Short-Term Effects of Ambient Ozone, PM2.5, and Meteorological Factors on COVID-19 Confirmed Cases and Deaths in Queens, New York


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area, Air Pollutant, and Meteorological Data Collection Sites, and COVID-19 Data Collection
2.2. Statistical Analyses of Collected Data
3. Results and Discussions
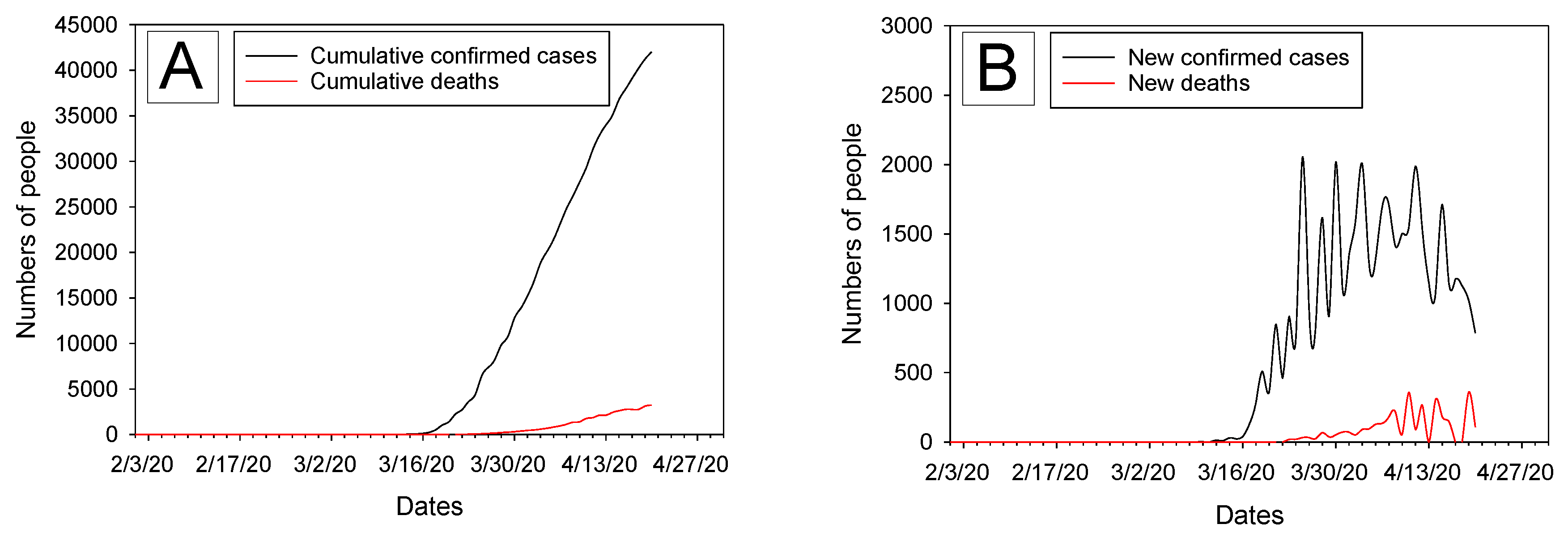
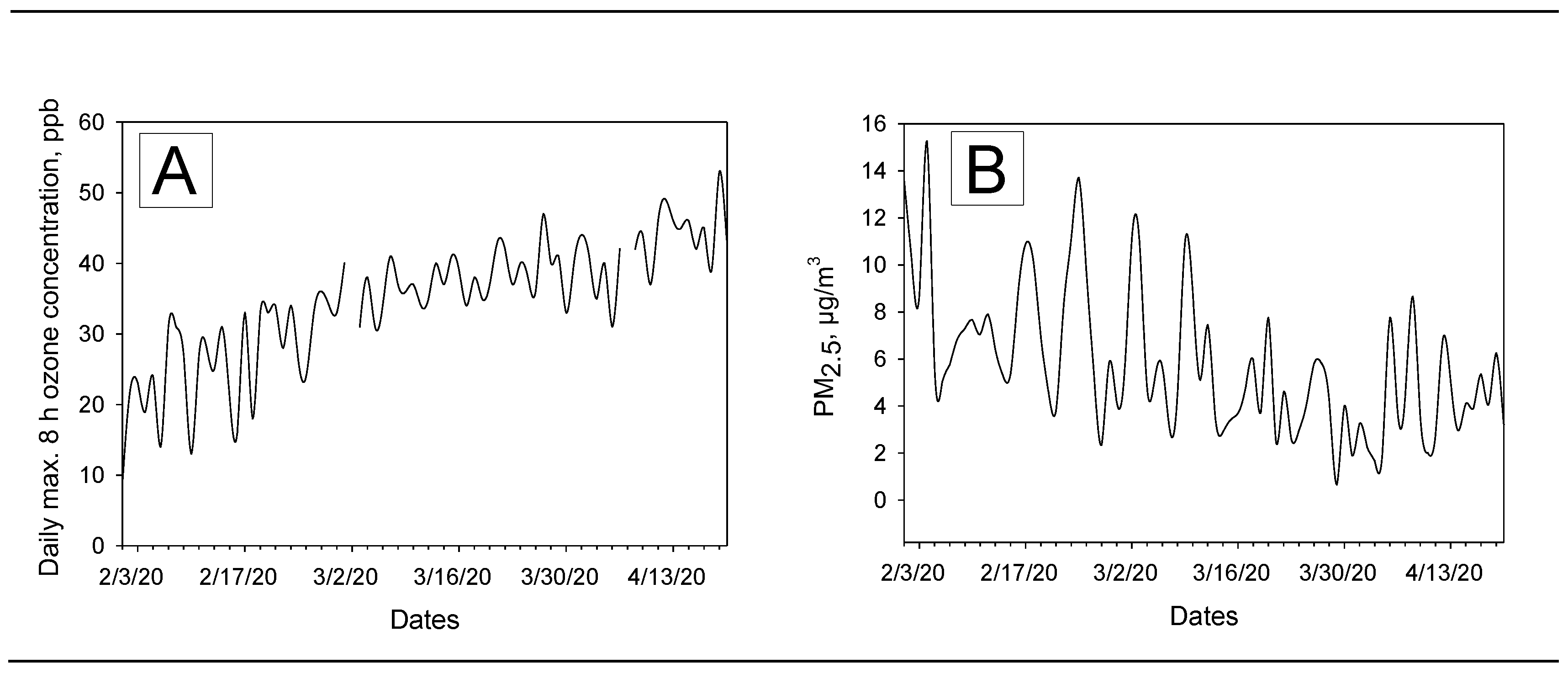
