Real-World Setting Cost-Effectiveness Analysis Comparing Three Therapeutic Schemes of One-Year Adjuvant Trastuzumab in HER2-Positive Early Breast Cancer from the Cyprus NHS Payer Perspective


Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodology, Subjects and Treatments
2.2. Cost Calculations
2.3. Data Collection
2.4. Statistical Analysis for Cost-Effectiveness Analysis
2.5. Ethics Approval
3. Results
3.1. The Costs of Examinations and Treatment
3.2. The Results of the Cost-Effectiveness Analysis over 20 Years and for a Lifetime Horizon
3.3. Sensitivity Analysis Based on All Trastuzumab Arms
3.4. Sensitivity Analysis Based on the three Subgroups of Trastuzumab Arms
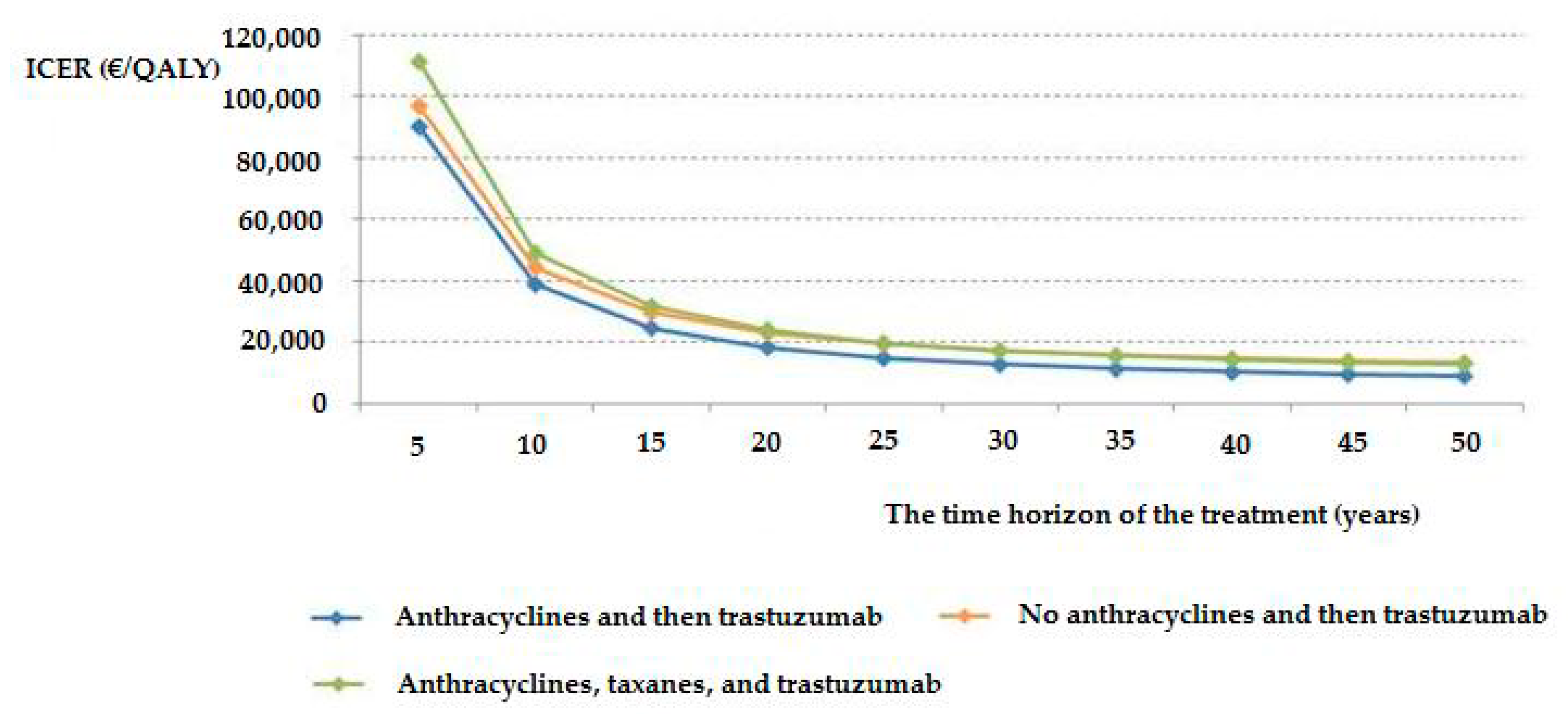
3.5. Impact of the Time Horizon on the ICER of Treatment
3.6. Multivariate Analysis with the Dependent Variable of the Cost/QALY Ratio
3.7. Correlation of the Cost/QALY Ratio with the Weight and Age of Patients at Diagnosis
3.8. Correlation of the Cost/QALY Ratio with the Stage and Grade of Patients
3.9. Correlation of the Cost/QALY Ratio with Age at Treatment Initiation
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variable | 20-Year Horizon | Lifetime Horizon | ||
|---|---|---|---|---|
| ICER (€/QALY) | ICER (€/QALY) | |||
| −10% | +10% | −10% | +10% | |
| Cost | ||||
| Total cost without trastuzumab | 40,824.22 | 40,047.94 | 17,924.26 | 17,583.42 |
| Total cost with trastuzumab | 36,004.33 | 44,867.87 | 15,808.04 | 19,699.66 |
| Discount rate | 38,890.04 | 42,030.80 | 16,489.50 | 19,085.66 |
| Utility weights | ||||
| EQ-5D For stable condition | 45,037.52 | 36,687.76 | 19,720.14 | 16,144.12 |
| EQ-5D For recurrence | 40,375.13 | 40,497.25 | 17,756.21 | 17,751.48 |
| EQ-5D For metastasis | 40,409.33 | 40,462.91 | 17,756.64 | 17,751.06 |
| Variable | 20 Years Horizon | |||||
|---|---|---|---|---|---|---|
| ICER 1 (€/QALY) | ICER 2 (€/QALY) | ICER 3 (€/QALY) | ||||
| −10% | +10% | −10% | +10% | −10% | +10% | |
| Cost | ||||||
| Total cost without trastuzumab | 18,496.57 | 18,106.51 | 23,370.82 | 22,906.95 | 24,477.41 | 24,032.02 |
| Total cost with anthracyclines and then trastuzumab | 16,276.37 | 20,326.74 | 23,138.90 | 23,138.90 | 24,254.73 | 24,254.73 |
| Total cost with no anthracyclines and trastuzumab | 18,301.55 | 18,301.55 | 20,593.10 | 25,684.74 | 24,254.73 | 24,254.73 |
| Total cost with anthracyclines, taxanes and trastuzumab | 18,301.55 | 18,301.55 | 23,138.90 | 23,138.90 | 21,606.53 | 26,902.90 |
| Discount rate | 17,710.87 | 18,905.05 | 22,414.49 | 23,877.66 | 23,495.30 | 25,029.62 |
| Utility weights | ||||||
| EQ-5DFor stable condition | 20,233.15 | 16,706.62 | 25,358.89 | 21,276.31 | 26,967.57 | 22,037.80 |
| EQ-5D For recurrence | 18,364.14 | 18,239.38 | 23,169.53 | 23,108.35 | 24,222.68 | 24,286.85 |
| EQ-5D For metastasis | 18,322.34 | 18,280.81 | 23,398.81 | 22,884.69 | 24,272.18 | 24,237.29 |
| Lifetime Horizon | |||||||
|---|---|---|---|---|---|---|---|
| Variable | ICER 1 (€/QALY) | ICER 2 (€/QALY) | ICER 3 (€/QALY) | ||||
| −10% | +10% | −10% | +10% | −10% | +10% | ||
| Cost | |||||||
| Total cost without trastuzumab | 9050.39 | 8859.54 | 13,580.40 | 13,310.85 | 13,231.82 | 12,991.05 | |
| Total cost with anthracyclines and then trastuzumab | 7964.05 | 9945.90 | 13,445.63 | 13,445.63 | 13,111.44 | 13,111.44 | |
| Total cost with no anthracyclines and trastuzumab | 8954.97 | 8954.97 | 11,966.31 | 14,924.98 | 13,111.44 | 13,111.44 | |
| Total cost with anthracyclines, taxanes, and trastuzumab | 8954.97 | 8954.97 | 13,445.63 | 13,445.63 | 11,679.90 | 14,542.97 | |
| Discount rate | 8370.58 | 9563.48 | 12,649.46 | 14,267.28 | 12,316.13 | 13,934.89 | |
| Utility weights | |||||||
| EQ-5D For stable condition | 9898.65 | 8175.55 | 14,646.77 | 12,426.57 | 14,561.12 | 11,924.28 | |
| EQ-5D For recurrence | 8986.22 | 8923.93 | 13,466.29 | 13,425.04 | 13,105.70 | 13,117.19 | |
