Estimated Cardiorespiratory Fitness Attenuates the Impacts of Sarcopenia and Obesity on Non-Alcoholic Fatty Liver in Korean Adults


Abstract
:1. Introduction
2. Materials and Methods
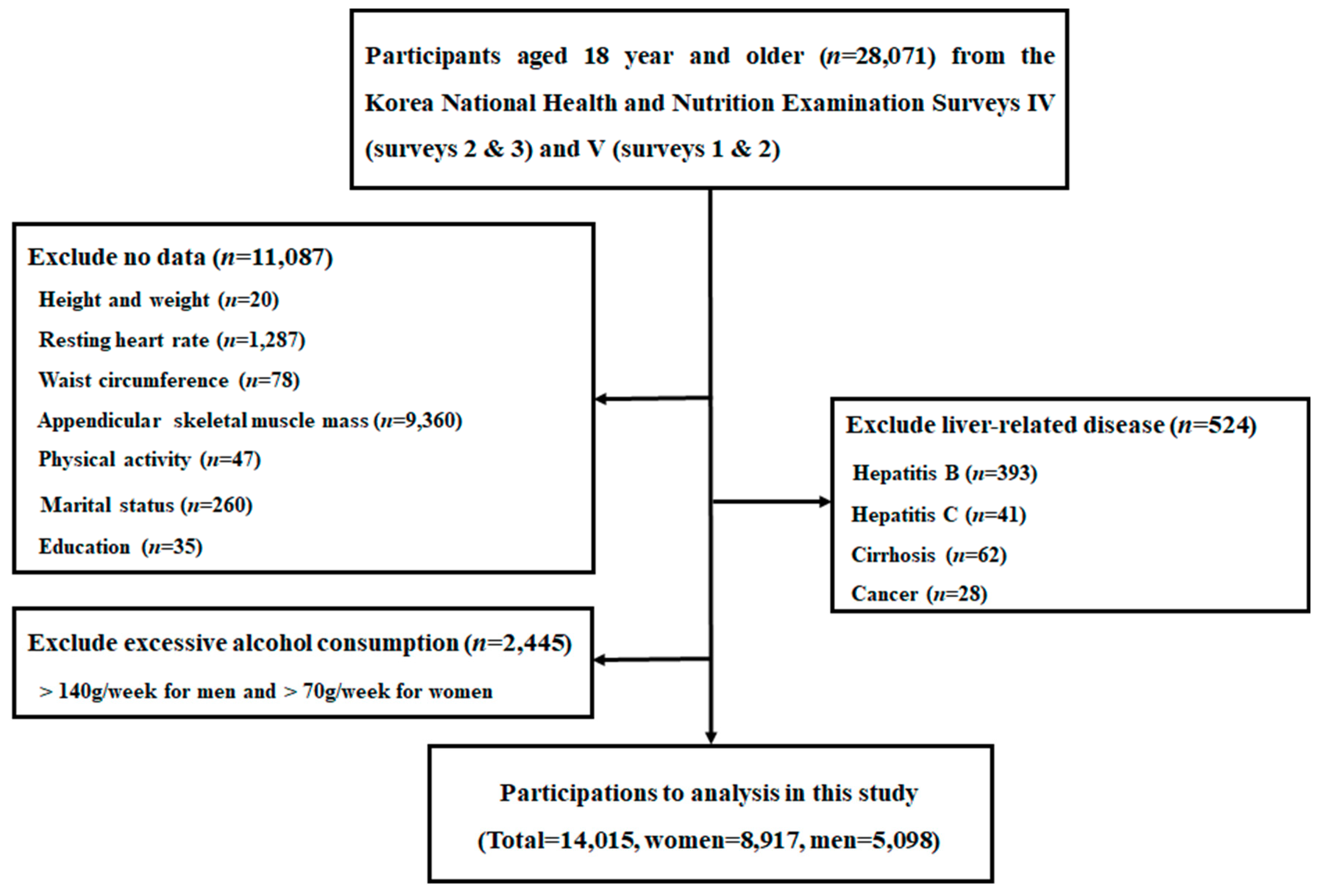
2.1. Data Source and Study Participants
2.2. Study Variables
2.2.1. Definition of Obesity and Sarcopenia
2.2.2. Calculation of eCRF
2.2.3. Definition of Hepatic Steatosis
2.2.4. Clinical and Laboratory Measurements
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CRF | cardiorespiratory fitness |
| eCRF | estimated cardiorespiratory fitness |
| WC | waist circumference |
| WHR | waist-to-hip ratio |
| BMI | body mass index |
| OR | odds ratio |
| CI | confidence interval |
| NAFLD | non-alcoholic fatty liver disease |
| NAFL | non-alcoholic fatty liver disease |
| NASH | non-alcoholic |
| CVDs | cardiovascular diseases |
| KNHNES | Korea National Health and Nutrition Examination Surveys |
| ASM | Appendic ular skeletal muscle mass |
| SMI | skeletal muscle index |
| DEXA | dual energy X-ray absorptiometry |
| METs | metabolic equivalents |
| NAFLD-LFS | NAFLD liver fat score |
| HSI | hepatic steatosis index |
| Mets | metabolic syndrome |
| RHR | resting heart rate |
| SBP | systolic blood pressure |
| DBP | diastolic blood pressure |
| TC | total cholesterol |
| TG | triglycerides |
| HDLC | high-density lipoprotein cholesterol |
| FBG | fasting blood glucose |
| ALT | alanine aminotransferase |
| AST | aspartate aminotransferase |
| HOMA-IR | homeostasis model assessment of insulin resistance |
| GLM | glucose-lowering medications |
| LLM | lipid-lowering medications |
References
- Araújo, A.R.; Rosso, N.; Bedogni, G.; Tiribelli, C.; Bellentani, S. Global epidemiology of non-alcoholic fatty liver disease/non-alcoholic steatohepatitis: What we need in the future. Liver Int. 2018, 38, 47–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherif, Z.A.; Saeed, A.; Ghavimi, S.; Nouraie, S.M.; Laiyemo, A.O.; Brim, H.; Ashktorab, H. Global epidemiology of nonalcoholic fatty liver disease and prespectives on US minority populations. Dig. Dis. Sci. 2016, 61, 1214–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, J.G.; Kim, S.U.; Wong, V.W. New trends on obesity and NAFLD in Asia. J. Hepatol. 2017, 67, 862–873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younossi, Z.M. Non-alcoholic fatty liver disease—A global public health perspective. J. Hepatol. 2019, 70, 531–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballestri, S.; Zona, S.; Targher, G.; Romagnoli, D.; Baldelli, E.; Nascimbeni, F.; Roverato, A.; Guaraldi, G.; Lonardo, A. Nonalcoholic fatty liver disease is associated with an almost twofold increased risk of incident type 2 diabetes and metabolic syndrome. Evidence from a systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2016, 31, 936–944. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Do, K.; Brown, R.E.; Wharton, S.; Ardern, C.I.; Kuk, J.L. Association between cardiorespiratory fitness and metabolic risk factors in a population with mild to severe obesity. BMC Obes. 2018, 5, 5. [Google Scholar] [CrossRef]
