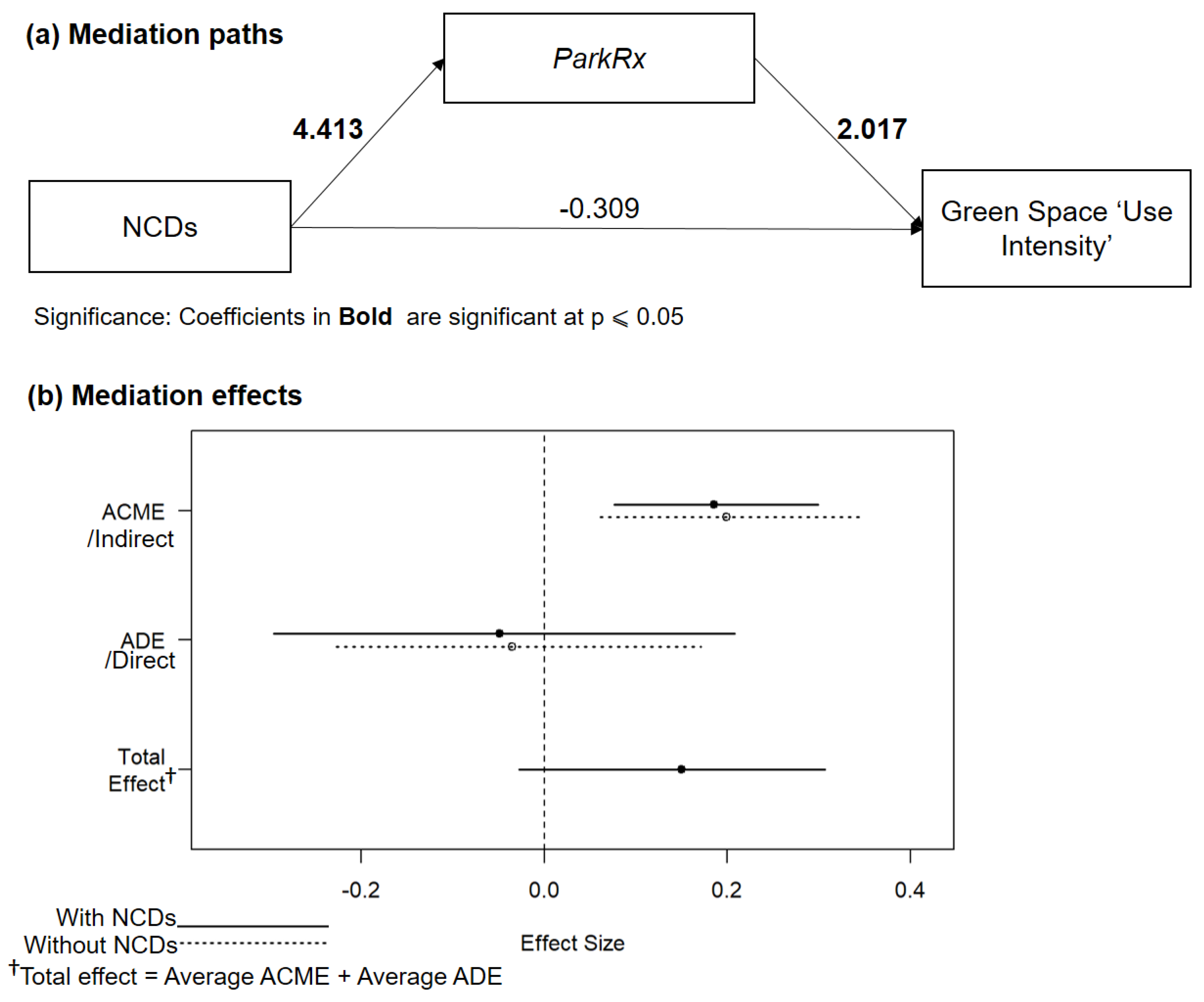
3.3.2. Mediation Effect of ParkRx on Green Space ‘Use Intensity’
4. Discussion
4.1. General Findings
4.2. Policy and Practice Implications
4.3. Strengths, Limitations, and Future Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Model 4 † | |||
|---|---|---|---|
| Odds | 95% CI | p-Value | |
| Attractiveness | 0.726 | 0.503–1.031 | 0.0788 |
| Accessibility | 1.159 | 0.746–1.809 | 0.5093 |
| Attachment | 1.222 | 0.843–1.799 | 0.2945 |
| Green space per capita | 1.164 | 1.03–1.357 | 0.029 |
| NCDs | 82.589 | 19.524−711.112 | 0.000000439 |
| Constant | 0.232 | 0.007–5.801 | 0.3842 |
| Pseudo R2 | 0.57 | ||
| AIC | 158.85 | ||
| Model 5 † | |||
|---|---|---|---|
| Odds | 95% CI | p-Value | |
| Attractiveness | 0.734 | 0.522–1.015 | 0.0665 |
| Accessibility | 0.756 | 0.505–1.121 | 0.1688 |
| Attachment | 2.104 | 1.497–3.062 | 0.0000401 |
| Green space per capita | 1.01 | 0.92–1.09 | 0.7972 |
| NCDs/Chronic | 0.733 | 0.202–2.543 | 0.6273 |
| ParkRx | 7.519 | 2.554–25.663 | 0.000539 |
| Constant | 0.051 | 0.003–0.736 | 0.031588 |
| Pseudo R2 | 0.355 | ||
| AIC | 189.18 | ||
| Estimate | 95% CI Lower | 95% CI Upper | p-Value | |
|---|---|---|---|---|
| ACME (without NCDs) | 0.1991 | 0.061 | 0.35 | 0.002 |
| ACME (with NCDs) | 0.1852 | 0.0762 | 0.3 | 0.002 |
| ADE (without NCDs) | −0.0352 | −0.2273 | 0.17 | 0.712 |
| ADE (with NCDs) | −0.0491 | −0.2957 | 0.21 | 0.712 |
| Total Effect | 0.15 | −0.028 | 0.31 | 0.076 |
| Prop. Mediated (without NCDs) | 1.2626 | −2.6145 | 8.83 | 0.078 |
| Prop. Mediated (with NCDs) | 1.1933 | −2.0749 | 7.68 | 0.078 |
| ACME (average) | 0.1921 | 0.0696 | 0.32 | 0.002 |
| ADE (average) | −0.0421 | −0.2583 | 0.19 | 0.712 |
| Prop. Mediated | 1.228 | −2.3953 | 8.1 | 0.078 |
References
- Kondo, M.C.; Fluehr, J.M.; McKeon, T.; Branas, C.C. Urban green space and its impact on human health. Int. J. Environ. Res. Public Health 2018, 15, 445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leng, H.; Li, S.; Yan, S.; An, X. Exploring the relationship between green space in a neighbourhood and cardiovascular health in the winter city of China: A study using a health survey for harbin. Int. J. Environ. Res. Public Health 2020, 17, 513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schinasi, L.H.; Quick, H.; Clougherty, J.E.; De Roos, A.J. Greenspace and Infant Mortality in Philadelphia, PA. J. Urban Heal. 2019, 96, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Greener neighborhoods, slimmer people evidence from 246 920 Australians. Int. J. Obes. 2014, 38, 156–159. [Google Scholar] [CrossRef]
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef] [Green Version]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef]
