An Exploratory Research of 18 Years on the Economic Burden of Diabetes for the Romanian National Health Insurance System

 , ,
, ,  , ,
, ,  , ,
, ,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Background
- Until 2003, the drugs could be purchased from some pharmacies (hospital or community), and the Romanian National Health Insurance House (RNHIH) discharged their costs without any compulsory reduction from the maximum price approved by the Ministry of Health.
- Between 2003 and 2007, the antidiabetic drugs were discharged by RNHIH, at a price established on base of the national bidding. In this period, only a few hospital pharmacies were included in NDP for supplying related drugs.
- During 2007-2011, the antidiabetic drugs could be acquired from community pharmacies. The cost discharged by the RNHIH must be reduced according to the negotiations organized by RNHIH.
- After 2012, antidiabetics can be purchased from community pharmacy, and RNHIH reimburses the total cost of these drugs, which is the maximum price of generics approved by the Ministry of Health.
1.2. Objectives
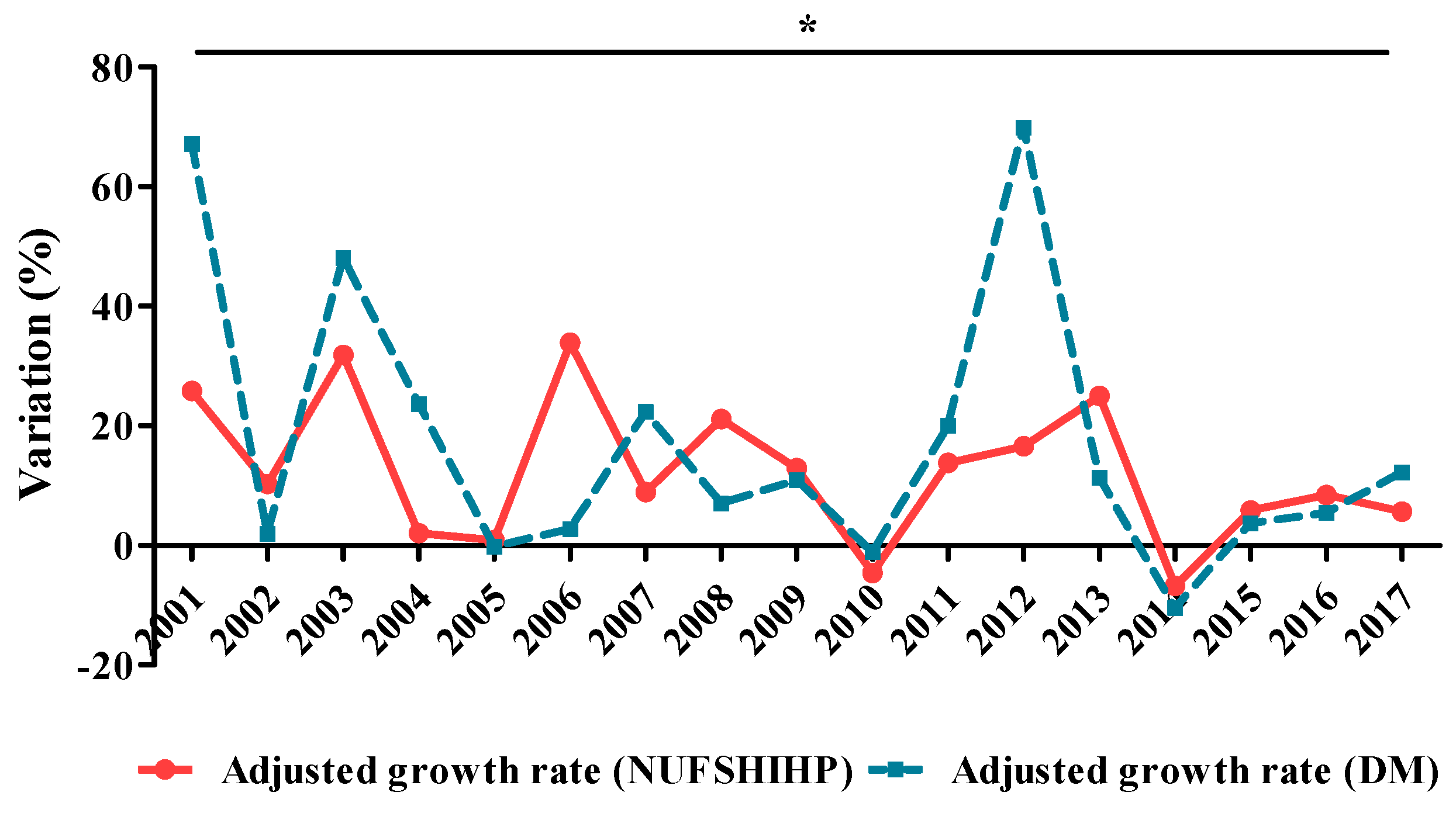
- Studying the diabetes mellitus funds (DMF) evolution as part of the total cost of National Health Programmes (NUFSHI HP);
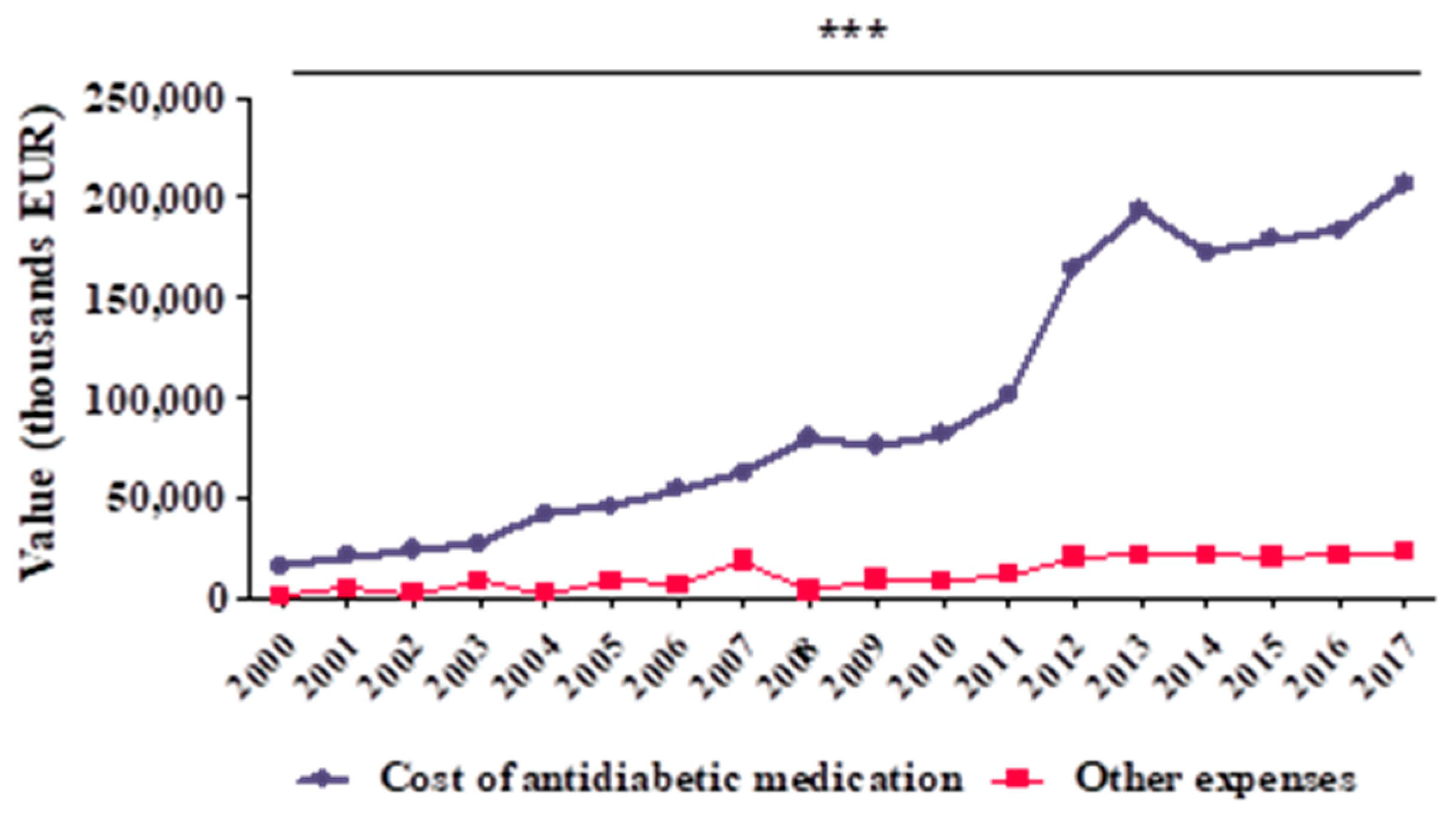
- Analysing the structure of DMF (medication and other expenses);
- Identifying the physical and efficiency indicators and their evolution over time;
- Identifying the possible correlations between these variables.