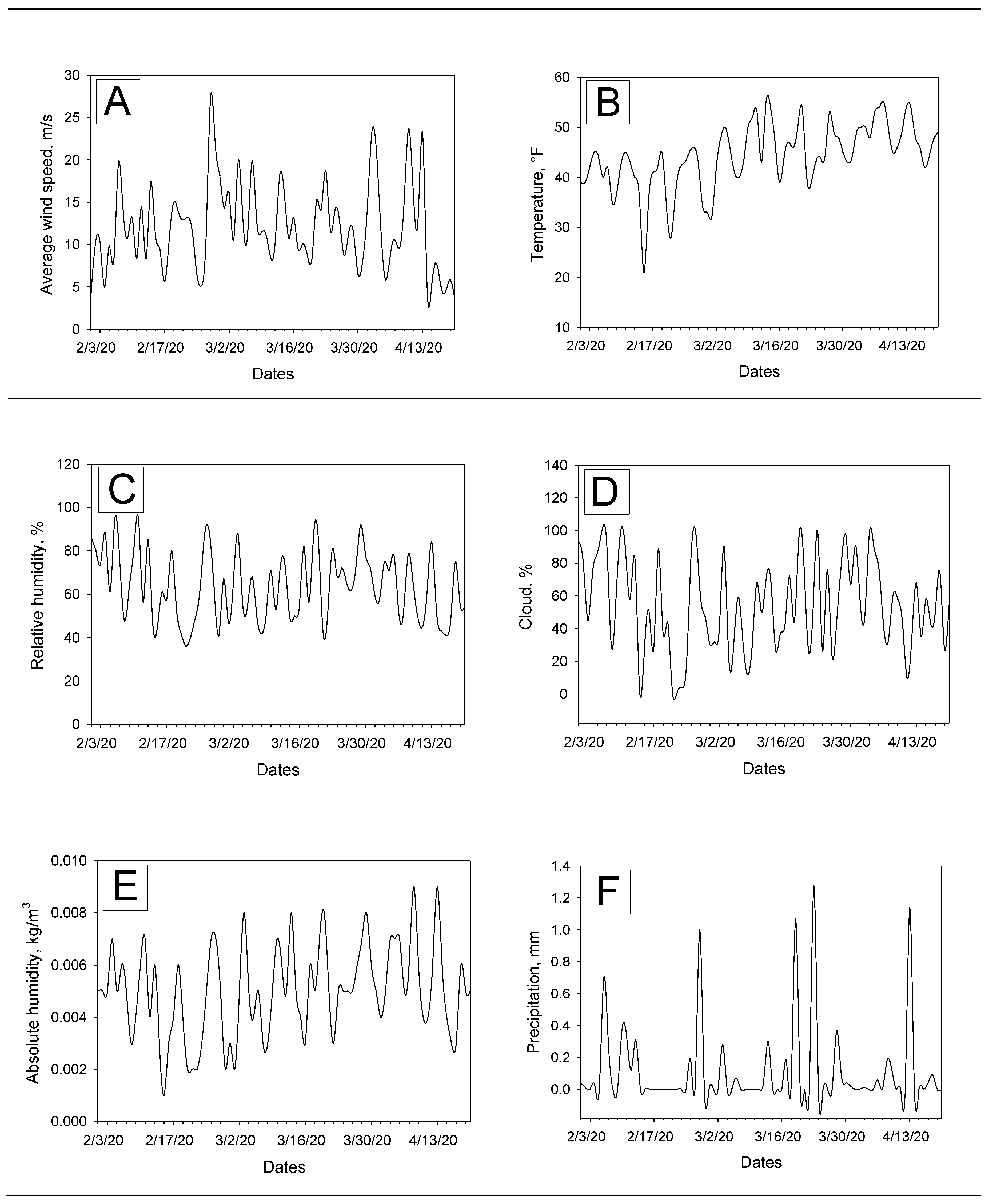
3.1. Descriptive Analysis of Data on COVID-19 Cases and Deaths, Ozone, PM2.5, and Meteorological Factors
3.2. Correlations among Ozone, PM2.5, and Meteorological Variables
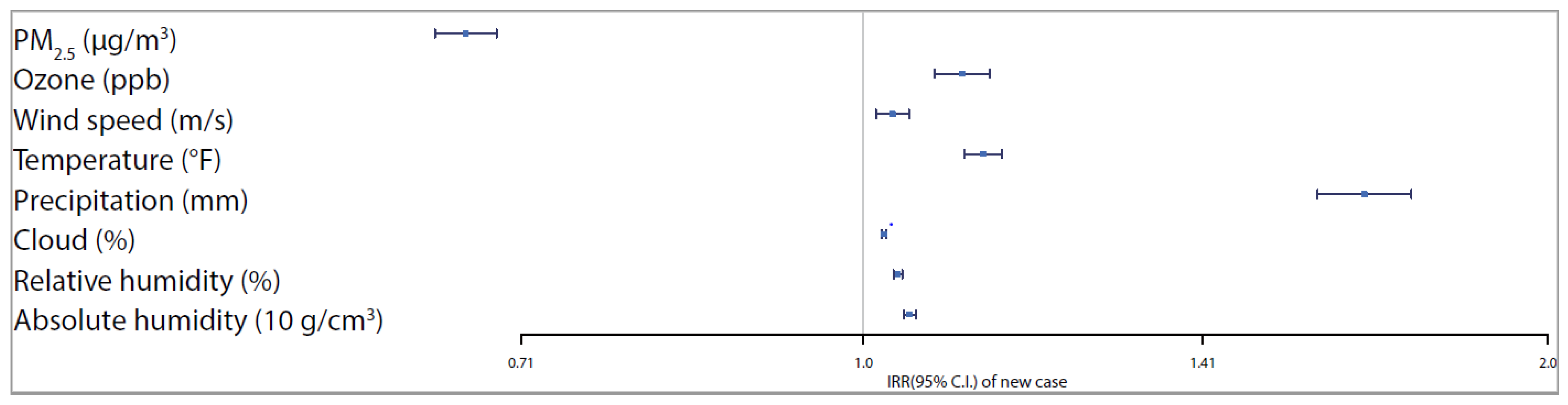
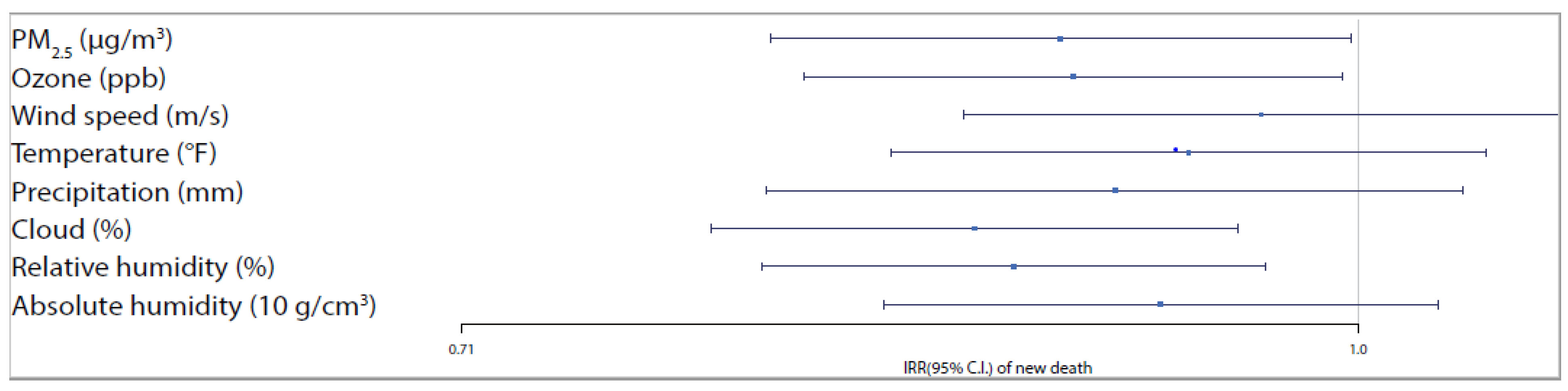
3.3. Relationships among COVID-19 Confirmed Cases/Deaths, Ozone, PM2.5, and Meteorological Variables
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report—36; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200225-sitrep-36-covid-19.pdf?sfvrsn=2791b4e0_2 (accessed on 24 April 2020).
- World Health Organization. Coronavirus Disease (COVID-19) Outbreak Situation; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 24 April 2020).
- Cases of Coronavirus Disease (COVID-19) in the US: Centers for Disease Control and Prevention (CDC). 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html (accessed on 24 April 2020).
- New York Department of Health. Information on Novel Coronavirus. Available online: https://coronavirus.health.ny.gov/home (accessed on 24 April 2020).
- State of the Air: American Lung Association. Available online: http://www.stateoftheair.org/city-rankings/states/new-york/ (accessed on 24 April 2020).