- Lee, J.; Cho, Y.K.; Kang, Y.M.; Kim, H.S.; Jung, C.H.; Kim, H.K.; Park, J.Y.; Lee, W.J. The impact of NAFLD and waist circumference changes on diabetes development in prediabetes subjects. Sci. Rep. 2019, 9, 17258. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.Y.; Zmora, R.; Duval, S.; Chow, L.S.; Lloyd-Jones, D.M.; Schreiner, P.J. Cardiorespiratory fitness, adiposity, and heart rate variability: The coronary artery risk development in young adults study. Med. Sci. Sports Exerc. 2019, 51, 509–514. [Google Scholar] [CrossRef]
- Haufe, S.; Engeli, S.; Budziarek, P.; Utz, W.; Schulz-Menger, J.; Hermsdorf, M.; Wiesner, S.; Otto, C.; Haas, V.; de Greiff, A.; et al. Cardiorespiratory fitness and insulin sensitivity in overweight or obese subjects may be linked through intrahepatic lipid content. Diabetes 2010, 59, 1640–1647. [Google Scholar] [CrossRef] [Green Version]
- Madssen, E.; Skaug, E.A.; Wisløff, U.; Ellingsen, Ø.; Videm, V. Inflammation is strongly associated with cardiorespiratory fitness, sex, BMI, and the metabolic syndrome in a self-reported healthy population: HUNT3 fitness study. Mayo Clin. Proc. 2019, 94, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Wijarnpreecha, K.; Kim, D.; Raymond, P.; Scribani, M.; Ahmed, A. Associations between sarcopenia and nonalcoholic fatty liver disease and advanced fibrosis in the USA. Eur. J. Gastroenterol. Hepatol. 2019, 31, 1121–1128. [Google Scholar] [CrossRef] [PubMed]
- Peng, T.C.; Wu, L.W.; Chen, W.L.; Liaw, F.Y.; Chang, Y.W.; Kao, T.W. Nonalcoholic fatty liver disease and sarcopenia in a Western population (NHANES III): The importance of sarcopenia definition. Clin. Nutr. 2019, 38, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Lee, S.E.; Lee, Y.B.; Jun, J.E.; Ahn, J.; Bae, J.C.; Jin, S.M.; Hur, K.Y.; Jee, J.H.; Lee, M.K.; et al. Relationship between relative skeletal muscle mass and non-alcoholic fatty liver disease: A 7-year longitudinal study. Hepatology 2018, 86, 1755–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, B.; Kim, D.; Joo, S.; Kim, J.; Chang, M.; Kim, B.; Lee, K.; Kim, W. Sarcopenia is an independent risk factor for non-alcoholic steatohepatitis and significant fibrosis. J. Hepatol. 2017, 66, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Kim, S.U.; Song, K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Lee, B.W.; Kang, E.S.; Cha, B.S.; Han, K.H. Sarcopenia is associated with significant liver fibrosis independently of obesity and insulin resistance in nonalcoholic fatty liver disease: Nationwide surveys (KNHANES 2008-2011). Hepatology 2016, 63, 776–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merli, M.; Lattanzi, B.; Aprile, F. Sarcopenic obesity in fatty liver. Curr. Opin. Clin. Nutr. Metab. Care 2019, 22, 185–190. [Google Scholar] [CrossRef]
