Finding the Hidden Risk Profiles of the United States Opioid Epidemic: Using a Person-Centered Approach on a National Dataset of Noninstitutionalized Adults Reporting Opioid Misuse


Abstract
:1. Introduction
2. Materials and Methods
2.1. Other Substance Dependence or Abuse Covariates
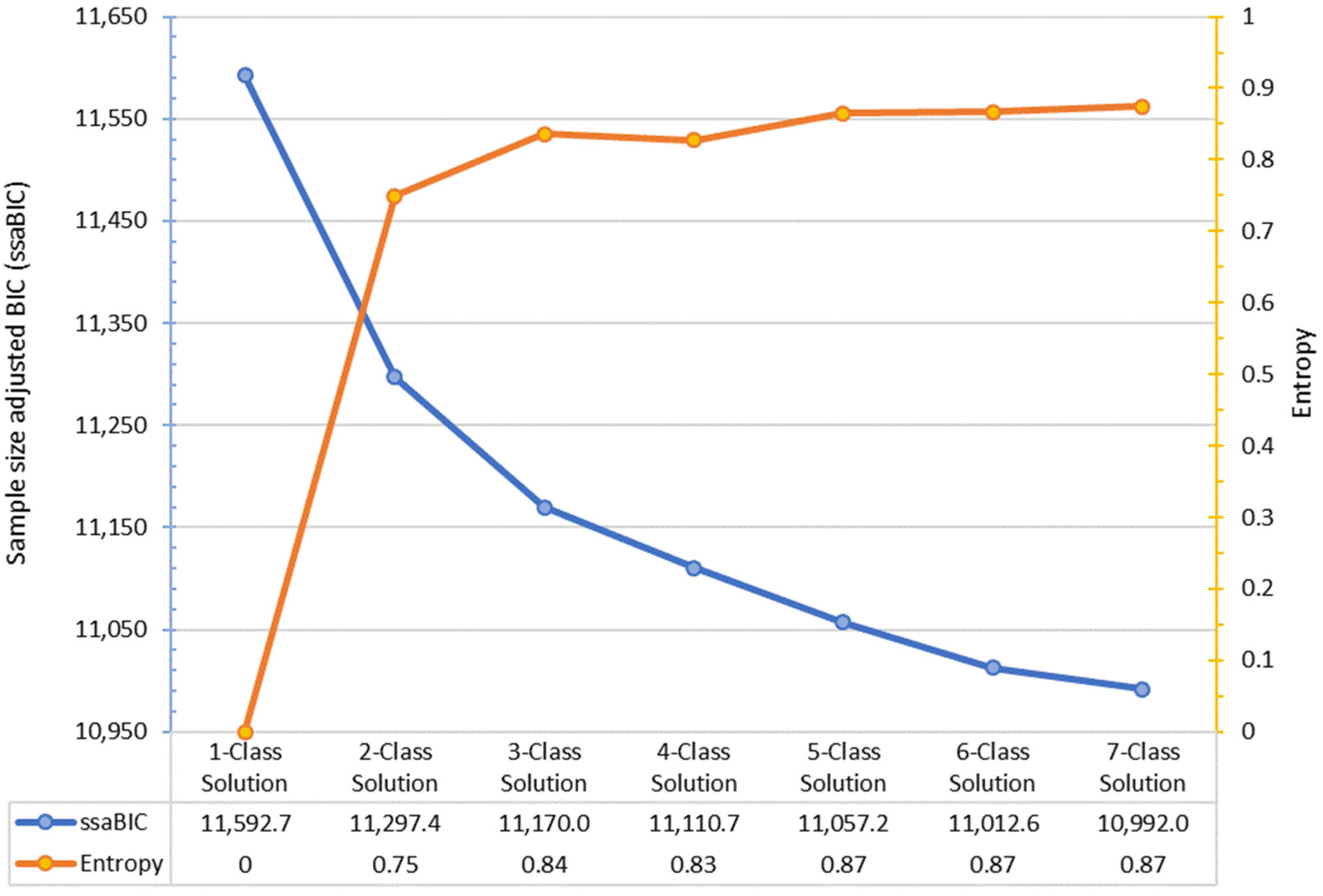
2.2. Latent Class Analysis Model Selection Criteria
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gomes, T.; Tadrous, M.; Mamdani, M.M.; Paterson, J.M.; Juurlink, D.N. The burden of opioid-related mortality in the United States. JAMA Netw. Open 2018, 1, e180217. [Google Scholar] [CrossRef] [PubMed]
- Scholl, L.; Seth, P.; Kariisa, M.; Wilson, N.; Baldwin, G. Drug and opioid-involved overdose deaths—United States, 2013–2017. MMWR Morb. Mortal. Wkly. Rep. 2019, 67, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Palamar, J.J. Barriers to accurately assessing prescription opioid misuse on surveys. Am. J. Drug Alcohol Abus. 2019, 45, 117–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seth, P.; Rudd, R.A.; Noonan, R.K.; Haegerich, T.M. Quantifying the epidemic of prescription opioid overdose deaths. Am. J. Public Health 2018, 108, 500–502. [Google Scholar] [CrossRef]
- Opioid Overdose Crisis. Available online: https://www.drugabuse.gov/drugs-abuse/opioids/opioid-overdose-crisis (accessed on 1 April 2019).
- Chen, Q.; Larochelle, M.R.; Weaver, D.T.; Lietz, A.P.; Mueller, P.P.; Mercaldo, S.; Wakeman, S.E.; Freedberg, K.A.; Raphel, T.J.; Knudsen, A.B.; et al. Prevention of prescription opioid misuse and projected overdose deaths in the United States. JAMA Netw. Open 2019, 2, e187621. [Google Scholar] [CrossRef] [Green Version]
- Van Zee, A. The Promotion and Marketing of OxyContin: Commercial Triumph, Public Health Tragedy. Am. J. Public Health 2009, 99, 221–227. [Google Scholar] [CrossRef]
- Griesler, P.C.; Hu, M.-C.; Wall, M.M.; Kandel, D.B. Medical Use and Misuse of Prescription Opioids in the US Adult Population: 2016–2017. Am. J. Public Health 2019, 109, 1258–1265. [Google Scholar] [CrossRef]