- Kabisch, N.; Qureshi, S.; Haase, D. Human-environment interactions in urban green spaces—A systematic review of contemporary issues and prospects for future research. Environ. Impact Assess. Rev. 2015, 50, 25–34. [Google Scholar] [CrossRef]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A Review of the Health Benefits of Greenness. Curr. Epidemiol. Reports 2015, 2, 131–142. [Google Scholar] [CrossRef] [Green Version]
- Lindley, S.J.; Cook, P.A.; Dennis, M.; Gilchrist, A. Biodiversity, Physical Health and Climate Change: A Synthesis of Recent Evidence. In Biodiversity and Health in the Face of Climate Change; Springer Open: Cham, Switzerland, 2019; pp. 17–46. [Google Scholar]
- Bezold, C.P.; Stark, J.H.; Rundle, A.; Konty, K.; Day, S.E.; Quinn, J.; Neckerman, K.; Roux, A.V.D. Relationship between Recreational Resources in the School Neighborhood and Changes in Fitness in New York City Public School Students. J. Urban Heal. 2017, 94, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Chodzko-Zajko, W.; Schwingel, A. Chae Hee Park Successful Aging: The Role of Physical Activity. Am. J. Lifestyle Med. 2009, 3, 20–28. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Green space is associated with walking and moderate-to-vigorous physical activity (MVPA) in middle-to-older-aged adults: Findings from 203 883 Australians in the 45 and Up Study. Br. J. Sports Med. 2014, 48, 404–406. [Google Scholar] [CrossRef]
- Rojas-Rueda, D.; Nieuwenhuijsen, M.J.; Gascon, M.; Perez-Leon, D.; Mudu, P. Green spaces and mortality: A systematic review and meta-analysis of cohort studies. Lancet Planet. Heal. 2019, 3, e469–e477. [Google Scholar] [CrossRef] [Green Version]
- Browning, M.H.E.M.; Rigolon, A. School Green Space and Its Impact on Academic Performance: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2019, 16, 429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dzhambov, A.M.; Markevych, I.; Hartig, T.; Tilov, B.; Arabadzhiev, Z.; Stoyanov, D.; Gatseva, P.; Dimitrova, D.D. Multiple pathways link urban green- and bluespace to mental health in young adults. Environ. Res. 2018, 166, 223–233. [Google Scholar] [CrossRef] [PubMed]
- 1 Maas, J.; van Dillen, S.M.E.; Verheij, R.A.; Groenewegen, P.P. Social contacts as a possible mechanism behind the relation between green space and health. Heal. Place 2009, 15, 586–595. [Google Scholar] [CrossRef] [Green Version]
- Dadvand, P.; Nieuwenhuijsen, M.J.; Esnaola, M.; Forns, J.; Basagaña, X.; Alvarez-Pedrerol, M.; Rivas, I.; López-Vicente, M.; De Pascual, M.C.; Su, J.; et al. Green spaces and cognitive development in primary schoolchildren. Proc. Natl. Acad. Sci. USA 2015, 112, 7937–7942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Economic Situation and Prospects (WESP) 2017 | Multimedia Library—United Nations Department of Economic and Social Affairs. Available online: https://www.un.org/development/desa/publications/world-economic-situation-and-prospects-wesp-2017.html (accessed on 16 April 2020).