| EQ-5D For metastasis | 8965.70 | 8944.26 | 13,670.06 | 13,228.46 | 13,122.93 | 13,099.97 | |
Appendix B
| All Trastuzumab Arms | ||||
|---|---|---|---|---|
| β + | SE ++ | p | ||
| BSA (m2) | 64,936.5 | 13,108.6 | <0.001 | |
| The degree of positive expression of progesterone receptors | −5025.1 | 1575.1 | 0.002 | |
| Radiotherapy | No (ref.) | |||
| Yes | 14,604.0 | 5196.9 | 0.006 | |
| The number of infiltrated lymph nodes (ΤΝΜ) | 5095.7 | 2247.3 | 0.025 | |
| Patients who received anthracyclines and then trastuzumab | ||||
| The age at diagnosis | −1016.21 | 353.74 | 0.006 | |
| BMI | 1490.76 | 575.28 | 0.012 | |
| Patients who received no anthracyclines and then trastuzumab | ||||
| Radiotherapy | No (ref.) | |||
| Yes | 35,142.76 | 12,002.59 | 0.006 | |
| Patients who received anthracyclines, taxanes, and trastuzumab | ||||
| BSA (m2) | 63,184.62 | 17,131.82 | <0.001 | |
| The degree of positive expression of progesterone receptors | −5811.02 | 2099.99 | 0.007 | |
| Radiotherapy | No (ref.) | |||
| Yes | 20,007.28 | 7839.48 | 0.012 | |
| The number of filtered lymph nodes (ΤΝΜ) | 8363.22 | 2877.73 | 0.004 | |
References
- Cooter, M.; Soliman, A.S.; Pavlou, P.; Demetriou, A.; Orphanides, C.; Kritioti, E.; Banerjee, M.; Farazi, P. Incidence and time trends of cancer in Cyprus over 11 years (1998–2008). Tumori J. 2015, 101, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Eurostat, A. Cancer Statistics—Specific Cancers. In Statistics Explained, 1st ed.; Hinton, P.R., Ed.; Routledge: Abingdon, UK, 2018; pp. 1–17. [Google Scholar]
- Choritz, H.; Büsche, G.; Kreipe, H.; Study Group HER2 Monitor. Quality assessment of HER2 testing by monitoring of positivity rates. Virchows Arch. 2011, 459, 283–289. [Google Scholar] [CrossRef] [Green Version]
- Slamon, D.; Clark, G.; Wong, S.; Levin, W.; Ullrich, A.; McGuire, W. Human breast cancer: Correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987, 235, 177–182. [Google Scholar] [CrossRef] [Green Version]
- Gianni, L.; Dafni, U.; Gelber, R.D.; De Azambuja, E.; Muehlbauer, S.; Goldhirsch, A.; Untch, M.; Smith, I.; Baselga, J.; Jackisch, C.; et al. Treatment with trastuzumab for 1 year after adjuvant chemotherapy in patients with HER2-positive early breast cancer: A 4-year follow-up of a randomised controlled trial. Lancet Oncol. 2011, 12, 236–244. [Google Scholar] [CrossRef]
- Piccart-Gebhart, M.J.; Procter, M.; Leyland-Jones, B.; Goldhirsch, A.; Untch, M.; Smith, I.; Gianni, L.; Baselga, J.; Bell, R.; Jackisch, C.; et al. Trastuzumab after Adjuvant Chemotherapy in HER2-Positive Breast Cancer. N. Engl. J. Med. 2005, 353, 1659–1672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romond, E.H.; Perez, E.A.; Bryant, J.; Suman, V.J.; Geyer, C.E.; Davidson, N.E.; Tan-Chiu, E.; Martino, S.; Paik, S.; Kaufman, P.A.; et al. Trastuzumab plus Adjuvant Chemotherapy for Operable HER2-Positive Breast Cancer. N. Engl. J. Med. 2005, 353, 1673–1684. [Google Scholar] [CrossRef] [Green Version]
- Slamon, D.J.; Eiermann, W.; Robert, N.; Pienkowski, T.; Martín, M.; Press, M.; Mackey, J.; Glaspy, J.; Chan, A.; Pawlicki, M.; et al. Adjuvant trastuzumab in HER2-positive breast cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar] [CrossRef] [Green Version]
- Aboutorabi, A.; Hadian, M.; Ghaderi, H.; Salehi, M.; Ghiasipour, M. Cost-Effectiveness Analysis of Trastuzumab in the Adjuvant Treatment for Early Breast Cancer. Glob. J. Health Sci. 2014, 7, 98–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buendia, J.; Vallejos, C.; Pichón-Rivière, A. Evaluación económica del trastuzumab como tratamiento adyuvante en cáncer de mama HER2-positivo en Colombia. Biomédica 2013, 33, 411–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.; Jiang, Z.; Shao, Z.; Sun, Q.; Shen, K. An Economic Evaluation of Adjuvant Trastuzumab Therapy in HER2-Positive Early Breast Cancer. Value Health 2009, 12, S82–S84. [Google Scholar] [CrossRef] [Green Version]