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Statistical Methods
3. Results
3.1. Outcome Data-Evolution of DMF in Romania during 2000–2017
3.2. Main Results—Physical Indicators
3.2.1. Number of Diabetic Patients
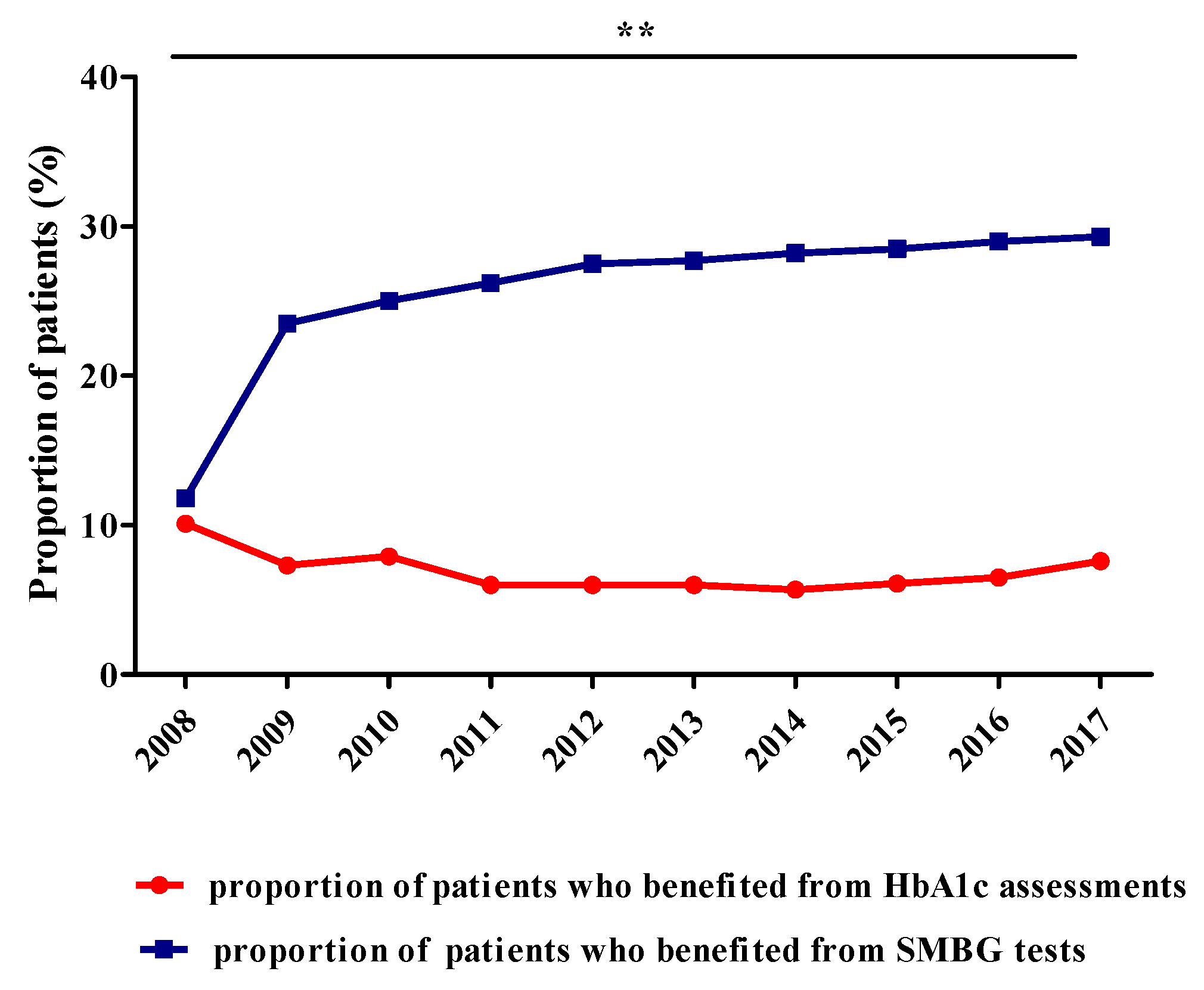
3.2.2. Number of Patients Who Benefited from HbA1c Assessments, SMBG Tests, Insulin Pumps or Supplies for Insulin Pumps
3.3. Main Results—Efficiency Indicators
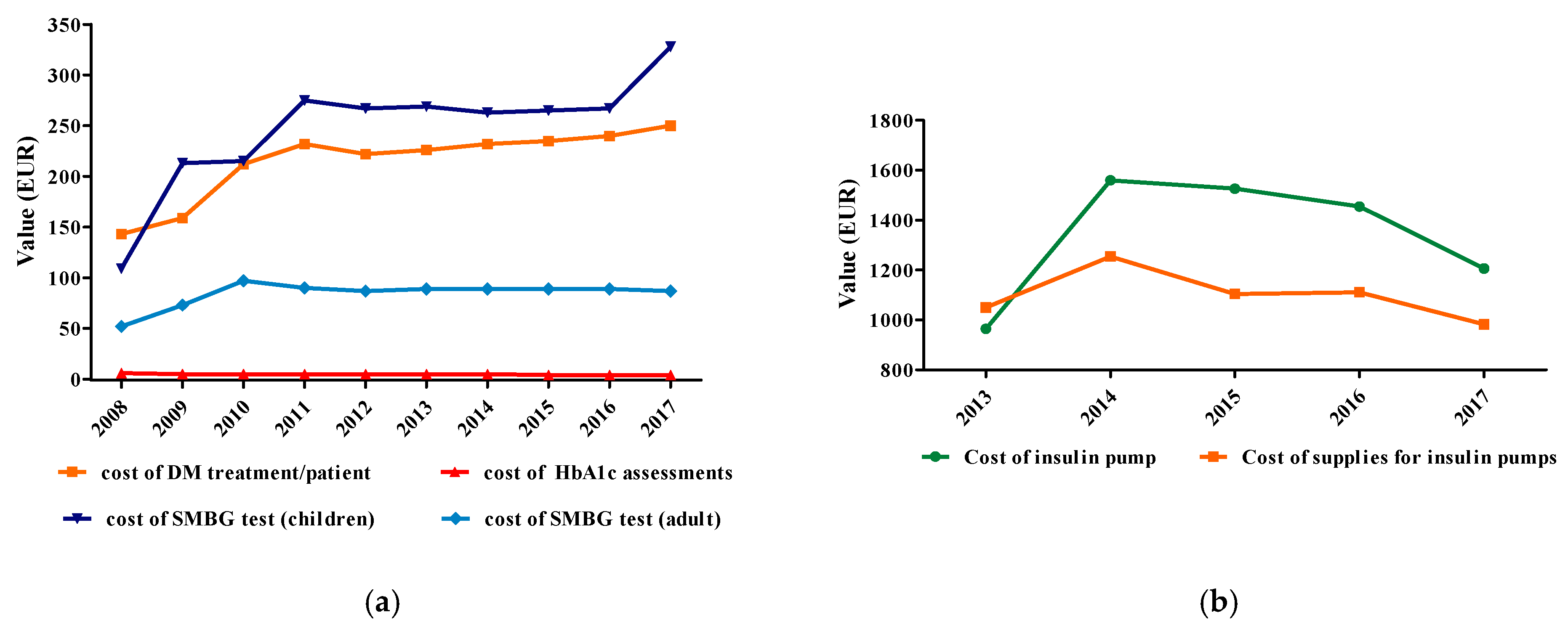
3.3.1. Cost of DM Treatment/Patient/Year
3.3.2. Cost of HbA1c Assessment
3.3.3. Cost of SMBG Test
3.3.4. Cost of Insulin Pumps/Patient and Cost of Supplies for Insulin Pumps/Patient/Year
3.4. Other Analyses-Association between DMF (EUR) and Other Indicators
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| DM | Diabetes mellitus |
| DMF | Diabetes mellitus fund |
| DPP-4 | Dipeptidyl peptidase-4 |
| GLP-1 | Glucagon-like peptide-1 |
| HbA1c | Glycated haemoglobin |
| IDF | International Diabetes Federation |
| NDP | National Diabetes Program |
| NUFSHI HP | National Unique Fund of Social Health Insurance for Health Programmes |
| OADs | Oral antidiabetic drugs (including GLP-1 analogues) |
| RNHIH | Romanian National Health Insurance House |
| SGLT-2 | Sodium-glucose co-transporter-2 |
| SMBG | Self-monitoring blood glucose |
References
- International Diabetes Federation (IDF). The IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017; Available online: http://fmdiabetes.org/wp-content/uploads/2018/03/IDF-2017.pdf (accessed on 26 December 2019).
- International Diabetes Federation (IDF). The IDF Diabetes Atlas, 5th ed.; International Diabetes Federation: Brussels, Belgium, 2011; Available online: https://www.idf.org/e-library/epidemiology-research/diabetes-atlas/20-atlas-5th-edition.html (accessed on 27 December 2019).