- Fraser, M.; Plescia, M. The opioid epidemic’s prevention problem. Am. J. Public Health 2019, 109, 215–217. [Google Scholar] [CrossRef]
- Pitt, A.L.; Humphreys, K.; Brandeau, M.L. Modeling health benefits and harms of public policy responses to the US opioid epidemic. Am. J. Public Health 2018, 108, 1394–1400. [Google Scholar] [CrossRef]
- Nicholson, H.L.; Vincent, J. Gender differences in prescription opioid misuse among US Black adults. Subst. Use Misuse 2019, 54, 639–650. [Google Scholar] [CrossRef]
- Tetrault, J.M.; Desai, R.A.; Becker, W.C.; Fiellin, D.A.; Concato, J.; Sullivan, L.E. Gender and non-medical use of prescription opioids: Results from a national US survey. Addiction 2008, 103, 258–268. [Google Scholar] [CrossRef] [PubMed]
- Winkelman, T.N.A.; Chang, V.W.; Binswanger, I.A. Health, polysubstance use, and criminal justice involvement among adults with varying levels of opioid use. JAMA Netw. Open 2018, 1, e180558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, W.C.; Sullivan, L.E.; Tetrault, J.M.; Desai, R.A.; Fiellin, D.A. Non-medical use, abuse and dependence on prescription opioids among U.S. adults: Psychiatric, medical and substance use correlates. Drug Alcohol Depend. 2008, 94, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Braden, J.B.; Edlund, M.J.; Sullivan, M.D. Suicide deaths with opioid poisoning in the United States: 1999–2014. Am. J. Public Health 2017, 107, 421–426. [Google Scholar] [CrossRef]
- Grigsby, T.J.; Howard, J.T. Prescription opioid misuse and comorbid substance use: Past 30-day prevalence, correlates and co-occurring behavioral indicators in the 2016 National Survey on Drug Use and Health. Am. J. Addict. 2019, 28, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Rajabi, A.; Dehghani, M.; Shojaei, A.; Farjam, M.; Motevalian, S.A. Association between tobacco smoking and opioid use: A meta-analysis. Addict. Behav. 2018, 92, 225–235. [Google Scholar] [CrossRef]
- Havens, J.R.; Stoops, W.W.; Leukefeld, C.G.; Garrity, T.F.; Carlson, R.G.; Falck, R.; Booth, B.M. Prescription opiate misuse among rural stimulant users in a multistate community-based study. Am. J. Drug Alcohol Abus. 2009, 35, 18–23. [Google Scholar] [CrossRef]
