Examining User’s Initial Trust Building in Mobile Online Health Community Adopting


Abstract
:1. Introduction
- (1)
- In the provision of MOHC service, how are the different initial trust elements interrelated and further influence users’ adoption?
- (2)
- For different initial trust elements in the MOHC, how are they formed based on the performance-based and transfer-based, respectively?
2. Literature Review
2.1. Online Health Community User Behavior
2.2. Initial Trust
2.3. Trust Transfer
2.4. Elaboration Likelihood Model
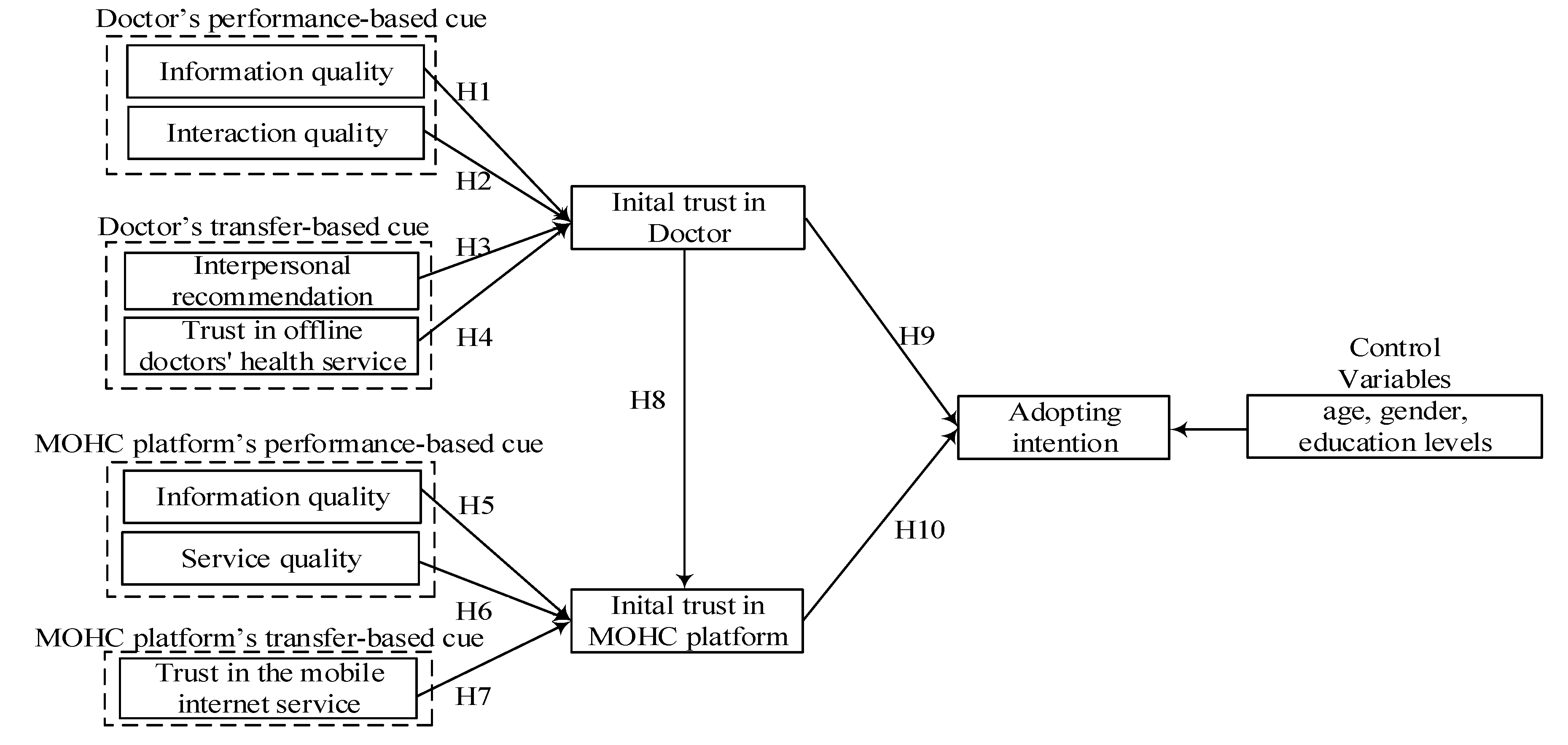
3. Research Model and Hypotheses
3.1. Doctor’s Initial Trust Formation Process
3.2. MOHC Platform’s Initial Trust Formation Process
3.3. Relationship Between Doctor’s Initial Trust and MOHC Platform’s Initial Trust
3.4. Initial Trust and Adopting Intention
4. Methodology
4.1. Measurement
4.2. Sampling Design
5. Data Analysis and Result
5.1. Measurement Model
5.2. Common Method Variance Testing
5.3. Structural Model
6. Discussion
6.1. Key Finding
6.2. Theory Implications
6.3. Practical Contributions
7. Conclusions
7.1. Study Limitations
7.2. Future Work
Author Contributions
Funding
Conflicts of Interest
References
- Zhang, X.F.; Guo, X.T.; Lai, K.; Yin, C.X.; Meng, F. From offline healthcare to online health services: The role of offline healthcare satisfaction and habits. J. Electron. Commer. Res. 2017, 18, 138–154. [Google Scholar]
- Alam, M.Z.; Hoquec, M.R.; Hud, W.; Baruae, Z. Factors in fluencing the adoption of mHealth services in a developing country: A patient-centric study. Int. J. Inf. Manag. 2020, 50, 128–143. [Google Scholar] [CrossRef]
- Gong, Z.P.; Han, Z.Q.; Li, X.D.; Yu, C.; Reinhardt, J. Factors influencing the adoption of online health consultation services: The role of subjective norm, trust, perceived benefit, and offline habit. Front. Public Health 2019, 7, 286. [Google Scholar] [CrossRef] [PubMed]
- Hoque, M.R. An empirical study of mHealth adoption in a developing country: The moderating effect of gender concern. BMC Med. Inform. Decis. Mak. 2016, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Zhou, T. Examining users’ knowledge sharing behaviour in online health communities. Data Technol. Appl. 2019, 53, 442–455. [Google Scholar] [CrossRef]
- Liu, W.L.; Fan, X.C.; Ji, R.R.; Jiang, Y. Perceived community support, users’ interactions, and value co-creation in online health community: The moderating effect of social exclusion. Int. J. Environ. Res. Public Health 2020, 17, 204. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.F.; Song, Y.Y.; Zhao, W.; Guo, X.T.; Ju, X.F.; Vogel, D. Exploring the role of online health community information in patients’ decisions to switch from online to offline medical services. Int. J. Med. Inform. 2019, 130, 103951. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, S.; Chen, X.; Gong, Y.Y. Social capital, motivations, and knowledge sharing intention in health Q&A communities. Manag. Decis. 2017, 55, 1536–1557. [Google Scholar]
- Hsiao, C.; Tang, K. Examining a model of mobile healthcare technology acceptance by the elderly in Taiwan. J. Glob. Inf. Technol. Manag. 2015, 18, 292–311. [Google Scholar] [CrossRef]
- Duarte, P.; Pinho, J.C. A mixed methods UTAUT2-based approach to assess mobile health adoption. J. Bus. Res. 2019, 102, 140–150. [Google Scholar] [CrossRef]