- Dedes, K.; Szucs, T.; Imesch, P.; Fedier, A.; Fehr, M.; Fink, D. Cost-effectiveness of trastuzumab in the adjuvant treatment of early breast cancer: A model-based analysis of the HERA and FinHer trial. Ann. Oncol. 2007, 18, 1493–1499. [Google Scholar] [CrossRef]
- Doan, T.N.; Barendregt, J. Adjuvant trastuzumab chemotherapy in early breast cancer: Meta-analysis of randomised trials and cost-effectiveness analysis. Swiss Med. Wkly. 2019, 149, w20082. [Google Scholar] [CrossRef]
- Garrison, L.P.; Lubeck, D.; Lalla, D.; Paton, V.; Dueck, A.; Perez, E.A. Cost-effectiveness analysis of trastuzumab in the adjuvant setting for treatment of HER2-positive breast cancer. Cancer 2007, 110, 489–498. [Google Scholar] [CrossRef]
- Genuino, A.J.; Chaikledkaew, U.; Guerrero, A.M.; Reungwetwattana, T.; Thakkinstian, A. Cost-utility analysis of adjuvant trastuzumab therapy for HER2-positive early-stage breast cancer in the Philippines. BMC Health Serv. Res. 2019, 19, 874. [Google Scholar] [CrossRef] [Green Version]
- Gershon, N.; Berchenko, Y.; Hall, P.S.; Goldstein, D.A. Cost effectiveness and affordability of trastuzumab in sub-Saharan Africa for early stage HER2-positive breast cancer. Cost Eff. Resour. Alloc. 2019, 17, 5. [Google Scholar] [CrossRef]
- Hajjar, A.; Ergun, M.A.; Alagoz, O.; Rampurwala, M. Cost-effectiveness of adjuvant paclitaxel and trastuzumab for early-stage node-negative, HER2-positive breast cancer. PLoS ONE 2019, 14, e0217778. [Google Scholar] [CrossRef] [PubMed]
- Hall, P.S.; Hulme, C.; McCabe, C.; Oluboyede, Y.; Round, J.; Cameron, D.A. Updated cost-effectiveness analysis of trastuzumab for early breast cancer: A UK perspective considering duration of benefit, long-term toxicity and pattern of recurrence. PharmacoEconomics 2011, 29, 415–432. [Google Scholar] [CrossRef]
- Hedden, L.; O’Reilly, S.; Lohrisch, C.; Chia, S.; Speers, C.; Kovacic, L.; Taylor, S.; Peacock, S. Assessing the Real-World Cost-Effectiveness of Adjuvant Trastuzumab in HER-2/neu Positive Breast Cancer. Oncologist 2012, 17, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Kurian, A.W.; Thompson, R.N.; Gaw, A.F.; Arai, S.; Ortiz, R.; Garber, A.M. A Cost-Effectiveness Analysis of Adjuvant Trastuzumab Regimens in Early HER2/neu–Positive Breast Cancer. J. Clin. Oncol. 2007, 25, 634–641. [Google Scholar] [CrossRef] [Green Version]
- Lang, H.-C.; Chen, H.-W.; Chiou, T.-J.; Chan, A.L.F. The real-world cost-effectiveness of adjuvant trastuzumab in HER-2/neu-positive early breast cancer in Taiwan. J. Med. Econ. 2016, 19, 1–12. [Google Scholar] [CrossRef]
- Leung, W.; Kvizhinadze, G.; Nair, N.; Blakely, T. Adjuvant Trastuzumab in HER2-Positive Early Breast Cancer by Age and Hormone Receptor Status: A Cost-Utility Analysis. PLoS Med. 2016, 13, e1002067. [Google Scholar] [CrossRef] [Green Version]
- Liberato, N.L.; Marchetti, M.; Barosi, G. Cost Effectiveness of Adjuvant Trastuzumab in Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer. J. Clin. Oncol. 2007, 25, 625–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millar, J.A.; Millward, M.J.; Millar, J.A. Cost Effectiveness of Trastuzumab in the Adjuvant Treatment of Early Breast Cancer. PharmacoEconomics 2007, 25, 429–442. [Google Scholar] [CrossRef]
- Norum, J.; Olsen, J.A.; Wist, E.A.; Lønning, P.E. Trastuzumab in adjuvant breast cancer therapy. A model based cost-effectiveness analysis. Acta Oncol. 2007, 46, 153–164. [Google Scholar] [CrossRef]
- Seferina, S.C.; Ramaekers, B.L.T.; De Boer, M.; Dercksen, M.W.; Berkmortel, F.V.D.; Van Kampen, R.J.; Van De Wouw, A.J.; Voogd, A.C.; Heijnen, V.C.T.; Joore, M. Cost and cost-effectiveness of adjuvant trastuzumab in the real world setting: A study of the Southeast Netherlands Breast Cancer Consortium. Oncotarget 2017, 8, 79223–79233. [Google Scholar] [CrossRef] [Green Version]