- Schuler, M.S.; Rice, C.E.; Evans-Polce, R.J.; Collins, R.L. Disparities in substance use behaviors and disorders among adult sexual minorities by age, gender, and sexual identity. Drug Alcohol Depend. 2018, 189, 139–146. [Google Scholar] [CrossRef]
- Perlman, D.C.; Jordan, A.E. The syndemic of opioid misuse, overdose, HCV, and HIV: Structural-level causes and interventions. Curr. HIV/AIDS Rep. 2018, 15, 96–112. [Google Scholar] [CrossRef]
- Center for Behavioral Health Statistics. 2017 National Survey of Drug Use and Health Final Analytic Codebook; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2018.
- Office of Management and Budget. OMB Bulletin No. 10-02: Update of Statistical Area Definitions and Guidance on their Uses; The White House: Washington, DC, USA, 2009.
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Struct. Equ. Model. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Hansen, H.; Netherland, J. Is the prescription opioid epidemic a white problem? Am. J. Public Health 2018, 106, 2127–2129. [Google Scholar] [CrossRef]
- Carlson, R.G.; Nahhas, R.W.; Martins, S.S.; Daniulaityte, R. Predictors of transition to heroin use among initially non-opioid dependent illicit pharmaceutical opioid users: A natural history study. Drug Alcohol Depend. 2016, 160, 127–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicero, T.J.; Ellis, M.S.; Surratt, H.L.; Kurtz, S.P. The changing face of heroin use in the United States: A retrospective analysis of the past 50 years. JAMA Psychiatry 2014, 71, 821–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, C.M. Heroin use and heroin use risk behaviors among nonmedical users of prescription opioid pain relievers—United States, 2002–2004 and 2008–2010. Drug Alcohol Depend. 2013, 132, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Muhuri, P.K.; Gfroerer, J.C.; Davies, M.C. Associations of Nonmedical Pain Reliever Use and Initiation of Heroin Use in the United States; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2013.
