Bottom-Up Kinetic Chain in Drop Landing among University Athletes with Normal Dynamic Knee Valgus


Abstract
:1. Introduction
2. Materials and Methods
2.1. Drop Vertical Jump at Different Heights
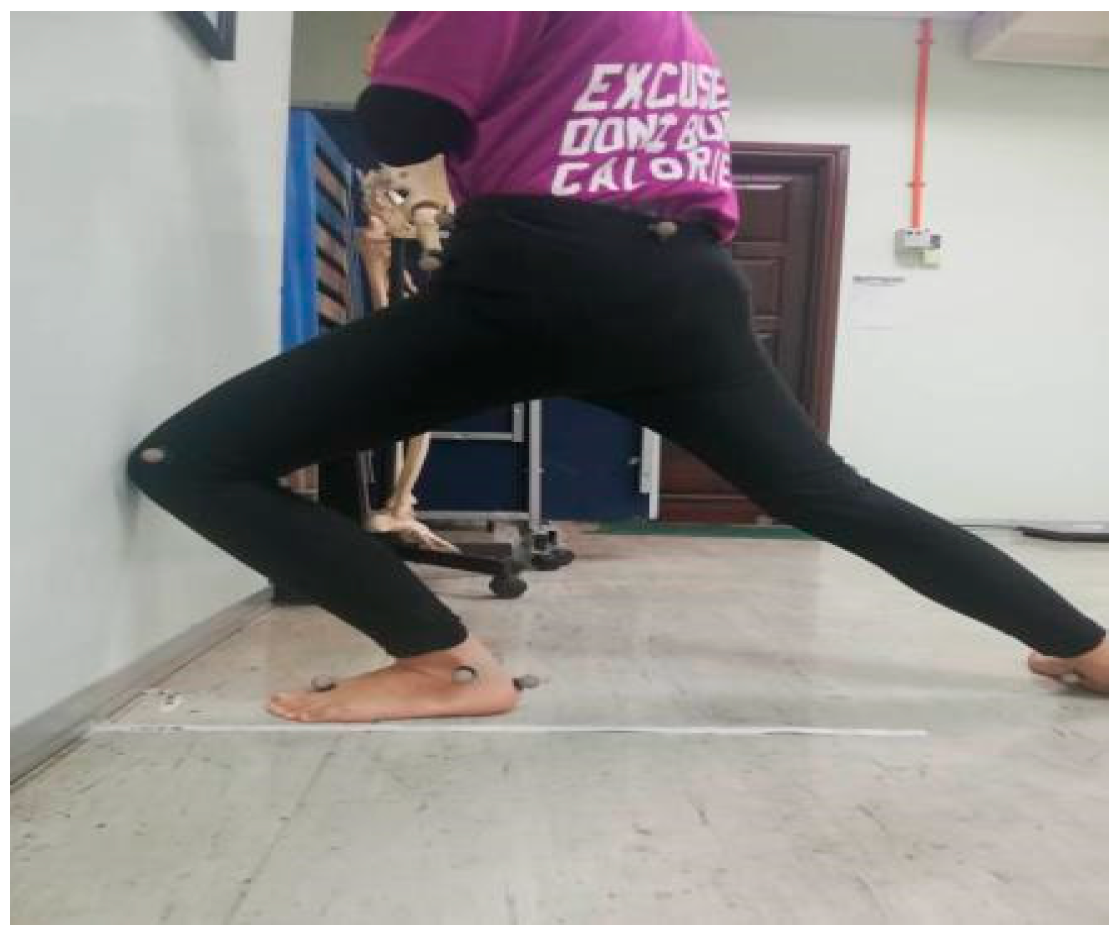
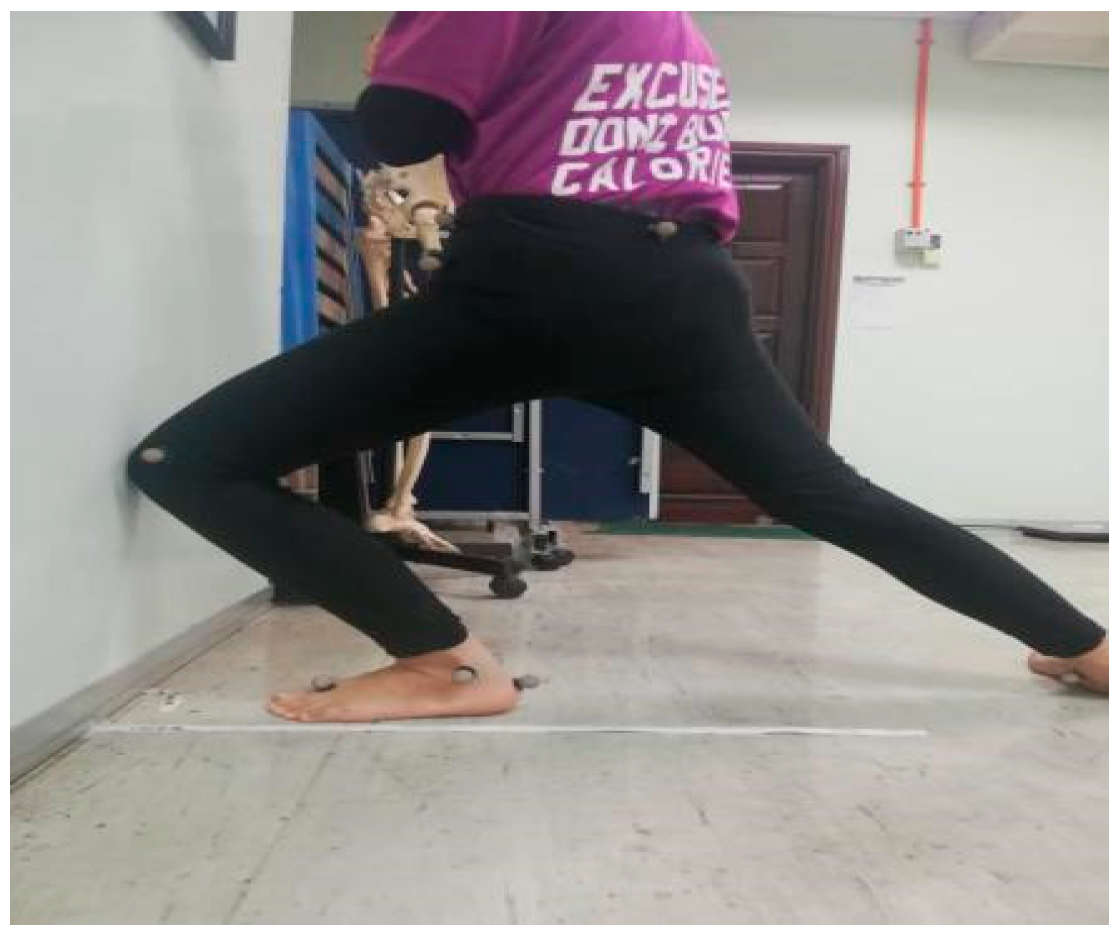
2.2. Weight-Bearing Lunge Test
2.3. Isokinetic Ankle Strength Test
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Willson, J.D.; Davis, I.S. Utility of the frontal plane projection angle in females with patellofemoral pain. J. Orthop. Sports Phys. Ther. 2008, 38, 606–615. [Google Scholar] [CrossRef]
- Dufek, J.S.; Bates, B.T. Biomechanical factors associated with injury during landing in jump sports. Sports Med. 1991, 12, 326–337. [Google Scholar] [CrossRef]
- Pattyn, E.; Verdonk, P.; Steyaert, A.; Vanden Bossche, L.C.; Van den Broecke, W.; Thijs, Y.; Witvrouw, E. Vastus medialis obliquus atrophy: Does it exist in patellofemoral pain syndrome? Am. J. Sports Med. 2011, 39, 1450–1455. [Google Scholar] [CrossRef]
- Barton, C.; Lack, S.; Hemmings, S.; Tufail, S.; Morrissey, D. The ‘best practice guide to conservative management of patellofemoral pain’: Incorporating level 1 evidence with expert clinical reasoning. Br. J. Sports Med. 2015, 49, 923–934. [Google Scholar] [CrossRef]
- Barwick, A.; Smith, J.; Chuter, V. The relationship between foot motion and lumbopelvic-hip function: A review of the literature. Foot Ankle Int. 2012, 22, 224–231. [Google Scholar] [CrossRef]
- Dix, J.; Marsh, S.; Dingenen, B.; Malliaras, P. The relationship between hip muscle strength and dynamic knee valgus in asymptomatic females: A systematic review. Phys. Ther. Sport. 2019, 37, 197–209. [Google Scholar] [CrossRef] [Green Version]
- Snyder, K.R.; Earl, J.E.; O’Connor, K.M.; Ebersole, K.T. Resistance training is accompanied by increases in hip strength and changes in lower extremity biomechanics during running. Clin. Biomech. 2009, 24, 26–34. [Google Scholar] [CrossRef]
- Baldon, R.D.M.; Lobato, D.F.M.; Carvalho, L.P.; Wun, P.Y.L.; Santiago, P.R.P.; Serrão, F.V. Effect of functional stabilization training on lower limb biomechanics in women. Med. Sci. Sports Exerc. 2012, 44, 135–145. [Google Scholar] [CrossRef]
- Khamis, S.; Yizhar, Z. Effect of feet hyperpronation on pelvic alignment in a standing position. Gait Posture 2007, 25, 127–134. [Google Scholar] [CrossRef]