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.; Lau, E.H.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.-W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.-Y.; Poon, R.W.-S. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan. China. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.M.; Midgley, C.M.; Dratch, A.; Fenstersheib, M.; Haupt, T.; Holshue, M.; Ghinai, I.; Jarashow, M.C.; Lo, J.; McPherson, T.D.; et al. Active monitoring of persons exposed to patients with confirmed COVID-19—United States, January–February 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 245–246. [Google Scholar] [CrossRef] [Green Version]
- Yongjian, Z.; Jingu, X.; Fengming, H.; Liqing, C. Association between short-term exposure to air pollution and COVID-19 infection: Evidence from China. Sci. Total Environ. 2020, 15, 138704. [Google Scholar] [CrossRef]
- Zhu, Y.; Xie, J. Association between ambient temperature and COVID-19 infection in 122 cities from China. Sci. Total Environ. 2020, 724, 138201. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Nethery, R.C.; Sabath, B.M.; Braun, D.; Dominici, F. Exposure to air pollution and COVID-19 mortality in the United States. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Jakab, G.J.; Spannhake, E.W.; Canning, B.J.; Kleeberger, S.R.; Gilmour, M.I. The effects of ozone on immune function. Environ. Health Perspect. 1995, 103 (Suppl. 2), 77–89. [Google Scholar]
- Wu, W.; Doreswamy, V.; Diaz-Sanchez, D.; Samet, J.M.; Kesic, M.; Dailey, L.; Zhang, W.; Jaspers, I.; Peden, D.B. GSTM1 modulation of IL-8 expression in human bronchial epithelial cells exposed to ozone. Free Radic. Biol. Med. 2011, 51, 522–529. [Google Scholar] [CrossRef] [Green Version]
- Ciriolo, M.R.; Palamara, A.T.; Incerpi, S.; Lafavia, E.; Buè, M.C.; De Vito, P.; Garaci, E.; Rotilio, G. Loss of GSH, oxidative stress, and decrease of intracellular pH as sequential steps in viral infection. J. Biol. Chem. 1997, 272, 2700–2708. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, K.B. Oxidative stress during viral infection: A review. Free Radic. Biol. Med. 1996, 21, 641–649. [Google Scholar] [CrossRef]
- Cho, H.Y.; Kleeberger, S.R. Nrf2 protects against airway disorders. Toxicol. Appl. Pharmacol. 2010, 244, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Kesic, M.J.; Meyer, M.; Bauer, R.; Jaspers, I. Exposure to ozone modulates human airway protease/antiprotease balance contributing to increased influenza A infection. PLoS ONE 2012, 7, e35108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowell, G.; Echevarría-Zuno, S.; Viboud, C.; Simonsen, L.; Tamerius, J.; Miller, M.A.; Borja-Aburto, V.H. Characterizing the epidemiology of the 2009 influenza A/H1N1 pandemic in Mexico. PLoS Med. 2011, 8, e1000436. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.; Soukup, J.M.; Reed, W.; Carson, J.; Devlin, R.B.; Noah, T.L. Effect of ozone on susceptibility to respiratory viral infection and virus-induced cytokine secretion. Environ. Toxicol. Pharmacol. 1998, 6, 257–265. [Google Scholar] [CrossRef]
- Purvis, M.R.; Miller, S.; Ehrlich, R. Effect of atmospheric pollutants on susceptibility to respiratory infection: I. Effect of ozone. J. Infect. Dis. 1961, 109, 238–242. [Google Scholar] [CrossRef]
- Becker, S.; Soukup, J.M. Exposure to urban air particulates alters the macrophage-mediated inflammatory response to respiratory viral infection. J. Toxicol. Environ. Health Part A 1999, 57, 445–457. [Google Scholar]
- Horne, B.D.; Joy, E.A.; Hofmann, M.G.; Gesteland, P.H.; Cannon, J.B.; Lefler, J.S.; Blagev, D.P.; Korgenski, E.K.; Torosyan, N.; Hansen, G.I.; et al. Short-term elevation of fine particulate matter air pollution and acute lower respiratory infection. Am. J. Respir. Crit. Care Med. 2018, 198, 759–766. [Google Scholar] [CrossRef]
- Mäkinen, T.M.; Juvonen, R.; Jokelainen, J.; Harju, T.H.; Peitso, A.; Bloigu, A.; Silvennoinen-Kassinen, S.; Leinonen, M.; Hassi, J. Cold temperature and low humidity are associated with increased occurrence of respiratory tract infections. Respir. Med. 2009, 103, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Lowen, A.C.; Mubareka, S.; Steel, J.; Palese, P. Influenza virus transmission is dependent on relative humidity and temperature. PLoS Pathog. 2007, 3, e151. [Google Scholar] [CrossRef] [PubMed]
- Welliver, R.C.C., Sr. Temperature, humidity, and ultraviolet B radiation predict community respiratory syncytial virus activity. Pediatric Infect. Dis. J. 2007, 26, S29–S35. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Tang, K.; Feng, K.; Lv, W. High Temperature and High Humidity Reduce the Transmission of COVID-19. 2020. Available online: https://papers.ssrn.com/sol3/Papers.cfm?abstract_id=3551767 (accessed on 29 April 2020).
