Inclusion of Health in Impact Assessment: A Review of Current Practice in Sub-Saharan Africa

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
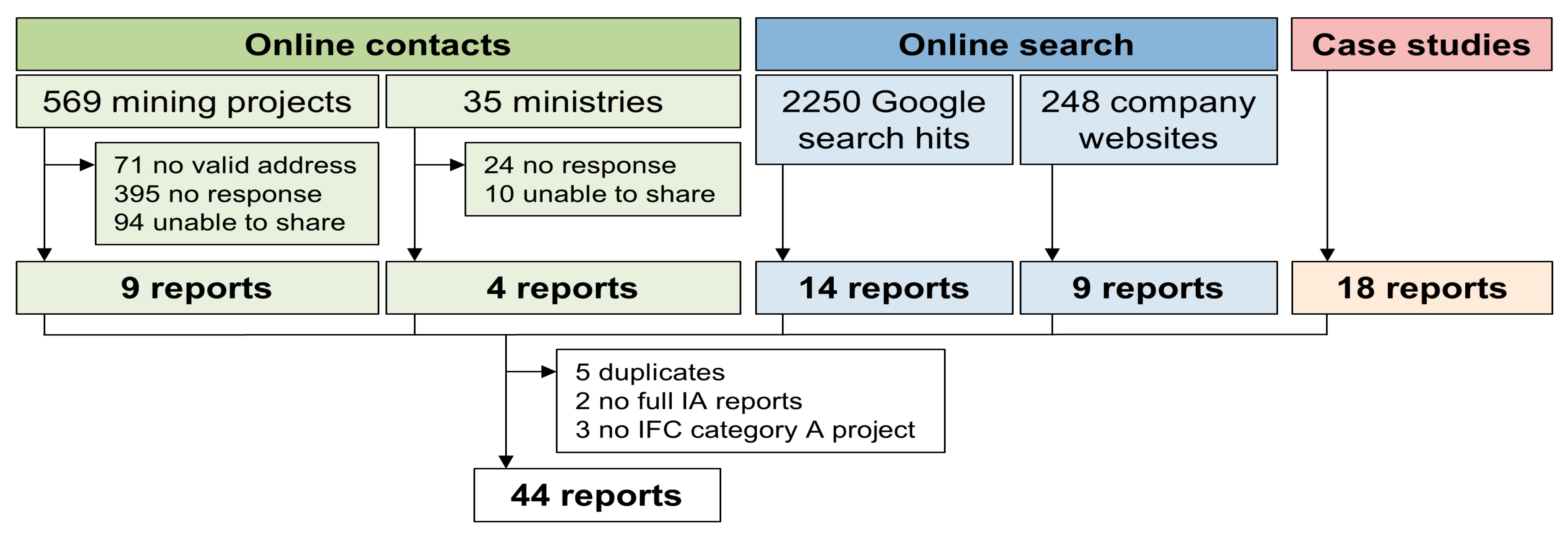
2.1. Strategy for Identification of Relevant Reports
2.1.1. Online Contacts within Mining Companies and Ministries
2.1.2. Online Search
2.1.3. Case Studies
2.2. Screening of IA Reports
2.3. Data Extraction and Analysis
3. Results
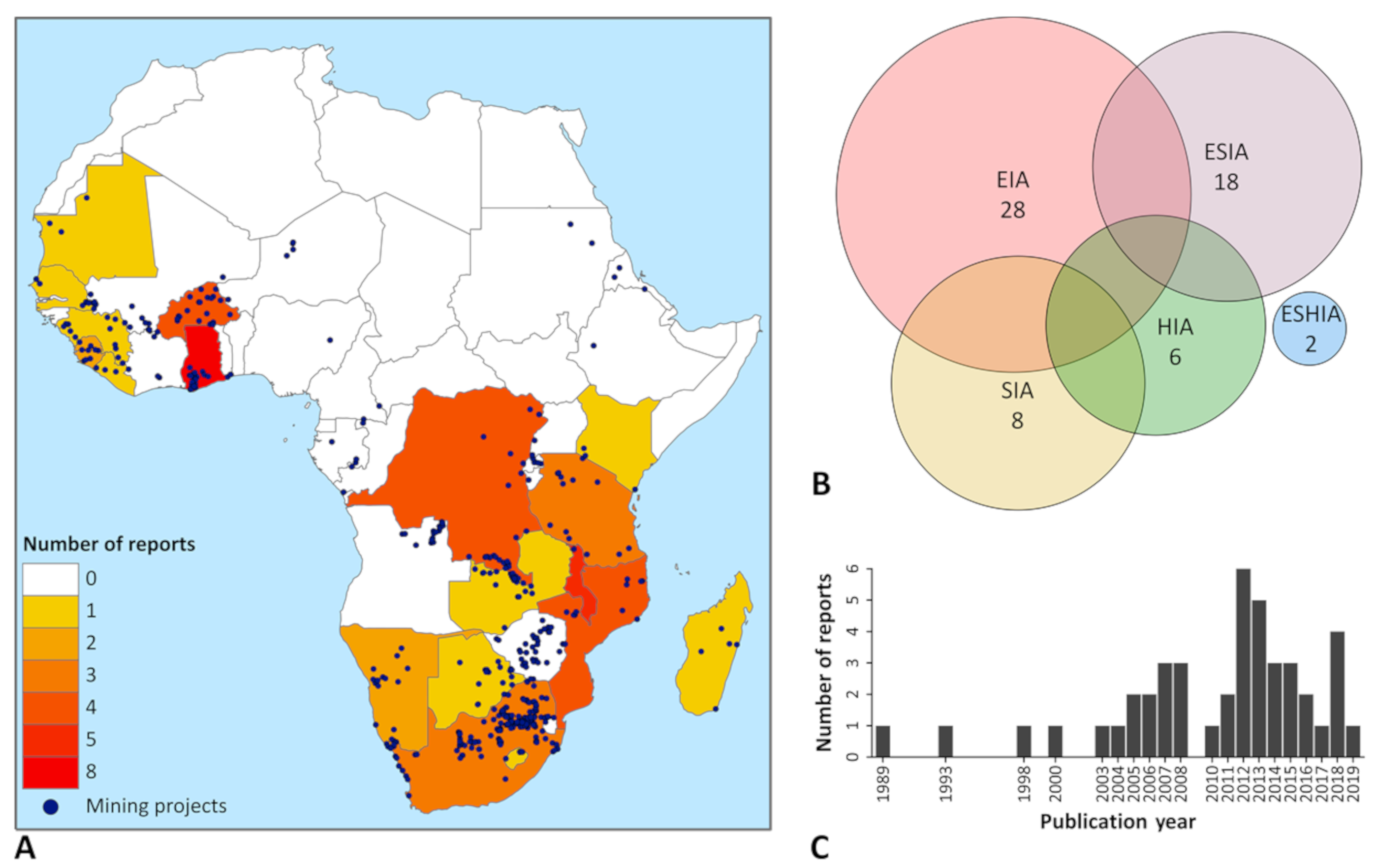
3.1. Report Characteristics
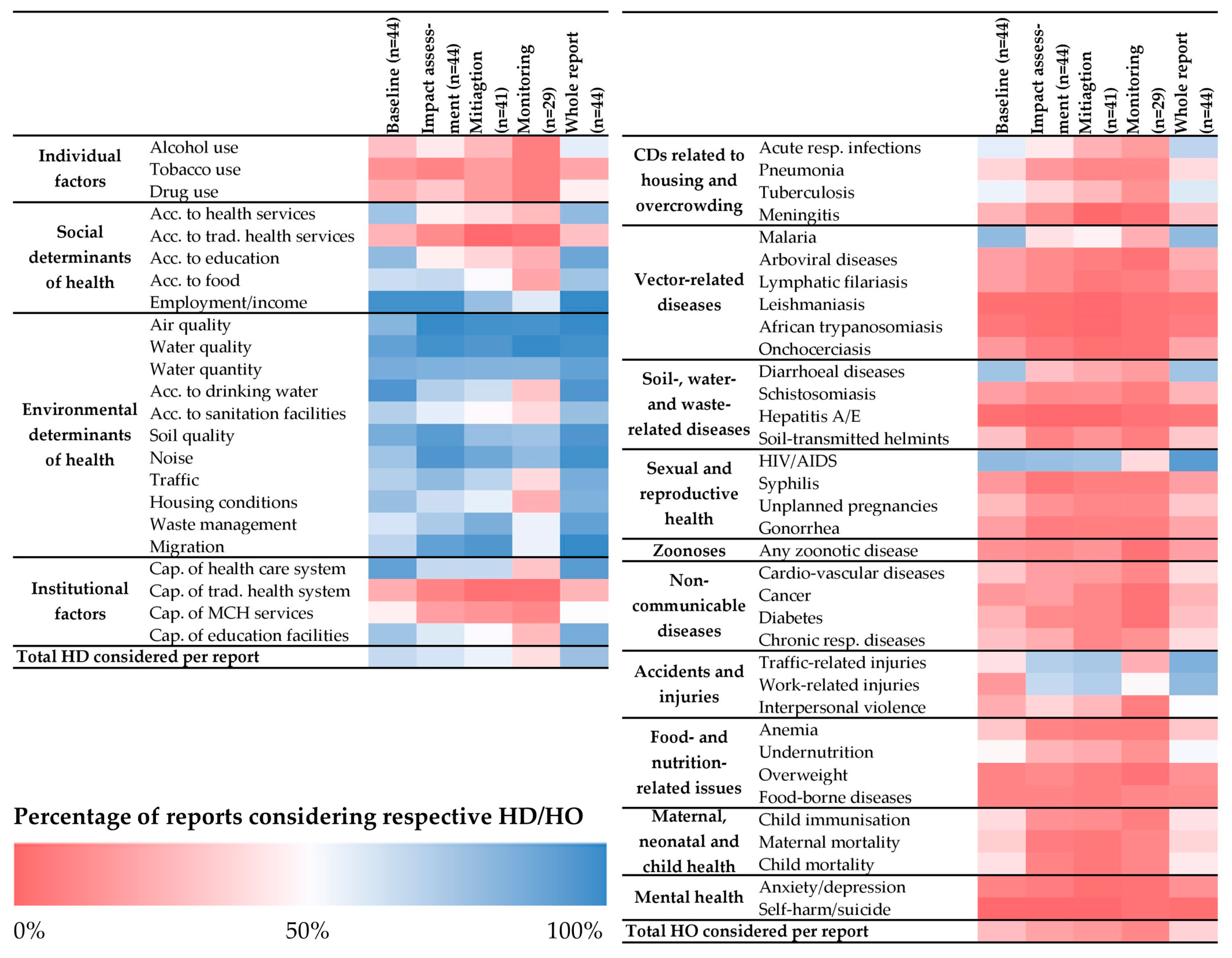
3.2. Inclusion of Health Aspects
3.2.1. Inclusion of Health Determinants
3.2.2. Inclusion of Health Outcomes
3.3. Data Sources
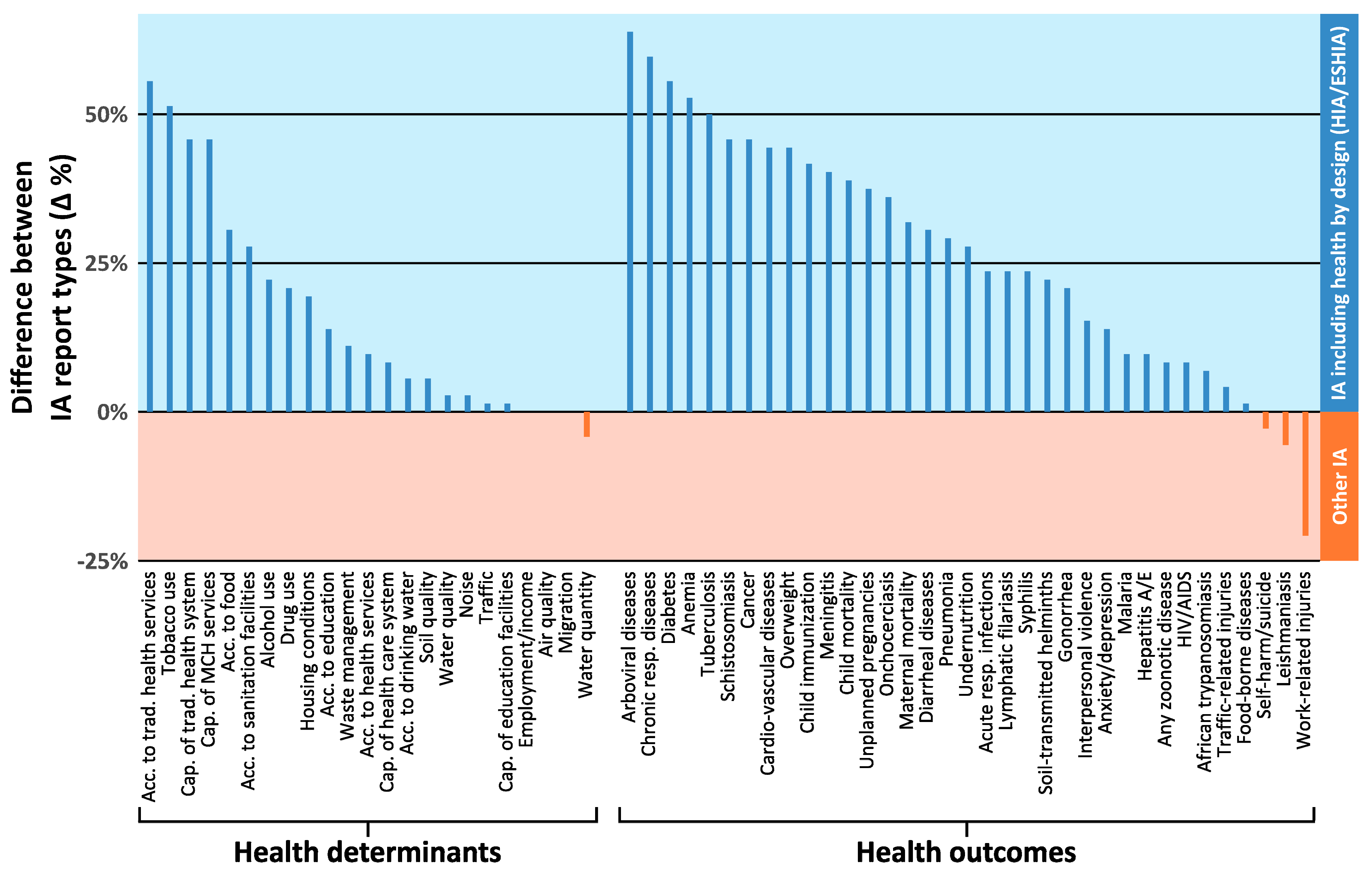
3.4. Comparison between IA Report Types
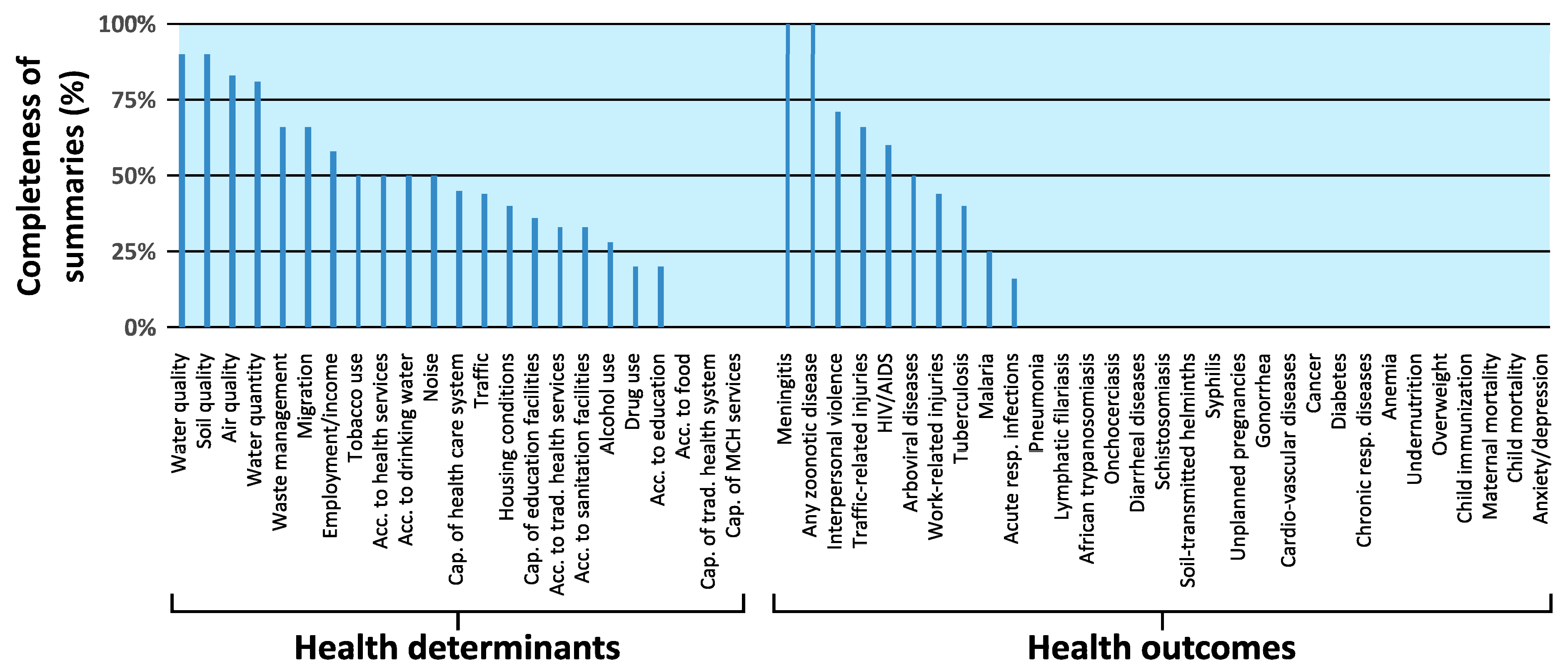
3.5. Completeness of Executive Summaries
4. Discussion
4.1. Lack of Transparency
4.2. Narrow Range of Health Aspects Considered
4.3. Lack of Primary Data Collection
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Determinant Categories | Description |
|---|---|
| Individual factors | Factors related to the individual’s biology and behavior. These comprise for example gender, age, ethnicity, dietary intake, level of physical activity, tobacco use, alcohol intake, personal safety, sense of control over own life, employment status, educational attainment, self-esteem, life skills, stress levels, resilience and risk behavior. |
| Social determinants of health | Conditions in which people are born, grow, live, work and age. These include access to services and community (health, education, nutrition, institutional and social support, social and health insurance); income/unemployment rate; distribution of wealth; empowerment of women; sexual customs and tolerance; racism; attitudes to disability; trust; sites of cultural and spiritual significance. |
| Environmental determinants of health | Physical, chemical, and biological factors external to a person, and all the related factors impacting behaviors, such as exposure to heavy metals, pesticides and other compounds, solvents or spills and releases from road traffic; air pollution (indoor and outdoor); noise pollution and exposure to malodors. It also includes factors, such as inadequate housing, water and sanitation services, and the mixing of population groups with different levels of communicable diseases which can be associated with in-migration. |
| Institutional factors | Availability of services, including (traditional) health services, transport and communication networks; educational and employment; environmental and public health legislation; environmental and health monitoring systems; laboratory facilities; social and health insurance schemes. |
| Health Outcome Categories | Description |
|---|---|
| Communicable diseases related to housing and overcrowding | Transmission of communicable diseases (e.g., acute respiratory infections, pneumonia, tuberculosis, meningitis, plague, leprosy, etc.) that can be linked to inadequate housing design, overcrowding and housing inflation |
| Vector-related diseases | Mosquito, fly, tick and lice-related diseases (e.g., malaria, dengue, yellow fever, lymphatic filariasis, leishmaniasis, human African trypanosomiasis, onchocerciasis, etc.) |
| Soil-, water- and waste-related diseases | Diseases that are transmitted directly or indirectly through contaminated water, soil or non-hazardous waste (e.g., diarrheal diseases, schistosomiasis, hepatitis A and E, poliomyelitis, soil-transmitted helminthiases, etc.) |