- Hoque, R.; Sorwar, G. Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int. J. Med. Inform. 2017, 101, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.; Mo, X.; Liu, S. Comparison of the middle-aged and older users’ adoption of mobile health services in China. Int. J. Med. Inform. 2014, 83, 210–224. [Google Scholar] [CrossRef] [PubMed]
- Quaosar, G.M.A.A.; Hoque, M.R.; Bao, Y. Investigating factors affecting elderly’s intention to use m-health services: An empirical study. Telemed. e-Health 2018, 24, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Han, S.; Jo, S.H. Consumer choice of on-demand mHealth app services: Context and contents values using structural equation modeling. Int. J. Med. Inform. 2017, 97, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Lu, Y.; Wang, B. Examining online consumers’ initial trust building from an elaboration likelihood model perspective. Inf. Syst. Front. 2016, 18, 265–275. [Google Scholar] [CrossRef]
- Zhou, T. An empirical examination of initial trust in mobile payment. Wirel. Pers. Commun. 2014, 77, 1519–1531. [Google Scholar] [CrossRef]
- Gao, L.; Waechter, K.A. Examining the role of initial trust in user adoption of mobile payment services: An empirical investigation. Inf. Syst. Front. 2015, 19, 525–548. [Google Scholar] [CrossRef]
- Talwar, S.; Dhir, A.; Khalil, A.; Mohan, G.; Islam, A.K.M.N. Point of adoption and beyond. Initial trust and mobile-payment continuation intention. J. Retail. Consum. Serv. 2020, 55, 102086. [Google Scholar] [CrossRef]
- Zhou, T. Understanding users’ initial trust in mobile banking: An elaboration likelihood perspective. Comput. Human Behav. 2012, 28, 1518–1525. [Google Scholar] [CrossRef]
- Liu, L.L.; Lee, M.K.O.; Liu, R.J.; Chen, J.W. Trust transfer in social media brand communities: The role of consumer engagement. Int. J. Inf. Manag. 2018, 41, 1–13. [Google Scholar] [CrossRef]
- Mohr, H.; Walter, Z. Formation of consumers’ perceived information security: Examining the transfer of trust in online retailers. Inf. Syst. Front. 2019, 21, 1231–1250. [Google Scholar] [CrossRef]
- Chen, X.; Huang, Q.; Davison, R.M.; Hua, Z. What drives trust transfer? The moderating roles of seller-specific and general institutional mechanisms. Int. J. Electron. Commer. 2015, 20, 261–289. [Google Scholar] [CrossRef]
- Vennika, F.D.; Adamsa, S.A.; Faberb, M.J.; Puttersa, K. Expert and experiential knowledge in the same place: Patients’ experiences with online communities connecting patients and health professionals. Patient Educ. Couns. 2014, 95, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Yang, Z. Examining mobile payment user adoption from the perspective of trust. Int. J. e-Serv. Sci. Technol. 2015, 8, 117–130. [Google Scholar]
- Kaabachi, S.; Mrad, B.S.; O’Leary, B. Consumer’s initial trust formation in IOB’s acceptance: The role of social influence and perceived compatibility. Int. J. Bank Mark. 2019, 37, 507–530. [Google Scholar] [CrossRef]
- Wu, C.C.; Huang, Y.; Hsu, C.L. Benevolence trust: A key determinant of user continuance use of online social networks. Inf. Syst. E-Bus. Manag. 2014, 12, 189–211. [Google Scholar] [CrossRef]
- Belanche, D.; Casaló, L.V.; Flavián, C.; Schepers, J. Trust transfer in the continued usage of public e-services. Inf. Manag. 2014, 51, 627–640. [Google Scholar] [CrossRef] [Green Version]