- Kapadia, S.N.; Bao, Y. Prescription painkiller misuse and the perceived risk of harm from using heroin. Addict. Behav. 2019, 93, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Gasior, M.; Bond, M.; Malamut, R. Routes of abuse of prescription opioid analgesics: A review and assessment of the potential impact of abuse-deterrent formulations. Postgrad. Med. 2016, 128, 85–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kestenbaum, M.G.; Vilches, A.O.; Messersmith, S.; Connor, S.R.; Fine, P.G.; Murphy, B.; Muir, J.C. Alternative routes to oral opioid administration in palliative care: A review and clinical summary. Pain Med. 2014, 15, 1129–1153. [Google Scholar] [CrossRef] [Green Version]
- Kirsh, K.; Peppin, J.; Coleman, J. Characterization of prescription opioid abuse in the United States: Focus on route of administration. J. Pain Palliat. Care Pharmacother. 2012, 26, 348–361. [Google Scholar] [CrossRef]
- Havens, J.R.; Walker, R.; Leukefeld, C.G. Prevalence of opioid analgesic injection among rural nonmedical opioid analgesic users. Drug Alcohol Depend. 2007, 87, 98–102. [Google Scholar] [CrossRef]
- Surratt, H.; Kurtz, S.P.; Cicero, T.J. Alternate routes of administration and risk for HIV among prescription opioid abusers. J. Addict. Dis. 2011, 30, 334–341. [Google Scholar] [CrossRef] [Green Version]
- Zibbell, J.E.; Asher, A.K.; Patel, R.C.; Kupronis, B.; Iqbal, K.; Ward, J.W.; Holtzman, D. Increases in acute hepatitis C virus infection related to a growing opioid epidemic and associated injection drug use, United States, 2004 to 2014. Am. J. Public Health 2018, 108, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Whiteford, H.A.; Ferrari, A.J.; Baxter, A.J.; Charlson, F.J.; Hall, W.D.; Freedman, G.; Burstein, R.; Johns, N.; Engell, R.E. Global burden of disease attributable to illicit drug use and dependence: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1564–1574. [Google Scholar] [CrossRef]
- John, W.S.; Zhu, H.; Mannelli, P.; Subramaniam, G.A.; Schwartz, R.P.; McNeely, J.; Wu, L.-T. Prevalence and patterns of opioid misuse and opioid use disorder among primary care patients who use tobacco. Drug Alcohol Depend. 2019, 194, 468–475. [Google Scholar] [CrossRef]