- Jeong, E.H.; Jun, D.W.; Cho, Y.K.; Choe, Y.G.; Ryu, S.; Lee, S.M.; Jang, E.C. Regional prevalence of non-alcoholic fatty liver disease in Seoul and Gyeonggi-do, Korea. Clin. Mol. Hepatol. 2013, 19, 266–272. [Google Scholar] [CrossRef]
- Kim, T.N.; Park, M.S.; Kim, Y.J.; Lee, E.J.; Kim, M.K.; Kim, J.M.; Ko, K.S.; Rhee, B.D.; Won, J.C. Association of low muscle mass and combined low muscle mass and visceral obesity with low cardiorespiratory fitness. PLoS ONE 2014, 9, e100118. [Google Scholar] [CrossRef] [Green Version]
- Jurca, R.; Jackson, A.S.; LaMonte, M.J.; Morrow, J.R., Jr.; Blair, S.N.; Wareham, N.J.; Haskell, W.L.; van Mechelen, W.; Church, T.S.; Jakicic, J.M.; et al. Assessing cardiorespiratory fitness without performing exercise testing. Am. J. Prev. Med. 2005, 29, 185–193. [Google Scholar] [CrossRef]
- Korean Centers for Disease Control and Prevention. Korea National Health and Nutrition Examination Surveys. Available online: http://knhanes.cdc.go.kr (accessed on 10 October 2019).
- Kweon, A.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirsa, A. Ethnic-specific criteria for classification of body mass index: A perspective for Asian Indians and American Diabetes Association Position Statement. Diabetes Technol. Ther. 2015, 17, 667–671. [Google Scholar]
- Sayer, A.A.; Syddall, H.; Martin, H.; Patel, H.; Baylis, D.; Cooper, C. The developmental origins of sarcopenia. J. Nutr. Health Aging 2008, 12, 427–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, C.S.; Massaro, J.M.; Hoffmann, U.; Pou, K.M.; Maurovich-Horvat, P.; Liu, C.Y.; Vasan, R.S.; Murabito, J.M.; Meigs, J.B.; Cupples, L.A.; et al. Abdominal visceral and subcutaneous adipose tissue compartments: Association with metabolic risk factors in the Framingham Heart Study. Circulation 2007, 116, 39–48. [Google Scholar] [CrossRef] [Green Version]
- Pouliot, M.C.; Després, J.P.; Lemieux, S.; Moorjani, S.; Bouchard, C.; Tremblay, A.; Nadeau, A.; Lupien, P.J. Waist circumference and abdominal sagittal diameter: Best simple anthropometric indexes of abdominal visceral adipose tissue accumulation and related cardiovascular risk in men and women. Am. J. Cardiol. 1994, 73, 460–468. [Google Scholar] [CrossRef]
- Cho, G.J.; Yoo, H.J.; Hwang, S.Y.; Choi, J.; Lee, K.M.; Choi, K.M.; Baik, S.H.; Han, S.W.; Kim, T. Differential relationship between waist circumference and mortality according to age, sex, and body mass index in Korean with age of 30–90 years; a nationwide health insurance database study. BMC Med. 2018, 16, 131. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.Y.; Park, H.S.; Kim, D.J.; Han, J.H.; Kim, S.M.; Cho, G.J.; Kim, D.Y.; Kwon, H.S.; Kim, S.R.; Lee, C.B.; et al. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res. Clin. Pract. 2007, 75, 72–80. [Google Scholar] [CrossRef]
- Lee, Y.H.; Jung, K.S.; Kim, S.U.; Yoon, H.J.; Yun, Y.J.; Lee, B.W.; Kang, E.S.; Han, K.H.; Lee, H.C.; Cha, B.S. Sarcopaenia is associated with NAFLD independently of obesity and insulin resistance: Nationwide surveys (KNHANES 2008-2011). J. Hepatol. 2015, 63, 486–493. [Google Scholar] [CrossRef]