- Labib, S.M.; Lindley, S.; Huck, J.J. Spatial dimensions of the influence of urban green-blue spaces on human health: A systematic review. Environ. Res. 2020, 180, 108869. [Google Scholar] [CrossRef] [PubMed]
- Cleland, C.; Reis, R.S.; Ferreira Hino, A.A.; Hunter, R.; Fermino, R.C.; de Paiva, H.K.; Czestschuk, B.; Ellis, G. Built environment correlates of physical activity and sedentary behaviour in older adults: A comparative review between high and low-middle income countries. Heal. Place 2019, 57, 277–304. [Google Scholar] [CrossRef]
- Schetke, S.; Qureshi, S.; Lautenbach, S.; Kabisch, N. What determines the use of urban green spaces in highly urbanized areas? - Examples from two fast growing Asian cities. Urban For. Urban Green. 2016, 16, 150–159. [Google Scholar] [CrossRef]
- Van Cauwenberg, J.; Nathan, A.; Barnett, A.; Barnett, D.W.; Cerin, E. Relationships Between Neighbourhood Physical Environmental Attributes and Older Adults’ Leisure-Time Physical Activity: A Systematic Review and Meta-Analysis. Sport. Med. 2018, 48, 1635–1660. [Google Scholar] [CrossRef]
- Rigolon, A.; Browning, M.; Lee, K.; Shin, S. Access to Urban Green Space in Cities of the Global South: A Systematic Literature Review. Urban Sci. 2018, 2, 67. [Google Scholar] [CrossRef] [Green Version]
- Nagendra, H.; Bai, X.; Brondizio, E.S.; Lwasa, S. The urban south and the predicament of global sustainability. Nat. Sustain. 2018, 1, 341–349. [Google Scholar] [CrossRef]
- Braimoh, A.K.; Onishi, T. Spatial determinants of urban land use change in Lagos, Nigeria. Land Use Policy 2007, 24, 502–515. [Google Scholar] [CrossRef]
- Dewan, A.M.; Yamaguchi, Y. Land use and land cover change in Greater Dhaka, Bangladesh: Using remote sensing to promote sustainable urbanization. Appl. Geogr. 2009, 29, 390–401. [Google Scholar] [CrossRef]
- Zérah, M.H. Conflict between green space preservation and housing needs: The case of the Sanjay Gandhi National Park in Mumbai. Cities 2007, 24, 122–132. [Google Scholar] [CrossRef]
- Ahmed, B.; Ahmed, R. Modeling urban land cover growth dynamics using multioral satellite images: A case study of Dhaka, Bangladesh. ISPRS Int. J. Geo-Inf. 2012, 1, 3–31. [Google Scholar] [CrossRef] [Green Version]
- Labib, S.M.; Neema, M.N.; Rahaman, Z.; Patwary, S.H.; Shakil, S.H. Carbon dioxide emission and bio-capacity indexing for transportation activities: A methodological development in determining the sustainability of vehicular transportation systems. J. Environ. Manag. 2018, 223, 57–73. [Google Scholar] [CrossRef] [Green Version]
- McCormack, G.R.; Rock, M.; Toohey, A.M.; Hignell, D. Characteristics of urban parks associated with park use and physical activity: A review of qualitative research. Heal. Place 2010, 16, 712–726. [Google Scholar] [CrossRef]
- Wang, D.; Brown, G.; Zhong, G.; Liu, Y.; Mateo-Babiano, I. Factors influencing perceived access to urban parks: A comparative study of Brisbane (Australia) and Zhongshan (China). Habitat Int. 2015, 50, 335–346. [Google Scholar] [CrossRef]
- Zhang, W.; Yang, J.; Ma, L.; Huang, C. Factors affecting the use of urban green spaces for physical activities: Views of young urban residents in Beijing. Urban For. Urban Green. 2015, 14, 851–857. [Google Scholar] [CrossRef]
- Razani, N.; Morshed, S.; Kohn, M.A.; Wells, N.M.; Thompson, D.; Alqassari, M.; Agodi, A.; Rutherford, G.W. Effect of park prescriptions with and without group visits to parks on stress reduction in low-income parents: SHINE randomized trial. PLoS ONE 2018, 13, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schipperijn, J.; Cerin, E.; Adams, M.A.; Reis, R.; Smith, G.; Cain, K.; Christiansen, L.B.; Dyck, D.; van Gidlow, C.; Frank, L.D.; et al. Access to parks and physical activity: An eight country comparison. Urban For. Urban Green. 2017, 27, 253–263. [Google Scholar] [CrossRef]
- Müller-Riemenschneider, F.; Petrunoff, N.; Yao, J.; Ng, A.; Sia, A.; Ramiah, A.; Wong, M.; Han, J.; Tai, B.C.; Uijtdewilligen, L. Effectiveness of prescribing physical activity in parks to improve health and wellbeing-the park prescription randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Yigitcanlar, T.; Kamruzzaman, M.; Teimouri, R.; Degirmenci, K.; Alanjagh, F. Association between park visits and mental health in a developing country context: The case of Tabriz, Iran. Landsc. Urban Plan. 2020, 199, 103805. [Google Scholar] [CrossRef]
- Nath, T.K.; Zhe Han, S.S.; Lechner, A.M. Urban green space and well-being in Kuala Lumpur, Malaysia. Urban For. Urban Green. 2018, 36, 34–41. [Google Scholar] [CrossRef]
- Gaikwad, A.; Shinde, K. Use of parks by older persons and perceived health benefits: A developing country context. Cities 2019, 84, 134–142. [Google Scholar] [CrossRef]
- Patel, A.; Schofield, G.M.; Kolt, G.S.; Keogh, J.W. General practitioners’ views and experiences of counselling for physical activity through the New Zealand Green Prescription program. BMC Fam. Pract. 2011, 12, 119. [Google Scholar] [CrossRef] [Green Version]
