Fear of COVID-19 Scale—Associations of Its Scores with Health Literacy and Health-Related Behaviors among Medical Students

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Settings
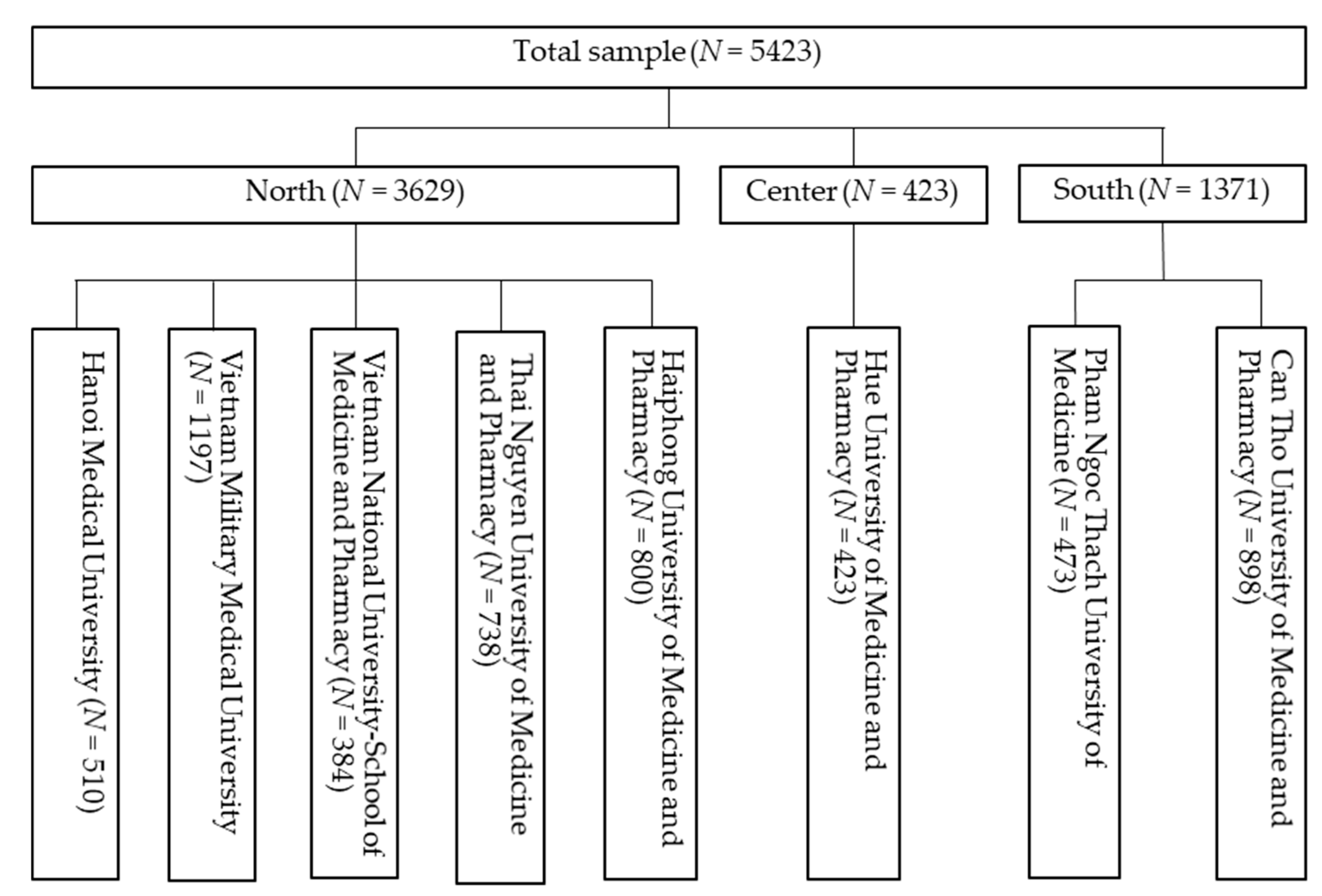
2.2. Study Participants
2.3. Assessments and Measurements
2.3.1. Social Demographics and Clinical Indicators
2.3.2. Health-Related Behaviors
2.3.3. Health Literacy
2.3.4. Fear of COVID-19
2.4. Data Collection Procedure
2.5. Data Analysis
2.6. Ethical Consideration
3. Results
3.1. Participants’ Characteristics
3.2. Psychometric Properties of FCoV-19
3.3. Factors Associated with FCoV-19
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The Lancet Infectious Diseases. COVID-19: Endgames. Lancet Infect. Dis. 2020, 20, 511. [Google Scholar] [CrossRef]
- Duan, H.; Wang, S.; Yang, C. Coronavirus: Limit short-term economic damage. Nature 2020, 578, 515. [Google Scholar] [CrossRef] [Green Version]
- Rosenbaum, L. The Untold Toll—The Pandemic’s Effects on Patients without Covid-19. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Coronavirus Disease (COVID-2019) Situation Reports; WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 4 May 2020).