- Abdullah, H. The Relationship between Hip Strength and Peak Knee Valgus Angle during Single Leg Squat. J. Nurs. Health Sci. 2016, 5, 99–106. [Google Scholar]
- Ishida, T.; Yamanaka, M.; Takeda, N.; Aoki, Y. Knee rotation associated with dynamic knee valgus and toe direction. Knee 2014, 21, 563–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nigg, B.M.; Balich, J.; Federolf, P.; Manz, S.; Nigg, S. Functional relevance of the small muscles crossing the ankle joint—The bottom-up approach. Curr. Issues Sport Sci. 2017, 2. [Google Scholar] [CrossRef]
- Mason-Mackay, A.; Whatman, C.; Reid, D. The effect of reduced ankle dorsiflexion on lower extremity mechanics during landing: A systematic review. J. Sci. Med. Sport 2017, 20, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Fong, C.M.; Blackburn, J.T.; Norcross, M.F.; McGrath, M.; Padua, D.A. Ankle-dorsiflexion range of motion and landing biomechanics. J. Athl. Train. 2011, 46, 5–10. [Google Scholar] [CrossRef] [Green Version]
- Lopes, L.; Matheus, V.; Lima, P.; Bezerra, M. The association of ankle dorsiflexion range of motion and dynamic knee valgus: A systematic review and meta-analysis. Phys. Ther. Sport 2017, 16, 1–4. [Google Scholar] [CrossRef]
- Malloy, P.; Morgan, A.; Meinerz, C.; Geiser, C.; Kipp, K. The association of dorsiflexion flexibility on knee kinematics and kinetics during a drop vertical jump in healthy female athletes. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 3550–3555. [Google Scholar] [CrossRef]
- Hoch, M.C.; Farwell, K.E.; Gaven, S.L.; Weinhandl, J.T. Weight-bearing dorsiflexion range of motion and landing biomechanics in individuals with chronic ankle instability. J. Athl. Train. 2015, 50, 833–839. [Google Scholar] [CrossRef] [Green Version]
- Yeow, C.; Lee, P.; Goh, J. Effect of landing height on frontal plane kinematics, kinetics and energy dissipation at lower extremity joints. J. Biomech. 2009, 42, 1967–1973. [Google Scholar] [CrossRef]
- Munro, A.; Herrington, L.; Carolan, M. Reliability of 2-dimensional video assessment of frontal-plane dynamic knee valgus during common athletic screening tasks. J. Sport Rehabil. 2012, 21, 7–11. [Google Scholar] [CrossRef]
- Nimphius, S. Exercise and sport science failing by design in understanding female athletes. Int. J. Sports Physiol. Perform. 2019, 14, 1157–1158. [Google Scholar] [CrossRef]