- Akter, S.; Ray, P.; D’Ambra, J. Continuance of mHealth services at the bottom of the pyramid: The roles of service quality and trust. Electron. Mark. 2013, 23, 29–47. [Google Scholar] [CrossRef]
- Guo, X.T.; Zhang, X.F.; Sun, Y.Q. The privacy-personalization paradox in mHealth services acceptance of different age groups. Electron. Commer. Res. Appl. 2016, 16, 55–65. [Google Scholar] [CrossRef]
- Mpinganjira, M. Precursors of trust in virtual health communities: A hierarchical investigation. Inf. Manag. 2018, 55, 686–694. [Google Scholar] [CrossRef]
- Audrain-Pontevia, A.F.; Menvielle, L. Effects of interpersonal trust among users of online health communities on patient trust in and satisfaction with their physician. Int. J. Technol. Assess. Health Care 2018, 34, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Yang, S. Role of transfer-based and performance-based cues on initial trust in mobile shopping services: A cross-environment perspective. Inf. Syst. E-Bus. Manag. 2016, 14, 47–70. [Google Scholar] [CrossRef]
- Zhou, T. An empirical examination of initial trust in mobile banking. Internet Res. 2011, 21, 527–540. [Google Scholar] [CrossRef]
- Xiao, L.; Guo, Z.X.; D’Ambra, J.; Fu, B. Building loyalty in e-commerce: Towards a multidimensional trust-based framework for the case of china. Progr. Electron. Libr. Inf. Syst. 2016, 50, 431–461. [Google Scholar] [CrossRef]
- Lu, Y.B.; Yang, S.Q.; Chau, P.Y.K.; Cao, Y.Z. Dynamics between the trust transfer process and intention to use mobile payment services: A cross-environment perspective. Inf. Manag. 2011, 48, 393–403. [Google Scholar] [CrossRef]
- Kim, J.B. An empirical study on consumer first purchase intention in online shopping: Integrating initial trust and TAM. Electron. Commer. Res. 2012, 12, 125–150. [Google Scholar] [CrossRef]
- Hong, I.B.; Cho, H. The impact of consumer trust on attitudinal loyalty and purchase intentions in b2c e-marketplaces: Intermediary trust vs. seller trust. Int. J. Inf. Manage. 2011, 31, 469–479. [Google Scholar] [CrossRef]
- Briñol, P.; Petty, R.E. Handbook of Theories of Social Psychology; Sage: London, UK, 2012. [Google Scholar]
- Tseng, S.Y.; Wang, C.N. Perceived risk influence on dual-route information adoption processes on travel websites. J. Bus. Res. 2016, 69, 2289–2296. [Google Scholar] [CrossRef]
- Nel, J.; Boshoff, C. Development of application-based mobile-service trust and online trust transfer: An elaboration likelihood model perspective. Behav. Inf. Technol. 2017, 36, 809–826. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, L.; Zhang, M.; Yang, J. Central or peripheral? Cognition elaboration cues’ effect on users’ continuance intention of mobile health applications in the developing markets. Int. J. Med. Inform. 2018, 116, 33–45. [Google Scholar] [CrossRef]
- Venkatesh, V.; Thong, J.Y.; Xu, X. Consumer acceptance and use of information technology: Extending the unified theory of acceptance and use of technology. MIS Q. 2012, 36, 157–178. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.L.; Deng, Z.H.; Zhang, D.L.; Buchanan, P.R.; Zha, D.Q.; Wang, R.X. Seeking and using intention of health information from doctors in social media: The effect of doctor-consumer interaction. Int. J. Med. Inform. 2018, 115, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Akter, S.; D’Ambra, J.; Ray, P. Development and validation of an instrument to measure user perceived service quality of mHealth. Inf. Manag. 2013, 50, 181–195. [Google Scholar] [CrossRef] [Green Version]