| Sexual and reproductive health | Sexually-transmitted infections such as syphilis, gonorrhea, Chlamydia, hepatitis B and, most importantly, HIV/AIDS |
| Veterinary medicine and zoonotic diseases | Diseases affecting animals (e.g., bovine tuberculosis, swinepox, avian influenza) or that can be transmitted from animal to human (e.g., rabies, brucellosis, Rift Valley fever, monkey pox, Ebola, leptospirosis, etc.) |
| Non-communicable diseases | Cardiovascular diseases, cancer, diabetes, that can be linked to changes in lifestyle, exposure to hazardous materials in air, water or soil, and noise |
| Accidents/injuries | Road traffic or work-related accidents and injuries (home and project related); drowning; unintentional poisoning |
| Food- and nutrition-related issues | Adverse health effects such as malnutrition, anemia, micronutrient deficiencies or obesity due to e.g., changes in agricultural and subsistence practices, or food inflation; gastroenteritis, food-borne trematodiases, etc. |
| Maternal and child health | Prenatal, natal and postpartum health conditions, infant and child health and immunization |
| Mental health | Psychological health conditions linked to resettlement of populations or changes in lifestyles (e.g., anxiety, depression, stress symptoms, suicide) |
| Health Determinant Categories | Baseline (n = 44) | Impact Assessment (n = 44) | Mitigation (n = 41) | Monitoring (n = 29) | Whole Report (n = 44) | |
|---|---|---|---|---|---|---|
| Individual factors | Alcohol use | 29.5 | 43.2 | 26.8 | 6.9 | 56.8 |
| Tobacco use | 13.6 | 9.1 | 17.1 | 6.9 | 20.5 | |
| Drug use | 22.7 | 31.8 | 17.1 | 6.9 | 45.5 | |
| Social determinants of health | Access to health services | 75.0 | 45.5 | 39.0 | 27.6 | 79.5 |
| Access to trad. health services | 25.0 | 11.4 | 0 | 3.4 | 29.5 | |
| Access to education | 79.5 | 45.5 | 36.6 | 24.1 | 88.6 | |
| Access to food | 63.6 | 65.9 | 51.2 | 20.7 | 75.0 | |
| Employment/income | 97.7 | 97.7 | 78.0 | 58.6 | 100 | |
| Environmental determinants of health | Air quality | 81.8 | 100 | 97.6 | 96.6 | 100 |
| Water quality | 90.9 | 98.0 | 95.1 | 100 | 98.0 | |
| Water quantity | 86.4 | 84.1 | 82.9 | 82.8 | 90.9 | |
| Access to drinking water | 95.5 | 70.5 | 63.4 | 31.0 | 95.5 | |
| Access to sanitation facilities | 70.5 | 56.8 | 48.8 | 37.9 | 77.3 | |
| Soil quality | 86.4 | 93.2 | 78.0 | 75.9 | 95.5 | |
| Noise | 75.0 | 95.5 | 87.8 | 79.3 | 97.7 | |
| Traffic | 70.5 | 79.5 | 68.3 | 37.9 | 86.4 | |
| Housing conditions | 77.3 | 63.6 | 56.1 | 24.1 | 84.1 | |
| Waste management | 61.4 | 72.7 | 85.4 | 55.2 | 90.9 | |
| Migration | 68.2 | 90.9 | 95.1 | 55.2 | 100 | |
| Institutional factors | Cap. of health care system | 90.9 | 65.9 | 65.9 | 31.0 | 93.2 |
| Cap. of traditional health system | 22.7 | 9.1 | 2.4 | 3.4 | 25.0 | |
| Cap. of MCH services | 45.5 | 18.2 | 14.6 | 10.3 | 50.0 | |
| Cap. of education facilities | 75.0 | 59.1 | 51.2 | 27.6 | 86.4 | |
| Total health determinants considered per report | 65.4 | 61.2 | 54.7 | 39.3 | 76.8 | |
| Health Outcome Categories | Baseline (n = 44) | Impact Assessment (n = 44) | Mitigation (n = 41) | Monitoring (n = 29) | Whole Report (n = 44) | |
|---|---|---|---|---|---|---|
| Communicable diseases related to housing and overcrowding | Acute respiratory infections | 56.8 | 43.2 | 24.4 | 17.2 | 68.2 |
| Pneumonia | 36.4 | 15.9 | 9.8 | 10.3 | 38.6 | |
| Tuberculosis | 54.5 | 36.4 | 26.8 | 13.8 | 59.1 | |
| Meningitis | 25.0 | 11.4 | 0 | 3.4 | 29.5 | |
| Vector-related diseases | Malaria | 79.5 | 40.9 | 46.3 | 24.1 | 79.5 |
| Arboviral diseases | 18.2 | 11.4 | 7.3 | 3.4 | 22.7 | |
| Lymphatic filariasis | 18.2 | 11.4 | 4.9 | 6.9 | 18.2 | |