- Ministry of Health. Coronavirus Disease (COVID-19) Outbreak in VIETNAM. Available online: https://ncov.moh.gov.vn/ (accessed on 4 May 2020).
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV Epidemic: Address Mental Health Care to Empower Society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.; Li, S.; Tian, S.; Li, H.; Kong, L.-Q. Full spectrum of COVID-19 severity still being depicted. Lancet 2020, 395, 947–948. [Google Scholar] [CrossRef]
- Lazzerini, M.; Barbi, E.; Apicella, A.; Marchetti, F.; Cardinale, F.; Trobia, G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc. Health 2020, 4, e10–e11. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Sanchez, V.; Adiukwu, F.; El Hayek, S.; Bytyçi, D.G.; Gonzalez-Diaz, J.M.; Kundadak, G.K.; Larnaout, A.; Nofal, M.; Orsolini, L.; Ramalho, R.; et al. COVID-19 effect on mental health: Patients and workforce. Lancet Psychiatry 2020, 7, e29–e30. [Google Scholar] [CrossRef]
- Shimizu, K. 2019-nCoV, fake news, and racism. Lancet 2020, 395, 685–686. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Paige, S.R.; Krieger, J.L.; Stellefson, M.L. The Influence of eHealth Literacy on Perceived Trust in Online Health Communication Channels and Sources. J. Health Commun. 2017, 22, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, H.C.; Nguyen, M.H.; Do, B.N.; Tran, C.Q.; Nguyen, T.T.P.; Pham, K.M.; Pham, L.V.; Tran, K.V.; Duong, T.T.; Tran, T.V.; et al. People with Suspected COVID-19 Symptoms Were More Likely Depressed and Had Lower Health-Related Quality of Life: The Potential Benefit of Health Literacy. J. Clin. Med. 2020, 9, 965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaper, M.S.; Reijneveld, S.A.; van Es, F.D.; de Zeeuw, J.; Almansa, J.; Koot, J.A.R.; de Winter, A.F. Effectiveness of a Comprehensive Health Literacy Consultation Skills Training for Undergraduate Medical Students: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 17, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, N.K.; Ferguson, R.P.; Mitha, S.; Hanlon, A. Do medical trainees feel confident communicating with low health literacy patients? J. Community Hosp. Intern. Med. Perspect. 2014, 4, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Shaikh, A.; Singh, R.; Singh, A.K. COVID-19: From bench to bed side. Diabetes Metab. Syndr. 2020, 14, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.-Y.; Jian, S.-W.; Liu, D.-P.; Ng, T.-C.; Huang, W.-T.; Lin, H.-H. For the Taiwan COVID-19 Outbreak Investigation Team. Contact Tracing Assessment of COVID-19 Transmission Dynamics in Taiwan and Risk at Different Exposure Periods Before and After Symptom Onset. JAMA Intern. Med. 2020, e202020. [Google Scholar]