- Sefcik, J.S.; Kondo, M.C.; Klusaritz, H.; Sarantschin, E.; Solomon, S.; Roepke, A.; South, E.C.; Jacoby, S.F. Perceptions of nature and access to green space in four urban neighborhoods. Int. J. Environ. Res. Public Health 2019, 16, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Razani, N.; Hills, N.K.; Thompson, D.; Rutherford, G.W. The association of knowledge, attitudes and access with park use before and after a park-prescription intervention for low-income families in the U.S. Int. J. Environ. Res. Public Health 2020, 17, 701. [Google Scholar] [CrossRef] [Green Version]
- Seltenrich, N. Just What the Doctor Ordered: Using Parks to Improve Children’s Health. Environ. Health Perspect. 2015, 123, A255–A259. [Google Scholar] [CrossRef] [Green Version]
- James, J.J.; Christiana, R.W.; Battista, R.A. A historical and critical analysis of park prescriptions. J. Leis. Res. 2019, 50, 311–329. [Google Scholar] [CrossRef]
- Robinson, J.; Breed, M. Green Prescriptions and Their Co-Benefits: Integrative Strategies for Public and Environmental Health. Challenges 2019, 10, 9. [Google Scholar] [CrossRef] [Green Version]
- Mnich, C.; Weyland, S.; Jekauc, D.; Schipperijn, J. Psychosocial and physiological health outcomes of green exercise in children and adolescents—A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 4266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crnic, M.; Kondo, M.C. Nature RX: Reemergence of pediatric nature-based therapeutic programs from the late 19th and early 20th centuries. Am. J. Public Health 2019, 109, 1371–1378. [Google Scholar] [CrossRef] [PubMed]
- Zarr, R.; Cottrell, L.; Merrill, C. Park prescription (DC Park Rx): A new strategy to combat chronic disease in children. J. Phys. Act. Heal. 2017, 14, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Razani, N.; Niknam, K.; Wells, N.M.; Thompson, D.; Hills, N.K.; Kennedy, G.; Gilgoff, R.; Rutherford, G.W. Clinic and park partnerships for childhood resilience: A prospective study of park prescriptions. Heal. Place 2019, 57, 179–185. [Google Scholar] [CrossRef]
- BBC “Nature” Being Prescribed by GPs in Shetland—BBC News. Available online: https://www.bbc.co.uk/news/uk-scotland-north-east-orkney-shetland-45758016 (accessed on 16 April 2020).
- Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 15 April 2020).
- Ghaffar, A.; Reddy, K.S.; Singhi, M. Burden of non-communicable diseases in South Asia. BMJ 2002, 325, 475. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.; Nahiduzzaman, K.M.; Hasan, M.M.U. Dhaka, Bangladesh: Unpacking challenges and reflecting on unjust transitions. Cities 2018, 77, 142–157. [Google Scholar] [CrossRef]
- Labib, S.M.; Harris, A. The potentials of Sentinel−2 and LandSat−8 data in green infrastructure extraction, using object based image analysis (OBIA) method. Eur. J. Remote Sens. 2018, 51, 231–240. [Google Scholar] [CrossRef]
- Kumar, P.; Druckman, A.; Gallagher, J.; Gatersleben, B.; Allison, S.; Eisenman, T.S.; Hoang, U.; Hama, S.; Tiwari, A.; Sharma, A.; et al. The nexus between air pollution, green infrastructure and human health. Environ. Int. 2019, 133, 105181. [Google Scholar] [CrossRef]
- Bloemsma, L.D.; Wijga, A.H.; Klompmaker, J.O.; Janssen, N.A.H.; Smit, H.A.; Koppelman, G.H.; Brunekreef, B.; Lebret, E.; Hoek, G.; Gehring, U. The associations of air pollution, traffic noise and green space with overweight throughout childhood: The PIAMA birth cohort study. Environ. Res. 2019, 169, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Labib, S.M.; Mohiuddin, H.; Hasib, I.M.A.; Sabuj, S.H.; Hira, S. Integrating Data Mining and Microsimulation Modelling to Reduce Traffic Congestion: A Case Study of Signalized Intersections in Dhaka, Bangladesh. Urban Sci. 2019, 3, 41. [Google Scholar] [CrossRef] [Green Version]
- Rahman, K.M.A.; Zhang, D. Analyzing the level of accessibility of public urban green spaces to different socially vulnerable groups of people. Sustain. 2018, 10, 3917. [Google Scholar] [CrossRef] [Green Version]
- Labib, S.M. Volunteer GIS (VGIS) Based Waste Management A conceptual design and use of Web 2.0 for Smart Waste Management in Dhaka City. In Third International Conference on Research in Computational Intelligence and Communication Networks (ICRCICN); IEEE: Kolkata, India, 2017; pp. 137–141. [Google Scholar]
- Byomkesh, T.; Nakagoshi, N.; Dewan, A.M. Urbanization and green space dynamics in Greater Dhaka, Bangladesh. Landsc. Ecol. Eng. 2012, 8, 45–58. [Google Scholar] [CrossRef]
- About Parks: NYC Parks. Available online: https://www.nycgovparks.org/about (accessed on 16 April 2020).
- Comber, A.; Brunsdon, C.; Green, E. Using a GIS-based network analysis to determine urban greenspace accessibility for different ethnic and religious groups. Landsc. Urban Plan. 2008, 86, 103–114. [Google Scholar] [CrossRef] [Green Version]
- 10minutewalk | The Trust for Public Land. Available online: https://www.tpl.org/10minutewalk (accessed on 8 April 2020).