| Leishmaniasis | 2.3 | 2.3 | 0 | 3.4 | 4.5 | |
| African trypanosomiasis | 4.5 | 2.3 | 0 | 3.4 | 6.8 | |
| Onchocerciasis | 15.9 | 6.8 | 2.4 | 3.4 | 20.5 | |
| Soil-, water- and waste-related diseases | Diarrheal diseases | 75.0 | 29.5 | 22.0 | 17.2 | 75.0 |
| Schistosomiasis | 18.2 | 11.4 | 12.2 | 6.9 | 25.0 | |
| Hepatitis A/E | 2.3 | 0 | 0 | 3.4 | 4.5 | |
| Soil-transmitted helminths | 29.5 | 9.1 | 14.6 | 6.9 | 31.8 | |
| Sexual and reproductive health | HIV/AIDS | 79.5 | 77.3 | 75.6 | 37.9 | 93.2 |
| Syphilis | 15.9 | 4.5 | 7.3 | 6.9 | 18.2 | |
| Unplanned pregnancies | 27.3 | 13.6 | 9.8 | 10.3 | 31.8 | |
| Gonorrhea | 18.2 | 6.8 | 7.3 | 6.9 | 20.5 | |
| Zoonoses | Any zoonotic disease | 13.6 | 11.4 | 14.6 | 3.4 | 18.2 |
| Non-communicable diseases | Cardio-vascular diseases | 31.8 | 18.2 | 17.1 | 10.3 | 38.6 |
| Cancer | 15.9 | 18.2 | 9.8 | 3.4 | 25.0 | |
| Diabetes | 25.0 | 11.4 | 9.8 | 3.4 | 29.5 | |
| Chronic respiratory diseases | 29.5 | 22.7 | 9.8 | 13.8 | 38.6 | |
| Accidents and injuries | Traffic-related injuries | 40.9 | 70.5 | 73.2 | 24.1 | 84.1 |
| Work-related injuries | 15.9 | 65.9 | 70.7 | 48.3 | 79.5 | |
| Interpersonal violence | 22.7 | 36.4 | 26.8 | 6.9 | 50.0 | |
| Food- and nutrition-related issues | Anemia | 31.8 | 9.1 | 7.3 | 6.9 | 31.8 |
| Undernutrition | 47.7 | 25.0 | 22.0 | 13.8 | 52.3 | |
| Overweight | 9.1 | 11.4 | 7.3 | 3.4 | 13.6 | |
| Food-borne diseases | 9.1 | 9.1 | 7.3 | 10.3 | 11.4 | |
| Maternal, neonatal and child health | Child immunization | 38.6 | 13.6 | 12.2 | 6.9 | 40.9 |
| Maternal mortality | 34.1 | 6.8 | 4.9 | 10.3 | 36.4 | |
| Child mortality | 40.9 | 9.1 | 4.9 | 10.3 | 43.2 | |
| Mental health | Anxiety/depression | 9.1 | 6.8 | 2.4 | 3.4 | 13.6 |
| Self-harm/suicide | 0 | 0 | 0 | 3.4 | 2.3 | |
| Total health outcomes considered per report | 28.4 | 19.4 | 16.3 | 10.5 | 35.9 | |
| Health Determinant and Health Outcome Categories | Any Primary Data Source | Any Secondary Data Source | Key Informant Interviews | Focus Group Discussions | Household Surveys | Env. Sample, Observation | Routine Health Surveillance | National/Re-gional Surveys | Official Statistics | Peer-Reviewed Literature | Grey Literature | Unknown, Other | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Individual factors | Alcohol use (n = 13) | 69.2 | 61.5 | 38.5 | 38.5 | 30.8 | 7.7 | 15.4 | 7.7 | 23.1 | 0 | 23.1 | 0 |
| Tobacco use (n = 6) | 83.3 | 66.7 | 33.3 | 16.7 | 50 | 16.7 | 16.7 | 33.3 | 33.3 | 0 | 16.7 | 0 | |
| Drug use (n = 10) | 80 | 60 | 50 | 40 | 30 | 10 | 20 | 0 | 30 | 0 | 20 | 0 | |
| Social determinants of health | Access to health services (n = 33) | 57.6 | 54.5 | 24.2 | 24.2 | 21.2 | 6.1 | 18.2 | 12.1 | 24.2 | 3 | 15.2 | 24.2 |
| Access to trad. health services (n = 11) | 45.5 | 36.4 | 27.3 | 9.1 | 27.3 | 9.1 | 9.1 | 0 | 18.2 | 9.1 | 9.1 | 27.3 | |
| Access to education (n = 35) | 45.7 | 65.7 | 17.1 | 11.4 | 25.7 | 5.7 | 2.9 | 5.7 | 42.9 | 2.9 | 28.6 | 25.7 | |
| Access to food (n = 28) | 60.7 | 46.4 | 25 | 25 | 28.6 | 17.9 | 0 | 7.1 | 21.4 | 0 | 25 | 17.9 | |
| Employment/income (n = 43) | 51.2 | 74.4 | 23.3 | 18.6 | 27.9 | 4.7 | 2.3 | 9.3 | 44.2 | 0 | 34.9 | 27.9 | |
| Environmental determinants of health | Air quality (n = 36) | 69.4 | 30.6 | 5.6 | 8.3 | 11.1 | 58.3 | 0 | 0 | 2.8 | 0 | 27.8 | 22.2 |
| Water quality (n = 40) | 90 | 32.5 | 10 | 12.5 | 7.5 | 82.5 | 0 | 2.5 | 5 | 2.5 | 27.5 | 10 | |
| Water quantity (n = 38) | 84.2 | 50 | 10.5 | 10.5 | 10.5 | 63.2 | 0 | 5.3 | 13.2 | 2.6 | 36.8 | 10.5 | |
| Access to drinking water (n = 42) | 66.7 | 52.4 | 26.2 | 14.3 | 28.6 | 28.6 | 0 | 9.5 | 23.8 | 0 | 33.3 | 14.3 | |