- Chan, C.S.C. Mistrust of physicians in China: Society, institution, and interaction as root causes. Dev. World Bioeth. 2018, 18, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Kaur, P.; Dhir, A.; Chen, S.; Malibari, A.; Almotairi, M. Why do people purchase virtual goods? A uses and gratification (U&G) theory perspective. Telemat. Inform. 2020, 101376, in press. [Google Scholar] [CrossRef]
- Kaur, P.; Dhir, A.; Singh, N.; Sahu, G.; Almotairi, M. An innovation resistance theory perspective on mobile payment solutions. J. Retail. Consum. Serv. 2020, 55, 102059. [Google Scholar] [CrossRef]
- Zhong, J.; Dhir, A.; Nieminen, M.; Hämäläinen, M.; Laine, J. Exploring consumer adoption of mobile payments in China. In Proceedings of the 17th International on Making Sense of Converging Media, Tampere, Finland, 1–4 October 2013; Association for Computing Machinery: New York, NY, USA, 2013; pp. 318–325. [Google Scholar]
- Fu, S.; Yan, Q.; Feng, G.C. Who will attract you? Similarity effect among users on online purchase intention of movie tickets in the social shopping context. Int. J. Inf. Manage. 2018, 40, 88–102. [Google Scholar] [CrossRef]
- Terres, M.D.S.; Basso, K. The art of building initial trust in medical services. Int. J. Pharm. Healthc. Mark. 2018, 12, 94–112. [Google Scholar] [CrossRef]
- Meng, F.; Guo, X.; Peng, Z.; Lai, K.H.; Zhao, X. Investigating the adoption of mobile health services by elderly users: Trust transfer model and survey study. J. Med. Internet Res. 2019, 21, e12269. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Shen, X.L.; Wang, N. Understanding the role of consistency during web–mobile service transition: Dimensions and boundary conditions. Int. Inf. Manag. 2014, 34, 465–473. [Google Scholar] [CrossRef]
- Lien, C.H.; Wu, J.J.; Chen, Y.H.; Wang, C.J. Trust transfer and the effect of service quality on trust in the healthcare industry. Manag. Serv. Qual. 2014, 24, 399–416. [Google Scholar] [CrossRef]
- Lu, Y.B.; Zhao, L.; Wang, B. From virtual community members to C2C e-commerce buyers: Trust in virtual communities and its effect on consumers’ purchase intention. Electron. Commer. Res. Appl. 2010, 9, 346–360. [Google Scholar] [CrossRef]
- Ahn, J.; Back, K. The role of autonomy, competence and relatedness Applying self-determination theory to the integrated resort setting. Int. J. Contemp. Hosp. Manag. 2019, 31, 87–104. [Google Scholar] [CrossRef]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); Sage: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Chaouali, W. Once a user, always a user: Enablers and inhibitors of continuance intention of mobile social networking sites. Telemat. Inform. 2016, 33, 1022–1033. [Google Scholar] [CrossRef]
- Gong, X.; Zhang, K.Z.K.; Chen, C.; Cheung, C.M.K.; Lee, M.K.O. Transition from web to mobile payment services: The triple effects of status quo inertia. Int. J. Inf. Manage. 2020, 50, 310–324. [Google Scholar] [CrossRef]