- Tabassum, S.; Sharmin, F. Accessibility Analysis of Parks at Urban Neighborhood: The Case of Dhaka; Asian Journal of Applied Science and Engineering: Dhaka, Bangladesh, 2013; Volume 2. [Google Scholar]
- Shanahan, D.F.; Bush, R.; Gaston, K.J.; Lin, B.B.; Dean, J.; Barber, E.; Fuller, R.A. Health Benefits from Nature Experiences Depend on Dose. Sci. Rep. 2016, 6, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Cleary, A.; Roiko, A.; Burton, N.W.; Fielding, K.S.; Murray, Z.; Turrell, G. Changes in perceptions of urban green space are related to changes in psychological well-being: Cross-sectional and longitudinal study of mid-aged urban residents. Heal. Place 2019, 59, 102201. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Mental health benefits of neighbourhood green space are stronger among physically active adults in middle-to-older age: Evidence from 260,061 Australians. Prev. Med. 2013, 57, 601–606. [Google Scholar] [CrossRef]
- Hunter, R.F.; Christian, H.; Veitch, J.; Astell-Burt, T.; Hipp, J.A.; Schipperijn, J. The impact of interventions to promote physical activity in urban green space: A systematic review and recommendations for future research. Soc. Sci. Med. 2015, 124, 246–256. [Google Scholar] [CrossRef] [Green Version]
- Akpinar, A. How is quality of urban green spaces associated with physical activity and health? Urban For. Urban Green. 2016, 16, 76–83. [Google Scholar] [CrossRef]
- Shuvo, F.K. Do the Features of Urban Green Spaces that Promote Social and Active Ageing Vary by International Context? Comparison between and within Sydney, Dhaka and Singapore; University of Wollongong: Wollongong, Australia, 2020. [Google Scholar]
- Khan, M. Study of Open Spaces in the Context of Dhaka City for Sustainable Use: A Syntactic Approach. Int. J. Eng. Technol. 2014, 6, 238–243. [Google Scholar] [CrossRef] [Green Version]
- Siddiqui, N.I.; Nessa, A.; Hossain, M.A. Regular physical exercise: Way to healthy life. Mymensingh Med. J. 2010, 19, 154–158. [Google Scholar] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The physical activity guidelines for Americans. JAMA J. Am. Med. Assoc. 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- JMR, G.; AR, C. Physical activity and prevention of type 2 diabetes mellitus. Sport. Med. 2008, 38, 807–824. [Google Scholar]
- Hillsdon, M.; Panter, J.; Foster, C.; Jones, A. The relationship between access and quality of urban green space with population physical activity. Public Health 2006, 120, 1127–1132. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Broomhall, M.H.; Knuiman, M.; Collins, C.; Douglas, K.; Ng, K.; Lange, A.; Donovan, R.J. Increasing walking: How important is distance to, attractiveness, and size of public open space? Am. J. Prev. Med. 2005, 28, 169–176. [Google Scholar] [CrossRef]
- Sugiyama, T.; Francis, J.; Middleton, N.J.; Owen, N.; Giles-CortI, B. Associations between recreational walking and attractiveness, size, and proximity of neighborhood open spaces. Am. J. Public Health 2010, 100, 1752–1757. [Google Scholar] [CrossRef]
- Koohsari, M.J.; Kaczynski, A.T.; Giles-Corti, B.; Karakiewicz, J.A. Effects of access to public open spaces on walking: Is proximity enough? Landsc. Urban Plan. 2013, 117, 92–99. [Google Scholar] [CrossRef]
- Brindley, P.; Cameron, R.W.; Ersoy, E.; Jorgensen, A.; Maheswaran, R. Is more always better? Exploring field survey and social media indicators of quality of urban greenspace, in relation to health. Urban For. Urban Green. 2019, 39, 45–54. [Google Scholar] [CrossRef]
- Ekkel, E.D.; de Vries, S. Nearby green space and human health: Evaluating accessibility metrics. Landsc. Urban Plan. 2017, 157, 214–220. [Google Scholar] [CrossRef]
- Kaczynski, A.T.; Besenyi, G.M.; Stanis, S.W.A.; Koohsari, M.J.; Oestman, K.B.; Bergstrom, R.; Potwarka, L.R.; Reis, R.S. Are park proximity and park features related to park use and park-based physical activity among adults? Variations by multiple socio-demographic characteristics. Int. J. Behav. Nutr. Phys. Act. 2014, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shwe Zin Nyunt, M.; Shuvo, F.K.; Yen Eng, J.; Bee Yap, K.; Scherer, S.; Min Hee, L.; Pang Chan, S.; Pin Ng, T. Objective and subjective measures of neighborhood environment (NE): Relationships with transportation physical activity among older persons. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giles-Corti, B.; Donovan, R.J. Socioeconomic status differences in recreational physical activity levels and real and perceived access to a supportive physical environment. Prev. Med. 2002, 35, 601–611. [Google Scholar] [CrossRef] [PubMed]
- Hoehner, C.M.; Brennan Ramirez, L.K.; Elliott, M.B.; Handy, S.L.; Brownson, R.C. Perceived and objective environmental measures and physical activity among urban adults. Am. J. Prev. Med. 2005, 28, 105–116. [Google Scholar] [CrossRef]
- Cerin, E.; Leslie, E.; Owen, N.; Bauman, A. An Australian version of the neighborhood environment walkability scale: Validity evidence. Meas. Phys. Educ. Exerc. Sci. 2008, 12, 31–51. [Google Scholar] [CrossRef]
- Lee, T.H.; Shen, Y.L. The influence of leisure involvement and place attachment on destination loyalty: Evidence from recreationists walking their dogs in urban parks. J. Environ. Psychol. 2013, 33, 76–85. [Google Scholar] [CrossRef]
- Lewicka, M. Place attachment: How far have we come in the last 40 years? J. Environ. Psychol. 2011, 31, 207–230. [Google Scholar] [CrossRef]
- Clark, W.A.V.; Duque-Calvache, R.; Palomares-Linares, I. Place Attachment and the Decision to Stay in the Neighbourhood. Popul. Space Place 2017, 23, e2001. [Google Scholar] [CrossRef]
- Ryan, R.L. The role of place attachment in sustaining urban parks. In The Humane Metropolis: People and Nature in the 21st-Century City; Lincoln Institute of Land Policy: Cambridge, MA, USA, 2006; pp. 61–74. [Google Scholar]
- Lewicka, M. Ways to make people active: The role of place attachment, cultural capital, and neighborhood ties. J. Environ. Psychol. 2005, 25, 381–395. [Google Scholar] [CrossRef]
- Arnberger, A.; Eder, R. The influence of green space on community attachment of urban and suburban residents. Urban For. Urban Green. 2012, 11, 41–49. [Google Scholar] [CrossRef]
- Budruk, M.; Thomas, H.; Tyrrell, T. Urban green spaces: A study of place attachment and environmental attitudes in India. Soc. Nat. Resour. 2009, 22, 824–839. [Google Scholar] [CrossRef]
- Triguero-Mas, M.; Donaire-Gonzalez, D.; Seto, E.; Valentín, A.; Smith, G.; Martínez, D.; Carrasco-Turigas, G.; Masterson, D.; van den Berg, M.; Ambròs, A.; et al. Living close to natural outdoor environments in four European cities: Adults’ contact with the environments and physical activity. Int. J. Environ. Res. Public Health 2017, 14, 1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maas, J.; Verheij, R.A.; Groenewegen, P.P.; De Vries, S.; Spreeuwenberg, P. Green space, urbanity, and health: How strong is the relation? J. Epidemiol. Commun. Health 2006, 60, 587–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO (World Health Organization). Noncommunicable Diseases. Available online: http://www.searo.who.int/bangladesh/noncommunicable-diseases/en/ (accessed on 30 November 2019).