| Access to sanitation facilities (n = 31) | 67.7 | 51.6 | 25.8 | 22.6 | 32.3 | 16.1 | 3.2 | 12.9 | 29 | 0 | 29 | 9.7 | |
| Soil quality (n = 38) | 73.7 | 42.1 | 13.2 | 10.5 | 2.6 | 65.8 | 0 | 5.3 | 7.9 | 5.3 | 28.9 | 10.5 | |
| Noise (n = 33) | 84.8 | 18.2 | 9.1 | 9.1 | 15.2 | 75.8 | 0 | 3 | 3 | 0 | 15.2 | 12.1 | |
| Traffic (n = 31) | 71 | 19.4 | 19.4 | 6.5 | 6.5 | 45.2 | 0 | 3.2 | 6.5 | 0 | 12.9 | 19.4 | |
| Housing conditions (n = 34) | 67.6 | 38.2 | 20.6 | 14.7 | 26.5 | 20.6 | 0 | 11.8 | 11.8 | 0 | 26.5 | 17.6 | |
| Waste management (n = 27) | 59.3 | 33.3 | 25.9 | 14.8 | 18.5 | 3.7 | 0 | 3.7 | 14.8 | 0 | 18.5 | 22.2 | |
| Migration (n = 30) | 50 | 66.7 | 23.3 | 6.7 | 20 | 3.3 | 0 | 10 | 36.7 | 3.3 | 33.3 | 16.7 | |
| Institutional factors | Capacity of health care system (n = 40) | 52.5 | 67.5 | 20 | 15 | 7.5 | 22.5 | 15 | 5 | 25 | 0 | 30 | 22.5 |
| Capacity of trad. health system (n = 10) | 40 | 20 | 20 | 20 | 0 | 0 | 0 | 0 | 10 | 0 | 10 | 50 | |
| Capacity of MCH services (n = 20) | 50 | 65 | 25 | 5 | 10 | 20 | 15 | 5 | 40 | 5 | 15 | 5 | |
| Capacity of education facilities (n = 33) | 36.4 | 57.6 | 18.2 | 9.1 | 0 | 18.2 | 3 | 0 | 33.3 | 0 | 27.3 | 21.2 | |
| CDs related to housing and overcrowding | Acute respiratory infections (n = 3) | 32 | 68 | 16 | 16 | 12 | 0 | 36 | 4 | 20 | 4 | 20 | 32 |
| Pneumonia (n = 16) | 25 | 62.5 | 6.2 | 6.2 | 12.5 | 0 | 37.5 | 6.2 | 25 | 6.2 | 6.2 | 31.2 | |
| Tuberculosis (n = 24) | 29.2 | 87.5 | 12.5 | 8.3 | 12.5 | 0 | 33.3 | 8.3 | 25 | 4.2 | 33.3 | 20.8 | |
| Meningitis (n = 11) | 27.3 | 81.8 | 18.2 | 9.1 | 9.1 | 0 | 18.2 | 9.1 | 27.3 | 0 | 27.3 | 0 | |
| Vector-related diseases | Malaria (n = 35) | 45.7 | 71.4 | 17.1 | 25.7 | 25.7 | 5.7 | 31.4 | 5.7 | 22.9 | 2.9 | 28.6 | 34.3 |
| Arboviral diseases (n = 8) | 0 | 87.5 | 0 | 0 | 0 | 0 | 37.5 | 0 | 25 | 12.5 | 12.5 | 12.5 | |
| Lymphatic filariasis (n = 8) | 12.5 | 87.5 | 0 | 0 | 12.5 | 12.5 | 50 | 0 | 50 | 25 | 12.5 | 12.5 | |
| Leishmaniasis (n = 1) | 0 | 100 | 0 | 0 | 0 | 0 | 0 | 0 | 100 | 0 | 0 | 0 | |
| African trypanosomiasis (n = 2) | 0 | 50 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 50 | 50 | |
| Onchocerciasis (n = 7) | 28.6 | 57.1 | 14.3 | 0 | 14.3 | 0 | 28.6 | 0 | 28.6 | 0 | 14.3 | 14.3 | |
| Soil-, water- and waste-related diseases | Diarrheal diseases (n = 33) | 39.4 | 69.7 | 12.1 | 15.2 | 24.2 | 0 | 33.3 | 6.1 | 15.2 | 0 | 27.3 | 24.2 |
| Schistosomiasis (n = 8) | 50 | 37.5 | 25 | 12.5 | 0 | 25 | 25 | 0 | 12.5 | 12.5 | 0 | 25 | |
| Hepatitis A/E (n = 1) | 0 | 100 | 0 | 0 | 0 | 0 | 0 | 0 | 100 | 0 | 0 | 0 | |
| Soil-transmitted helminths (n = 13) | 30.8 | 76.9 | 7.7 | 0 | 7.7 | 15.4 | 38.5 | 0 | 23.1 | 7.7 | 30.8 | 7.7 | |
| Sexually-transmitted infections | HIV/AIDS (n = 35) | 40 | 82.9 | 22.9 | 8.6 | 17.1 | 0 | 25.7 | 22.9 | 28.6 | 2.9 | 42.9 | 20 |
| Syphilis (n = 7) | 42.9 | 71.4 | 14.3 | 14.3 | 14.3 | 14.3 | 14.3 | 0 | 57.1 | 0 | 14.3 | 14.3 | |
| Unplanned pregnancies (n = 12) | 41.7 | 66.7 | 8.3 | 33.3 | 16.7 | 0 | 50 | 8.3 | 16.7 | 0 | 0 | 8.3 | |
| Gonorrhea (n = 8) | 25 | 87.5 | 12.5 | 0 | 12.5 | 0 | 37.5 | 0 | 50 | 0 | 12.5 | 12.5 | |
| Zoonoses | Any zoonotic disease (n = 6) | 16.7 | 33.3 | 16.7 | 0 | 0 | 0 | 16.7 | 0 | 16.7 | 16.7 | 16.7 | 83.3 |
| Non-communicable diseases | Cardio-vascular diseases (n = 14) | 35.7 | 71.4 | 14.3 | 14.3 | 0 | 14.3 | 28.6 | 0 | 21.4 | 7.1 | 28.6 | 14.3 |
| Cancer (n = 7) | 14.3 | 85.7 | 14.3 | 0 | 0 | 0 | 28.6 | 0 | 14.3 | 0 | 57.1 | 14.3 | |
| Diabetes (n = 11) | 27.3 | 81.8 | 27.3 | 9.1 | 0 | 0 | 45.5 | 0 | 18.2 | 9.1 | 18.2 | 18.2 | |
