Interventions across the Retirement Transition for Improving Well-Being: A Scoping Review

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
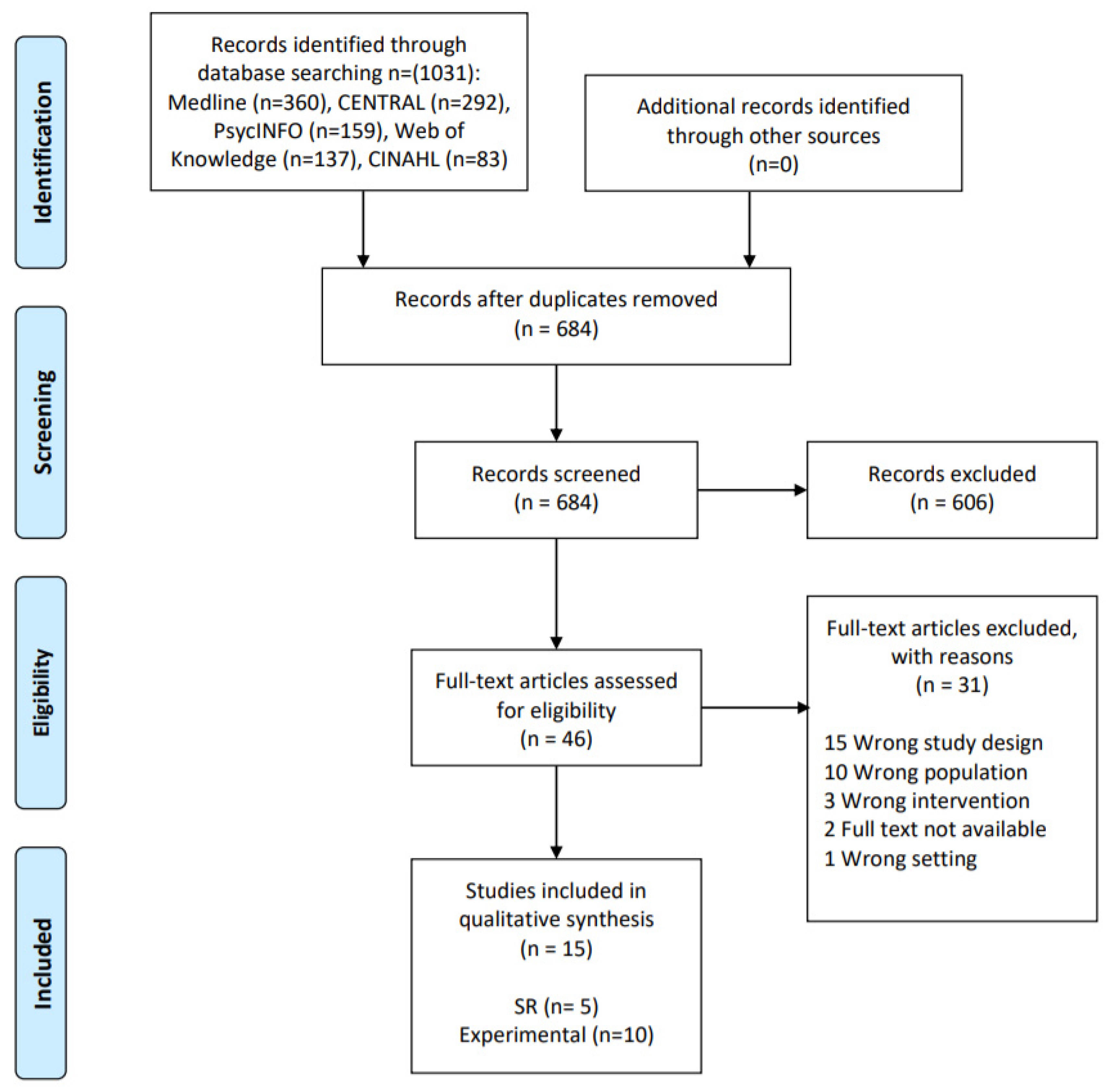
2.3. Screening and Study Selection
2.4. Data Abstraction
- Author, year of publication, journal, or other information source.
- Study population characteristics (ethnicity, age, sex, educational level, presence of physical, psychological, or social problems at baseline).
- Transition to retirement definition.
- Design of the study.
- Follow-up and retention rates.
- Intervention (type, setting, professional/person involved in the delivery, duration).
- Outcome effects (including measurement approach and tools).
- Outcome analysis.
- Study quality.
