The Impact of Internet Usage and Knowledge-Intensive Activities on Households’ Healthcare Expenditures

 , ,
, ,
Abstract
:1. Introduction
2. Context Description
2.1. Health Population
2.2. The Internet, Health Information and Knowledge-Intensive Activities
- (1)
- (2)
- (3)
- (1)
- Internet access of households is influencing in a positive manner the internet usage and the Knowledge intensive activities.
- (2)
- Internet usage is influencing in a positive manner both the search for healthcare information on the internet and also the knowledge intensive activities.
- (3)
- Internet search for healthcare is affecting the spending of households on healthcare.
3. Materials and Methods
- Internet access of households (IA): the statistics is presenting the use within househoulds of Information and Communication Technologies at European level. Data for this collection are supplied directly from the surveys with no separate treatment, presenting the access to and use of ICTs by individuals and/or in households and the use of the Internet and other electronic networks for different purposes by individuals and/or in households;
- Individuals frequently using the internet (IU): the statistics is presenting the access to and use of ICTs by individuals in order to measure the access to selected IC technologies, the use of computers, location, frequency of use, activities (data collected at individual level), the use of the Internet (data collected at individual level), internet commerce (data collected at individual level), e-skills;
- Individuals searching on the internet for health-related information (HI): the statistics is presenting the percentage of individuals seeking Health-related information, such as: injury, disease, nutrition, improving health, etc. The data is collected taking into consideration the last three months before the survey.
- Payments made by households for healthcare (PHH): the statistics is presenting household payment’ means a direct payment for healthcare goods and services from the household primary income or savings, where the payment is made by the user at the time of the purchase of goods or the use of the services. The statistics is expressed as euro per inhabitants.
- Employment in knowledge-intensive activities (KI): the statistics is presenting employment in Knowledge Intensive Activities (KIA) identified based on a level of educated persons in sectors of economic activity. The data is covering EU Member States, EFTA and candidate countries are extracted and compiled from EU-Labour Force Survey for the population, using annual average data.
4. Results
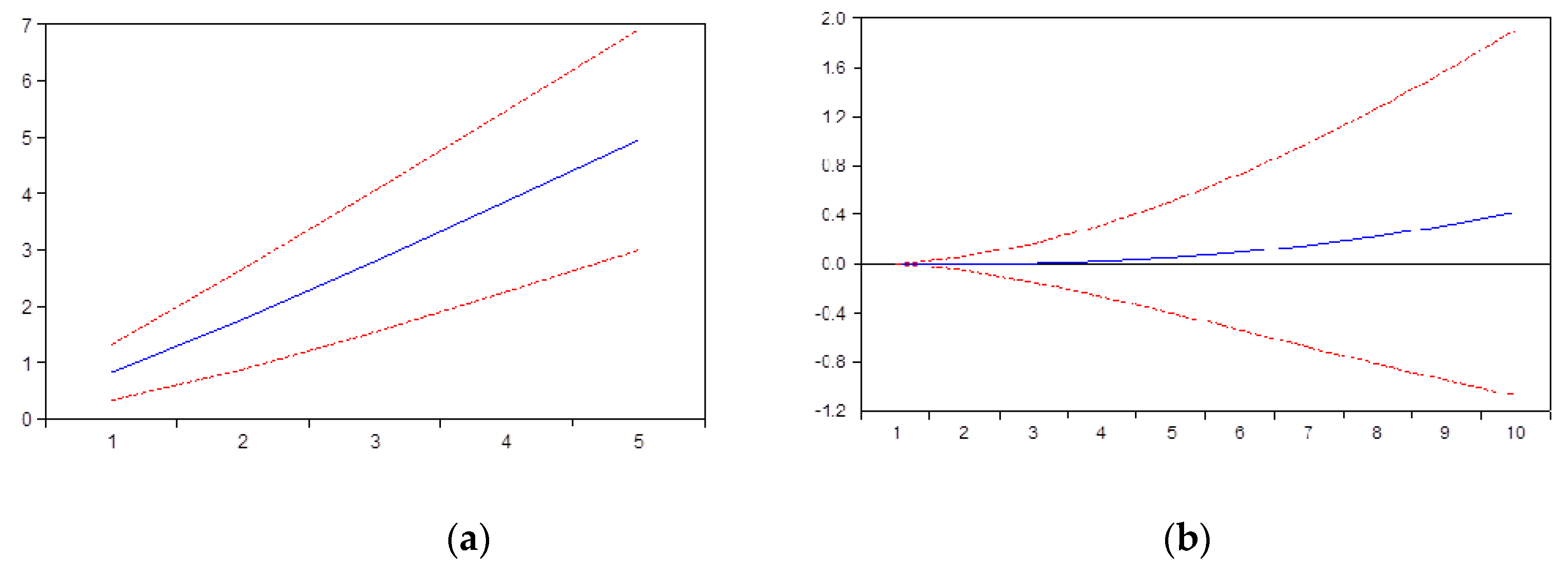
4.1. The Relationship between Internet Access and Internet Usage
4.2. The Relationship between Internet Usage and Internet Search for Seeking Health Related Information
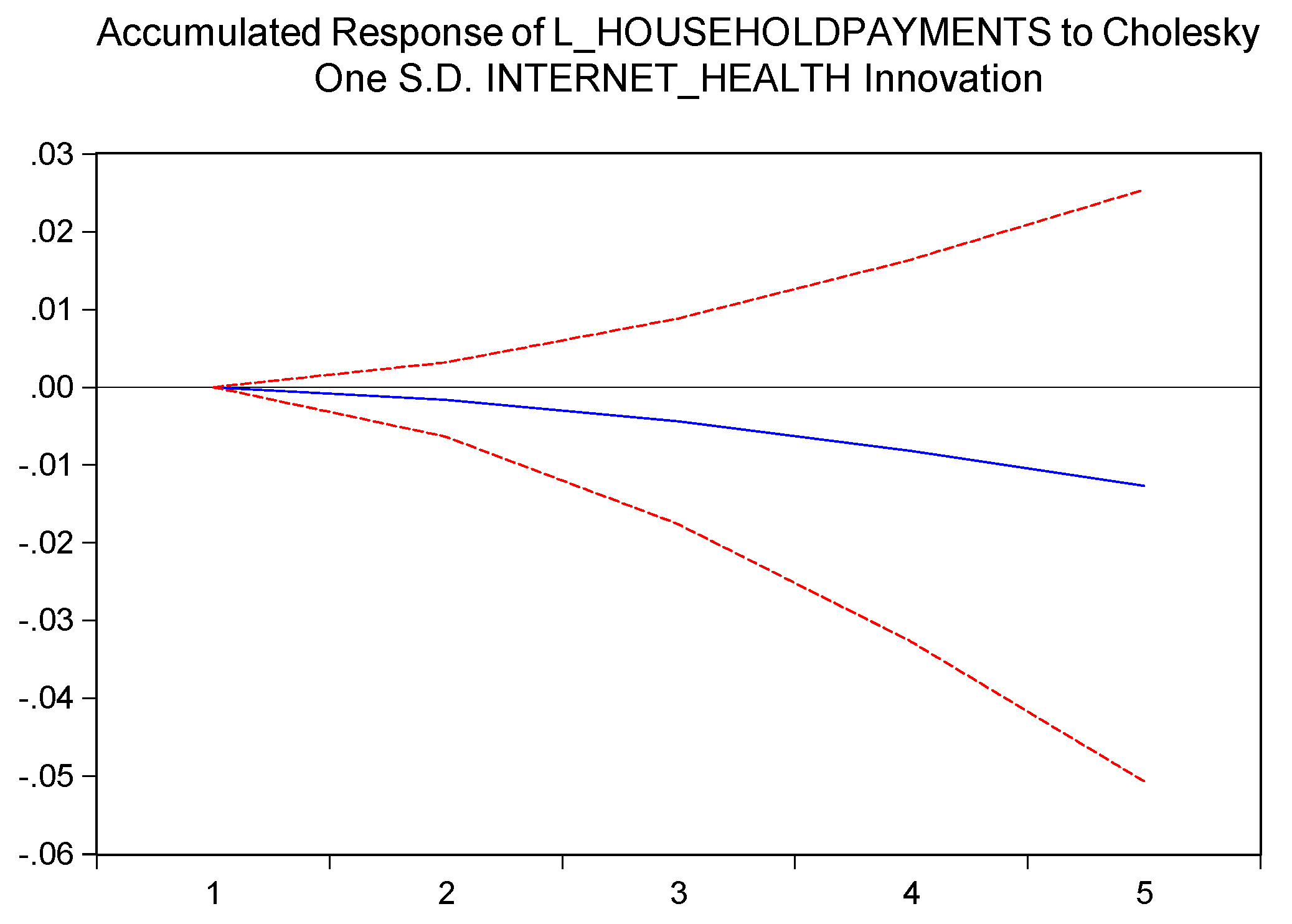
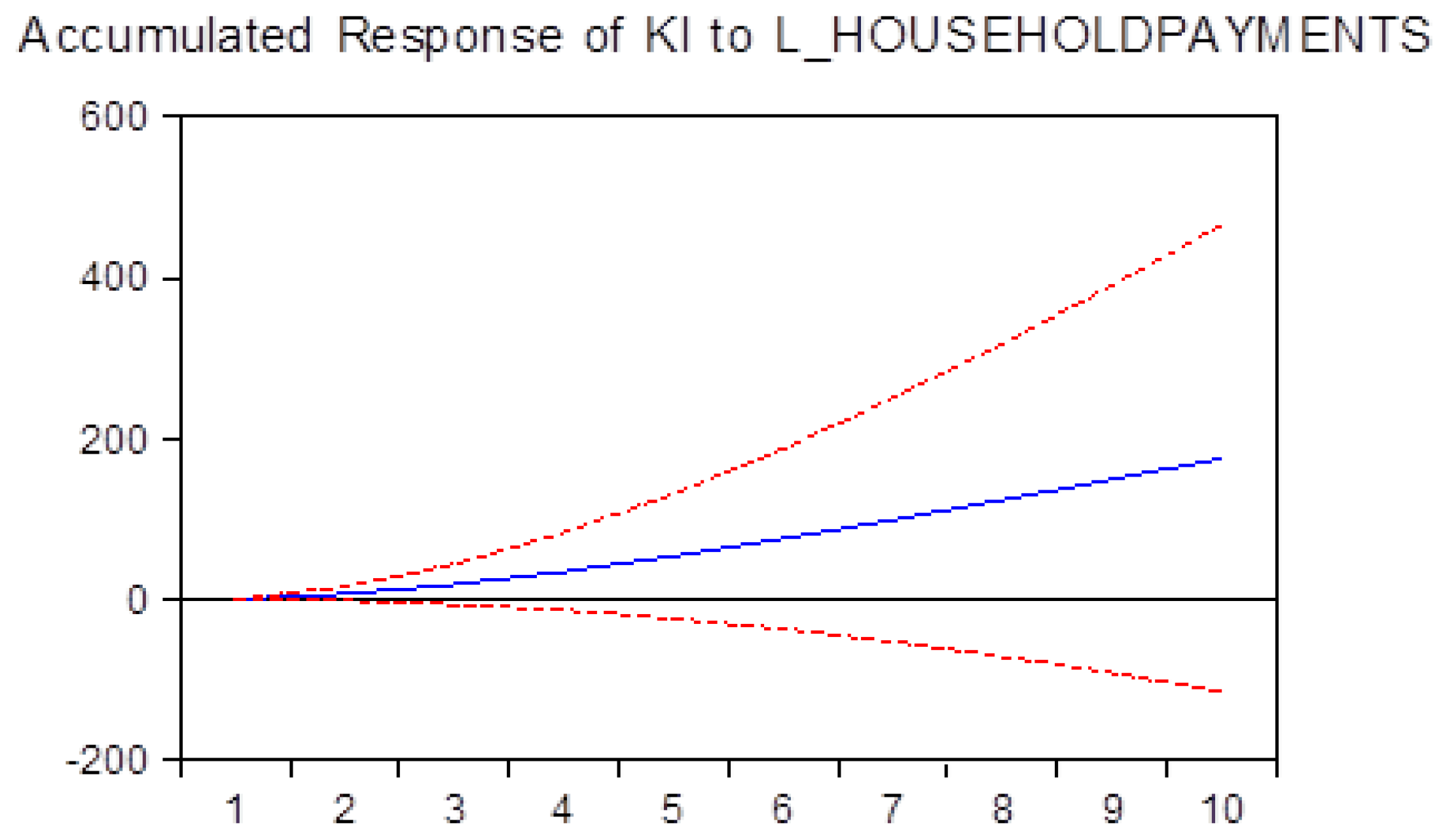
4.3. The Relationship between Using Internet for Health-Related Information and Payments Made by Households for Healthcare Expenses
5. Discussion
5.1. Research Implications
5.2. Practical Implications
5.3. Originality/Value
5.4. Future Research Opportunities
6. Conclusions
6.1. Search Limits
6.2. Future Research Opportunities
Author Contributions
Funding