| Chronic respiratory diseases (n = 13) | 15.4 | 84.6 | 15.4 | 0 | 0 | 0 | 30.8 | 0 | 38.5 | 0 | 23.1 | 15.4 | |
| Accidents and injuries | Traffic-related injuries (n = 18) | 27.8 | 77.8 | 16.7 | 16.7 | 5.6 | 0 | 27.8 | 0 | 27.8 | 0 | 38.9 | 11.1 |
| Work-related injuries (n = 7) | 28.6 | 85.7 | 0 | 0 | 28.6 | 0 | 42.9 | 0 | 42.9 | 0 | 28.6 | 0 | |
| Interpersonal violence (n = 10) | 40 | 50 | 30 | 20 | 10 | 0 | 20 | 0 | 10 | 0 | 20 | 20 | |
| Food- and nutrition-related issues | Anemia (n = 14) | 35.7 | 71.4 | 14.3 | 0 | 14.3 | 14.3 | 42.9 | 7.1 | 28.6 | 0 | 7.1 | 28.6 |
| Undernutrition (n = 21) | 23.8 | 71.4 | 23.8 | 14.3 | 4.8 | 14.3 | 33.3 | 14.3 | 23.8 | 0 | 23.8 | 23.8 | |
| Overweight (n = 4) | 50 | 75 | 25 | 25 | 25 | 25 | 25 | 25 | 25 | 25 | 25 | 0 | |
| Food-borne diseases (n = 4) | 25 | 100 | 25 | 0 | 0 | 0 | 75 | 0 | 50 | 0 | 0 | 0 | |
| MNCH | Child immunization (n = 17) | 29.4 | 82.4 | 11.8 | 5.9 | 11.8 | 0 | 23.5 | 17.6 | 29.4 | 5.9 | 29.4 | 17.6 |
| Maternal mortality (n = 15) | 13.3 | 93.3 | 6.7 | 6.7 | 6.7 | 0 | 33.3 | 13.3 | 46.7 | 0 | 20 | 13.3 | |
| Child mortality (n = 18) | 5.6 | 94.4 | 0 | 0 | 5.6 | 0 | 27.8 | 16.7 | 44.4 | 0 | 27.8 | 16.7 | |
| Mental health | Anxiety/depression (n = 4) | 50 | 75 | 25 | 25 | 25 | 0 | 0 | 0 | 25 | 0 | 50 | 0 |
| Self-harm/suicide (n = 0) | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | n.a. | |
References
- Esteves, A.M.; Franks, D.; Vanclay, F. Social impact assessment: The state of the art. Impact Assess Proj. Apprais. 2012, 30, 34–42. [Google Scholar] [CrossRef]
- Harris-Roxas, B.; Viliani, F.; Bond, A.; Cave, B.; Divall, M.; Furu, P.; Harris, P.; Soeberg, M.; Wernham, A.; Winkler, M. Health impact assessment: The state of the art. Impact Assess Proj. Apprais. 2012, 30, 43–52. [Google Scholar] [CrossRef]
- Morgan, R.K. Environmental impact assessment: The state of the art. Impact Assess Proj. Apprais. 2012, 30, 5–14. [Google Scholar] [CrossRef]
- Mindell, J.; Joffe, M. Health impact assessment in relation to other forms of impact assessment. J. Public Health Med. 2003, 25, 107–112. [Google Scholar] [CrossRef] [Green Version]
- Harris-Roxas, B.; Harris, E. Differing forms, differing purposes: A typology of health impact assessment. Environ. Impact Asses. 2011, 31, 396–403. [Google Scholar] [CrossRef]
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Balge, M.Z.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: The centrality of scoping. Environ. Impact Asses. 2011, 31, 310–319. [Google Scholar] [CrossRef]
- Winkler, M.S.; Furu, P.; Viliani, F.; Cave, B.; Divall, M.; Ramesh, G.; Harris-Roxas, B.; Knoblauch, A.M. Current global health impact assessment practice. Int. J. Environ. Res. Public Health 2020, 17, 2988. [Google Scholar] [CrossRef] [PubMed]
- Nigri, G.; Michelini, L. A systematic literature review on social impact assessment: Outlining main dimensions and future research lines. In International Dimensions of Sustainable Management: Latest Perspectives from Corporate Governance, Responsible Finance and CSR; Schmidpeter, R., Capaldi, N., Idowu, S.O., Stürenberg Herrera, A., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 53–67. [Google Scholar]
- Bhatia, R.; Wernham, A. Integrating human health into environmental impact assessment: An unrealized opportunity for environmental health and justice. Environ. Health Perspect. 2009, 14, 1159–1175. [Google Scholar] [CrossRef] [PubMed]