2.5. Quality Assessment
2.6. Data Analysis
2.7. Consultation
3. Results
3.1. Experimental Designs
3.1.1. General Characteristics of Included Studies
Study Design and Country
Participants
3.1.2. Objectives and Retirement Definition
3.1.3. Main Findings and Conclusions
Physical Activity
Psychological and Social Interventions
Multimodal Interventions: Physical Activity, Dietary Habits, and Social Aspects
Healthy Habits
3.1.4. Quality Assessment
3.2. Systematic Reviews
3.2.1. General Characteristics of Included Studies
3.2.2. Objectives and Retirement Definition
3.2.3. Main Findings and Conclusions
3.2.4. Quality Assessment
3.3. Gray Literature: Collection of Observational Data on Retirement and Healthy Aging
3.4. Stakeholder Consultation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, M.; Shi, J. Psychological research on retirement. Annu. Rev. Psychol. 2014, 65, 209–233. [Google Scholar] [CrossRef]
- McDonald, S.; O’Brien, N.; White, M.; Sniehotta, F.F. Changes in physical activity during the retirement transition: A theory-based, qualitative interview study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 25. [Google Scholar] [CrossRef] [Green Version]
- Lindwall, M.; Berg, A.I.; Bjälkebring, P.; Buratti, S.; Hansson, I.; Hassing, L.; Henning, G.; Kivi, M.; König, S.; Thorvaldsson, V. Psychological health in the retirement transition: rationale and first findings in the health, aging and retirement transitions in Sweden (HEARTS) study. Front. Psychol. 2017, 26, 1634. [Google Scholar] [CrossRef]
- Bender, K.A. An analysis of well-being in retirement: The role of pensions, health, and ‘voluntariness’ of retirement. J. Socio. Econ. 2012, 1, 424–433. [Google Scholar] [CrossRef] [Green Version]
- Hershey, D.A.; Henkens, K. Impact of different types of retirement transitions on perceived satisfaction with life. Gerontologist 2014, 54, 232–244. [Google Scholar] [CrossRef] [Green Version]
- Van Solinge, H. Adjustment to retirement. In The Oxford Handbook of Retirement; Wang, M., Ed.; Oxford University Press: New York, NY, USA, 2013; pp. 311–324. [Google Scholar]
- Syse, A.; Veenstra, M.; Furunes, T.; Mykletun, R.J.; Solem, P.E. Changes in health and health behavior associated with retirement. J. Aging Health 2017, 29, 99–127. [Google Scholar] [CrossRef] [Green Version]
- Van der Heide, I.; van Rijn, R.M.; Robroek, S.J.; Burdorf, A.; Proper, K.I. Is retirement good for your health? A systematic review of longitudinal studies. BMC Public Health 2013, 13, 1180. [Google Scholar] [CrossRef] [Green Version]
- Zantinge, E.M.; van den Berg, M.; Smit, H.A.; Picavet, H.S.J. Retirement and a healthy lifestyle: Opportunity or pitfall? A narrative review of the literature. Eur. J. Public Health 2014, 24, 433–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiba, K.; Kondo, N.; Kondo, K.; Kawachi, I. Retirement and mental health: Does social participation mitigate the association? A fixed-effects longitudinal analysis. BMC Public Health 2017, 17, 526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaap, R.; de Wind, A.; Coenen, P.; Proper, K.; Boot, C. The effects of exit from work on health across different socioeconomic groups: A systematic literature review. Soc. Sci. Med. 2018, 198, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shlomo, Y. A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. Int. J. Epidemiol. 2002, 31, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Hill, P.L.; Weston, S.J.; Jackson, J.J. Connecting social environment variables to the onset of major specific health outcomes. Psychol. Health 2014, 29, 753–767. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Aging and Health. Available online: http://www.who.int/news-room/fact-sheets/detail/aging-and-health (accessed on 17 September 2018).
- Ministerio de Sanidad SeS e I. Indicadores Clave del Sistema Nacional de Salud MSSS. 2015. Available online: http://inclasns.msssi.es/main.html (accessed on 20 January 2019).
- European Commission. Directorate-General for Economic and Financial Affairs, Economic Policy Committee of the European Communities. The 2018 Aging Report: Economic and Budgetary Projections for the EU Member States [2016–2070]. 2018. Available online: https://ec.europa.eu/info/sites/info/files/economy-finance/ip079_en.pdf (accessed on 1 April 2020).