- Lai, S.; Ruktanonchai, N.W.; Zhou, L.; Prosper, O.; Luo, W.; Floyd, J.R.; Wesolowski, A.; Santillana, M.; Zhang, C.; Du, X.; et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature 2020. [Google Scholar] [CrossRef]
- Armitage, R.; Nellums, L.B. COVID-19 and the consequences of isolating the elderly. Lancet Public Health 2020, 5, e256. [Google Scholar] [CrossRef] [Green Version]
- Lima, C.K.T.; Carvalho, P.M.M.; Lima, I.; Nunes, J.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.L.; Neto, M.L.R. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Qiao, M.; Jiang, R.; Bi, J.; Zhan, G.; Xu, X.; Wang, L.; et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain Behav. Immun. 2020. [Google Scholar] [CrossRef]
- Wu, W.; Zhang, Y.; Wang, P.; Zhang, L.; Wang, G.; Lei, G.; Xiao, Q.; Cao, X.; Bian, Y.; Xie, S.; et al. Psychological stress of medical staffs during outbreak of COVID-19 and adjustment strategy. J. Med. Virol. 2020. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Mental Health and the Covid-19 Pandemic. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Gallagher, T.H.; Schleyer, A.M. “We Signed Up for This!”—Student and Trainee Responses to the Covid-19 Pandemic. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bauchner, H.; Sharfstein, J. A Bold Response to the COVID-19 Pandemic: Medical Students, National Service, and Public Health. JAMA 2020, 323, 1790–1791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, D.; Wilder-Smith, A. The global community needs to swiftly ramp up the response to contain COVID-19. Lancet 2020, 395, 1109–1110. [Google Scholar] [CrossRef]
- Baker, D.M.; Bhatia, S.; Brown, S.; Cambridge, W.; Kamarajah, S.K.; McLean, K.A.; Brindl, N.; Lapolla, P.; Pérez-Ajates, S.; Raubenheimer, K.; et al. Medical student involvement in the COVID-19 response. Lancet 2020, 395, 1254. [Google Scholar] [CrossRef]
- Rasmussen, S.; Sperling, P.; Poulsen, M.S.; Emmersen, J.; Andersen, S. Medical students for health-care staff shortages during the COVID-19 pandemic. Lancet 2020, 395, e79–e80. [Google Scholar] [CrossRef]
- Pham, T.; Bui, L.; Nguyen, A.; Nguyen, B.; Tran, P.; Vu, P.; Dang, L. The prevalence of depression and associated risk factors among medical students: An untold story in Vietnam. PLoS ONE 2019, 14, e0221432. [Google Scholar] [CrossRef]
- Goyal, K.; Chauhan, P.; Chhikara, K.; Gupta, P.; Singh, M.P. Fear of COVID 2019: First suicidal case in India! Asian J. Psychiatr. 2020, 49, 101989. [Google Scholar] [CrossRef]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Duan, L.; Zhu, G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 2020, 7, 300–302. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Editorial Team. Overview of Novel Coronavirus (2019-nCoV). BMJ Best Practice. Available online: https://0-bestpractice-bmj-com.brum.beds.ac.uk/topics/en-gb/3000165 (accessed on 10 February 2020).