- Gu, D.X.; Deng, S.Y.; Zheng, Q.; Liang, C.Y.; Wu, J. Impacts of case-based health knowledge system in hospital management: The mediating role of group effectiveness. Inf. Manag. 2019, 56, 103162. [Google Scholar] [CrossRef]
- Rönkkö, M.; Ylitalo, J. PLS marker variable approach to diagnosing and controlling for method variance. In Proceedings of the ICIS 2011 Proceedings, Shanghai, China, 4–7 December 2011; pp. 1–16. [Google Scholar]
- Annual Comprehensive Research Report on Internet Medical Treatment in China. Available online: http://www.sohu.com/a/244840736_354988 (accessed on 2 August 2018).
- Gu, D.X.; Liang, C.L.; Kim, K.S.; Yang, C.H.; Cheng, W.J.; Wang, J. Which is more reliable, expert experience or information itself? weight scheme of complex cases for health management decision making. Int. J. Inf. Technol. Decis. Mak. 2015, 14, 597–620. [Google Scholar] [CrossRef]
- Gu, D.X.; Liang, C.Y.; Zhao, H.M. A case-based reasoning system based on weighted heterogeneous value distance metric for breast cancer diagnosis. Artif. Intell. Med. 2017, 77, 31–47. [Google Scholar] [CrossRef]
- Lu, J.; Chen, L.; Meng, K.; Wang, F.; Xiang, J.; Chen, N.; Han, X.; Li, B. Identifying User Profile by Incorporating Self-Attention Mechanism based on CSDN Data Set. Data Intell. 2019, 1, 160–175. [Google Scholar] [CrossRef]
- Xing, G.; Gao, H.; Cao, Q.; Yue, X.; Xu, B.; Cen, K.; Shen, H. User Profiling for CSDN: Keyphrase Extraction, User Tagging and User Growth Value Prediction: First-place Entry for User Profiling Technology Evaluation Campaign in SMP Cup. Data Intell. 2019, 1, 137–159. [Google Scholar] [CrossRef]
- Dhir, A.; Kaur, P.; Rajala, R. Continued use of mobile instant messaging apps: A new perspective on theories of consumption, flow, and planned behavior. Soc. Sci. Comput. Rev. 2020, 38, 147–169. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Source | Theoretical Framework | Significant Key Factors Affecting the Adoption |
|---|---|---|
| Alam et al. (2020) [2] | UTAUT + perceived reliability, price value | performance expectancy, effort expectancy, social influence, facilitating conditions, perceived reliability, price value |
| Duarte and Pinbo (2019) [10] | UTAUT + hedonic motivations, price value, habit | performance expectancy, effort expectancy, social influence, facilitating conditions, hedonic motivations, price value, habit |
| Quaosar et al. (2018) [13] | UTAUT + perceived credibility | performance expectancy, effort expectancy, social influence, perceived credibility |
| Hoque and Sorwar (2017) [11] | UTAUT + technology anxiety, resistance to change | performance expectancy, effort expectancy, social influence, technology anxiety, resistance to change |
| Lee et al. (2017) [14] | Content value, Context value | content value: usefulness, convenience; context value: health stress, epistemic value |
| Hoque and Raki bul (2016) [4] | TAM + subjective norm, personal innovativeness in IT | perceived ease of use, perceived usefulness, subjective norm, gender |
| Hsiao andTang (2015) [9] | TAM + perceived ubiquity, health knowledge, health care need, subjective norm | perceived ease of use, perceived ubiquity, health knowledge, health care need, subjective norm |