Conflicts of Interest
References
- Commission of the European Communities. The Future Evolution of Social Protection from a Long-Term Point of View: Safe and Sustainable Pensions; Commission of the European Communities: Brussels, Belgium, 2000; p. 20. [Google Scholar]
- Organization, W.H. Active Ageing—A Policy Framework; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Commission of the European Communities. Green Paper “Confronting Demographic Change: A New Solidarity between the Generations”; Commission of the European Communities: Brussels, Belgium, 2005; p. 27. [Google Scholar]
- Organization, W.H. Changing History; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Börsch-supan, A.; Brugiavini, A.; Jürges, H.; Mackenbach, J.; Siegrist, J.; Weber, G. Health, Ageing and Retirement in Europe; GmbH, S., Ed.; Mannheim Research Institute for the Economics of Aging (MEA): Mannheim, Germany, 2005; pp. 81–161. [Google Scholar]
- WHO. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020. In MEO Design & Communication; Rossinière, S., Ed.; WHO Document Production Services: Geneva, Switzerland, 2013. [Google Scholar]
- EU. Cost of Non-Communicable Diseases in the EU; European Commission: Brussels, Belgium, 2020; Available online: https://ec.europa.eu/jrc/en/health-knowledge-gateway/societal-impacts/costs (accessed on 7 February 2020).
- OECD/EU. Health at a Glance: Europe 2018—State of Health in the EU Cycle; OECD Publishing: Paris, France, 2018. [Google Scholar] [CrossRef]