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and Validating the Charlson Comorbidity Index and Score for Risk Adjustment in Hospital Discharge Abstracts Using Data From 6 Countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Duong, T.V.; Aringazina, A.; Baisunova, G.; Nurjanah, N.; Pham, T.V.; Pham, K.M.; Truong, T.Q.; Nguyen, K.T.; Oo, W.M.; Su, T.T.; et al. Development and validation of a new short-form health literacy instrument (HLS-SF12) for the general public in six Asian countries. Health Lit. Res. Pract. 2019, 3, e91–e102. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, K.; Van den Broucke, S.; Brand, H.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonszka, Z. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Duong, T.V.; Chang, P.W.; Yang, S.-H.; Chen, M.-C.; Chao, W.-T.; Chen, T.; Chiao, P.; Huang, H.-L. A new comprehensive short-form health literacy survey tool for patients in general. Asian Nurs. Res. (Korean Soc. Nurs. Sci.) 2017, 11, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Duong, T.V.; Nguyen, T.T.P.; Pham, K.M.; Nguyen, K.T.; Giap, M.H.; Tran, T.D.X.; Nguyen, C.X.; Yang, S.-H.; Su, C.-T. Validation of the Short-Form Health Literacy Questionnaire (HLS-SF12) and Its Determinants among People Living in Rural Areas in Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 3346. [Google Scholar] [CrossRef] [Green Version]
- Ho, H.V.; Hoang, G.T.; Pham, V.T.; Duong, T.V.; Pham, K.M. Factors associated with health literacy among the elderly people in Vietnam. Biomed. Res. Int. 2020, 2020, 1–7. [Google Scholar]
- HLS-EU Consortium. Comparative Report of Health literacy in Eight EU Member States. The European Health Literacy Project 2009–2012. Maastricht University. Available online: https://www.healthliteracyeurope.net/hls-eu (accessed on 22 October 2012).
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Pollack, A.A.; Weiss, B.; Trung, L.T. Mental health, life functioning and risk factors among people exposed to frequent natural disasters and chronic poverty in Vietnam. BJPsych Open 2016, 2, 221–232. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Monahan, P.O.; Löwe, B. Anxiety disorders in primary care: Prevalence, impairment, comorbidity, and detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef]