- Campbell, G.; Hall, W.; Nielsen, S. What does the ecological and epidemiological evidence indicate about the potential for cannabinoids to reduce opioid use and harms? A comprehensive review. Int. Rev. Psychiatry 2018, 30, 91–106. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Age Groups | ||
| 18–25 | 102 | 21.5 |
| 26–34 | 133 | 27.9 |
| 35–49 | 111 | 23.4 |
| 50 and older | 129 | 27.2 |
| Sex | ||
| Male | 288 | 60.6 |
| Female | 188 | 39.4 |
| Race/Ethnicity | ||
| Non-Hispanic white | 371 | 77.9 |
| Non-Hispanic black | 47 | 9.8 |
| Hispanic | 32 | 6.7 |
| Other | 27 | 5.6 |
| Sexual Identity | ||
| Heterosexual | 421 | 90.5 |
| Sexual minority | 44 | 9.5 |
| Family Income | ||
| Less than $20,000 | 131 | 27.5 |
| $20,000-$49,999 | 156 | 32.7 |
| $50,000 or more | 190 | 39.8 |
| Educational Attainment | ||
| Less than high school | 86 | 18.1 |
| High school graduate | 135 | 28.5 |
| Some college/associate’s degree | 187 | 39.2 |
| College graduate | 68 | 14.2 |
| Area of Residence | ||
| CBSA of 1 million or more | 225 | 47.2 |
| CBSA with less than 1 million | 231 | 48.4 |
| Not in a CBSA | 21 | 4.3 |
| Employment (past week) | ||
| Employed | 253 | 53.3 |
| Unemployed | 66 | 13.9 |
| Disabled | 65 | 13.8 |
| Other | 90 | 19.0 |
| Ever Arrested and Booked | ||
| No | 188 | 38.2 |
| Yes | 293 | 61.8 |
| Self-reported Health Status | ||
| Fair/poor | 134 | 28.3 |
| Good | 176 | 37.1 |
| Very good/excellent | 164 | 34.6 |
| Covered by Private Health Insurance | ||
| No | 305 | 64.4 |
| Yes | 169 | 35.6 |
| Serious Psychological Distress (past year) | ||
| No | 208 | 43.8 |
| Yes | 268 | 56.2 |
| Suicidality (past year) | ||
| No | 340 | 71.9 |
| Yes | 133 | 28.1 |
| Nicotine Dependence (past month) | ||
| No | 209 | 44.4 |
| Yes | 267 | 55.6 |
| Alcohol Dependence or Abuse (past year) | ||
| No/Unknown | 334 | 75.3 |
| Yes | 142 | 24.7 |
| Marijuana Dependence or Abuse (past year) | ||
| No/Unknown | 394 | 82.4 |
| Yes | 82 | 17.6 |
| Other Illicit Substance Dependence or Abuse (past year) | ||
| No/Unknown | 301 | 64.8 |
| Yes | 60 | 35.3 |
| Opioid Dependence or Abuse (past year) | ||
| Heroin only | 102 | 21.5 |
| Prescription pain reliever only | 314 | 66.0 |
| Heroin and prescription | 59 | 12.5 |
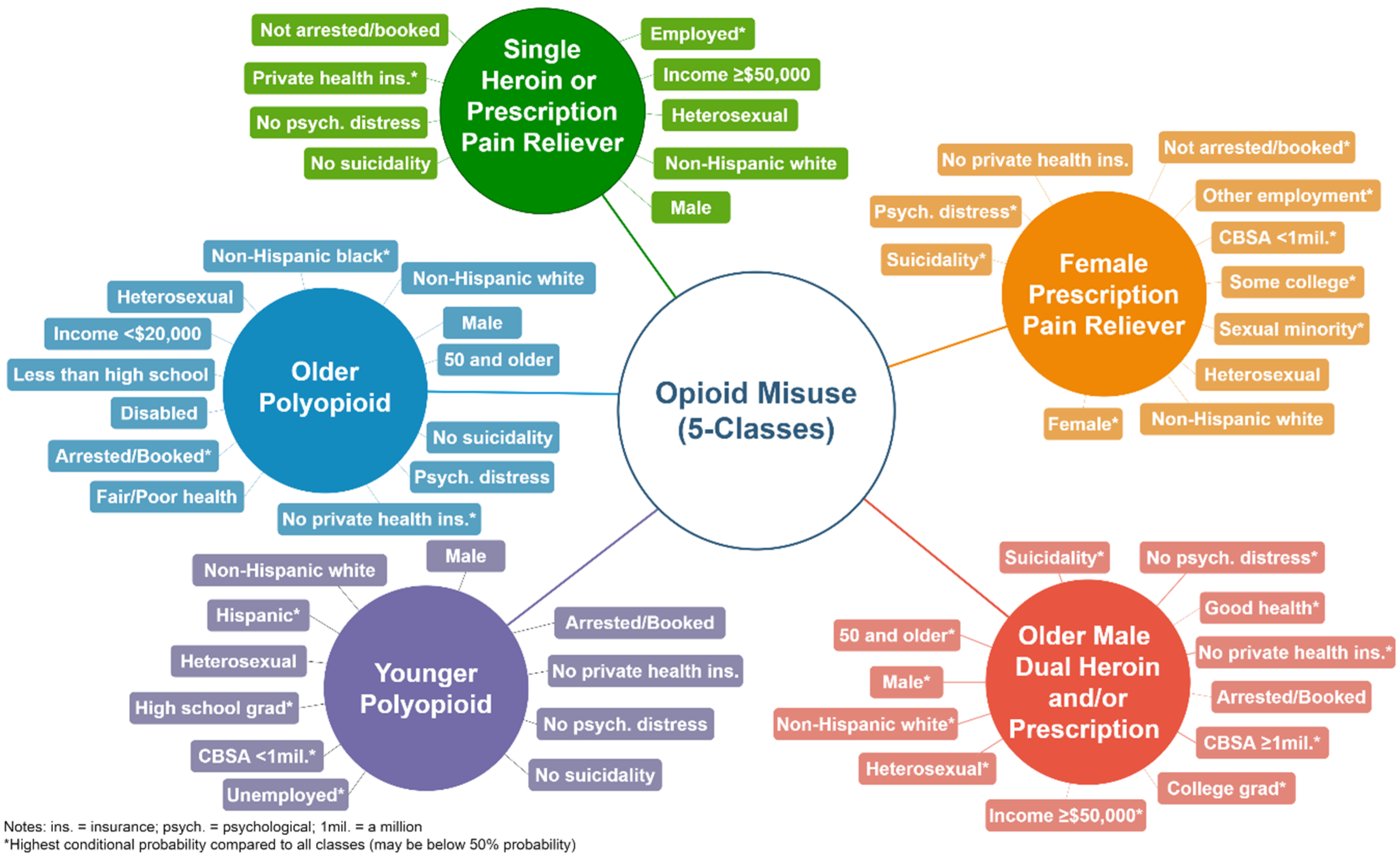
| Class 1 Single Heroin or Prescription Misuse | Class 2 Female Prescription Pain Reliever Misuse | Class 3 Younger Polyopioid Misuse | Class 4 Older Polyopioid Misuse | Class 5 Older Male Dual Heroin and/or Prescription Misuse | |