- Chowdhury, M.A.B.; Uddin, M.J.; Haque, M.R.; Ibrahimou, B. Hypertension among adults in Bangladesh: Evidence from a national cross-sectional survey. BMC Cardiovasc. Disord. 2016, 16, 22. [Google Scholar] [CrossRef] [Green Version]
- Biswas, T.; Pervin, S.; Tanim, M.I.A.; Niessen, L.; Islam, A. Bangladesh policy on prevention and control of non-communicable diseases: A policy analysis. BMC Public Health 2017, 17, 582. [Google Scholar] [CrossRef] [Green Version]
- Zaman, M.M.; Rahman, M.M.; Rahman, M.R.; Bhuiyan, M.R.; Karim, M.N.; Chowdhury, M.A.J. Prevalence of risk factors for non-communicable diseases in Bangladesh: Results from STEPS survey 2010. Indian J. Public Health 2016, 60, 17–25. [Google Scholar] [CrossRef]
- Diabetic Association of Bangladesh Diabetic Association of Bangladesh-Magazine Kanti. Available online: https://www.dab-bd.org/kanti.php (accessed on 16 April 2020).
- Mendenhall, E.; Kohrt, B.A.; Norris, S.A.; Ndetei, D.; Prabhakaran, D. Non-communicable disease syndemics: Poverty, depression, and diabetes among low-income populations. Lancet 2017, 389, 951–963. [Google Scholar] [CrossRef] [Green Version]
- Pfeiffer, B.A.; Clay, S.W.; Conatser, R.R. A Green Prescription Study. J. Aging Health 2001, 13, 527–538. [Google Scholar] [CrossRef]
- Browning, M.; Lee, K. Within what distance does “greenness” best predict physical health? A systematic review of articles with gis buffer analyses across the lifespan. Int. J. Environ. Res. Public Health 2017, 14, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Ripley, B.; Bill, V.; Douglas, M.; Bates, K.H.; Albrecht, G.; David Firth, M.B.R. Package “MASS”. 2013. Available online: ftp://192.218.129.11/pub/CRAN/web/packages/MASS/MASS (accessed on 16 April 2020).
- Fox, J.; Weisberg, S.; Adler, D.; Bates, D.; Baud-Bovy, G.; Ellison, S.; Firth, D.; Friendly, M.; Gorjanc, G.; Graves, S.; et al. Package ‘Car’. 2016. Available online: https://cran.microsoft.com/snapshot/2017-06-17/web/packages/car/car (accessed on 16 April 2020).
- Tingley, D.; Yamamoto, T.; Hirose, K.; Keele, L.; Imai, K. Mediation: R package for causal mediation analysis. J. Stat. Softw. 2014, 59, 1–38. [Google Scholar] [CrossRef] [Green Version]
- Dzhambov, A.M.; Browning, M.H.; Markevych, I.; Hartig, T.; Lercher, P. Analytical approaches to testing pathways linking greenspace to health: A scoping review of the empirical literature. Environ. Res. 2020, 186, 109613. [Google Scholar] [CrossRef]
- Imai, K.; Keele, L.; Tingley, D. A General Approach to Causal Mediation Analysis. Psychol. Methods 2010, 15, 309–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klompmaker, J.O.; Janssen, N.A.H.; Bloemsma, L.D.; Gehring, U.; Wijga, A.H.; Brink, C.; Van den Lebret, E.; Brunekreef, B.; Hoek, G. Associations of combined exposures to surrounding green, air pollution, and road traffic noise with cardiometabolic diseases. Environ. Health Perspect. 2019, 127, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quddus, M.; Rahman, F.; Monsuur, F.; de Ona, J.; Enoch, M. Analyzing Bus Passengers’ Satisfaction in Dhaka using Discrete Choice Models. Transp. Res. Rec. J. Transp. Res. Board 2019, 2673, 758–768. [Google Scholar] [CrossRef]
- Labib, S.M.; Mohiuddin, H.; Shakil, S.H. Transport Sustainability of Dhaka: A Measure of Ecological Footprint and Means for Sustainable Transportation System. J. Bangladesh Inst. Planners 2013, 6, 137–147. [Google Scholar]
- Klompmaker, J.O.; Hoek, G.; Bloemsma, L.D.; Gehring, U.; Strak, M.; Wijga, A.H.; van den Brink, C.; Brunekreef, B.; Lebret, E.; Janssen, N.A.H. Green space definition affects associations of green space with overweight and physical activity. Environ. Res. 2018, 160, 531–540. [Google Scholar] [CrossRef]
- Pietilä, M.; Neuvonen, M.; Borodulin, K.; Korpela, K.; Sievänen, T.; Tyrväinen, L. Relationships between exposure to urban green spaces, physical activity and self-rated health. J. Outdoor Recreat. Tour. 2015, 10, 44–54. [Google Scholar] [CrossRef]
- Shuvo, F.K.; Feng, X.; Akaraci, S.; Astell-Burt, T. Urban green space and health in low and middle-income countries: A critical review. Urban For. Urban Green. 2020, 52, 126662. [Google Scholar] [CrossRef]