- Giovagnoli, M.R.; Bonifacino, A.; Neglia, C.; Benvenuto, M.; Sambati, F.V.; Giolli, L.; Giovagnoli, A.; Piscitelli, P. Diagnostic and Therapeutic Path of Breast Cancer: Effectiveness, Appropriateness, and Costs—Results from the DOCMa Study. Clin. Interv. Aging 2015, 10, 741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benvenuto, M.; Viola, C.; Sambati, F. A New Social and Technological Paradigm to Assess Chronic Patient Management Process: Preliminary Results. Manag. Stud. 2017, 5, 525–540. [Google Scholar] [CrossRef] [Green Version]
- European Commission. The 2014 EU Summit on Chronic Diseases Brussels, 3 and 4 April 2014; European Commission: Brussels, Belgium, 2014; pp. 1–4. [Google Scholar]
- European Heart Network. European Cardiovascular Disease Statistics 2017 Edition; European Heart Network: Brussels, Belgium, 2017. [Google Scholar]
- Murakami, Y.; Morgan, D. Expenditure by Disease, Age and Gender; OECD: Paris, France, 2016; Available online: https://www.oecd.org/health/Expenditure-by-disease-age-and-gender-FOCUS-April2016.pdf (accessed on 7 February 2020).
- Gravili, G.; Benvenuto, M.; Avram, A.; Viola, C. The Influence of the Digital Divide on Big Data Generation within Supply Chain Management. Int. J. Logist. Manag. 2018, 29, 592–628. [Google Scholar] [CrossRef]
- Internet World Stats. Internet Usage Statistics, Miniwatts Marketing Group. 2020. Available online: https://www.internetworldstats.com/stats.htm (accessed on 7 February 2020).
- International Telecommunication Union. Core List of Ict Indicators; International Telecommunication Union: Geneva, Switzerland, 2016; pp. 1–34. Available online: https://www.itu.int/en/ITU-D/Statistics/Documents/coreindicators/Core-List-of-Indicators_March2016.pdf (accessed on 7 February 2020).