- Ross, R.M.; Jackson, A.S. Exercise Concepts, Calculations, and Computer Applications; Benchmark Press: Carmel, IN, USA, 1990; pp. 95–109. [Google Scholar]
- Kotronen, A.; Peltonen, M.; Hakkarainen, A.; Sevastianova, K.; Bergholm, R.; Johansson, L.M.; Lundbom, N.; Rissanen, A.; Ridderstråle, M.; Groop, L.; et al. Prediction of non-alcoholic fatty liver disease and liver fat using metabolic and genetic factors. Gastroenterology 2009, 137, 865–872. [Google Scholar] [CrossRef]
- Grundy, S.M.; Brewer, H.B.; Cleeman, J.I.; Smith, S.C., Jr.; Lenfant, C. National Heart, Lung, and Blood Institute; American Heart Association. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Arterioscler. Thromb. Vasc. Biol. 2004, 24, e13–e18. [Google Scholar]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Jung, H.S.; Cho, J.; Zhang, Y.; Yun, K.E.; Lazo, M.; Pastor-Barriuso, R.; Ahn, J.; Kim, C.W.; Rampal, S.; et al. Metabolically healthy obesity and the development of nonalcoholic fatty liver disease. Am. J. Gastroenterol. 2016, 111, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.M.; Oh, S.W.; Hwang, S.S.; Lee, C.; Kwon, H.; Chung, G.E. Association of non-alcoholic fatty liver disease with components of metabolic syndrome according to body mass index in Korean adults. Am. J. Gastroenterol. 2012, 107, 1852–1858. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.C.; Hung, H.F.; Lu, C.W.; Chang, H.H.; Lee, L.T.; Huang, K.C. Association of non-alcoholic fatty liver disease with metabolic syndrome independently of central obesity and insulin resistance. Sci. Rep. 2016, 6, 27034. [Google Scholar] [CrossRef] [Green Version]
- Polyzos, S.A.; Kountouras, J.; Mantzoros, C.S. Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics. Metabolism 2019, 92, 82–97. [Google Scholar] [CrossRef]
- Lee, M.J.; Kim, E.H.; Bae, S.J.; Kim, G.A.; Park, S.W.; Choe, J.; Jung, C.H.; Lee, W.J.; Kim, H.K. Age-related decrease in skeletal muscle mass is an independent risk factor for incident nonalcoholic fatty liver disease: A 10-year retrospective cohort study. Gut Liver 2019, 13, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Cai, C.; Song, X.; Chen, Y.; Chen, X.; Yu, C. Relationship between relative skeletal muscle mass and nonalcoholic fatty liver disease: A systematic review and meta-analysis. Hepatol. Int. 2020, 14, 115–126. [Google Scholar] [CrossRef] [Green Version]
- Glass, O.K.; Radia, A.; Kraus, W.E.; Abdelmalek, M.F. Exercise Training as Treatment of Nonalcoholic Fatty Liver Disease. J. Funct. Morphol. Kinesiol. 2017, 2, 35. [Google Scholar] [CrossRef]
- Kantartzis, K.; Thamer, C.; Peter, A.; Machann, J.; Schick, F.; Schraml, C.; Konigsrainer, A.; Konigsrainer, I.; Krober, S.; Niess, A.; et al. High cardiorespiratory fitness is an independent predictor of the reduction in liver fat during a lifestyle intervention in non-alcoholic fatty liver disease. Gut 2009, 58, 1281–1288. [Google Scholar] [CrossRef]