- Shiroiwa, T.; Fukuda, T.; Shimozuma, K.; Ohashi, Y.; Tsutani, K. The model-based cost-effectiveness analysis of 1-year adjuvant trastuzumab treatment: Based on 2-year follow-up HERA trial data. Breast Cancer Res. Treat. 2007, 109, 559–566. [Google Scholar] [CrossRef]
- Skedgel, C.; Rayson, D.; Younis, T. The Cost-Utility of Sequential Adjuvant Trastuzumab in Women with Her2/Neu-Positive Breast Cancer: An Analysis Based on Updated Results from the HERA Trial. Value Health 2009, 12, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.L.F.; Leung, H.W.C.; Lu, C.-L.; Lin, S.J. Cost-Effectiveness of Trastuzumab as Adjuvant Therapy for Early Breast Cancer: A Systematic Review. Ann. Pharmacother. 2009, 43, 296–303. [Google Scholar] [CrossRef]
- Reed, S.; Schulman, K.A. Cost Utility of Sequential Adjuvant Trastuzumab for HER2/Neu-Positive Breast Cancer. Value Health 2009, 12, 637–640. [Google Scholar] [CrossRef] [Green Version]
- Fung, V.; Brand, R.J.; Newhouse, J.P.; Hsu, J. Using medicare data for comparative effectiveness research: Opportunities and challenges. Am. J. Manag. Care 2011, 17, 488–496. [Google Scholar]
- Garrison, L.P.; Neumann, P.J.; Erickson, P.; Marshall, D.A.; Mullins, C.D. Using Real-World Data for Coverage and Payment Decisions: The ISPOR Real-World Data Task Force Report. Value Health 2007, 10, 326–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romio, S.; Sturkenboom, M.; Corrao, G. Real-World Data from the Health Decision Maker Perspective What Are We Talking About? Epidemiol. Biostat. Public Health 2013, 10, 1–9. [Google Scholar] [CrossRef]
- Aggarwal, A.; Fojo, T.; Chamberlain, C.; Davis, C.; Sullivan, R. Do patient access schemes for high-cost cancer drugs deliver value to society?—Lessons from the NHS Cancer Drugs Fund. Ann. Oncol. 2017, 28, 1738–1750. [Google Scholar] [CrossRef]
- Drummond, M.F.; Sculpher, M.J.; Torrance, G.W.; O’Brien, B.J.; Stoddart, G.L. Methods for the Economic Evaluation of Health Care Programme, 3rd ed.; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Makady, A.; Ham, R.T.; De Boer, A.; Hillege, H.; Klungel, O.; Goettsch, W. Policies for Use of Real-World Data in Health Technology Assessment (HTA): A Comparative Study of Six HTA Agencies. Value Health 2017, 20, 520–532. [Google Scholar] [CrossRef] [Green Version]
- Campbell, J.D.; McQueen, R.B.; Briggs, A.H. The “E” in Cost-Effectiveness Analyses. A Case Study of Omalizumab Efficacy and Effectiveness for Cost-Effectiveness Analysis Evidence. Ann. Am. Thorac. Soc. 2014, 11. [Google Scholar] [CrossRef]
- Kontopantelis, E.; Doran, T.; A Springate, D.; Buchan, I.; Reeves, D. Regression based quasi-experimental approach when randomisation is not an option: Interrupted time series analysis. BMJ 2015, 350, h2750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonnenberg, F.A.; Beck, J.R. Markov Models in Medical Decision Making. Med. Decis. Mak. 1993, 13, 322–338. [Google Scholar] [CrossRef] [PubMed]
- Lidgren, M.; Wilking, N.; Jonsson, B.; Rehnberg, C. Health related quality of life in different states of breast cancer. Qual. Life Res. 2007, 16, 1073–1081. [Google Scholar] [CrossRef]
- Peasgood, T.; Ward, S.; Brazier, J. Health-state utility values in breast cancer. Expert Rev. Pharm. Outcomes Res. 2010, 10, 553–566. [Google Scholar] [CrossRef]
- Barbieri, M.; Hawkins, N.; Sculpher, M. Who Does the Numbers? The Role of Third-Party Technology Assessment to Inform Health Systems’ Decision-Making about the Funding of Health Technologies. Value Health 2009, 12, 193–201. [Google Scholar] [CrossRef] [Green Version]
- Pharmaceutical Services. Uniform Pricelist Valid Since 2/10/2017; Ministry of Health: Nicosia, Turkey, 2017.