- Ma, Y.; Zhao, Y.; Liu, J.; He, X.; Wang, B.; Fu, S.; Yan, J.; Niu, J.; Zhou, J.; Luo, B. Effects of temperature variation and humidity on the death of COVID-19 in Wuhan, China. Sci. Total Environ. 2020, 724, 138226. [Google Scholar] [CrossRef] [PubMed]
- Oliveiros, B.; Caramelo, L.; Ferreira, N.C.; Caramelo, F.; Role of temperature and humidity in the modulation of the doubling time of COVID-19 cases. Preprint. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.03.05.20031872v1 (accessed on 29 April 2020).
- Pawar, S.; Stanam, A.; Chaudhari, M.; Rayudu, D. Effects of Temperature on COVID-19 Transmission. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.03.29.20044461v1 (accessed on 4 June 2020). [CrossRef] [Green Version]
- QuickFacts for Queens County (Queens Borough), New York; New York City, New York; United States, United States Census Bureau. Available online: https://www.census.gov/quickfacts/fact/table/queenscountyqueensboroughnewyork,newyorkcitynewyork/PST045219 (accessed on 4 June 2020).
- The Coronavirus Crisis. NPR Repor. Available online: https://www.npr.org/sections/coronavirus-live-updates/2020/04/11/ 832572922/ queens-among-hardest-hit-minority-communities-in-nyc (accessed on 25 April 2020).
- Coronavirus Stats & Data. Available online: https://usafacts.org/issues/coronavirus/ (accessed on 4 June 2020).
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Wang, M. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [Green Version]
- Coronavirus Incubation Could be as long as 27 Days, Chinese Provincial Government Says—Reuters. 22 February 2020. Available online: https://www.reuters.com/article/us-china-health-incubation/coronavirus-incubation-could-be-as-long-as-27-days-chinese-provincial-government-says-idUSKCN20G06W (accessed on 29 April 2020).
- Venables, W.N.; Ripley, B.D. Modern Applied Statistics with S, 4th ed.; Springer: New York, NY, USA, 2020. [Google Scholar]
- Jackman, S. pscl: Classes and Methods for R Developed in the Political Science Computational Laboratory; United States Studies Centre, University of Sydney: Sydney, NSW, Australia, 2020; R package version 1.5.5. [Google Scholar]
- Zeileis, A.; Kleiber, C.; Jackman, S. Regression Models for Count Data in R. J. Stat. Softw. 2008, 27. [Google Scholar] [CrossRef] [Green Version]
- Diagnostics for HierArchical Regession Models. Available online: http://florianhartig.github.io/DHARMa/ (accessed on 4 June 2020).
- Di, Q.; Dai, L.; Wang, Y.; Zanobetti, A.; Choirat, C.; Schwartz, J.D.; Dominici, F. Association of short-term exposure to air pollution with mortality in older adults. JAMA 2017, 318, 2446–2456. [Google Scholar] [CrossRef]
- US EPA. What are the Air Quality Standards for PM? Available online: https://www3.epa.gov/region1/airquality/pm-aq-standards.html (accessed on 28 April 2020).
- Mishra, R.; Pandikannan, K.; Gangamma, S.; Raut, A.A.; Kumar, H. Imperative Role of Particulate Matter in Innate Immunity During RNA Virus Infection. Non-Peer Reviewed Preprint. 2020. Available online: https://www.biorxiv.org/content/10.1101/2020.03.28.013169v1.full (accessed on 28 April 2020).