- Plummer, F.; Manea, L.; Trepel, D.; McMillan, D. Screening for anxiety disorders with the GAD-7 and GAD-2: A systematic review and diagnostic metaanalysis. Gen. Hosp. Psychiatry 2016, 39, 24–31. [Google Scholar] [CrossRef]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Cronbach, L.J.; Shavelson, R.J. My current thoughts on coefficient alpha and successor procedures. Educ. Psychol. Meas. 2004, 64, 391–418. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Maldonado, G.; Greenland, S. Simulation Study of Confounder-Selection Strategies. Am. J. Epidemiol. 1993, 138, 923–936. [Google Scholar] [CrossRef] [Green Version]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; Sage: London, UK, 2013. [Google Scholar]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression, 3rd ed.; John Wiley & Sons: New York, NY, USA, 2013; p. 500. [Google Scholar]
- The, L. The gendered dimensions of COVID-19. Lancet 2020, 395, 1168. [Google Scholar]
- Harkness, K.L.; Alavi, N.; Monroe, S.M.; Slavich, G.M.; Gotlib, I.H.; Bagby, R.M. Gender differences in life events prior to onset of major depressive disorder: The moderating effect of age. J. Abnorm. Psychol. 2010, 119, 791–803. [Google Scholar] [CrossRef] [Green Version]
- Conklin, A.I.; Guo, S.X.; Tam, A.C.; Richardson, C.G. Gender, stressful life events and interactions with sleep: A systematic review of determinants of adiposity in young people. BMJ Open 2018, 8, e019982. [Google Scholar] [CrossRef] [Green Version]
- Evans, T.M.; Bira, L.; Gastelum, J.B.; Weiss, L.T.; Vanderford, N.L. Evidence for a mental health crisis in graduate education. Nat. Biotechnol. 2018, 36, 282–284. [Google Scholar] [CrossRef] [PubMed]
- Eaton, N.R.; Keyes, K.M.; Krueger, R.F.; Balsis, S.; Skodol, A.E.; Markon, K.E.; Grant, B.F.; Hasin, D.S. An invariant dimensional liability model of gender differences in mental disorder prevalence: Evidence from a national sample. J. Abnorm. Psychol. 2012, 121, 282–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woolston, C. A better future for graduate-student mental health. Nature 2019. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Swendsen, J.; Conway, K.P.; Degenhardt, L.; Glantz, M.; Jin, R.; Merikangas, K.R.; Sampson, N.; Kessler, R.C. Mental disorders as risk factors for substance use, abuse and dependence: Results from the 10-year follow-up of the National Comorbidity Survey. Addiction 2010, 105, 1117–1128. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, B.; Veronese, N.; Vancampfort, D.; Prina, A.M.; Lin, P.Y.; Tseng, P.T.; Evangelou, E.; Solmi, M.; Kohler, C.; Carvalho, A.F.; et al. Perceived stress and smoking across 41 countries: A global perspective across Europe, Africa, Asia and the Americas. Sci. Rep. 2017, 7, 7597. [Google Scholar] [CrossRef]
- Choi, D.; Ota, S.; Watanuki, S. Does cigarette smoking relieve stress? Evidence from the event-related potential (ERP). Int. J. Psychophysiol. 2015, 98, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Awaworyi Churchill, S.; Farrell, L. Alcohol and depression: Evidence from the 2014 health survey for England. Drug Alcohol Depend. 2017, 180, 86–92. [Google Scholar] [CrossRef]