- Ghibu, S.; Craciun, C.E.; Rusu, R.; Morgovan, C.; Mogosan, C.; Rochette, L.; Gal, A.F.; Dronca, M. Impact of Alpha-Lipoic Acid Chronic Discontinuous Treatment in Cardiometabolic Disorders and Oxidative Stress Induced by Fructose Intake in Rats. Antioxidants 2019, 8, 636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vergari, F.; Tibuzzi, A.; Basile, G. An overview of the functional food market: From marketing issues and commercial players to future demand from life in space. Adv. Exp. Med. Biol. 2010, 698, 308–321. [Google Scholar] [PubMed]
- Han, K.-T.; Cho, G.; Kim, E. Evaluation of the Association between Gestational Diabetes Mellitus at First Pregnancy and Cancer within 10 Years Postpartum Using National Health Insurance Data in South Korea. Int. J. Environ. Res. Pub. Health 2018, 15, 2646. [Google Scholar] [CrossRef] [Green Version]
- Quarti Machado Rosa, M.; dos Santos Rosa, R.; Correia, M.G.; Araujo, D.V.; Bahia, L.R.; Toscano, C.M. Disease and economic burden of hospitalizations attributable to diabetes mellitus and its complications: A nationwide study in Brazil. Int. J. Environ. Res. Pub. Health 2018, 15, 294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leese, B. Diabetes mellitus and the St Vincent Declaration. The economic implications. PharmacoEconomics 1995, 7, 292–307. [Google Scholar] [CrossRef]
- Morgovan, C.; Ghibu, S.; Bota, M.; Fleşeriu, C.; Cosma, S. Cost for diabetes mellitus care in Romania and the world in the interval 1998–2007. In Proceedings of the 5th WSEAS International Conference on Economy and Management Transformation (EMT’10), Timisoara, Romania, 24–26 October 2010; pp. 714–719. [Google Scholar]
- Wake, N.; Hisashige, A.; Katayama, T.; Kishikawa, H.; Ohkubo, Y.; Sakai, M.; Araki, E.; Shichiri, M. Cost-effectiveness of intensive insulin therapy for type 2 diabetes: A 10-year follow-up of the Kumamoto study. Diabetes Res. Clini. Pract. 2000, 48, 201–210. [Google Scholar] [CrossRef]
- Cefalu, W.T. Diabetes care to date: “The hits just keep on coming!”. Diabetes Care 2013, 36, 1801–1803. [Google Scholar] [CrossRef] [Green Version]
- Veresiu, I.A.; Hancu, N.; Roman, G. Insulin and Insulin-Therapy; Echinox: Cluj-Napoca, Romanian, 2004. [Google Scholar]
- Department of Health and Human Services (DHHS), National Diabetes Fact Sheet United States. CDS Diabetes. Available online: http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2005.pdf (accessed on 25 March 2016).
- American Diabetes Association Economic Costs of Diabetes in the U. Diabetes Care 2018, 41, 917–928.
- Public Health Agency of Canada. Diabetes in Canada, 2nd ed.; Public Health Agency of Canada: Ottawa, ON, Canada, 2002; Available online: http://www.phac-aspc.gc.ca/publicat/dic-dac2/pdf/dic-dac2_en.pdf (accessed on 12 December 2010).
- European Commission Health and Consumers Directorate-General (ECHCDG)—Public Health C2—Health Information. Estimates of Cost of Diabetes per Year in the European Union and in Other European Countries. Revised by SANCO.C2 in April 2012. 2012. Available online: https://ec.europa.eu/health//sites/health/files/major_chronic_diseases/docs/idf_cost_2011 (accessed on 26 April 2019).