- Nimphius, S.; McBride, J.; Rice, P.; Goodman-Capps, C.; Capps, C. Comparison of quadriceps and hamstring muscle activity during an isometric squat between strength-matched men and women. J. Sci. Med. Sport 2019, 18, 101–108. [Google Scholar]
- Ghasemi, A.; Zahediasl, S. Normality tests for statistical analysis: A guide for non-statisticians. Int. J. Endocrinol. Metab. 2012, 10, 486–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaminski, T.W.; Hartsell, H.D. Factors contributing to chronic ankle instability: A strength perspective. J. Athl. Train. 2002, 37, 394–405. [Google Scholar] [PubMed]
- Decker, M.J.; Torry, M.R.; Wyland, D.J.; Sterett, W.I.; Steadman, J.R. Gender differences in lower extremity kinematics, kinetics and energy absorption during landing. Clin. Biomech. 2003, 18, 662–669. [Google Scholar] [CrossRef]
- Lin, J.Z.; Lin, Y.A.; Lee, H.J. Are landing biomechanics altered in elite athletes with chronic ankle instability? J. Sports Sci. Med. 2019, 18, 653–662. [Google Scholar] [PubMed]
- Ward, R.E.; Yan, A.F.; Kremenic, L.J.; Orishimo, K.; Marshall, H. Comparison of lower limb stiffness between male and female dancers and athletes during drop jump landings. Scand. J. Med. Sci. Sports 2018, 29, 71–81. [Google Scholar] [CrossRef]
- Sugimoto, D.; Kartsson, J.; Samuelsson, K.; Myer, G. Biomechanical and neuromuscular characteristics of male athletes: Implications for the development of anterior cruciate ligament injury prevention programs. Sports Med. 2015, 45, 809–822. [Google Scholar] [CrossRef]
- Brookreson, N. The Relationship between Dorsiflexion Range of Motion and Knee Kinematics in a Land-And-Jump Task. Master’s Thesis, Eastern Washington University, Cheney, WA, USA, 2014. [Google Scholar]
- Bell-Jenje, T.; Olivier, B.; Wood, W.; Rogers, S.; Green, A.; McKinon, W. The association between loss of ankle dorsiflexion range of movement, and hip adduction and internal rotation during a step down test. Man. Ther. 2016, 21, 256–261. [Google Scholar] [CrossRef]
- Hankemeier, D.A.; Thrasher, A.B. Relationship between the weight-bearing lunge and nonweight-bearing dorsiflexion range of motion measures. Athl. Train. Sports Health Care 2014, 6, 128–134. [Google Scholar] [CrossRef]