- IBM Corp. IBM SPSS Statistics for Windows, Version 22.0.; IBM Corp: Armonk, NY, USA, 2013. [Google Scholar]
- TreeAge, Software. TreeAge Pro 2017 Program; TreeAge, Software: Williamstown, MA, USA, 2017. [Google Scholar]
- Kontodimopoulos, N.; Pappa, E.; Niakas, D.; Dimitrakaki, C.; Tountas, Y. Validity of the EuroQoL (EQ-5D) Instrument in a Greek General Population. Value Health 2008, 11, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.H.; Sculpher, M.J.; Claxton, K. Decision Modelling for Health Economic Evaluation, 1st ed.; Oxford Handbooks in Health Economic Evaluation; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Bertram, M.Y.; A Lauer, J.; De Joncheere, K.; Edejer, T.; Hutubessy, R.; Kieny, M.-P.; Hill, S.R. Cost–effectiveness thresholds: Pros and cons. Bull. World Heal. Organ. 2016, 94, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Eichler, H.-G.; Kong, S.X.; Gerth, W.C.; Mavros, P.; Jonsson, B. Use of Cost-Effectiveness Analysis in Health-Care Resource Allocation Decision-Making: How Are Cost-Effectiveness Thresholds Expected to Emerge? Value Heal. 2004, 7, 518–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Macroeconomics and Health: Investing in Health for Economic Development; Report of the Commission on Macroeconomics and Health; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- World Health Organization. The World Health Report 2002. Reducing Risks, Promoting Healthy Life; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Eurostat. Real GDP per Capita (Code: Sdg_08_10); Eurostat: Brussels, Belgium, 2018. [Google Scholar]
- Lopes, G.D.L. Societal Costs and Benefits of Treatment with Trastuzumab in Patients with Early HER2neu-Overexpressing Breast Cancer in Singapore. BMC Cancer 2011, 11, 178. [Google Scholar] [CrossRef] [Green Version]
- Rafar, N.R.A.; Hong, Y.H.; Wu, D.B.-C.; Othman, M.F.; Neoh, C.F. Cost-Effectiveness of Adjuvant Trastuzumab Therapy for Early Breast Cancer in Asia: A Systematic Review. Value Health Reg. Issues 2019, 18, 151–158. [Google Scholar] [CrossRef]
- Kongsakon, R.; Lochid-Amnuay, S.; Kapol, N.; Pattanaprateep, O. From Research to Policy Implementation: Trastuzumab in Early-Stage Breast Cancer Treatment in Thailand. Value Health Reg. Issues 2019, 18, 47–53. [Google Scholar] [CrossRef]
- The European Central Bank. Euro Foreign Exchange Reference Rates; The European Central Bank: Frankfurt, Germany, 2006. [Google Scholar]
- Luengo-Fernandez, R.; Leal, J.; Gray, A.; Sullivan, R. Economic burden of cancer across the European Union: A population-based cost analysis. Lancet Oncol. 2013, 14, 1165–1174. [Google Scholar] [CrossRef]
- Van Harten, W.; Wind, A.; De Paoli, P.; Saghatchian, M.; Oberst, S. Actual costs of cancer drugs in 15 European countries. Lancet Oncol. 2016, 17, 18–20. [Google Scholar] [CrossRef]
- Vogler, S.; Vitry, A.; Babar, Z.-U.-D. Cancer drugs in 16 European countries, Australia, and New Zealand: A cross-country price comparison study. Lancet Oncol. 2016, 17, 39–47. [Google Scholar] [CrossRef]