| Deng et al. (2014) [12] | value attitude behavior model (VAB), theory of planned behavior (TPB) | For the middle-aged group: perceived value, attitude, perceived behavior control and resistance to change; for the older group: perceived value, attitude, perceived behavior control, technology anxiety and self-actualization need. |
| Construct | Operational Definition and Measurement Items | Sources |
|---|---|---|
| Doctor’s information quality (DIT) | The usefulness, sufficiency and accuracy of the information offered by the doctor in MOHC | |
| DIT1: The doctor provides me with useful health information | [41,44] | |
| DIT2: The doctor provides me with sufficient health information | ||
| DIT3: The doctor provides me with reliable health information | ||
| Doctor’s interaction quality (DIQ) | The caring and individualized attention from the doctors to the MOHC users | |
| DIQ1: The doctor understands my specific needs | [41,44] | |
| DIQ2: The doctor has my best interests at heart | ||
| DIQ3: The doctor gives me individual care | ||
| Interpersonal recommendation (IR) | The informal or non-commercial information exchanges about the doctors in the MOHC between the potential user and other professionals, friends or relatives | |
| IR1: My family recommend the use of MOHC to me | [27] | |
| IR2: My colleagues recommend the use of MOHC to me | ||
| IR3: My friends recommend the use of mobile MOHC to me | ||
| Trust in offline doctors’ health service (TODHS) | The users’ belief in the integrity and benevolence of the offline doctors’ health service | |
| TODHS1: I trust the doctor who I am consult can provide effective treatment in the offline hospital | [50,51] | |
| TODHS2: I think I can trust the doctor I’m about to consult in the offline hospital | ||
| TODHS3: The doctor I am about to consult should probably be very reliable in the offline hospital | ||
| MOHC platform’s information quality (MIQ) | The timeliness, sufficient and relevance of the information offered by the MOHC platform | |
| MIQ1: This MOHC platform provides me with information relevant to my needs | [19] | |
| MIQ2: This MOHC platform provides me with sufficient information | ||
| MIQ3: This MOHC platform provides me with up-to-date information | ||
| MOHC platform’s service quality (MSQ) | The reliability, efficiency and personalized of the service offered by the MOHC platform | |
| MSQ1: This MOHC platform provides prompt services | [19] | |
| MSQ2: This MOHC platform provides personalized services | ||
| MSQ3: This MOHC platform provides dependable services | ||
| Trust in the mobile internet service (TMIS) | The users’ belief in the integrity and benevolence of the mobile internet service | |
| TMIS1: I trust the mobile internet service | [27] | |
| TMIS2: The mobile internet is a reliable mean to carry out transactions | ||
| TMIS3: When making transactions the mobile internet is trustworthy | ||
| Initial trust in Doctor (ITD) | The users’ initial belief in the competence, integrity and benevolence of the doctor in the MOHC | |
| ITD1: I believe the doctors in the MOHC platform have medical qualifications | [3] | |
| ITD 2: The consultation or diagnosis provided by the doctors in MOHC platform is reliable | ||
| ITD 3: In my opinion, the doctors in the MOHC platform are trustworthy | ||
| Initial trust in MOHC platform (ITM) | The users’ initial belief in the ability, integrity and benevolence of the MOHC platform | |