- Gasmi, A.; Noor, S.; Tippairote, T.; Dadar, M.; Menzel, A.; Bjørklund, G. Individual risk management strategy and potential therapeutic options for the COVID-19 pandemic. Clin. Immunol. 2020, 215, 108409. [Google Scholar] [CrossRef]
- Vardavas, C.I.; Nikitara, K. COVID-19 and smoking: A systematic review of the evidence. Tob. Induc. Dis. 2020, 18, 20. [Google Scholar] [CrossRef]
- Diviani, N.; van den Putte, B.; Giani, S.; van Weert, J.C. Low Health Literacy and Evaluation of Online Health Information: A Systematic Review of the Literature. J. Med. Internet Res. 2015, 17, e112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, C.D.; Skinner, H.A. eHealth Literacy: Essential Skills for Consumer Health in a Networked World. J. Med. Internet Res. 2006, 8, e9. [Google Scholar] [CrossRef] [PubMed]
- Duong, T.V.; Lin, I.-F.; Sørensen, K.; Pelikan, J.M.; Van den Broucke, S.; Lin, Y.-C.; Chang, P.W. Health literacy in Taiwan: A population-based study. Asia-Pac. J. Public Health 2015, 27, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Kayupova, G.; Turdaliyeva, B.; Tulerayev, K.; Duong, T.V.; Chang, P.W.; Zagulova, D. Health literacy among visitors of district polyclinics in Almaty, Kazakhstan. Iran. J. Public Health 2017, 46, 1062–1070. [Google Scholar] [PubMed]
- Watson, R. Europeans with poor "health literacy" are heavy users of health services. BMJ 2011, 343, d7741. [Google Scholar] [CrossRef]
- Greenhalgh, T. Health literacy: Towards system level solutions. BMJ 2015, 350, h1026. [Google Scholar] [CrossRef] [Green Version]
- Paakkari, L.; Okan, O. COVID-19: Health literacy is an underestimated problem. Lancet Public Health 2020, 5, e249–e250. [Google Scholar] [CrossRef]
- Sentell, T.; Vamos, S.; Okan, O. Interdisciplinary Perspectives on Health Literacy Research Around the World: More Important Than Ever in a Time of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3010. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Total (n = 5423) | FCoV-19S (n = 5423) | |
|---|---|---|---|
| Frequency (%) | Mean ± SD | p * | |
| Age, year | <0.001 | ||
| 19–22 | 3162 (58.3) | 17.0 ± 5.3 | |
| 23–26 | 2261 (41.6) | 16.0 ± 5.1 | |
| Gender | <0.001 | ||
| Women | 2821 (52.0) | 17.0 ± 4.8 | |
| Men | 2602 (47.9) | 16.2 ± 5.6 | |
| Ability to pay for medication | <0.001 | ||
| Very or fairly difficult | 2496 (46.0) | 16.9 ± 5.3 | |
| Very or fairly easy | 2927 (53.9) | 16.4 ± 5.1 | |
| BMI, kg/m2 | 0.018 | ||