|---|---|---|---|---|---|
| 27% | 20% | 38% | 10% | 5% | |
| (n = 130) | (n = 97) | (n = 179) | (n = 48) | (n = 22) | |
| Age group | |||||
| 18–25 years old | 0.218 | 0.324 | 0.236 | 0.000 | 0.000 |
| 26–34 years old | 0.202 | 0.313 | 0.424 | 0.000 | 0.000 |
| 35–49 years old | 0.229 | 0.181 | 0.299 | 0.231 | 0.000 |
| 50 and older | 0.351 | 0.181 | 0.041 | 0.769 | 1.000 |
| Sex/Gender | |||||
| Male | 0.630 | 0.221 | 0.710 | 0.790 | 1.000 |
| Female | 0.370 | 0.779 | 0.290 | 0.210 | 0.000 |
| Race/Ethnicity | |||||
| Non-Hispanic white | 0.781 | 0.792 | 0.763 | 0.695 | 1.000 |
| Non-Hispanic black | 0.100 | 0.074 | 0.085 | 0.236 | 0.000 |
| Other race | 0.053 | 0.068 | 0.055 | 0.070 | 0.000 |
| Hispanic | 0.065 | 0.066 | 0.096 | 0.000 | 0.000 |
| Sexual Identity | |||||
| Heterosexual | 0.940 | 0.779 | 0.938 | 0.926 | 1.000 |
| Lesbian, gay, or bisexual | 0.060 | 0.221 | 0.062 | 0.074 | 0.000 |
| Family Income | |||||
| Less than $20,000 | 0.000 | 0.342 | 0.395 | 0.529 | 0.013 |
| $20,000–$49,999 | 0.282 | 0.404 | 0.325 | 0.344 | 0.214 |
| $50,000 or more | 0.718 | 0.254 | 0.280 | 0.127 | 0.773 |
| Educational Attainment | |||||
| Less than high school | 0.060 | 0.112 | 0.199 | 0.514 | 0.325 |
| High school grad | 0.169 | 0.214 | 0.456 | 0.237 | 0.000 |
| Some college/associate’s | 0.472 | 0.500 | 0.345 | 0.250 | 0.129 |
| College graduate | 0.299 | 0.174 | 0.000 | 0.000 | 0.547 |
| Area of Residence | |||||
| CBSA with ≥1 million | 0.495 | 0.435 | 0.408 | 0.484 | 1.000 |
| CBSA with <1 million | 0.468 | 0.528 | 0.538 | 0.462 | 0.000 |
| Not in a CBSA | 0.038 | 0.036 | 0.054 | 0.055 | 0.000 |
| Employment (past week) | |||||
| Employed full/part time | 0.927 | 0.449 | 0.421 | 0.203 | 0.347 |
| Unemployed | 0.003 | 0.163 | 0.274 | 0.000 | 0.000 |
| Disabled | 0.016 | 0.087 | 0.037 | 0.797 | 0.440 |
| Other | 0.054 | 0.301 | 0.268 | 0.000 | 0.214 |
| Arrested and booked in lifetime | |||||
| No | 0.572 | 0.672 | 0.168 | 0.082 | 0.342 |
| Yes | 0.428 | 0.328 | 0.832 | 0.918 | 0.658 |
| Self-reported health status | |||||
| Fair/Poor | 0.081 | 0.414 | 0.190 | 1.000 | 0.000 |
| Good | 0.448 | 0.213 | 0.430 | 0.000 | 1.000 |
| Very good/Excellent | 0.472 | 0.373 | 0.380 | 0.000 | 0.000 |
| Private health insurance | |||||
| No | 0.000 | 0.660 | 0.952 | 1.000 | 1.000 |
| Yes | 1.000 | 0.340 | 0.048 | 0.000 | 0.000 |