- Kirsten, T.G.J.C.; Van der Walt, H.J.L.; Viljoen, C.T. Health, well-being and wellness: An anthropological eco-systemic approach. Heal SA Gesondheid. 2009, 14, 7. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Constitution [Internet]. 2019 [Cited 2020 Apr 22]. Available online: https://www.who.int/about/who-we-are/constitution (accessed on 1 April 2020).
- Lara, J.; Evans, E.H.; O’Brien, N.; Moynihan, P.J.; Meyer, T.D.; Adamson, A.J.; Errington, L.; Sniehotta, F.; White, M.; Mathers, J. Association of behavior change techniques with effectiveness of dietary interventions among adults of retirement age: A systematic review and meta-analysis of randomised controlled trials. BMC Med. 2014, 12, 177. [Google Scholar]
- Heaven, B.; Brown, L.J.E.; White, M.; Errington, L.; Mathers, J.C.; Moffatt, S. Supporting well-being in retirement through meaningful social roles: Systematic review of intervention studies. Milbank Q. 2013, 91, 222–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, S.; Vieira, R.; Godfrey, A.; O’Brien, N.; White, M.; Sniehotta, F.F. Changes in physical activity during the retirement transition: A series of novel n-of-1 natural experiments. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 167. [Google Scholar] [CrossRef] [Green Version]
- Lara, J.; O’Brien, N.; Godfrey, A.; Heaven, B.; Evans, E.H.; Lloyd, S.; Moffatt, S.; Moynihan, P.; Meyer, T.; Rochester, L. Pilot randomised controlled trial of a web-based intervention to promote healthy eating, physical activity and meaningful social connections compared with usual care control in people of retirement age recruited from workplaces. PLoS ONE 2016, 11, e0159703. [Google Scholar] [CrossRef] [Green Version]
- Werkman, A.; Hulshof, P.J.; Stafleu, A.; Kremers, S.P.; Kok, F.J.; Schouten, E.G.; Schuit, A.J. Effect of an individually tailored one-year energy balance program on body weight, body composition and lifestyle in recent retirees: A cluster randomised controlled trial. BMC Public Health 2010, 10, 110. [Google Scholar] [CrossRef] [Green Version]
- Marmot, M. Social justice, epidemiology and health inequalities. Eur. J. Epidemiol. 2017, 32, 537–546. [Google Scholar] [CrossRef]
- WHO Europe. Review of Social Determinants and the Health Divide in the WHO European Region: Final Report; WHO Regional Office Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Berkman, L.; Kawachi, I. A historical franmework for social epidemiology. In Social Epidemiology, 2nd ed.; Berkman, L., Kawachi, I., Glymour, M., Eds.; Oxford University Press: New York, NY, USA, 2014; pp. 1–16. [Google Scholar]
- Einolf, C.J. Gender differences in the correlates of volunteering and charitable giving. Nonprofit Volunt Sect Q. 2011, 40, 1092–1112. [Google Scholar] [CrossRef]
- Arcaya, M.C.; Arcaya, A.L.; Subramanian, S.V. Inequalities in health: Definitions, concepts, and theories Motivation for studying health inequalities. Glob. Health Action. 2015, 8. [Google Scholar] [CrossRef] [PubMed]
- Blane, D.; Netuveli, G.; Stone, J. The development of life course epidemiology. Rev. Epidemiol. Sante Publique. 2007, 55, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peteres, M.D.J.; Horsley, T.; Weeks, L. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, M.D.J.; Godfrey, C.M.; Mcinerney, P.; Soares, C.B.; Khalil, H.; Parker, D. Methodology for JBI Scoping Reviews. Joanna Briggs Insitute. 2015. Available online: https://nursing.lsuhsc.edu/JBI/docs/ReviewersManuals/Scoping-.pdf (accessed on 22 April 2020).
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred Reporting Items for Systematic review and Meta-Analysis Protocols (PRISMA-P) 2015 Elaboration and Explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Monforte, M.; Fernández-Jané, C.; Martin-Arribas, A.; Sitjà-Rabert, M.; Canet Vélez, O.; Sanromà-Ortiz, M.; Vilaró, J.; Carrillo-Alvarez, E. Interventions across the retirement transition for improving well-being: A scoping review protocol. BMJ Open 2019, 9, e030484. [Google Scholar]
- CADTH: Canadian Agency for Drugs and Technologies in Health. Gray Matters: A Practical Search Tool for Evidence-Based Medicine. CADTH. 2014. Available online: https://www.cadth.ca/resources/finding-evidence/grey-matters (accessed on 22 April 2020).