| Underweight (BMI < 18.5) | 945 (17.4) | 17.0 ± 4.8 | |
| Normal weight (18.5 ≤ BMI < 25.0) | 4034 (74.3) | 16.5 ± 5.3 | |
| Overweight/obese (BMI ≥ 25.0) | 444 (8.2) | 16.7 ± 5.5 | |
| Academic year | <0.001 | ||
| 1 | 1171 (21.5) | 17.0 ± 5.3 | |
| 2 | 773 (14.2) | 17.3 ± 5.5 | |
| 3 | 762 (14.0) | 17.2 ± 5.2 | |
| 4 | 738 (13.6) | 16.9 ± 5.2 | |
| 5 | 920 (16.9) | 15.9 ± 5.2 | |
| 6 | 1059 (19.5) | 15.8 ± 4.9 | |
| S-COVID-19-S ** | 0.186 | ||
| No | 4396 (81.0) | 16.6 ± 5.3 | |
| Yes | 1027 (18.9) | 16.8 ± 5.0 | |
| Comorbidity | 0.768 | ||
| None | 5180 (95.5) | 16.6 ± 5.2 | |
| One or more | 243 (4.5) | 16.5 ± 5.2 | |
| Eating behavior *** | 0.205 | ||
| Eat less healthy | 377 (7.0) | 16.9 ± 5.4 | |
| Unchanged or healthier | 5046 (93.0) | 16.6 ± 5.2 | |
| Smoking *** | <0.001 | ||
| Never, stopped, or smoke less | 5255 (96.9) | 16.5 ± 5.1 | |
| Unchanged or smoke more | 168 (3.1) | 19.4 ± 7.6 | |
| Drinking alcohol *** | 0.001 | ||
| Never, stopped, or drink less | 5048 (93.0) | 16.5 ± 5.1 | |
| Unchanged or drink more | 375 (6.9) | 17.5 ± 6.7 | |
| Physical activity *** | 0.599 | ||
| Never, stopped, or exercise less | 1728 (31.8) | 16.6 ± 5.4 | |
| Unchanged or exercise more | 3695 (68.1) | 16.6 ± 5.1 | |
| Anxiety | <0.001 | ||
| GAD < 8 | 5007 (92.3) | 16.4 ± 5.1 | |
| GAD ≥ 8 | 416 (7.7) | 19.3 ± 6.3 | |
| FCoV-19, mean ± SD | 16.7 ± 5.3 | ||
| HL index, mean ± SD | 34.7 ± 7.0 |
| Items | FCoV-19 Scale |
|---|---|
| 1. I am most afraid of COVID-19. | 0.84 |
| 2. It makes me uncomfortable to think about COVID-19. | 0.83 |
| 3. My hands become clammy when I think about COVID-19. | 0.81 |
| 4. I am afraid of losing my life because of COVID-19. | 0.81 |
| 5. When watching news and stories about COVID-19 on social media, I become nervous or anxious. | 0.78 |
| 6. I cannot sleep because I’m worrying about getting COVID-19. | 0.76 |
| 7. My heart races or palpitates when I think about getting COVID-19. | 0.69 |
| Percentage of variance, % | 62.15 |
| Item–scale convergent validity, mean of Rho (range) | 0.77 (0.66–0.84) |
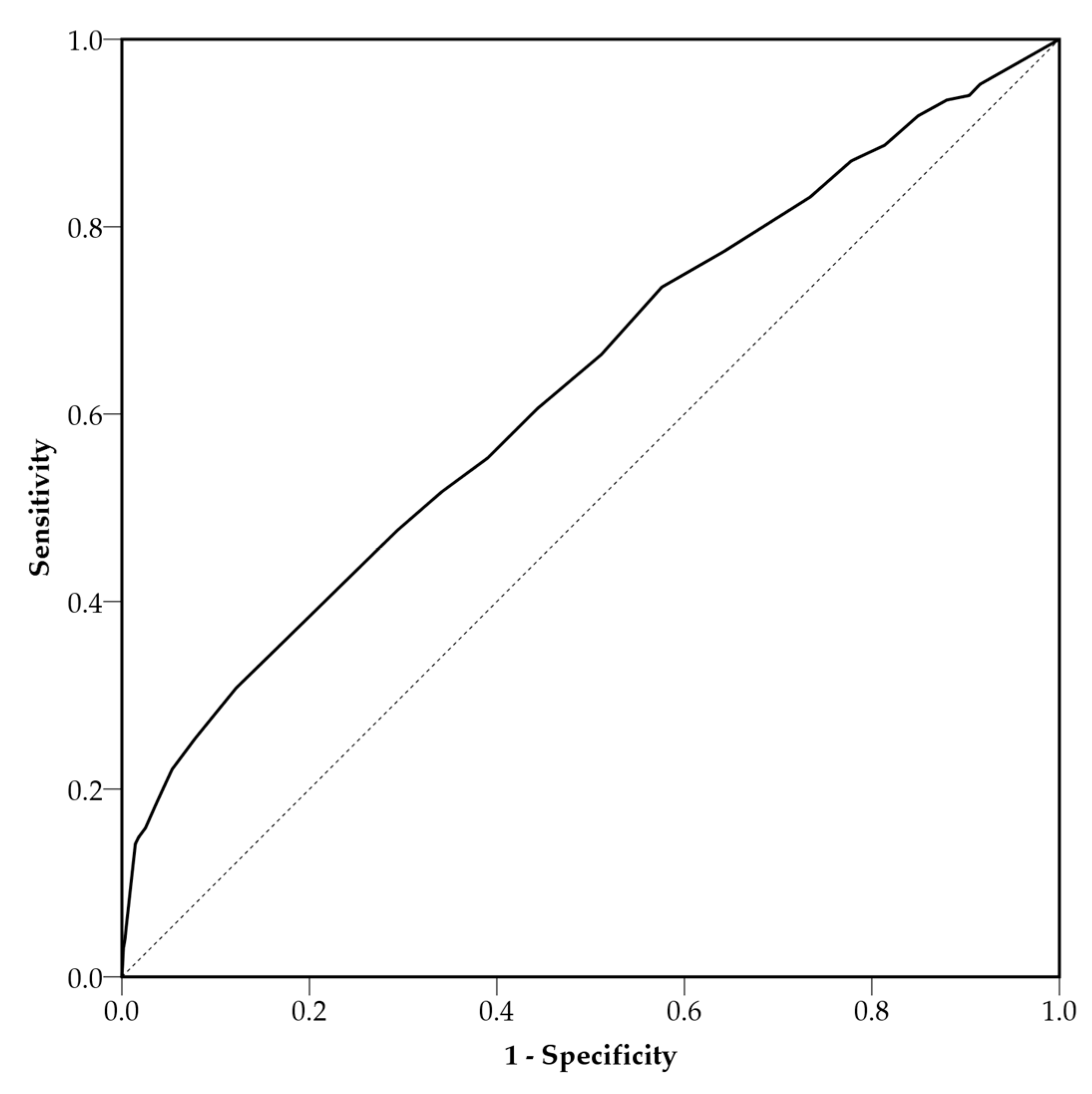
| AUC (95%CI), GAD ≥ 8 as the reference | 0.63 (0.60–0.66) |
| Internal consistency, Cronbach’s alpha | 0.90 |
| Floor effects, % | 8.20 |
| Ceiling effect, % | 0.40 |
| Variables | FCoV-19S | |||
|---|---|---|---|---|
| Simple Model | Multiple Model | |||
| B (95%CI) | p * | B (95%CI) | p * | |
| Age, year | ||||
| 19–22 | 0.00 | 0.00 | ||
| 23–26 | −1.02 (−1.31, −0.74) | <0.001 | −0.96 (−1.24, −0.67) | <0.001 |
| Gender | ||||
| Women | 0.00 | |||
| Men | −0.71 (−0.99, −0.43) | <0.001 | −0.68 (−0.97, −0.38) | <0.001 |
| Ability to pay for medication | ||||