- Green, L.; Gray, B.J.; Edmonds, N.; Parry-Williams, L. Development of a quality assurance review framework for health impact assessments. Impact Assess. Proj. Apprais. 2019, 37, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Steinemann, A. Rethinking human health impact assessment. Environ. Impact Asses. 2000, 20, 627–645. [Google Scholar] [CrossRef]
- Harris, P.J.; Harris, E.; Thompson, S.; Harris-Roxas, B.; Kemp, L. Human health and wellbeing in environmental impact assessment in New South Wales, Australia: Auditing health impacts within environmental assessments of major projects. Environ. Impact Asses. 2009, 29, 310–318. [Google Scholar] [CrossRef]
- Fischer, T.B.; Matuzzi, M.; Nowacki, J. The consideration of health in strategic environmental assessment (SEA). Environ. Impact Asses. 2010, 30, 200–210. [Google Scholar] [CrossRef]
- Baumgart, S.; Hartlik, J.; Machtolf, M. Improving the consideration of human health in environmental planning and decision-making—Perspectives from Germany. Impact Assess. Proj. Apprais. 2018, 36, 57–67. [Google Scholar] [CrossRef]
- Riley, E.; Harris, P.; Kent, J.; Sainsbury, P.; Lane, A.; Baum, F. Including health in environmental assessments of major transport infrastructure projects: A documentary analysis. Int. J. Health Policy 2018, 7, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Riley, E.; Sainsbury, P.; McManus, P.; Colagiuri, R.; Viliani, F.; Dawson, A.; Duncan, E.; Stone, Y.; Pham, T.; Harris, P. Including health impacts in environmental impact assessments for three Australian coal-mining projects: A documentary analysis. Health Promot. Int. 2019. [Google Scholar] [CrossRef] [PubMed]
- Erlanger, T.E.; Krieger, G.R.; Singer, B.H.; Utzinger, J. The 6/94 gap in health impact assessment. Environ. Impact Asses. 2008, 28, 349–358. [Google Scholar] [CrossRef]
- Winkler, M.S.; Krieger, G.R.; Divall, M.J.; Cisse, G.; Wielga, M.; Singer, B.H.; Tanner, M.; Utzinger, J. Untapped potential of health impact assessment. Bull. World Health Organ. 2013, 91, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Chilaka, M.A.; Ndioho, I. Health impact assessment in Nigeria: An initiative whose time has come. J. Public Health Afr. 2020, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Balge, M.Z.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: Advancing tools and methods. Environ. Impact Asses. 2010, 30, 52–61. [Google Scholar] [CrossRef]
- Krieger, G.; Singer, B.; Winkler, M.; Divall, M.; Tanner, M.; Utzinger, J. Health impact assessment in developing countries. In Health Impact Assessment: Past Achievement, Current Understanding, and Future Progress; Kemm, J., Ed.; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Brisbois, B.W.; Reschny, J.; Fyfe, T.M.; Harder, H.G.; Parkes, M.W.; Allison, S.; Buse, C.G.; Fumerton, R.; Oke, B. Mapping research on resource extraction and health: A scoping review. Extr. Ind. Soc. 2019, 6, 250–259. [Google Scholar] [CrossRef]
- United Nations Economic Commission for Africa. Minerals and Africa’s Development: The International Study Group Report on Africa’s Mineral Regimes; United Nations Economic Commission for Africa: Addis Abeba, Ethiopia, 2011. [Google Scholar]
- Arrobas, D.L.P.; Hund, K.L.; Mccormick, M.S.; Ningthoujam, J.; Drexhage, J.R. The Growing Role of Minerals and Metals for a Low Carbon Future; World Bank Group: Washington, DC, USA, 2017. [Google Scholar]