- Pace, R.; Pluye, P.; Bartlett, G.; Macaulay, A.C.; Salsberg, J.; Jagosh, J.; Seller, R. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int. J. Nurs. Stud. 2012, 49, 47–53. [Google Scholar] [CrossRef]
- Shea, B.J.; Hamel, C.; Wells, G.A.; Bouter, L.M.; Kristjansson, E.; Grimshaw, J.; Henry, A.D.; Boers, M. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J. Clin. Epidemiol. 2009, 62, 1013–1020. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, D.; Rechnitzer, P.; Howard, J.; Donner, A. Exercise training of men at retirement: A clinical trial. J. Gerontol. 1987, 42, 17–23. [Google Scholar] [CrossRef]
- Fries, J.F.; Bloch, D.A.; Harrington, H.; Richardson, N.; Beck, R. Two-year results of a randomized controlled trial of a health promotion program in a retiree population: The Bank of America Study. Am. J. Med. 1993, 94, 455–462. [Google Scholar] [CrossRef]
- Fries, J.F.; Harrington, H.; Edwards, R.; Kent, L.A.; Richardson, N. Randomized controlled trial of cost reductions from a health education program: The California Public Employees’ Retirement System (PERS) study. Am. J. Heal Promot. 1994, 8, 216–223. [Google Scholar] [CrossRef]
- Dubé, M.; Bouffard, L.; Lapierre, S.; Alain, M. La santé mentale par la gestion des projets personnels: Une intervention auprès de jeunes retraités. Santé Ment Quebeq. 2005, 2, 221–244. [Google Scholar]
- Lapierre, S.; Dube, M.; Bouffard, L.L.; Alain, M. Addressing suicidal ideations through the realization of meaningful personal goals. Crisis 2007, 28, 16–25. [Google Scholar] [CrossRef]
- Ashe, M.C.; Winters, M.; Hoppmann, C.A.; Dawes, M.G.; Gardiner, P.A.; Giangregorio, L.M.; Madden, K.M.; McAllister, M.M.; Wong, G.; Puyat, J.H. “Not just another walking program”: Everyday Activity Supports You (EASY) model-a randomized pilot study for a parallel randomized controlled trial. Pilot Feasibility Stud. 2015, 1, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stancliffe, R.J.; Bigby, C.; Balandin, S.; Wilson, N.J.; Craig, D. Transition to retirement and participation in mainstream community groups using active mentoring: A feasibility and outcomes evaluation with a matched comparison group. J. Intell. Disabil. Res. 2015, 59, 703–718. [Google Scholar] [CrossRef] [PubMed]
- Van Dyck, D.; Plaete, J.; Cardon, G.; Crombez, G.; De Bourdeaudhuij, I. Effectiveness of the self-regulation eHealth intervention “MyPlan1.0.” on physical activity levels of recently retired Belgian adults: A randomized controlled trial. Health Educ. Res. 2016, 31, 653–664. [Google Scholar] [CrossRef] [Green Version]
- Vrkljan, B.; Montpetit, A.; Naglie, G.; Rapoport, M.; Mazer, B. Interventions that support major life transitions in older adulthood: A systematic review. Int. Psychogeriatrics. 2018, 31, 1–23. [Google Scholar] [CrossRef]
- Baxter, S.; Johnson, M.; Payne, N.; Buckley-Woods, H.; Blank, L.; Hock, E.; Daley, A.; Taylor, A.; Pavey, T.; Mountain, G. Promoting and maintaining physical activity in the transition to retirement: A systematic review of interventions for adults around retirement age. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loureiro, H.; Mendes, A.; Rodrigues, R.R.; Apostolo, J.; Rodrigues, M.A.A.; Cardoso, D.; Pedreiro, A.T. The experience of programs to promote health in retirement: A systematic review of qualitative evidence. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 276–294. [Google Scholar] [CrossRef]
- Wilson, D.M.; Palha, P. A systematic review of published research articles on health promotion at retirement: Clinical scholarship. J. Nurs. Scholarsh. 2007, 39, 330–337. [Google Scholar] [CrossRef]
- Gateway to Global Aging Data. Available online: https://g2aging.org/ (accessed on 22 April 2020).
- The Survey of Health, Aging and Retirement in Europe (SHARE): Home. Available online: http://www.share-project.org/home0.html (accessed on 22 April 2020).
- WHO Study on Global Aging and Adult Health (SAGE). WHO. 2003, 9. Available online: https://www.who.int/healthinfo/sage/en/ (accessed on 22 April 2020).