- Baglivo, M.; Baronio, M.; Natalini, G.; Beccari, T.; Chiurazzi, P.; Fulcheri, E.; Petralia, P.P.; Michelini, S.; Fiorentini, G.; Miggiano, G.A.; et al. Natural small molecules as inhibitors of coronavirus lipid-dependent attachment to host cells: A possible strategy for reducing SARS-COV-2 infectivity? Acta Biomed. 2020, 91, 161–164. [Google Scholar]
- Polozov, I.V.; Bezrukov, L.; Gawrisch, K.; Zimmerberg, J. Progressive ordering with decreasing temperature of the phospholipids of influenza virus. Nat. Chem. Biol. 2008, 4, 248. [Google Scholar] [CrossRef] [Green Version]
- Luo, W.; Majumder, M.; Liu, D.; Poirier, C.; Mandl, K.; Lipsitch, M.; Santillana, M. The Role of Absolute Humidity on Transmission Rates of the COVID-19 Outbreak. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.02.12.20022467v1.full.pdf (accessed on 28 April 2020).
- Roussel, M.; Pontier, D.; Cohen, J.M.; Lina, B.; Fouchet, D. Quantifying the role of weather on seasonal influenza. Bmc Public Health 2016, 16, 441. [Google Scholar] [CrossRef] [Green Version]
- Schuit, M.; Gardner, S.; Wood, S.; Bower, K.; Williams, G.; Freeburger, D.; Dabisch, P. The influence of simulated sunlight on the inactivation of influenza virus in aerosols. J. Infect. Dis. 2020, 221, 372–378. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Meteorological Variables | Mean | SD | Min. | Max. |
|---|---|---|---|---|
| PM2.5 (µg/m3) | 4.733 | 2.398 | 0.650 | 11.150 |
| Ozone (ppm) | 0.040 | 0.005 | 0.031 | 0.053 |
| Wind speed (m/s) | 12.114 | 5.050 | 3.610 | 23.710 |
| Temperature (°F) | 47.088 | 4.976 | 32.000 | 55.000 |
| Precipitation (mm) | 0.106 | 0.280 | 0.000 | 1.280 |
| Cloud (%) | 53.882 | 24.188 | 10.000 | 99.000 |
| Relative humidity (%) | 62.902 | 13.967 | 41.000 | 92.000 |
| Absolute humidity (kg/m3) | 0.005 | 0.002 | 0.002 | 0.009 |
| Var1 | Var2 | Spearman’s ρ | p Value |
|---|---|---|---|
| PM2.5 | Ozone | −0.8174 | <0.0001 |
| PM2.5 | Wind speed | 0.5846 | <0.0001 |
| Ozone | Wind speed | −0.5391 | <0.0001 |
| PM2.5 | Temperature | −0.7562 | <0.0001 |
| Ozone | Temperature | 0.9661 | <0.0001 |
| Windspeed | Temperature | −0.5381 | <0.0001 |
| PM2.5 | Precipitation | −0.5587 | <0.0001 |
| Ozone | Precipitation | 0.3277 | 0.0177 |
| Wind speed | Precipitation | −0.5687 | <0.0001 |
| Temperature | Precipitation | 0.3530 | 0.0103 |
| PM2.5 | Cloud | −0.7975 | <0.0001 |
| Ozone | Cloud | 0.8391 | <0.0001 |
| Wind speed | Cloud | −0.6048 | <0.0001 |
| Temperature | Cloud | 0.7965 | <0.0001 |
| Precipitation | Cloud | 0.6382 | <0.0001 |
| PM2.5 | Relative humidity | −0.7415 | <0.0001 |
| Ozone | Relative humidity | 0.7705 | <0.0001 |
| Wind speed | Relative humidity | −0.5700 | <0.0001 |
| Temperature | Relative humidity | 0.7516 | <0.0001 |
| Precipitation | Relative humidity | 0.6986 | <0.0001 |
| Cloud | Relative humidity | 0.9727 | <0.0001 |
| PM2.5 | Absolute humidity | −0.7911 | <0.0001 |