- Saha, S.; Pattanayak, S.K.; Sills, E.O.; Singha, A.K. Under-mining health: Environmental justice and mining in India. Health Place 2011, 17, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Knoblauch, A.M.; Divall, M.J.; Owuor, M.; Archer, C.; Nduna, K.; Ng’uni, H.; Musunka, G.; Pascall, A.; Utzinger, J.; Winkler, M.S. Monitoring of selected health indicators in children living in a copper mine development area in northwestern Zambia. Int. J. Environ. Res. Public Health 2017, 14, 315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mactaggart, F.; McDermott, L.; Tynan, A.; Whittaker, M. Exploring the broader health and well-being outcomes of mining communities in low- and middle-income countries: A systematic review. Glob. Public Health 2018, 13, 899–913. [Google Scholar] [CrossRef] [PubMed]
- Wilches-Gutierrez, J.; Documet, P. What is known about sexual and reproductive health in latin American and Caribbean mining contexts? A systematic scoping review. Public Health Rev. 2018, 39, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noronha, L. Designing tools to track health and well-being in mining regions of India. Nat. Resour. Forum. 2001, 25, 53–65. [Google Scholar] [CrossRef]
- Yelpaala, K.; Ali, S.H. Multiple scales of diamond mining in Akwatia, Ghana: Addressing environmental and human development impact. Resour. Policy 2005, 30, 145–155. [Google Scholar] [CrossRef]
- Sun, H.-P.; Sun, W.-F.; Geng, Y.; Kong, Y.-S. Natural resource dependence, public education investment, and human capital accumulation. Pet. Sci. 2018, 15, 657–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von der Goltz, J.; Barnwal, P. Mines: The local wealth and health effects of mineral mining in developing countries. J. Dev. Econ. 2019, 139, 1–16. [Google Scholar] [CrossRef]
- Sun, H.-P.; Sun, W.-F.; Geng, Y.; Yang, X.; Edziah, B.K. How does natural resource dependence affect public education spending? Environ. Sci. Pollut. Res. 2019, 26, 3666–3674. [Google Scholar] [CrossRef] [PubMed]
- Dietler, D.; Farnham, A.; de Hoogh, K.; Winkler, M.S. Quantification of annual settlement growth in rural mining areas using machine learning. Remote Sens. 2020, 12, 235. [Google Scholar] [CrossRef] [Green Version]
- IPIECA; UNDP; IFC. Mapping the Oil and Gas Industry to the Sustainable Development Goals: An Atlas; IPIECA: London, UK; United Nations Development Programme: New York, NY, USA; International Finance Corporation: Washington, DC, USA, 2017. [Google Scholar]
- Standard & Poor’s Global. Market Intelligence Platform. Available online: https://www.spglobal.com/marketintelligence/en/solutions/market-intelligence-platform (accessed on 5 May 2020).
- Azevedo, S. Investigating the Inclusion of Health in Impact Assessment Reports of Natural Resource Extraction Projects in Sub-Saharan Africa; Term Paper; ETH Zurich: Zurich, Switzerland, 2019. [Google Scholar]
- Winkler, M.S.; Adongo, P.B.; Binka, F.; Brugger, F.; Diagbouga, S.; Macete, E.; Munguambe, K.; Okumu, F. Health impact assessment for promoting sustainable development: The HIA4SD project. Impact Assess Proj. Apprais. 2020, 38, 225–232. [Google Scholar] [CrossRef] [Green Version]
- Farnham, A.; Cossa, H.; Dietler, D.; Engebretsen, R.; Leuenberger, A.; Lyatuu, I.; Nimako, B.; Zabre, H.R.; Brugger, F.; Winkler, M.S. Investigating health impacts of natural resource extraction projects in Burkina Faso, Ghana, Mozambique, and Tanzania: Protocol for a mixed methods study. JMIR Res. Protoc. 2020, 9, e17138. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Op 4.01—Environmental Assessment; World Bank: Washington, DC, USA, 1999. [Google Scholar]
- International Finance Corporation. Interpretation Note on Environmental and Social Categorization. Available online: https://www.ifc.org/wps/wcm/connect/f873da60-4adf-4fa0-83ec-729227aa5511/Interpretation+Note+on+E+and+S+Categorization.pdf?MOD=AJPERES&CVID=mUtZ0yc (accessed on 26 March 2020).