- Garrison, L.P.; Towse, A.; Briggs, A.H.; De Pouvourville, G.; Grueger, J.; Mohr, P.E.; Severens, J. (Hans); Siviero, P.; Sleeper, M. Performance-Based Risk-Sharing Arrangements—Good Practices for Design, Implementation, and Evaluation: Report of the ISPOR Good Practices for Performance-Based Risk-Sharing Arrangements Task Force. Value Health 2013, 16, 703–719. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Nardini, H.K.G.; Ruger, J.P. Micro-costing studies in the health and medical literature: Protocol for a systematic review. Syst. Rev. 2014, 3, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]


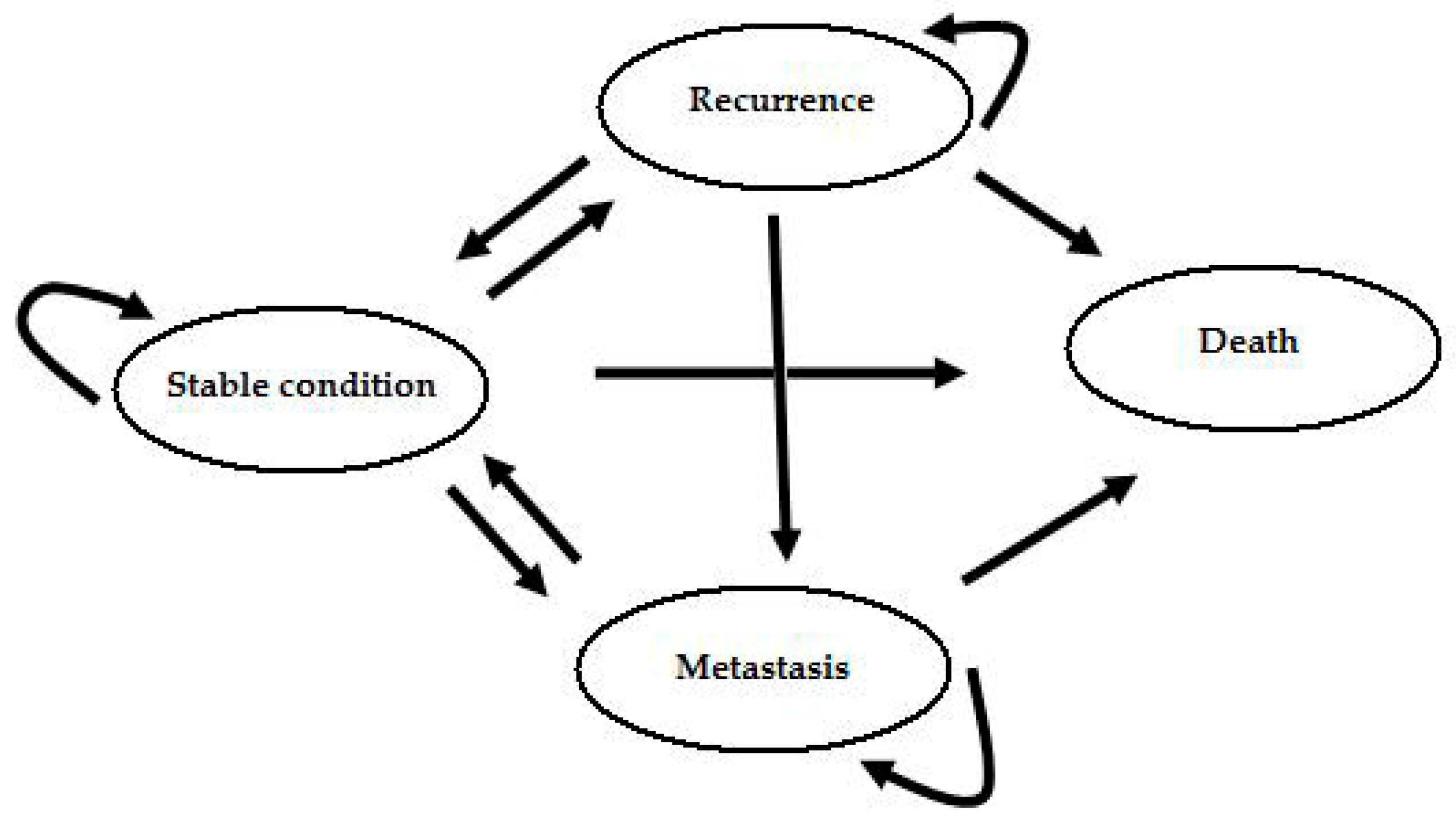
| Health States | All Trastuzumab Arms | Control Group | Three Subgroups of Trastuzumab Arms | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Transition | With Trastuzumab | Without Trastuzumab | Anthracyclines and then Trastuzumab | No Anthracyclines and Trastuzumab | Anthracyclines, Taxanes, and Trastuzumab | ||||||
| from: | to: | N | TP | N | TP | N | TP | N | TP | N | TP |
| Stable | Stable | 400 | 0.946 | 58 | 0.744 | 98 | 0.925 | 37 | 0.949 | 265 | 0.953 |
| Stable | Recurrence | 6 | 0.014 | 3 | 0.038 | 4 | 0.038 | 1 | 0.026 | 1 | 0.004 |
| Stable | Metastasis | 16 | 0.038 | 9 | 0.115 | 4 | 0.038 | 1 | 0.026 | 11 | 0.040 |
| Stable | Death | 1 | 0.002 | 8 | 0.103 | 0 | 0.000 | 0 | 0.000 | 1 | 0.004 |
| Recurrence | Stable | 5 | 0.714 | 3 | 1.000 | 3 | 0.750 | 1 | 1.000 | 1 | 0.500 |
| Recurrence | Recurrence | 1 | 0.143 | 0 | 0.000 | 0 | 0.000 | 0 | 0.000 | 1 | 0.500 |
| Recurrence | Metastasis | 1 | 0.143 | 0 | 0.000 | 1 | 0.250 | 0 | 0.000 | 0 | 0.000 |
| Recurrence | Death | 0 | 0.000 | 0 | 0.000 | 0 | 0.000 | 0 | 0.000 | 0 | 0.000 |
| Metastasis | Stable | 8 | 0.571 | 9 | 1.000 | 3 | 0.750 | 0 | 0.000 | 5 | 0.625 |
| Metastasis | Metastasis | 5 | 0.357 | 0 | 0.000 | 1 | 0.250 | 2 | 1.000 | 2 | 0.250 |
| Metastasis | Death | 1 | 0.072 | 0 | 0.000 | 0 | 0.000 | 0 | 0.000 | 1 | 0.125 |
| Parameters | Value of Basic Scenario | |||||
|---|---|---|---|---|---|---|
| Control Group | All Trastuzumab Arms | Three Subgroups of Trastuzumab Arms | Reference | |||
| without Trastuzumab | with Trastuzumab | Anthracyclines and Then Trastuzumab | No Anthracyclines and Trastuzumab | Anthracyclines, Taxanes, and Trastuzumab | ||
| Cost | ||||||
| Total costs * | € 3978.18 | € 45,420.45 | € 41,308.19 | € 43,664.83 | € 47,304.25 | ‡ |
| Utility weights | ||||||
| EQ-5D For stable condition | 0.620 | a | ||||
| EQ-5D For recurrence | 0.767 | a | ||||
| EQ-5D For metastasis | 0.692 | a | ||||
| Deducted for stable condition/recurrence | –0.215 | c | ||||
| Deducted for metastasis | –0.0519 | c | ||||
| Discount rate | ||||||
| Cost | 3% | b | ||||
| QALY | 3% | b | ||||
| Sample Characteristics | Treatment | ||||
|---|---|---|---|---|---|
| No Trastuzumab | Anthracyclines and Then Trastuzumab | No Anthracyclines and Then Trastuzumab | Anthracyclines, Taxanes, and Trastuzumab | ||
| Number of patients | 30 | 38 | 14 | 96 | |
| Height, cm (SD) | 158.0 (9.6) | 157.6 (8.4) | 158.7 (8.1) | 161.0 (9.5) | |
| Weight, kg (SD) | 68.9 (14.4) | 69.9 (10.4) | 68.1 (12.1) | 69.8 (12.4) | |