| Serious psychological distress | |||||
| No | 0.604 | 0.104 | 0.526 | 0.281 | 0.667 |
| Yes | 0.396 | 0.896 | 0.474 | 0.719 | 0.333 |
| Suicidality | |||||
| No | 0.780 | 0.468 | 0.839 | 0.779 | 0.440 |
| Yes | 0.220 | 0.532 | 0.161 | 0.221 | 0.560 |
| Opioid dependence or abuse | |||||
| Heroin only | 0.149 | 0.040 | 0.371 | 0.286 | 0.000 |
| Pain reliever only | 0.785 | 0.835 | 0.483 | 0.558 | 0.786 |
| Heroin and pain reliever | 0.066 | 0.125 | 0.146 | 0.156 | 0.214 |
| Odds Ratios (95% Confidence Intervals) | ||||
|---|---|---|---|---|
| Class 1 Single heroin or prescription misuse | Class 3 Younger polyopioid misuse | Class 4 Older polyopioid misuse | Class 5 Older male dual heroin and/or prescription misuse | |
| Nicotine Dependence | 0.56 (0.24, 1.30) | 4.49 (1.94, 10.4) * | 3.74 (1.00, 14.0) * | 2.17 (0.30, 15.9) |
| Alcohol Dependence/Abuse | 0.56 (0.24, 1.30) | 0.41 (0.15, 1.13) | 0.39 (0.13, 1.13) | 0.37 (0.03, 4.02) |
| Marijuana Dependence/Abuse | 0.63 (0.19, 0.83) | 0.22 (0.08, 0.60) * | 1.39 (0.45, 4.34) | 2.49 (0.24, 25.7) |
| Other Substance Dependence/Abuse | 0.53 (0.18, 1.53) | 1.51 (0.63, 3.65) | 1.50 (0.53, 4.25) | 0.95 (0.16, 5.55) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montiel Ishino, F.A.; Gilreath, T.; Williams, F. Finding the Hidden Risk Profiles of the United States Opioid Epidemic: Using a Person-Centered Approach on a National Dataset of Noninstitutionalized Adults Reporting Opioid Misuse. Int. J. Environ. Res. Public Health 2020, 17, 4321. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124321
Montiel Ishino FA, Gilreath T, Williams F. Finding the Hidden Risk Profiles of the United States Opioid Epidemic: Using a Person-Centered Approach on a National Dataset of Noninstitutionalized Adults Reporting Opioid Misuse. International Journal of Environmental Research and Public Health. 2020; 17(12):4321. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124321
Chicago/Turabian StyleMontiel Ishino, Francisco A., Tamika Gilreath, and Faustine Williams. 2020. "Finding the Hidden Risk Profiles of the United States Opioid Epidemic: Using a Person-Centered Approach on a National Dataset of Noninstitutionalized Adults Reporting Opioid Misuse" International Journal of Environmental Research and Public Health 17, no. 12: 4321. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124321