- International Finance Corporation. Performance Standards on Environmental and Social Sustainability; International Finance Corporation: Washington, DC, USA, 2012. [Google Scholar]
- International Finance Corporation. Introduction to Health Impact Assessment; International Finance Corporation: Washington, DC, USA, 2009. [Google Scholar]
- Quigley, R.; den Broeder, L.; Furu, P.; Bond, A.; Cave, B.; Bos, R. Health Impact Assessment International Best Practice Principles: Special Publication Series no 5; International Association for Impact Assessment: Fargo, ND, USA, 2006. [Google Scholar]
- R Core Team. R.: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- The Equator Principles Association. Equator Principles Association Members & Reporting. Available online: https://equator-principles.com/members-reporting/ (accessed on 24 April 2020).
- The Equator Principles Association. The Equator Principles: A Financial Industry Benchmark for Determining, Assessing and Managing Environmental and Social Risk in Projects. Available online: https://equator-principles.com/wp-content/uploads/2020/01/The-Equator-Principles-July-2020.pdf (accessed on 24 April 2020).
- Krieger, G.R.; Utzinger, J.; Winkler, M.S.; Divall, M.J.; Phillips, S.D.; Balge, M.Z.; Singer, B.H. Barbarians at the gate: Storming the Gothenburg consensus. Lancet 2010, 375, 2129–2131. [Google Scholar] [CrossRef]
- Franks, D.M.; Vanclay, F. Social impact management plans: Innovation in corporate and public policy. Environ. Impact Asses. 2013, 43, 40–48. [Google Scholar] [CrossRef]
- International Finance Corporation. International Finance Corporation: Access to Information Policy; International Finance Corporation: Washington, DC, USA, 2012. [Google Scholar]
- Aung, T.S. Evaluation of the environmental impact assessment system and implementation in Myanmar: Its significance in oil and gas industry. Environ. Impact Asses. 2017, 66, 24–32. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe; European Centre for Health Policy. Health Impact Assessment: Main Concepts and Suggested Approach: The Gothenburg Consensus Paper. Available online: http://www.impactsante.ch/pdf/HIA_Gothenburg_consensus_paper_1999 (accessed on 4 March 2020).
- Winkler, M.S.; Viliani, F.; Knoblauch, A.M.; Cave, B.; Divall, M.; Ramesh, G.; Harris-Roxas, B.; Furu, P. Health Impact Assessment International Best Practice Principles; International Association for Impact Assessment: Fargo, ND, USA, 2020; in preparation. [Google Scholar]
- Pham, T.; Riley, E.; Harris, P. Inclusion of health in environmental impact assessment of major transport infrastructure projects in Vietnam. Int. J. Health Policy 2018, 7, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Thondoo, M.; Rojas-Rueda, D.; Gupta, J.; de Vries, D.H.; Nieuwenhuijsen, M.J. Systematic literature review of health impact assessments in low and middle-income countries. Int. J. Environ. Res. Public Health 2019, 16, 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Schmidlin, S.; Magassouba, M.L.; Knoblauch, A.M.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: Modular baseline health surveys. Environ. Impact Asses. 2012, 33, 15–22. [Google Scholar] [CrossRef]
- Farnham, A.; Utzinger, J.; Kulinkina, A.V.; Winkler, M.S. Using district health information to monitor sustainable development. Bull. World Health Organ. 2020, 98, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.; Parry, J.; Mathers, J. Participation in health impact assessment: Objectives, methods and core values. Bull. World Health Organ. 2005, 83, 58–63. [Google Scholar] [PubMed]
- O’Faircheallaigh, C. Public participation and environmental impact assessment: Purposes, implications, and lessons for public policy making. Environ. Impact Asses. 2010, 30, 19–27. [Google Scholar] [CrossRef]
- Chilaka, M.A. Drawing from the well of community participation: An evaluation of the utility of local knowledge in the health impact assessment process. Community Dev. 2015, 46, 100–110. [Google Scholar] [CrossRef]
- den Broeder, L.; Uiters, E.; ten Have, W.; Wagemakers, A.; Schuit, A.J. Community participation in health impact assessment. A scoping review of the literature. Environ. Impact Asses. 2017, 66, 33–42. [Google Scholar] [CrossRef]
- Buse, C.G.; Lai, V.; Cornish, K.; Parkes, M.W. Towards environmental health equity in health impact assessment: Innovations and opportunities. Int. J. Public Health 2019, 64, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Leuenberger, A.; Farnham, A.; Azevedo, S.; Cossa, H.; Dietler, D.; Nimako, B.; Adongo, P.B.; Merten, S.; Utzinger, J.; Winkler, M.S. Health impact assessment and health equity in sub-Saharan Africa: A scoping review. Environ. Impact Asses. 2019, 79, 106288. [Google Scholar] [CrossRef]
- Knoblauch, A.M.; Hodges, M.H.; Bah, M.S.; Kamara, H.I.; Kargbo, A.; Paye, J.; Turay, H.; Nyorkor, E.D.; Divall, M.J.; Zhang, Y.; et al. Changing patterns of health in communities impacted by a bioenergy project in northern Sierra Leone. Int. J. Environ. Res. Public Health 2014, 11, 12997–13016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knoblauch, A.M.; Divall, M.J.; Owuor, M.; Nduna, K.; Ng’uni, H.; Musunka, G.; Pascall, A.; Utzinger, J.; Winkler, M.S. Experience and lessons from health impact assessment guiding prevention and control of HIV/AIDS in a copper mine project, northwestern Zambia. Infect. Dis. Poverty 2017, 6, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dietler, D.; Lewinski, R.; Azevedo, S.; Engebretsen, R.; Brugger, F.; Utzinger, J.; Winkler, M.S. Inclusion of Health in Impact Assessment: A Review of Current Practice in Sub-Saharan Africa. Int. J. Environ. Res. Public Health 2020, 17, 4155. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114155
Dietler D, Lewinski R, Azevedo S, Engebretsen R, Brugger F, Utzinger J, Winkler MS. Inclusion of Health in Impact Assessment: A Review of Current Practice in Sub-Saharan Africa. International Journal of Environmental Research and Public Health. 2020; 17(11):4155. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114155
Chicago/Turabian StyleDietler, Dominik, Ruth Lewinski, Sophie Azevedo, Rebecca Engebretsen, Fritz Brugger, Jürg Utzinger, and Mirko S. Winkler. 2020. "Inclusion of Health in Impact Assessment: A Review of Current Practice in Sub-Saharan Africa" International Journal of Environmental Research and Public Health 17, no. 11: 4155. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114155