- Pugh, C.J.; Sprung, V.S.; Jones, H.; Richardson, P.; Shojaee-Moradie, F.; Umpleby, A.M.; Green, D.J.; Cable, N.T.; Trenell, M.I.; Kemp, G.J.; et al. Exercise-induced improvements in liver fat and endothelial function are not sustained 12 months following cessation of exercise supervision in nonalcoholic fatty liver disease. Int. J. Obes. 2016, 40, 1927–1930. [Google Scholar] [CrossRef] [Green Version]
- Clarke, S.L.; Reaven, G.M.; Leonard, D.; Barlow, C.E.; Haskell, W.L.; Willis, B.L.; DeFina, L.; Knowles, J.W.; Maron, D.J. Cardiorespiratory fitness, body mass index, and markers of insulin resistance in apparently health women and men. Am. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Henningsen, J.; Rigbolt, K.T.; Blagoev, B.; Pedersen, B.K.; Kratchmarova, I. Dynamics of the skeletal muscle secretome during myoblast differentiation. Mol. Cell Proteomics 2010, 9, 2482–2496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wree, A.; Kahraman, A.; Gerken, G.; Canbay, A. Obesity affects the liver—The link between adipocytes and hepatocytes. Digestion 2011, 83, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Hadi, H.E.; Vincenzo, A.D.; Vettor, R.; Rossato, M. Cardio-metabolic disorders in non-alcoholic fatty liver disease. Int. J. Mol. Sci. 2019, 20, 2215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polyzos, S.A.; Margioris, A.N. Sarcopeni obesity. Hormones 2018, 7, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Fedchuk, L.; Nascimbeni, F.; Pais, R.; Charlotte, F.; Housset, C.; Ratziu, V.; LIDO Study Group. Performance and limitations of steatosis biomarkers in patients with nonalcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2014, 40, 1209–1222. [Google Scholar] [CrossRef]


{kind=link}
| Women (n = 8917) | Men (n = 5098) | Total (n = 14,015) | |
|---|---|---|---|
| Body fatness and fitness | |||
| Age (year) | 50.3 ± 16.2 | 49.7 ± 16.4 | 50.1 ± 16.3 |
| BMI (kg/m2) | 23.4 ± 3.4 | 23.9 ± 3.1 | 23.6 ± 3.3 |
| Body fat (%) | 33.0 ± 5.5 | 22.1 ± 5.5 | 29.1 ± 7.6 |
| WC (cm) | 78.8 ± 9.9 | 84.0 ± 9.0 | 80.7 ± 9.9 |
| SMI (%) | 26.9 ± 2.7 | 34.0 ± 3.0 | 29.5 ± 4.4 |
| RHR (beats/min) | 71.6 ± 9.3 | 70.0 ± 9.4 | 71.0 ± 9.3 |
| eCRF (METs) | 8.2 ± 2.2 | 11.2 ± 2.2 | 9.3 ± 2.7 |
| Socio-economic status | |||
| Income (10,000 won/month) | 345.2 ± 823.7 | 375.1 ± 1229.8 | 356.1 ± 990.9 |
| Marital status, n (%) | |||
| Married | 6308 (70.7) | 4055 (79.5) | 10,363 (73.9) |
| Widow/divorced | 1742 (19.6) | 232 (4.6) | 1974 (14.1) |
| Unmarried | 867 (9.7) | 811 (15.9) | 1678 (12.0) |
| Education, n (%) | |||
| Elementary | 3101 (34.8) | 923 (18.1) | 4024 (28.7) |
| Middle/high | 3672 (41.2) | 2426 (47.6) | 6098 (43.5) |
| College | 2144 (24.0) | 1749 (34.3) | 3893 (27.8) |
| Health conditions | |||
| Smoking, n (%) | 728 (8.2) | 3856 (75.6) | 4584 (32.7) |
| Alcohol, n (%) | 2049 (23.0) | 373 (7.3) | 2422 (17.3) |
| Inactivity, n (%) | 5540 (62.1) | 2831 (55.5) | 8371 (59.7) |
| Hypertension, n (%) | 2602 (29.2) | 1939 (38.0) | 4541 (32.4) |