| ITM1: This MOHC platform can fulfill its tasks | [19] | |
| ITM2: This MOHC platform will keep its promises | ||
| ITM3: This MOHC platform will keep the customers’ best interests in mind | ||
| Adopting intention (AI) | The users’ using intention of MOHC in the further | |
| AI1: I intend to use MOHC to consult health issues when needed in the future | [3] | |
| AI2: I predict that I will use MOHC to consult health issues when needed in the future | ||
| AI3: I plan to use MOHC to consult health issues when needed in the future |
| Construct | Indicator | Factor Loading | AVE | Composite Reliability | VIF |
|---|---|---|---|---|---|
| Doctors’ information quality | DIT1 | 0.877 | 0.798 | 0.921 | 1.423 |
| DIT2 | 0.906 | ||||
| DIT3 | 0.895 | ||||
| Doctors’ interaction quality | DIQ1 | 0.843 | 0.747 | 0.900 | 1.531 |
| DIQ2 | 0.876 | ||||
| DIQ3 | 0.873 | ||||
| Interpersonal recommendation | IR1 | 0.915 | 0.877 | 0.956 | 1.613 |
| IR2 | 0.951 | ||||
| IR3 | 0.943 | ||||
| Trust in offline doctors’ health service | TODHS1 | 0.891 | 0.782 | 0.915 | 1.286 |
| TODHS2 | 0.876 | ||||
| TODHS3 | 0.886 | ||||
| MOHC platform’s information quality | MIQ1 | 0.845 | 0.730 | 0.890 | 2.302 |
| MIQ2 | 0.854 | ||||
| MIQ3 | 0.862 | ||||
| MOHC platform’s service quality | MSQ1 | 0.857 | 0.721 | 0.886 | 1.739 |
| MSQ2 | 0.828 | ||||
| MSQ3 | 0.861 | ||||
| Trust in the mobile internet service | TMIS1 | 0.869 | 0.770 | 0.910 | 1.468 |
| TMIS2 | 0.890 | ||||
| TMIS3 | 0.872 | ||||
| Initial trust in Doctor | ITD1 | 0.866 | 0.819 | 0.931 | 1.936 |
| ITD2 | 0.936 | ||||
| ITD3 | 0.911 | ||||
| Initial trust in MOHC platform | ITM1 | 0.844 | 0.724 | 0.887 | 2.453 |
| ITM2 | 0.898 | ||||
| ITM3 | 0.809 | ||||
| Adopting intention | AII | 0.911 | 0.803 | 0.924 | 1.205 |
| AI2 | 0.915 | ||||
| AI3 | 0.861 |
| Construct | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. DIT | 0.893 | |||||||||
| 2. DIQ | 0.36 | 0.864 | ||||||||
| 3. IR | 0.39 | 0.46 | 0.936 | |||||||
| 4. TODHS | 0.18 | 0.43 | 0.39 | 0.884 | ||||||
| 5. MIQ | 0.42 | 0.35 | 0.35 | 0.36 | 0.854 | |||||
| 6. MSQ | 0.23 | 0.37 | 0.38 | 0.37 | 0.42 | 0.849 | ||||
| 7. TMIS | 0.34 | 0.51 | 0.28 | 0.34 | 0.54 | 0.43 | 0.877 | |||
| 8. ITD | 0.45 | 0.48 | 0.43 | 0.36 | 0.51 | 0.23 | 0.31 | 0.905 | ||
| 9. ITM | 0.27 | 0.41 | 0.43 | 0.31 | 0.39 | 0.38 | 0.25 | 0.30 | 0.851 | |
| 10. AI | 0.37 | 0.32 | 0.31 | 0.02 | 0.32 | 0.30 | 0.30 | 0.38 | 0.30 | 0.896 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, Y.; Zhang, J.; Ma, L.; Qin, X.; Li, J. Examining User’s Initial Trust Building in Mobile Online Health Community Adopting. Int. J. Environ. Res. Public Health 2020, 17, 3945. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113945
Cao Y, Zhang J, Ma L, Qin X, Li J. Examining User’s Initial Trust Building in Mobile Online Health Community Adopting. International Journal of Environmental Research and Public Health. 2020; 17(11):3945. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113945
Chicago/Turabian StyleCao, Yuanyuan, Jiantong Zhang, Liang Ma, Xinghong Qin, and Junjun Li. 2020. "Examining User’s Initial Trust Building in Mobile Online Health Community Adopting" International Journal of Environmental Research and Public Health 17, no. 11: 3945. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113945