| Ozone | Absolute humidity | 0.9478 | <0.0001 |
| Wind speed | Absolute humidity | −0.5327 | <0.0001 |
| Temperature | Absolute humidity | 0.9618 | <0.0001 |
| Precipitation | Absolute humidity | 0.4335 | 0.0013 |
| Cloud | Absolute humidity | 0.8867 | <0.0001 |
| Relative Humidity | Absolute humidity | 0.8658 | <0.0001 |
| Estimate | Std. Error | Z Score | IRR | 95% CI Lower | 95% CI Upper | Pr(>|z|) | |
|---|---|---|---|---|---|---|---|
| PM2.5 (µg/m3) | −0.4029 | 0.0160 | −25.2200 | 0.6684 | 0.6478 | 0.6896 | <0.0001 |
| Ozone (ppb) | 0.0999 | 0.0142 | 7.0179 | 1.1051 | 1.0747 | 1.1363 | <0.0001 |
| Wind speed (m/s) | 0.0295 | 0.0085 | 3.4566 | 1.0299 | 1.0128 | 1.0473 | 0.0005 |
| Temperature (°F) | 0.1210 | 0.0096 | 12.5792 | 1.1287 | 1.1076 | 1.1502 | <0.0001 |
| Precipitation (mm) | 0.5072 | 0.0243 | 20.8445 | 1.6606 | 1.5833 | 1.7417 | <0.0001 |
| Cloud (%) | 0.0209 | 0.0013 | 16.0021 | 1.0211 | 1.0185 | 1.0237 | <0.0001 |
| Relative humidity (%) | 0.0348 | 0.0022 | 15.6379 | 1.0354 | 1.0309 | 1.0399 | <0.0001 |
| Absolute humidity (10 g/cm3) | 0.0465 | 0.0032 | 14.6070 | 1.0476 | 1.0411 | 1.0542 | <0.0001 |
| Estimate | Std. Error | Z Score | IRR | 95% CI Lower | 95% CI Upper | Pr(>|z|) | |
|---|---|---|---|---|---|---|---|
| PM2.5 (µg/m3) | −0.1151 | 0.0573 | −2.0106 | 0.8912 | 0.7966 | 0.9971 | 0.0444 |
| Ozone (ppb) | −0.1101 | 0.0531 | −2.0722 | 0.8958 | 0.8072 | 0.9941 | 0.0382 |
| Wind speed (m/s) | −0.0375 | 0.0587 | −0.6396 | 0.9632 | 0.8585 | 1.0806 | 0.5224 |
| Temperature (°F) | −0.0655 | 0.0587 | −1.1160 | 0.9366 | 0.8349 | 1.0508 | 0.2644 |
| Precipitation (mm) | −0.0941 | 0.0688 | −1.3687 | 0.9102 | 0.7954 | 1.0415 | 0.1711 |
| Cloud (%) | −0.1484 | 0.0521 | −2.8469 | 0.8621 | 0.7784 | 0.9548 | 0.0044 |
| Relative humidity (%) | −0.1334 | 0.0497 | −2.6838 | 0.8752 | 0.7939 | 0.9647 | 0.0073 |
| Absolute humidity (10 g/cm3) | −0.0764 | 0.0547 | −1.3962 | 0.9264 | 0.8322 | 1.0313 | 0.1626 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adhikari, A.; Yin, J. Short-Term Effects of Ambient Ozone, PM2.5, and Meteorological Factors on COVID-19 Confirmed Cases and Deaths in Queens, New York. Int. J. Environ. Res. Public Health 2020, 17, 4047. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114047
Adhikari A, Yin J. Short-Term Effects of Ambient Ozone, PM2.5, and Meteorological Factors on COVID-19 Confirmed Cases and Deaths in Queens, New York. International Journal of Environmental Research and Public Health. 2020; 17(11):4047. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114047
Chicago/Turabian StyleAdhikari, Atin, and Jingjing Yin. 2020. "Short-Term Effects of Ambient Ozone, PM2.5, and Meteorological Factors on COVID-19 Confirmed Cases and Deaths in Queens, New York" International Journal of Environmental Research and Public Health 17, no. 11: 4047. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114047