- International Sister Studies. Health and Retirement Study. Available online: https://hrs.isr.umich.edu/about/international-sister-studies?_ga=2.114424135.1919987097.1584963781-1272461212.1584963781 (accessed on 22 April 2020).
- JSTAR (Japanese Study of Aging and Retirement). Available online: https://www.rieti.go.jp/en/projects/jstar/index.html (accessed on 22 April 2020).
- The Survey of Health, Aging and Retirement in Europe (SHARE): Spain. Available online: http://www.share-project.org/organisation/share-country-teams/spain.html (accessed on 22 April 2020).
- OECD. Pension Markets in Focus. 2019. Available online: https://www.oecd.org/daf/fin/private-pensions/Pension-Markets-in-Focus-2019.pdf (accessed on 1 April 2020).
- Carr, E.; Fleischmann, M.; Goldberg, M.; Kuh, D.; Murray, E.T.; Stafford, M.; Stasnfeld, S.; Vahtera, J.; Xue, B.; Zaninotto, P. Occupational and educational inequalities in exit from employment at older ages: Evidence from seven prospective cohorts. Occup. Environ. Med. 2018, 75, 369–377. [Google Scholar] [CrossRef]
- Green, J.; Tones, K.; Cross, R.; Woodall, J. Health Promotion: Planning & Strategies, 3rd ed.; SAGE: Los Angeles, CA, USA, 2015. [Google Scholar]
- Kampmeijer, R.; Pavlova, M.; Tambor, M.; Golinowska, S.; Groot, W. The use of e-health and m-health tools in health promotion and primary prevention among older adults: A systematic literature review. BMC Health Ser. Res. 2016, 16, 290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robbins, T.D.; Lim Choi Keung, S.N.; Arvanitis, T.N. E-health for active aging; A systematic review. Maturitas 2018, 114, 34–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Author, Year | Number of Participants (Male: Female) | Age: Mean (SD) | Ethnicity | Economic Level | Education Level | Presence of Physical, Psychological, or Social Problems at Baseline (Inclusion Criteria) |
|---|---|---|---|---|---|---|
| Cunningham, 1987 [37] | 224 (224: 0) | 62.7 | NR | $10,000 (C: 11.7, I: 8.8) 10,000–19,999 (C: 46.8, I: 47.8) 20,000–29,999 (C: 27, I: 25.7) 30,000–39,999 (C: 9,0, I: 11.5) 39,999 (C: 5.4, I: 6.2) | NR | NR |
| Fries, 1993 [38] | 1936 (977: 959) | I: 68.3 C: 68.7 | NR | NR | NR | NR |
| Fries, 1994 [39] | 12,838 | 63.6 | NR | NR | NR | NR |
| Dubé, 2005 [40] | 117 (81: 36) | I: 57.9 (3.26) C: 57.6 (3.01) | NR | NR | Mean years of education I: 14.1 (2.97); C: 14.2 (3.34) | None |
| Lapierre, 2007 [41] | 21 (11: 10) | 56.7 (1.9) | Caucasian | NR | Mean years of education: 15.2 (2.36) | Presence of suicidal ideations in the last week |
| Werkman, 2010 [23] | 413 (352: 61) | I: 59.5 (2.0) C: 59.4 (2.0) | NR | NR | Low education level (primary school or low vocational education) I: 25%; C: 23% | Not undergoing medical treatments that might affect body composition |
| Ashe, 2015 [42] | 20 (0: 20) | I: 64.8 (4.6) C: 63.1 (4.8) | NR | NR | Secondary education | Healthy inactive |
| Stancliffe, 2015 [43] | 58 (32: 16) | I: 57.4 C: 53.8 | NR | NR | NR | Presence of intellectual disability |
| Lara, 2016 [22] | 75 (18: 57) | 61.0 (4.0) | NR | NR | NR | Absence of depression or severe mental health conditions |
| Van Dyck, 2016 [44] | 284 (134: 150) | I: 63.1 (2.2) C: 63.2 (2.0) | NR | NR | University degree I: 55.1%; C: 53% | Ability to walk 100 m without assistance |
| Author, Year | Country (C) Settings (S) Funding (F) Design (D) | Aim | Transition to Retirement Definition | Intervention Description (ID), Provider (P) and Duration (DU) | Control | Outcomes Measures (OM), Endpoint (E) | Main Findings |
|---|---|---|---|---|---|---|---|
| Cunningham, 1987 [37] | C: Canada S: NR F: Ontario Ministry of Health D: RCT | To evaluate the effects of one-year exercise training on cardiorespiratory fitness, levels of daily leisure activity, and blood lipids (CT and HDL-CT) | 2–4 months prior to retirement | ID: Physical Activity: three group sessions per week (plus one day on their own). Each training session consisted of a 10- to 15-min warm-up, 30 min of walking or jogging at an individualized pace, and a 10-min warm-down P: exercise leader DU: 1 year | No intervention | OM: anthropometry measures (weight, fatness), cardiorespiratory fitness (VO2, respiratory exchange ratio, heart rate; ECG, treadmill test), blood lipids (CT, HDL-CT), leisure activity levels (Minnesota Leisure Time Activity questionnaire), grip strength and flexibility E: 1-year post-intervention | VO2 increased compared to controls. There were no significant changes in maximal heart rate and respiratory exchange ratio although ventilation increased significantly in the trained group No significant differences were found between the groups with respect to the remaining outcomes |