- International Telecommunication Union. Measuring the Information Society Report; International Telecommunication Union: Geneva, Switzerland, 2018; Volume 1. [Google Scholar]
- Benvenuto, M.; Sambati, F.V.; Viola, C. The Impact of Internet Usage on Health-Care Expenditures and Sustainability. In Proceedings of the 5th International Scientific Conference ERAZ—Knowledge Based Sustainable Development, Budapest, Hungary, 23 May 2019; pp. 95–107. [Google Scholar] [CrossRef] [Green Version]
- Norris, P. Digital Divide; Cambridge University Press: Cambridge, UK, 2001. [Google Scholar] [CrossRef]
- Ryder, M.; Brent, W. Affordances and Constraints of the Internet for Learning and Instruction. Proceedings of Selected Research and Development Presentations at the 1996 National Convention of the Association for Educational Communications and Technology, Indianapolis, IN, USA, 14–18 February 1996; Volume 1, pp. 1–14. [Google Scholar]
- DiMaggio, P.; Hargittai, E.; Celeste, C.; Shafer, S. Digital Inequality: From Unequal Access to Differentiated Use. In Social Inequality; Kathryn, N., Ed.; Russell Sage Foundation: New York, NY, USA, 2004; pp. 355–400. [Google Scholar]
- DiMaggio, P.; Hargittai, E.; Neuman, W.R.; Robinson, J.P. Social Implications of the Internet. Ann. Rev. Soc. 2001, 27, 307–336. [Google Scholar] [CrossRef] [Green Version]
- Whitaker, R. The End of Privacy: How Total Surveillance Is Becoming a Reality; The New Press: New York, NY, USA, 2000. [Google Scholar]
- Wilson, E.J. Closing the Digital Divide: An Initial Review. Briefing the President; Internet Policy Inst.: Washington, DC, USA, 2000. [Google Scholar]
- Cooper, J. The Digital Divide: The Special Case of Gender. J. Comput. Assist. Learn. 2006, 22, 320–334. [Google Scholar] [CrossRef]
- Ono, H.; Zavodny, M. Gender and the Internet *. Soc. Sci. Q. 2003, 84, 111–121. [Google Scholar] [CrossRef]
- Feng, Y.; Xie, W. Digital Divide 2.0: The Role of Social Networking Sites in Seeking Health Information Online from a Longitudinal Perspective. J. Health Commun. 2015, 20, 60–68. [Google Scholar] [CrossRef]
- Sato, A.; Costa-i-Font, J. Social Networking for Medical Information: A Digital Divide or a Trust Inquiry? Health Policy Technol. 2013, 2, 139–150. [Google Scholar] [CrossRef]
- Hallows, K.M. Health Information Literacy and the Elderly: Has the Internet Had an Impact? Ser. Libr. 2013, 65, 39–55. [Google Scholar] [CrossRef]
- Shah, C.; Marchionini, G. Awareness in CIS. Int. Rev. Res. Open Distance Learn. 2013, 14, 90–103. [Google Scholar] [CrossRef]
- Organisation for Economic Co-operation and Development. Innovation and Knowledge-Intensive Service Activities; OECD: Paris, France, 2006; Volume 9789264022. [Google Scholar] [CrossRef]
- Eurostat. High-Tech Statistics-Employment Statistics Explained. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=High-tech_statistics_-_employment&oldid=443530 (accessed on 18 February 2020).
- Madsen, H.; Neergaard, H.; Ulhøi, J.P. Knowledge-Intensive Entrepreneurship and Human Capital. J. Small Bus. Enterp. Dev. 2003, 10, 426–434. [Google Scholar] [CrossRef]
- Domenech, J.; Escamilla, R.; Roig-Tierno, N. Explaining Knowledge-Intensive Activities from a Regional Perspective. J. Bus. Res. 2016, 69, 1301–1306. [Google Scholar] [CrossRef]
- Avram, C.D. Some considerations relating to health management and occupational safety. Revista Economica; Sibiu, Romania, 2011; Volume 3, pp. 16–23. Available online: http://economice.ulbsibiu.ro/revista.economica/archive/RE%203-56-2011.pdf (accessed on 4 April 2020).
- Avram, C.D. The Balance between Flexibility and Security in the Labor Market in Romania. Ovidius Univ. Ann. Econ. Sci. Ser. 2013, 13, 415–418. Available online: http://stec.univ-ovidius.ro/html/anale/ENG/cuprins%20rezumate/volum2013p1.pdf (accessed on 5 April 2020).