- Jansen, M.; Kamphuis, C.B.M.; Pierik, F.H.; Ettema, D.F.; Dijst, M.J. Neighborhood-based PA and its environmental correlates: A GIS- and GPS based cross-sectional study in the Netherlands. BMC Public Health 2018, 18, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Broyles, S.T.; Mowen, A.J.; Theall, K.P.; Gustat, J.; Rung, A.L. Integrating social capital into a park-use and active-living framework. Am. J. Prev. Med. 2011, 40, 522–529. [Google Scholar] [CrossRef]
- Hong, A.; Sallis, J.F.; King, A.C.; Conway, T.L.; Saelens, B.; Cain, K.L.; Fox, E.H.; Frank, L.D. Linking green space to neighborhood social capital in older adults: The role of perceived safety. Soc. Sci. Med. 2018, 207, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Jennings, V.; Bamkole, O. The relationship between social cohesion and urban green space: An avenue for health promotion. Int. J. Environ. Res. Public Health 2019, 16, 452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reubi, D.; Herrick, C.; Brown, T. The politics of non-communicable diseases in the global South. Heal. Place 2016, 39, 179–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milà, C.; Ranzani, O.; Sanchez, M.; Ambrós, A.; Bhogadi, S.; Kinra, S.; Kogevinas, M.; Dadvand, P.; Tonne, C. Land-Use Change and Cardiometabolic Risk Factors in an Urbanizing Area of South India: A Population-Based Cohort Study. Environ. Health Perspect. 2020, 128, 047003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieuwenhuijsen, M.J.; Khreis, H.; Triguero-Mas, M.; Gascon, M.; Dadvand, P. Fifty shades of green. Epidemiology 2017, 28, 63–71. [Google Scholar] [CrossRef]
- Shuvo, F.K.; Hakim, S.S. A Proposed Framework for Regenerating Urban Green in Dhaka City. J. Bangladesh Inst. Planners 2013, 6, 13–22. [Google Scholar]
- Sultana, R.; Birtchnell, T.; Gill, N. Urban greening and mobility justice in Dhaka’s informal settlements. Mobilities 2020, 15, 273–289. [Google Scholar] [CrossRef]
- Nahar, K. Park-Playground Project: DSCC Revises Up Cost, Extends Tenure. The Financial Express. 2019. Available online: https://www.thefinancialexpress.com.bd/national/park-playground-project-dscc-revises-up-cost-extends-tenure-1559535808 (accessed on 16 April 2020).
- The World Bank Bangladesh-Dhaka City Neighborhood Upgrading Project: A More Liveable Dhaka City (English) The World Bank. Available online: http://documents.worldbank.org/curated/en/382111568359904697/Bangladesh-Dhaka-City-Neighborhood-Upgrading-Project-A-More-Liveable-Dhaka-City (accessed on 16 April 2020).
- Rigolon, A.; Browning, M.; Jennings, V. Inequities in the quality of urban park systems: An environmental justice investigation of cities in the United States. Landsc. Urban Plan. 2018, 178, 156–169. [Google Scholar] [CrossRef]
- Wolch, J.R.; Byrne, J.; Newell, J.P. Urban green space, public health, and environmental justice: The challenge of making cities “just green enough”. Landsc. Urban Plan. 2014, 125, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Rigolon, A.; Németh, J. “We’re not in the business of housing:” Environmental gentrification and the nonprofitization of green infrastructure projects. Cities 2018, 81, 71–80. [Google Scholar] [CrossRef]
- Hartig, T.; Mitchell, R.; de Vries, S.; Frumkin, H. Nature and Health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, D.A.; Browning, M.H.E.M.; Kuo, M.; Van Den Eeden, S.K. Is green land cover associated with less health care spending? Promising findings from county-level Medicare spending in the continental United States. Urban For. Urban Green. 2019, 41, 39–47. [Google Scholar] [CrossRef]
- Buckley, R.; Brough, P.; Hague, L.; Chauvenet, A.; Fleming, C.; Roche, E.; Sofija, E.; Harris, N. Economic value of protected areas via visitor mental health. Nat. Commun. 2019, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chen, X. Monetary valuation of urban nature’s health effects: A systematic review. J. Environ. Plan. Manag. 2020. [Google Scholar] [CrossRef]
| Frequency | |||
|---|---|---|---|
| Duration | Low | High | |
| Low | Low-frequency low-duration | High-frequency low-duration | |
| High | Low-frequency high-duration | High-frequency high-duration | |
| Attribute | Categories | Total Sample, 169 | |
|---|---|---|---|
| N | Percentage | ||
| Gender | Female | 65 | 38.5 |
| Male | 104 | 61.5 | |
| Education | None | 52 | 30.8 |
| Secondary School | 42 | 24.9 | |
| Higher Secondary School | 28 | 16.6 | |
| Bachelors | 11 | 6.5 | |
| Post-Graduate (MSc/PhD) | 36 | 21.2 | |