| Fries, 1993 [38] | C: USA S: On-line/post mail F: Blue Shield of California, and Bank of America D: RCT | To evaluate the effectiveness of a health promotion program in a retiree population in terms of health risk and medical cost reduction | 55–75 years | ID: health education emphasizing self-care: individualized reports and recommendations based on health assessment and provision of educational materials P: self-management DU: 24 months | Education regarding risk appraisals only, without feedback, for the first 12 months and subsequently the full intervention for the second 12 months | OM: health risk score (Framingham multiple risk logistic for CVD); health habits/indicators (seat belt use, BMI, dietary and saturated fat intake, cigarette-smoking, exercise) E: 6, 12, 18, 24 months | Health risk scores improved by 12% at 12 months compared with the control and by 23% at 24 months Individual health habit changes were favorable for all parameters studied and were highly statistically significant for most variables (except weight, CT and BP) |
| Fries, 1994 [39] | C: USA S: On-line/post mail F: Blue Shield of California, National Health Management Foundation D: RCT | To evaluate the cost trend reduction from a health promotion program | NR | ID: health education emphasizing self-care: individualized reports and recommendations based on health assessment and provision of educational materials P: self-management DU: 12 months | Passive portions of the program, including the self-management book and other educational materials. | OM: Health risk scores (Framingham multiple-risk logistic function); health habits/indicators (SBP, CT, seat belt use, pounds over ideal weight, high salt intake, salt dietary fat, cigarette smoking, alcohol intake, exercise, stress); self-reported medical utilization; claims paid E: 6, 12, 18 months | The program was associated with a reduction in health risk scores at 12 months, a reduction of subject reported medical utilization from baseline and a decrease in claims cost growth relative to controls |
| Dubé, 2005 [40] | C: Canada S: NR F: NR D: Pre-post | To evaluate the effectiveness of a goal-oriented intervention offered to retirees in order to increase their psychological well-being and their mental health and specifically to promote the expression, planning and realization of personal projects through a learning process based on a cognitive approach | 50–65 years | ID: social support and psychological adjustment: management of personal aims. The program consisted on 10 to 12 meetings a total of 10 h in groups of 7 to 10 people P: retiree and a psychologist graduate student DU: the duration of the 10 to 12 meetings | No intervention | OM: the psychological well-being was assessed using five different indicators and instruments: emotional well-being during retirement (Retirement Experience Assessment scale; Short-term happiness (Short Happiness and Affect Research Protocol (SHARP); meaning of life (Ryffs’ six scales of psychological well-being; inner peace (the Serenity Scale); distress during the past weeks (index of psychological distress) E: at the end of the intervention and 6 moths post intervention | The experimental group improved significantly more than the control group on all the goal and subjective well-being indicators Gain was maintained six months later |
| Lapierre, 2007 [41] | C: Canada S: NR F: Conseil Québécois de la Recherche Sociale D: Quasi experimental | To evaluate a personal goal intervention program for early retirees in terms of their subjective well-being and levels of depression in the participants with suicidal ideations | 50–65 years and being retired for more than 6 years | ID: psychological adjustment: cognitive-behavioral approach with 10 to 12 meetings of 2 h each week for small groups. P: retiree and a psychologist graduate student DU: 2.5 years | No intervention | OM: the psychological well-being was assessed using different indicators and instruments: positive experience with retirement, happiness, serenity, Ryffs’ well-being dimensions (personal growth, self-acceptance, positive relationships with others, environmental mastery, purpose in life, autonomy), flexibility, tenacity, depression, and distress. E: 12 weeks and 6 months | The experimental group had improved significantly more than the control group on hope, goal realization process, serenity, flexibility, and positive attitude toward retirement The levels of depression and psychological distress significantly decreased These gains were maintained 6 months later |