| BSA, m2 (SD) | 1.70 (0.17) | 1.71 (0.11) | 1.70 (0.15) | 1.73 (0.15) | |
| BMI, mean (SD) | 27.89 (7.08) | 28.47 (5.99) | 27.16 (5.36) | 27.16 (5.86) | |
| BMI | Normal, N (%) | 12 (40.0) | 12 (31.6) | 7 (50.0) | 38 (39.6) |
| Overweight, N (%) | 9 (30.0) | 12 (31.6) | 3 (21.4) | 35 (36.5) | |
| Obese, N (%) | 9 (30.0) | 14 (36.8) | 4 (28.6) | 23 (24.0) | |
| Age at diagnosis, mean (SD) | 53.5 (11.8) | 47.5 (8.4) | 58.8 (11.6) | 51.7 (9.7) | |
| Age at treatment initiation, mean (SD) | 53.5 (11.8) | 48.5 (8.2) | 59.8 (11.1) | 52.3 (9.7) | |
| N (%) | N (%) | N (%) | N (%) | ||
| Grade | 1 | 0 (0) | 1 (2.7) | 0 (0) | 0 (0) |
| 2 | 16 (53.3) | 19 (51.4) | 8 (57.1) | 37 (38.5) | |
| 3 | 14 (46.7) | 17 (45.9) | 6 (42.9) | 59 (61.5) | |
| Stage | IA | 7 (23.3) | 20 (52.6) | 7 (50) | 22 (22.9) |
| IB | 3 (10) | 1 (2.6) | 0 (0) | 5 (5.2) | |
| IIA | 12 (40) | 12 (31.6) | 4 (28.6) | 20 (20.8) | |
| IIB | 3 (10) | 3 (7.9) | 1 (7.1) | 22 (22.9) | |
| IIIA | 3 (10) | 1 (2.6) | 1 (7.1) | 17 (17.7) | |
| IIIB | 1 (3.3) | 1 (2.6) | 1 (7.1) | 3 (3.1) | |
| IIIC | 1 (3.3) | 0 (0) | 0 (0) | 7 (7.3) | |
| T | I | 11 (36.7) | 21 (55.3) | 9 (64.3) | 48 (50) |
| II | 16 (53.3) | 15 (39.5) | 4 (28.6) | 45 (46.9) | |
| III | 2 (6.7) | 1 (2.6) | 0 (0) | 1 (1) | |
| IV | 1 (3.3) | 1 (2.6) | 1 (7.1) | 2 (2.1) | |
| N | 0 | 19 (63.3) | 30 (78.9) | 8 (61.5) | 31 (33) |
| 1 | 8 (26.7) | 8 (21.1) | 4 (30.8) | 37 (39.4) | |
| 2 | 2 (6.7) | 0 (0) | 1 (7.7) | 19 (20.2) | |
| 3 | 1 (3.3) | 0 (0) | 0 (0) | 7 (7.4) | |
| Ki-67%, mean (SD) | 44.6 (25.2) | 30.8 (19.5) | 35 (24.8) | 38.4 (25.5) | |
| Estrogen receptors | − | 7 (23.3) | 12 (31.6) | 6 (42.9) | 33 (34.4) |
| + | 3 (10) | 3 (7.9) | 1 (7.1) | 8 (8.3) | |
| ++ | 7 (23.3) | 11 (28.9) | 2 (14.3) | 25 (26) | |
| +++ | 13 (43.3) | 12 (31.6) | 5 (35.7) | 30 (31.3) | |
| Progesteron receptors | − | 9 (30) | 15 (39.5) | 11 (78.6) | 57 (59.4) |
| + | 5 (16.7) | 8 (21.1) | 0 (0) | 11 (11.5) | |
| ++ | 6 (20) | 8 (21.1) | 1 (7.1) | 13 (13.5) | |
| +++ | 10 (33.3) | 7 (18.4) | 2 (14.3) | 15 (15.6) | |
| HER-2 | + | 1 (3.3) | 1 (2.6) | 0 (0) | 0 (0) |
| ++ | 2 (6.7) | 9 (23.7) | 3 (21.4) | 12 (12.5) | |
| +++ | 27 (90) | 28 (73.7) | 11 (78.6) | 84 (87.5) | |
| FISH, mean (SD) | 6.5 (2.4) | 5.3 (2.4) | 5.4 (2.6) | 5.1 (2.5) | |
| Hormone therapy | Yes | 26 (86.7) | 29 (76.3) | 8 (57.1) | 65 (67.7) |
| No | 4 (13.3) | 9 (23.7) | 6 (42.9) | 31 (32.3) | |
| Radiotherapy | Yes | 29 (96.7) | 31 (81.6) | 8 (57.1) | 79 (82.3) |
| No | 1 (3.3) | 7 (18.4) | 6 (42.9) | 17 (17.7) | |
| Parameters | The Three Subgroups of Trastuzumab Arms | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Control (N = 30) | Trastuzumab (N = 148) (All Trastuzumab Arms) | Anthracyclines and Then Trastuzumab (N = 38) | No Anthracyclines and Trastuzumab (N = 14) | Anthracyclines, Taxanes, and Trastuzumab (N = 96) | ||||||
| Costs (€) | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| 1st Chemo | 2786.90 | 604.85 | 2632.91 | 905.46 | 3097.47 | 396.03 | 182.14 | 63.87 | 2806.43 | 452.88 |
| 2nd Chemo * | 5105.47 | 238.88 | ||||||||