- Daina, L.G.; Sabău, M.; Daina, C.M.; Neamțu, C.; Tit, D.M.; Buhaș, C.L.; Bungau, C.; Aleya, L.; Bungau, S. Improving performance of a pharmacy in a Romanian hospital through implementation of an internal management control system. Sci. Total Environ. 2019, 675, 51–61. [Google Scholar] [CrossRef]
- Barceló, A.; Aedo, C.; Rajpathak, S.; Robles, S. The cost of diabetes in Latin America and the Caribbean. Bull. World Health Org. 2003, 81, 19–27. [Google Scholar]
- Charbonnel, B.; Simon, D.; Dallongeville, J.; Burreau, I.; Dejager, S.; Levy-Bachelot, L.; Gourmelen, J.; Detournay, B. Direct Medical Cost of Type 2 Diabetes in France: An Insurance Claims Database Analysis. Pharmacoecon. Open 2018, 2, 209–219. [Google Scholar] [CrossRef]
- Hirtzlin, I.; Preaubert, N.; Poutignat, N.; Rumeau-Pichon, C. Le coût médical direct du diabète de type 2 en France. J. d’Écon. Méd. 2003, 21, 341–351. [Google Scholar]
- Kusnik-Joinville, O.; Weill, A.; Salanave, B.; Ricordeau, P.; Allemand, H. Diabète traité: Quelles évolutions entre 2000 et 2005? PratiqesOrg. Soins 2007, 38, 1–11. [Google Scholar]
- Marissal, J.P.; Sailly, J.C.; Fontaine, P.; Eschwege, E.; Triomphe, A.; Lebrun, T. Estimation des économies potentielles, sur 10 ans, d’une action de sensibilisation à la mise en place des recommandations de l’ANAES dans la prise en charge du diabète de type 2 en région Ile-de-France. J. d’Écon. Méd. 2003, 21, 259–279. [Google Scholar]
- Colombo, G.L.; Rossi, E.; De Rosa, M.; Benedetto, D.; Gaddi, A.V. Antidiabetic therapy in real practice: Indicators for adherence and treatment cost. Patient Prefer. Adher. 2012, 6, 653–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission Health and Consumers Directorate-General (ECHCDG). Estimates of cost of Diabetes Per Year in the European Union. Available online: http://ec.europa.eu/health/major_chronic_diseases/docs/estimate_costs_diabete_en.pdf (accessed on 26 April 2018).
- Ministry of Public Health: Annexe 3/26: Summary of Funds Allocated by Sources and Expenditure Titles (in Romanian). Available online: http://www.cdep.ro/proiecte/2007/600/50/8/tit26.pdf (accessed on 7 April 2018).
- Spiru, L.; Traşcu, R.I.; Turcu, I.; Mǎrzan, M. Perpetual transitions in Romanian healthcare. EPMA J. 2011, 2, 341–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romanian National Health Insurance House (RNHIH) Activity Reports: 2007–2017. (In Romanian). Available online: http://www.cnas.ro/page/rapoarte-de-activitate.html (accessed on 7 June 2019).
- Ministry of Public Health. Evaluation Report of National Health Programs in 2007. Available online: http://www.ms.gov.ro/.../15_51_542_raport%20evaluare_pns_2007.doc (accessed on 12 December 2018).
- Romanian National Health Insurance House Activity Reports: 1999-2007. (In Romanian). Available online: http://www.cnas.ro/?id=126 (accessed on 2 July 2010).
- Morgovan, C.; Cosma, S.; Burta, C.; Ghibu, S.; Polinicencu, C.; Vasilescu, D. Measures to reduce the effects of the economic and financial crisis in pharmaceutical companies. Farmacia 2010, 58, 400–407. [Google Scholar]
- Morgovan, C.; Cosma, S.; Ghibu, S.; Burta, C.; Bota, M.; Polinicencu, C. Study of diabetes mellitus care cost in Romania during 2000–2008. Fund. Clin. Pharmacol. 2010, 24, 92. [Google Scholar]
- Morgovan, C.; Cosma, S.; Polinicencu, C.; Burta, C.; Ghibu, S. Comparative study regarding commercial policies for the Romanian antidiabetics’ market. Farmacia 2011, 59, 679–689. [Google Scholar]
- Joint Order of Ministry of Public Health and President of National House Insurance House no. 1061/425/ 2006 regarding the approval of the organization and conduct of the National Diabetes Program (in Romanian), Official Journal of Romania, part I, no. 803. 2006. Available online: https://lege5.ro/Gratuit/geydcmrwg4/ordinul-nr-1061-2006-privind-aprobarea-organizarii-si-desfasurarii-programului-national-de-diabet-zaharat (accessed on 12 December 2018).
- Morgovan, C.; Ghibu, S.; Maria Juncan, A.; Liviu Rus, L.; Butucă, A.; Vonica, L.; Muntean, A.; Moş, L.; Gligor, F.; Olah, N. Nutrivigilance: A new activity in the field of dietary supplements. Farmacia 2019, 67, 537–544. [Google Scholar] [CrossRef]
- Order no 245/2017 of the President of the National Health Insurance House Approving Technical Rules for Implementing the Curative National Health Programmes for 2017 and 2018. 2017.