| Werkman, 2010 [23] | C: The Netherlands S: Community and domiciliary F: Netherlands Heart Foundation D: RCT | To investigate the effect of a one year low-intensity computer-tailored energy balance program | 55–65 years and being retired for more than 6 months | ID: physical activity and diet: one-year multifaceted program including these factors using computer tailored feedback P: NR DU: 12 months | Newsletters with general information about the study, such as study progress, and information about art exhibitions and city trips for instance. | OM: waist circumference, body weight and body composition, BP, physical activity and dietary Intake E: 12- and 24-months follow-up | The program did not have a significant effect on any of the outcomes though it showed a pattern of small, non-significant effects on changes in body composition, physical activity and dietary behavior. Transition to occupational retirement and/or participation in research had a greater impact than the intervention program itself |
| Ashe, 2015 [42] | C: Canada S: NR F: Canadian Institutes of Health Research D: Pilot RCT | To test study feasibility for the Everyday Activity Supports You (EASY) model which seeks to encourage movement through daily activities and utilitarian walking | 55–70 years | ID: group-based education and social support, individualized physical activity prescription and use of an activity monitor (Fitbit) P: personal trainer or exercise physiologist, dietitian D: 6 months | Monthly education sessions, but did not receive information on the importance of exercise or how to sustain an active lifestyle. They had no interactions with the exercise professionals nor did they receive Fitbit monitors. | OM: recruitment and retention rates, satisfaction, physical activity (average daily step count), MVPA (min/day), sedentary behavior (min/day, percentage/day), BP, BMI, social connectedness, self-rated health, self-efficacy, and intentions for physical activity E: 3 and 6 months | The model was feasible to deliver in a community setting to women at retirement age. Partici-pants were highly engaged in, and satisfied with, the EASY model The intervention was effective to increase physical activity and decrease weight and BP |
| Stancliffe, 2015 [43] | C: Australia S: Domiciliary F: NR D: Pilot RCT | To examine the feasibility of supporting older adults with disability to attend a mainstream community group; the types of mainstream community groups or volunteering groups that participants joined; the duration of participants’ weekly attendance at their group; and changes in outcomes experienced by participants | ≥45 years | ID: social support and psychological adjustment: active mentoring - support from community group members. P: non-professional trained mentors from the community DU: 6 months | Paired working individuals who did not receive any intervention | OM: self-reported or proxy-reported: depression (GDS, Mini PAS-ADD); aloneness Loneliness (MWLQ); social satisfaction (MWLQ); loneliness (UCLA Loneliness Scale); quality of Life (SF-36); life events (Mini PAS-ADD); participation and social contacts (Weekly logs) E: 6 months | The community participation increased, making an average of four new social contacts and decreasing their work hours. Intervention participants were more socially satisfied post-intervention than comparison group members |
| Lara, 2016 [22] | C: UK S: On-line F: Lifelong Health and Well-being Cross-Council research initiative, UK Health Departments D: Pilot RCT | To assess the feasibility and acceptability of the intervention, the trial design, the procedures and the outcome measures of a web-based platform (Living, eating, activity and planning through retirement; LEAP) promoting healthy eating, physical activity and meaningful social roles | ≤2 years of retirement, pre-retired or to be retired in the following 2 years | ID: physical activity, healthy eating, meaningful social connections. The intervention comprises the following five modules: (1) time, (2) changing work, (3) moving more, (4) being social and (5) eating well P: on-line platform DU: 8 weeks | Usual care: comprehensive health information service which encourages people to make healthy choices | OM: anthropometric measures (weight, BMI, waist circumference, body fat mass, fat free mas, total body water); dietary intake (multiple pass 24-hour); physical activity (accelerometer) feasibility and acceptability (completion rates and qualitative feedback) E: 8 weeks | “Moving more,” “eating well,” and “being social” were the most visited modules. At interview, participants reported that diet and physical activity modules were important and acceptable within the context of healthy aging |
| Van Dyck, 2016 [44] | C: Belgium S: On-line F: Research Foundation Flanders, Ministry of the Flemish Community, Department of Welfare, Public Health and Family D: RCT | To test the effectiveness of the self-regulation eHealth intervention ‘MyPlan1.0.’ to increase physical activity in recently retired Belgian adults | >6 months and <5 years of retirement | ID: physical activity: self-regulation eHealth intervention focused on pre- and post-intentional processes of behavioral change P: on-line platform DU: 5 weeks | No intervention | OM: Self-reported physical activity (IPAQ) E: 1 week and 1 month | At 1 week, the intervention significantly increased walking for transport. At 1 month, the intervention increased transport related walking, leisure time walking, leisure time vigorous physical activity, moderate intensity gardening, voluntary work-related vigorous physical activity |