| Trastuzumab ** | 38,069.95 | 6226.03 | 38,210.71 | 5499.80 | 37,240.37 | 6380.80 | 38,135.20 | 6520.39 | ||
| Total cost | 3978.18 | 1763.79 | 45,420.45 | 7182.79 | 413,08.19 | 5588.75 | 43,664.83 | 6672.79 | 47,304.25 | 7125.32 |
| Treatment | 20 Years Horizon | Lifetime Horizon | ||||
|---|---|---|---|---|---|---|
| Total Cost (€) | QALYs | ICER * | Total Cost (€) | QALYs | ICER * | |
| Control (N = 30) | 3978.18 | 1.70 | 3978.18 | 1.82 | ||
| Trastuzumab (N = 148) (all trastuzumab arms) | 45,420.45 | 2.72 | 40,436.10 | 45,420.45 | 4.15 | 17,753.85 |
| Control (N = 30) | 3978.18 | 1.42 | 3978.18 | 1.51 | ||
| Anthracyclines and then trastuzumab (N = 38) | 41,308.19 | 3.46 | 18,301.55 | 41,308.19 | 4.17 | 8954.97 |
| No anthracyclines and trastuzumab (N = 14) | 43,664.83 | 3.14 | 23,138.90 | 43,664.83 | 2.95 | 13,445.63 |
| Anthracyclines, taxanes, and trastuzumab (N = 96) | 47,304.25 | 3.21 | 24,254.73 | 47,304.25 | 3.30 | 13,111.44 |
| Treatment | % of Simulations Made it More Cost-Effective | |||||
|---|---|---|---|---|---|---|
| 20-Year Time Horizon | Lifetime Horizon | |||||
| €20,000/QALY Gained | €40,000/QALY Gained | €60,000/QALY Gained | €20,000/QALY Gained | €40,000/QALY Gained | €60,000/QALY Gained | |
| Control group vs. Trastuzumab (all trastuzumab arms) | ||||||
| Without trastuzumab (control group) (N = 30) | 99.0% | 50.9% | 17.4% | 33.4% | 3.4% | 1% |
| Treatment with trastuzumab (N = 148) | 1.0% | 49.1% | 82.6% | 66.6% | 96.6% | 99% |
| Control group vs. three subgroups of trastuzumab arms | ||||||
| Without trastuzumab (control group) (N = 30) | 34.7% | 2.3% | 0.3% | 3.2% | 0.3% | 0% |
| Anthracyclines and then trastuzumab (N = 38) | 55.8% | 89.1% | 95.1% | 95.5% | 98.7% | 99% |
| No anthracyclines and trastuzumab (N = 14) | 5.5% | 5.8% | 3.4% | 1% | 0.9% | 1% |
| Anthracyclines, taxanes, and trastuzumab (N = 96) | 4% | 2.8% | 1.2% | 0.3% | 0.1% | 0% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ioannou, S.S.; Marcou, Y.; Kakouri, E.; Talias, M.A. Real-World Setting Cost-Effectiveness Analysis Comparing Three Therapeutic Schemes of One-Year Adjuvant Trastuzumab in HER2-Positive Early Breast Cancer from the Cyprus NHS Payer Perspective. Int. J. Environ. Res. Public Health 2020, 17, 4339. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124339
Ioannou SS, Marcou Y, Kakouri E, Talias MA. Real-World Setting Cost-Effectiveness Analysis Comparing Three Therapeutic Schemes of One-Year Adjuvant Trastuzumab in HER2-Positive Early Breast Cancer from the Cyprus NHS Payer Perspective. International Journal of Environmental Research and Public Health. 2020; 17(12):4339. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124339
Chicago/Turabian StyleIoannou, Savvas S., Yiola Marcou, Eleni Kakouri, and Michael A. Talias. 2020. "Real-World Setting Cost-Effectiveness Analysis Comparing Three Therapeutic Schemes of One-Year Adjuvant Trastuzumab in HER2-Positive Early Breast Cancer from the Cyprus NHS Payer Perspective" International Journal of Environmental Research and Public Health 17, no. 12: 4339. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124339