- Cho, K.H.; Jeon, Y.; Lee, H. Range of motion of the ankle according to pushing force, gender and knee position. Ann. Rehabil. Med. 2016, 40, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Lam, W.K.; Cheung, C.H.; Leung, A.K.L. Effects of red arch-support insoles on subjective comfort and movement biomechanics in various landing heights. Int. J. Environ. Res. Public Health 2020, 17, 2476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohd Azhar, N.; Affandi, N.F.; Mail, M.S.Z.; Shaharudin, S. The effects of foot position on lower extremity kinematics during single leg squat among adolescent male athletes. J. Taibah Univ. Med. Sci. 2019, 14, 343–349. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Ankle Strength (Peak Torque/Body Weight) | Mean (SD) | p-Value | |
|---|---|---|---|
| Male (n = 15) | Female (n = 15) | ||
| Eversion | 113.40 (13.42) | 119.95 (13.07) | 0.77 |
| Inversion | 136.49 (21.51) | 114.41 (17.49) | 0.01 * |
| Strength ratio (Evertors: Invertors) | 0.85 (0.18) | 0.98 (0.21) | 0.08 |
| Plantarflexion | 373.62 (24.44) | 336.52 (24.44) | 0.02 * |
| Dorsiflexion | 150.35 (27.31) | 140.45 (24.27) | 0.30 |
| Strength ratio (Plantarflexors: Dorsiflexors) | 2.517 (0.30) | 2.45 (0.35) | 0.55 |
| Phases of Landing | Knee Angle (°) | p-Value | |
|---|---|---|---|
| Male (n = 15) | Female (n = 15) | ||
| At 30 cm Initial Contact | 1.56 (4.86) | −2.04 (4.09) | 0.05 * |
| Maximum vGRF | 1.85 (7.52) | −2.00 (5.19) | 0.11 |
| Maximum knee flexion | 3.45 (8.82) | −1.01 (7.08) | 0.14 |
| At 45 cm Initial Contact | 0.29 (4.20) | 0.60 (6.31) | 1.00 |
| Maximum vGRF | −0.17 (6.45) | 1.05 (7.09) | 0.70 |
| Maximum knee flexion | 2.23 (8.20) | 3.80 (6.93) | 0.37 |
| Weight-Bearing Ankle Dorsiflexion | 30 cm Landing Height | 45 cm Landing Height | |||||
|---|---|---|---|---|---|---|---|
| Value | IC | MV GRF | MKF | IC | MV GRF | MKF | |
| Males (n = 15) | |||||||
| Dorsiflexion range of motion (cm) | P | 0.14 | 0.25 | 0.46 | 0.15 | 0.47 | 0.16 |
| R | −0.30 | −0.19 | 0.03 | −0.28 | 0.02 | 0.28 | |
| Females (n = 15) | |||||||
| Dorsiflexion range of motion (cm) | P | 0.05 | 0.04 * | 0.05 | 0.35 | 0.20 | 0.14 |
| R | 0.44 | 0.46 | 0.43 | 0.11 | 0.24 | 0.29 | |
| Isokinetic Ankle Strength | Value | 30 cm Landing Height | 45 cm Landing Height | ||||
|---|---|---|---|---|---|---|---|
| IC | MV GRF | MKF | IC | MV GRF | MKF | ||
| Males (n = 15) | |||||||
| Evertors | P | 0.43 | 0.39 | 0.35 | 0.29 | 0.36 | 0.26 |
| R | −0.05 | 0.07 | 0.11 | 0.16 | 0.10 | 0.18 | |
| Invertors | P | 0.48 | 0.27 | 0.25 | 0.32 | 0.28 | 0.42 |
| R | 0.15 | 0.17 | 0.19 | 0.13 | 0.17 | 0.54 | |