- INS CPI-Annual Data Series. Available online: http://www.insse.ro/cms/ro/content/ipc–serie-de-date-anuala (accessed on 21 June 2020).
- National Bank of Romania—Exchange Rates: Montly, Quartely and Annual Averages. Available online: https://www.bnr.ro/Exchange-Rates--3727.aspx (accessed on 7 April 2018).
- Cosma, S. Marketing Research; Alma Mater: Cluj-Napoca, Romania, 2008. [Google Scholar]
- Cosma, S.; Vǎleanu, M.; Cosma, D.; Vasilescu, D.; Moldovan, G. Efficient data organisation in distributed computer systems using data warehouse. Int. J. Comput. Commun. Control 2013, 8, 366–374. [Google Scholar] [CrossRef] [Green Version]
- Vǎleanu, M.; Cosma, S.; Cosma, D.; Moldovan, G.; Vasilescu, D. Optimization for date redistributed system with applications. Int. J. Comput. Commun. Control 2009, 4, 178–184. [Google Scholar] [CrossRef] [Green Version]
- Cokolic, M.; Lalic, N.M.; Micic, D.; Mirosevic, G.; Klobucar Majanovic, S.; Lefterov, I.N.; Graur, M. Patterns of diabetes care in Slovenia, Croatia, Serbia, Bulgaria and Romania: An observational, non-interventional, cross-sectional study. Wien. Klin. Wochenschr. 2017, 129, 192–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pozo, L.; Bello, F.; Suarez, A.; Ochoa-Martinez, F.E.; Mendez, Y.; Chang, C.H.; Surani, S. Novel pharmacological therapy in type 2 diabetes mellitus with established cardiovascular disease: Current evidence. World J. Diabetes. 2019, 10, 291–303. [Google Scholar] [CrossRef]
- McEwen, L.N.; Casagrande, S.S.; Kuo, S.; Herman, W.H. Why Are Diabetes Medications So Expensive and What Can Be Done to Control Their Cost? Curr Diabetes Rep. 2017, 17, 71. [Google Scholar] [CrossRef]
- Pollard, D.J.; Brennan, A.; Dixon, S.; Waugh, N.; Elliott, J.; Heller, S.; Lee, E.; Campbell, M.; Basarir, H.; White, D.; et al. Cost-effectiveness of insulin pumps compared with multiple daily injections both provided with structured education for adults with type 1 diabetes: A health economic analysis of the Relative Effectiveness of Pumps over Structured Education (REPOSE) randomised controlled trial. BMJ Open 2018, 8, e016766. [Google Scholar]
- Egede, L.E.; Ellis, C. Diabetes and depression: Global perspectives. Diabetes Res. Clin. Pract. 2010, 87, 302–312. [Google Scholar] [CrossRef]
- Sortsø, C.; Green, A.; Jensen, P.B.; Emneus, M. Societal costs of diabetes mellitus in Denmark. Diabetic Medic. 2016, 33, 877–885. [Google Scholar] [CrossRef] [Green Version]
- Jönsson, B. Revealing the cost of Type II diabetes in Europe. Diabetologia 2002, 45, S5–S12. [Google Scholar] [CrossRef] [Green Version]
- de Lagasnerie, G.; Aguadé, A.S.; Denis, P.; Fagot-Campagna, A.; Gastaldi-Menager, C. The economic burden of diabetes to French national health insurance: A new cost-of-illness method based on a combined medicalized and incremental approach. Eur. J. Health Econ. 2018, 19, 189–201. [Google Scholar] [CrossRef] [Green Version]
- Rathmann, W.; Haastert, B.; Icks, A.; Giani, G. Trends in outpatient prescription drug costs in diabetic patients in Germany, 1994-2004. Diabetes Care 2007, 30, 848–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seuring, T.; Archangelidi, O.; Suhrcke, M. The Economic Costs of Type 2 Diabetes: A Global Systematic Review. PharmacoEconomics 2015, 33, 811–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afroz, A.; Alramadan, M.J.; Hossain, M.N.; Romero, L.; Alam, K.; Magliano, D.J.; Billah, B. Cost-of-illness of type 2 diabetes mellitus in low and lower-middle income countries: A systematic review. BMC Health Serv. Res. 2018, 18, 972. [Google Scholar] [CrossRef]
- Cosma, S.A.; Bota, M.; Fleșeriu, C.; Morgovan, C.; Văleanu, M.; Cosma, D. Measuring Patients’ Perception and Satisfaction with the Romanian Healthcare System. Sustainability 2020, 12, 1612. [Google Scholar] [CrossRef] [Green Version]