| Author, Year | Objective/Research Question | Inclusion Criteria | Main Findings | |||
|---|---|---|---|---|---|---|
| Study Type | Participants | Intervention (I) Control (C) | Outcomes | |||
| Vrkljan, 2018 [45] | To examine the effectiveness of published interventions across the three most common life transitions in older adulthood, namely, bereavement, retirement from paid employment, and relocation of residence to a higher level of care | RCT, non RCT and systematic reviews | Intervention targeting individuals in bereavement, retirement from paid employment, and relocation to a higher level of care | I: Any C: Any | Any | N = 2 Results suggest that group-based approaches provided by trained personnel can be effective, but further study is warranted. |
| Baxter, 2016 [46] | To synthesize international evidence on the types and effectiveness of interventions to increase physical activity among people around the time of retirement | Experimental and observational studies | People during and shortly after the transition to retirement In the absence of literature, age was used as a proxy for the period of retirement transition | I: Interventions which aimed to increase and/or maintain levels of physical activity. C: Any | Direct and indirect measures of physical activity, Social, psychological, behavioral and environmental outcomes. | N = 64 Little research has been conducted to assess whether physical activity interventions at this time may be effective in promoting or maintaining activity or reducing health inequalities. No evidence supported that transition to retirement period was or was not a significant point for intervention. Studies in older adults more generally indicated that a range of interventions might be effective for people around retirement age. |
| Loureiro, 2015 [47] | To identify programs that have been implemented with the goal of promoting the health of individuals and their families during their adjustment to retirement | Interpretive or critical studies | Individuals newly retired (within five years of retirement) and their families | I: Any C: Any | Any | N = 0 Authors could not identify any program. |
| Heaven, 2013 [20] | What kinds of intervention have been developed to promote social roles in retirement? How much have they improved perceived roles? Have these roles improved health or well-being? | Intervention studies | Participants were included if they fulfilled one of the following conditions 3: 1-Median age was between 55 and 70 years 2-Had been selected for the study because they were about to retire or had retired within the past two years; or 3-If they were selected for the study because they had a partner who met one of these criteria | I: Interventions that could extend or support the participants’ social roles C: Any | Participants’ perception of their social roles or well-being | N = 11 Social roles are linked to well-being outcomes through the way in which they are interpreted (such as providing feelings of worth, purpose, or perceptions of usefulness and status) |
| Wilson, 2007 [48] | To assess the state of science and accumulated evidence on of health promotion at retirement | Any | Retired population | I: Any C: Any | Any | N = 0 Authors did not identify any experimental trial. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Monforte, M.; Fernández-Jané, C.; Martin-Arribas, A.; Costa-Tutusaus, L.; Sitjà-Rabert, M.; Ramírez-García, I.; Canet Vélez, O.; Kopp, J.; Vilaró, J.; Carrillo-Alvarez, E. Interventions across the Retirement Transition for Improving Well-Being: A Scoping Review. Int. J. Environ. Res. Public Health 2020, 17, 4341. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124341
Rodríguez-Monforte M, Fernández-Jané C, Martin-Arribas A, Costa-Tutusaus L, Sitjà-Rabert M, Ramírez-García I, Canet Vélez O, Kopp J, Vilaró J, Carrillo-Alvarez E. Interventions across the Retirement Transition for Improving Well-Being: A Scoping Review. International Journal of Environmental Research and Public Health. 2020; 17(12):4341. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124341
Chicago/Turabian StyleRodríguez-Monforte, Miriam, Carles Fernández-Jané, Anna Martin-Arribas, Lluís Costa-Tutusaus, Mercè Sitjà-Rabert, Inés Ramírez-García, Olga Canet Vélez, Jenna Kopp, Jordi Vilaró, and Elena Carrillo-Alvarez. 2020. "Interventions across the Retirement Transition for Improving Well-Being: A Scoping Review" International Journal of Environmental Research and Public Health 17, no. 12: 4341. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124341