| Diabetes, n (%) | 766 (9.0) | 548 (11.1) | 1314 (9.8) |
| Metabolic syndrome, n (%) | 2056 (24.2) | 1380 (28.0) | 3436 (25.6) |
| Menopause, n (%) | 4069 (45.6) | 0 (0.0) | 4069 (29.0) |
| GLM, n (%) | 568 (6.4) | 381 (7.5) | 949 (6.8) |
| LLM, n (%) | 499 (5.6) | 198 (3.9) | 697 (5.0) |
| Blood markers | |||
| FBG (mg/dL) | 96.2 ± 21.3 | 99.7 ± 26.2 | 97.5 ± 23.3 |
| Insulin (uIU/L) | 10.0 ± 5.6 | 9.9 ± 5.4 | 10.0 ± 5.5 |
| HOMA-IR | 2.4 ± 2.3 | 2.5 ± 1.7 | 2.5 ± 2.1 |
| TC (mg/dL) | 189.0 ± 36.0 | 186.7 ± 34.8 | 188.2 ± 35.6 |
| HDL-C (mg/dL) | 49.8 ± 10.9 | 44.5 ± 10.2 | 47.8 ± 11.0 |
| TG (mg/dL) | 115.0 ± 76.6 | 147.9 ± 104.6 | 127.1 ± 89.3 |
| AST (IU/L) | 20.3 ± 8.1 | 23.7 ± 12.2 | 21.5 ± 10.0 |
| ALT (IU/L) | 17.7 ± 12.7 | 26.2 ± 22.0 | 20.8 ± 17.2 |
| Platelet (109/L) | 264.2 ± 59.7 | 243.3 ± 54.1 | 256.5 ± 58.6 |
| Indices of hepatic steatosis | |||
| NAFLD-LFS | −1.44 ± 1.44 | −1.02 ± 1.47 | −1.29 ± 1.47 |
| HSI | 32.3 ± 4.8 | 32.7 ± 5.4 | 32.4 ± 5.0 |
| Optimal | Sarcopenia | Obesity | Sarcopenic Obesity | |
|---|---|---|---|---|
| Lower eCRF | 177 (14.9%) | 127 (27.9%) | 281 (61.2%) | 524 (69.4%) |
| Middle eCRF | 418 (11.2%) | 183 (20.7%) | 410 (59.8%) | 463 (63.3%) |
| Upper eCRF | 217 (9.3%) | 68 (18.3%) | 121 (49.0%) | 94 (54.3%) |
| p < 0.001 | p = 0.001 | p = 0.005 | p < 0.001 |
| Phenotypes | Lower 25% eCRF | Middle 50% eCRF | Upper 5% eCRF | ||||
|---|---|---|---|---|---|---|---|
| SAR | OB | Crude OR | Adjusted OR | Crude OR | Adjusted OR | Crude OR | Adjusted OR |
| - | - | 1 (referent) | 1 (referent) | 1 (referent) | 1 (referent) | 1 (referent) | 1 (referent) |
| + | - | 2.2 (1.7–2.9) ** | 2.1 (1.5–3.1) ** | 2.1 (1.7–2.5) ** | 1.6 (1.3–2.1) ** | 2.2 (1.6–3.0) ** | 2.1 (1.4–3.1) * |
| - | + | 9.0 (7.1–11.6) ** | 2.9 (2.0–4.2) ** | 11.8 (9.8–11.4) ** | 3.5 (2.7–4.6) ** | 9.4 (7.0–12.5) ** | 1.8 (1.2–2.8) * |
| + | + | 13.0 (10.4–16.2) ** | 5.9 (4.3–8.2) ** | 13.7 (11.4–16.4) ** | 4.2 (3.2–5.5) ** | 11.6 (8.3–16.1) ** | 2.5 (1.5–4.1) ** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, I.; Kim, J.; Kang, H. Estimated Cardiorespiratory Fitness Attenuates the Impacts of Sarcopenia and Obesity on Non-Alcoholic Fatty Liver in Korean Adults. Int. J. Environ. Res. Public Health 2020, 17, 3902. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113902
Lee I, Kim J, Kang H. Estimated Cardiorespiratory Fitness Attenuates the Impacts of Sarcopenia and Obesity on Non-Alcoholic Fatty Liver in Korean Adults. International Journal of Environmental Research and Public Health. 2020; 17(11):3902. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113902
Chicago/Turabian StyleLee, Inhwan, Jeonghyeon Kim, and Hyunsik Kang. 2020. "Estimated Cardiorespiratory Fitness Attenuates the Impacts of Sarcopenia and Obesity on Non-Alcoholic Fatty Liver in Korean Adults" International Journal of Environmental Research and Public Health 17, no. 11: 3902. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113902