- Avram, C.D.; Dan, R.L. Considerations Regarding the Role of Capital in the Financing Decision. Ann. Univ. Craiova-Econ. Sci. Ser. 2019, 2, 25–34. Available online: http://feaa.ucv.ro/annals/v2_2019/003.pdf (accessed on 2 April 2020).
- Dan, R.L.; Buglea, A.; Aniș, C. The main models of corporate governance. In Proceedings of the International Academic Conferences, Florence, Italy, 16–19 September 2015; International Institute of Social and Economic Sciences: Prague, Czech Republic, 2015. [Google Scholar] [CrossRef]
- Harvey, A. The Econometric Analysis of Time Series, 2nd ed.; The MIT Press: Cambridge, MA, USA, 1990. [Google Scholar]
- Canova, F.; Ciccarelli, M. Panel Vector Autoregressive Models a Surve; Working Paper Series, no. 1507; European Central Bank: Frankfurt, Germany, 2013. [Google Scholar]
- Luetkepohl, H. Helmut—Vector Autoregressive Models, EUI Working Paper; ECO: Florence, Italy, 2011; p. 6. [Google Scholar]
- World Health Organization. WHO Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clean Care Is Safer Care; Section 2, Patient Empowerment and Health Care; WHO Press: Geneva, Switzerland, 2009. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Root | Modulus |
|---|---|
| 0.985 | 0.985 |
| 0.920 | 0.920 |
| 0.908 | 0.908 |
| 0.810 − 0.012i | 0.810 |
| 0.810 + 0.012i | 0.810 |
| −0.211 | 0.211 |
| −0.129 | 0.129 |
| 0.101 | 0.101 |
| −0.031 − 0.082i | 0.088 |
| −0.031 + 0.082i | 0.088 |
| Lag | LogL | LR | FPE | AIC | SC | HQ |
|---|---|---|---|---|---|---|
| 0 | −1026.059 | NA | 2.64 × 1010 | 38.18 | 38.37 | 38.25 |
| 1 | −688.29 | 600.46 | 247,400.2 * | 26.60 | 27.70 * | 27.02 * |
| 2 | −671.48 | 26.76 | 343,363.9 | 26.90 | 28.93 | 27.68 |
| 3 | −654.45 | 23.97 | 491,056.5 | 27.20 | 30.14 | 28.33 |
| 4 | −621.81 | 39.89 * | 419,032.8 | 26.91 | 30.78 | 28.41 |
| 5 | −607.39 | 14.95 | 771,252.6 | 27.31 | 32.09 | 29.15 |
| 6 | −588.31 | 16.25 | 1,377,482.3 | 27.53 | 33.23 | 29.73 |
| 7 | −555.87 | 21.62 | 1,878,280.4 | 27.25 | 33.88 | 29.81 |
| 8 | −505.06 | 24.46 | 1,907,265.6 | 26.29 * | 33.84 | 29.21 |
| Lags | Q-Stat | Prob. | Adj Q-Stat | Prob. | df |
|---|---|---|---|---|---|
| 1 | 17.12 | NA * | 17.19 | NA * | NA * |
| 2 | 36.53 | 0.06 | 36.76 | 0.06 | 25 |
| Joint Test | ||
|---|---|---|
| Chi-sq | df | Prob. |
| 211.9654 | 150 | 0.0007 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benvenuto, M.; Avram, A.; Sambati, F.V.; Avram, M.; Viola, C. The Impact of Internet Usage and Knowledge-Intensive Activities on Households’ Healthcare Expenditures. Int. J. Environ. Res. Public Health 2020, 17, 4470. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124470
Benvenuto M, Avram A, Sambati FV, Avram M, Viola C. The Impact of Internet Usage and Knowledge-Intensive Activities on Households’ Healthcare Expenditures. International Journal of Environmental Research and Public Health. 2020; 17(12):4470. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124470
Chicago/Turabian StyleBenvenuto, Marco, Alexandru Avram, Francesco Vincenzo Sambati, Marioara Avram, and Carmine Viola. 2020. "The Impact of Internet Usage and Knowledge-Intensive Activities on Households’ Healthcare Expenditures" International Journal of Environmental Research and Public Health 17, no. 12: 4470. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124470