- Russo, P.; Rosano, G.M.C.; Favato, G.; Staniscia, T.; Romano, F. Cost-effectiveness of direct acting oral anticoagulants in the prevention of thromboembolic complications: Limits and concerns of economic evaluations. J. Cardiovasc. Medic. 2019, 20, 500–503. [Google Scholar] [CrossRef] [PubMed]
- Di Giovanni, P.; Scampoli, P.; Meo, F.; Cedrone, F.; D’Addezio, M.; Di Martino, G.; Valente, A.; Romano, F.; Staniscia, T. The impact of gender on diabetes-related lower extremity amputations: An Italian regional analysis on trends and predictors. Foot Ankle Surg. 2020. S1268-7731(20)30012-6. [Google Scholar] [CrossRef]
- Claessen, H.; Narres, M.; Haastert, B.; Arend, W.; Hoffmann, F.; Morbach, S.; Rümenapf, G.; Kvitkina, T.; Friedel, H.; Günster, C.; et al. Lower-extremity amputations in people with and without diabetes in Germany, 2008–2012—An analysis of more than 30 million inhabitants. Clin. Epid. 2018, 10, 475–488. [Google Scholar] [CrossRef] [Green Version]
- Bondor, C.I.; Veresiu, I.A.; Florea, B.; Vinik, E.J.; Vinik, A.I.; Gavan, N.A. Epidemiology of diabetic foot ulcers and amputations in Romania: Results of a cross-sectional quality of life questionnaire based survey. J. Diabetes Res. 2016, 2016, 5439521. [Google Scholar] [CrossRef] [Green Version]
- Veresiu, I.A.; Iancu, S.S.; Bondor, C. Trends in diabetes-related lower extremities amputations in Romania—A five year nationwide evaluation. Diabetes Res. Clin Pract. 2015, 109, 293–298. [Google Scholar] [CrossRef]
- Muntean, A.C.; Morgovan, C.; Cosma, S.; Butucă, A.; Juncan, A.M.; Rus, L.L.; Vonica, L.A.; Gligor, F.G.; Ghibu, S. Study of life quality and treatment satisfaction of Romanian diabetic patients. In Proceedings of the International Conference on Innovations in Science and Education, Prague, Czech Republic, 24–26 March 2019; pp. 771–777. Available online: https://ojs.journals.cz/index.php/CBUIC/article/view/1453/1979 (accessed on 6 June 2020).
- National Institute of Public Health (Romania). Available online: https://insp.gov.ro/sites/cnepss/resurse-imc-diabetul-zaharat/ (accessed on 4 June 2020).
- Romanian Society of Diabetes, Nutrition and Metabolic Diseases. Available online: http://www.srdnbm.ro/pdf/Proiect-de-activitate-GL-Eidemiologie3.pdf (accessed on 4 June 2020).
- Mota, M.; Popa, S.G.; Mota, E.; Mitrea, A.; Ctrinoiu, D.; Cheta, D.M.; Guja, C.; Hancu, N.; Ionescu-Targoviste, I.; Lichiardopol, R.; et al. Prevalence of diabetes mellitus and prediabetes in the adult Romanian population: PREDATORR study. J. Diabetes 2016, 8, 336–344. [Google Scholar] [CrossRef]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morgovan, C.; Cosma, S.A.; Valeanu, M.; Juncan, A.M.; Rus, L.L.; Gligor, F.G.; Butuca, A.; Tit, D.M.; Bungau, S.; Ghibu, S. An Exploratory Research of 18 Years on the Economic Burden of Diabetes for the Romanian National Health Insurance System. Int. J. Environ. Res. Public Health 2020, 17, 4456. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124456
Morgovan C, Cosma SA, Valeanu M, Juncan AM, Rus LL, Gligor FG, Butuca A, Tit DM, Bungau S, Ghibu S. An Exploratory Research of 18 Years on the Economic Burden of Diabetes for the Romanian National Health Insurance System. International Journal of Environmental Research and Public Health. 2020; 17(12):4456. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124456
Chicago/Turabian StyleMorgovan, Claudiu, Smaranda Adina Cosma, Madalina Valeanu, Anca Maria Juncan, Luca Liviu Rus, Felicia Gabriela Gligor, Anca Butuca, Delia Mirela Tit, Simona Bungau, and Steliana Ghibu. 2020. "An Exploratory Research of 18 Years on the Economic Burden of Diabetes for the Romanian National Health Insurance System" International Journal of Environmental Research and Public Health 17, no. 12: 4456. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124456