| Employment | Unemployed | 57 | 33.7 |
| Retired | 14 | 8.3 | |
| Employed | 98 | 58 | |
| Travel Mode | Walk | 134 | 79.3 |
| Bicycle or motorcycle | 10 | 5.9 | |
| Public transport (e.g., bus) | 14 | 8.3 | |
| Private vehicle | 6 | 3.6 | |
| Others (e.g., rickshaw) | 5 | 3.0 | |
| NCDs | No | 50 | 29.6 |
| Yes | 119 | 70.4 | |
| Park prescription (ParkRx) | No | 81 | 47.9 |
| Yes | 88 | 52.1 | |
| Measurements | Categories | N | Percentage |
|---|---|---|---|
| Perceived distance (accessibility) | Less than 5 min | 11 | 6.5 |
| 5 to 10 min | 67 | 39.6 | |
| 11 to 15 min | 45 | 26.6 | |
| 16 to 20 min | 31 | 18.3 | |
| More than 20 min | 15 | 8.9 | |
| Perceived attractiveness | Very low | 14 | 8.3 |
| Low | 44 | 26.0 | |
| Moderate | 47 | 27.8 | |
| High | 31 | 18.3 | |
| Very high | 33 | 19.5 | |
| Years using the green space (attachment) | <=1 year | 74 | 43.8 |
| 2−3 years | 47 | 27.8 | |
| 3−4 years | 29 | 17.2 | |
| 4−5 years | 7 | 4.1 | |
| >5 years | 12 | 7.1 | |
| Visit frequency (usual week) | Less or equal 4 days | 46 | 27.2 |
| More than 5 days | 123 | 72.8 | |
| Visit duration (min/visit on average) | Less than 30 min | 99 | 58.6 |
| More than 30 min | 70 | 41.4 | |
| Use intensity (omnibus measure from frequency and duration values) | Low | 111 | 65.7 |
| High | 58 | 34.3 |
| ParkRx | |||||
| No | Yes | Total Count | |||
| Do you have NCDs/chronic health issue(s)? | No | Count | 48 | 2 | 50 |
| % within NCDs | 96.0% | 4.0% | |||
| % within ParkRx | 59.3% | 2.3% | |||
| Yes | Count | 33 | 86 | 119 | |
| % within NCDs | 27.7% | 72.3% | |||
| % within ParkRx | 40.7% | 97.7% | |||
| Total Count | 81 | 88 | 169 | ||
| Green Space ‘Use Intensity’ | |||||
| Low | High | Total Count | |||
| Do you have NCDs/chronic health issue(s)? | No | Count | 40 | 10 | 50 |
| % within NCDs | 80.0% | 20.0% | |||
| % within use Intensity | 36.0% | 17.2% | |||
| Yes | Count | 71 | 48 | 119 | |
| % within NCDs | 59.7% | 40.3% | |||
| % within use Intensity | 64.0% | 82.8% | |||
| Total Count | 111 | 58 | 169 | ||
| Model 1 | Model 2 | Model 3 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Odds | 95% CI | p-value | Odds | 95% CI | p-value | Odds | 95% CI | p-value | |||
| Attractiveness | 0.712 | 0.52–0.959 | 0.0288 | 0.713 | 0.518–0.965 | 0.032 | 0.735 | 0.524–1.015 | 0.0667 | ||
| Accessibility | 0.824 | 0.568–1.187 | 0.3015 | 0.795 | 0.542–1.156 | 0.2327 | 0.75 | 0.501–1.108 | 0.1531 | ||
| Attachment | 2.095 | 1.528–2.972 | 0.0000114 | 2.004 | 1.453–2.851 | 0.0000469 | 2.08 | 1.486–3.013 | 0.0000429 | ||
| Green space per capita | 1.032 | 0.974–1.212 | 0.404 | 1.028 | 0.95–1.109 | 0.4719 | 1.011 | 0.93–1.095 | 0.775 | ||
| NCDs | - | - | 2.821 | 1.148–7.573 | 0.0296 | - | - | - | |||
| ParkRx | - | - | - | - | 6.328 | 2.706–16.075 | 0.0000438 | ||||
| Constant | 0.292 | 0.025–3.135 | 0.3147 | 0.119 | 0.008–1.512 | 0.1077 | 0.048 | 0.003–0.667 | 0.0264 | ||
| Pseudo R2 | 0.228 | 0.263 | 0.353 | ||||||||
| AIC | 204.86 | 201.68 | 187.42 | ||||||||
| Estimate | 95% CI Lower | 95% CI Upper | p-Value | |
|---|---|---|---|---|
| ACME (average) | 0.192 | 0.0696 | 0.32 | 0.002 |
| ADE (average) | −0.042 | −0.2583 | 0.19 | 0.712 |
| Total Effect | 0.15 | −0.028 | 0.31 | 0.076 |
| Prop. Mediated | 1.228 | −2.3953 | 8.1 | 0.078 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Labib, S.M.; Shuvo, F.K.; H. E. M. Browning, M.; Rigolon, A. Noncommunicable Diseases, Park Prescriptions, and Urban Green Space Use Patterns in a Global South Context: The Case of Dhaka, Bangladesh. Int. J. Environ. Res. Public Health 2020, 17, 3900. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113900
Labib SM, Shuvo FK, H. E. M. Browning M, Rigolon A. Noncommunicable Diseases, Park Prescriptions, and Urban Green Space Use Patterns in a Global South Context: The Case of Dhaka, Bangladesh. International Journal of Environmental Research and Public Health. 2020; 17(11):3900. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113900
Chicago/Turabian StyleLabib, S.M., Faysal Kabir Shuvo, Matthew H. E. M. Browning, and Alessandro Rigolon. 2020. "Noncommunicable Diseases, Park Prescriptions, and Urban Green Space Use Patterns in a Global South Context: The Case of Dhaka, Bangladesh" International Journal of Environmental Research and Public Health 17, no. 11: 3900. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113900