| Plantarflexors | P | 0.12 | 0.03 * | 0.01 * | 0.27 | 0.05 * | 0.36 |
| R | −0.32 | −0.50 | −0.59 | −0.18 | −0.45 | −0.48 | |
| Dorsiflexors | P | 0.09 | 0.03 * | 0.05 * | 0.15 | 0.05 * | 0.09 |
| R | −3.59 | −0.50 | −0.28 | −0.28 | −0.45 | −0.36 | |
| Evertors: Invertors | P | 0.44 | 0.37 | 0.42 | 0.50 | 0.38 | 0.42 |
| R | −0.04 | −0.04 | −0.06 | −0.00 | −0.08 | 0.06 | |
| Plantarflexors: Dorsiflexors | P | 0.23 | 0.24 | 0.48 | 0.21 | 0.32 | 0.42 |
| R | 0.21 | 0.20 | −0.11 | 0.22 | 0.13 | −0.05 | |
| Females (n = 15) | |||||||
| Evertors | P | 0.39 | 0.49 | 0.43 | 0.31 | 0.50 | 0.40 |
| R | −0.08 | −0.01 | −0.05 | −0.14 | 0.01 | 0.07 | |
| Invertors | P | 0.17 | 0.06 | 0.02 * | 0.25 | 0.09 | 0.03 * |
| R | 0.27 | 0.43 | 0.53 | 0.19 | 0.36 | 0.50 | |
| Plantarflexors | P | 0.00 * | 0.02 * | 0.10 | 0.22 | 0.18 | 0.41 |
| R | 0.70 | 0.55 | 0.35 | −0.22 | −0.26 | −0.07 | |
| Dorsiflexors | P | 0.12 | 0.20 | 0.29 | 0.44 | 0.36 | 0.28 |
| R | −3.59 | 0.23 | 0.15 | −0.04 | −0.10 | 0.17 | |
| Evertors: Invertors | P | 0.21 | 0.10 | 0.03 * | 0.05 * | 0.04 * | 0.03 * |
| R | −0.23 | −0.35 | −0.51 | −0.44 | −0.48 | −0.51 | |
| Plantarflexors: Dorsiflexors | P | 0.48 | 0.47 | 0.48 | 0.42 | 0.48 | 0.20 |
| R | −0.01 | 0.02 | −0.01 | −0.06 | −0.01 | −0.23 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jamaludin, N.I.; Sahabuddin, F.N.A.; Raja Ahmad Najib, R.K.M.; Shamshul Bahari, M.L.H.; Shaharudin, S. Bottom-Up Kinetic Chain in Drop Landing among University Athletes with Normal Dynamic Knee Valgus. Int. J. Environ. Res. Public Health 2020, 17, 4418. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124418
Jamaludin NI, Sahabuddin FNA, Raja Ahmad Najib RKM, Shamshul Bahari MLH, Shaharudin S. Bottom-Up Kinetic Chain in Drop Landing among University Athletes with Normal Dynamic Knee Valgus. International Journal of Environmental Research and Public Health. 2020; 17(12):4418. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124418
Chicago/Turabian StyleJamaludin, Nazatul Izzati, Farhah Nadhirah Aiman Sahabuddin, Raja Khairul Mustaqim Raja Ahmad Najib, Muhamad Lutfi Hanif Shamshul Bahari, and Shazlin Shaharudin. 2020. "Bottom-Up Kinetic Chain in Drop Landing among University Athletes with Normal Dynamic Knee Valgus" International Journal of Environmental Research and Public Health 17, no. 12: 4418. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124418