| Very or fairly difficult | 0.00 | |||
| Very or fairly easy | −0.55 (−0.83, −0.26) | <0.001 | −0.45 (−0.73, −0.17) | 0.002 |
| BMI, kg/m2 | ||||
| Underweight (BMI < 18.5) | 0.54 (0.16, 0.91) | 0.005 | 0.29 (−0.09, 0.67) | 0.133 |
| Normal weight (18.5 ≤ BMI < 25.0) | 0.00 | |||
| Overweight/obese (BMI ≥ 25.0) | 0.21 (−0.31, 0.73) | 0.421 | 0.48 (−0.04, 1.00) | 0.069 |
| Academic year | ||||
| 1 | 0.00 | |||
| 2 | 0.31 (−0.17, 0.79) | 0.203 | ||
| 3 | 0.23 (−0.25, 0.71) | 0.349 | ||
| 4 | −0.02 (−0.50, 0.46) | 0.933 | ||
| 5 | −1.10 (−1.56, −0.65) | <0.001 | ||
| 6 | −1.18 (−1.62, −0.74) | <0.001 | ||
| S-COVID-19-S ** | ||||
| No | 0.00 | |||
| Yes | 0.24 (−0.12, 0.6) | 0.186 | 0.07 (−0.29, 0.43) | 0.708 |
| Comorbidity | ||||
| None | 0.00 | |||
| One or more | −0.1 (−0.78, 0.58) | 0.768 | ||
| HL index, 1-score increment | −0.07 (−0.09, −0.05) | <0.001 | −0.06 (−0.08, −0.04) | <0.001 |
| FCoV-19S * | Unchanged or Eat Healthier ** | Unchanged or Smoke More ** | Unchanged or Drinking More ** | Unchanged or Exercise More ** | ||||
|---|---|---|---|---|---|---|---|---|
| OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | |
| Model 1 | 0.99 (0.97, 1.01) | 0.205 | 1.11 (1.08, 1.14) | <0.001 | 1.03 (1.01, 1.06) | 0.001 | 1 (0.99, 1.01) | 0.599 |
| Model 2 | 0.99 (0.97, 1.01) | 0.211 | 1.11 (1.08, 1.14) | <0.001 | 1.04 (1.02, 1.06) | <0.001 | 1 (0.99, 1.01) | 0.608 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, H.T.; Do, B.N.; Pham, K.M.; Kim, G.B.; Dam, H.T.B.; Nguyen, T.T.; Nguyen, T.T.P.; Nguyen, Y.H.; Sørensen, K.; Pleasant, A.; et al. Fear of COVID-19 Scale—Associations of Its Scores with Health Literacy and Health-Related Behaviors among Medical Students. Int. J. Environ. Res. Public Health 2020, 17, 4164. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114164
Nguyen HT, Do BN, Pham KM, Kim GB, Dam HTB, Nguyen TT, Nguyen TTP, Nguyen YH, Sørensen K, Pleasant A, et al. Fear of COVID-19 Scale—Associations of Its Scores with Health Literacy and Health-Related Behaviors among Medical Students. International Journal of Environmental Research and Public Health. 2020; 17(11):4164. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114164
Chicago/Turabian StyleNguyen, Hiep T., Binh N. Do, Khue M. Pham, Giang B. Kim, Hoa T.B. Dam, Trung T. Nguyen, Thao T.P. Nguyen, Yen H. Nguyen, Kristine Sørensen, Andrew Pleasant, and et al. 2020. "Fear of COVID-19 Scale—Associations of Its Scores with Health Literacy and Health-Related Behaviors among Medical Students" International Journal of Environmental Research and Public Health 17, no. 11: 4164. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114164