Functional and Clinical Characteristics for Predicting Sarcopenia in Institutionalised Older Adults: Identifying Tools for Clinical Screening

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
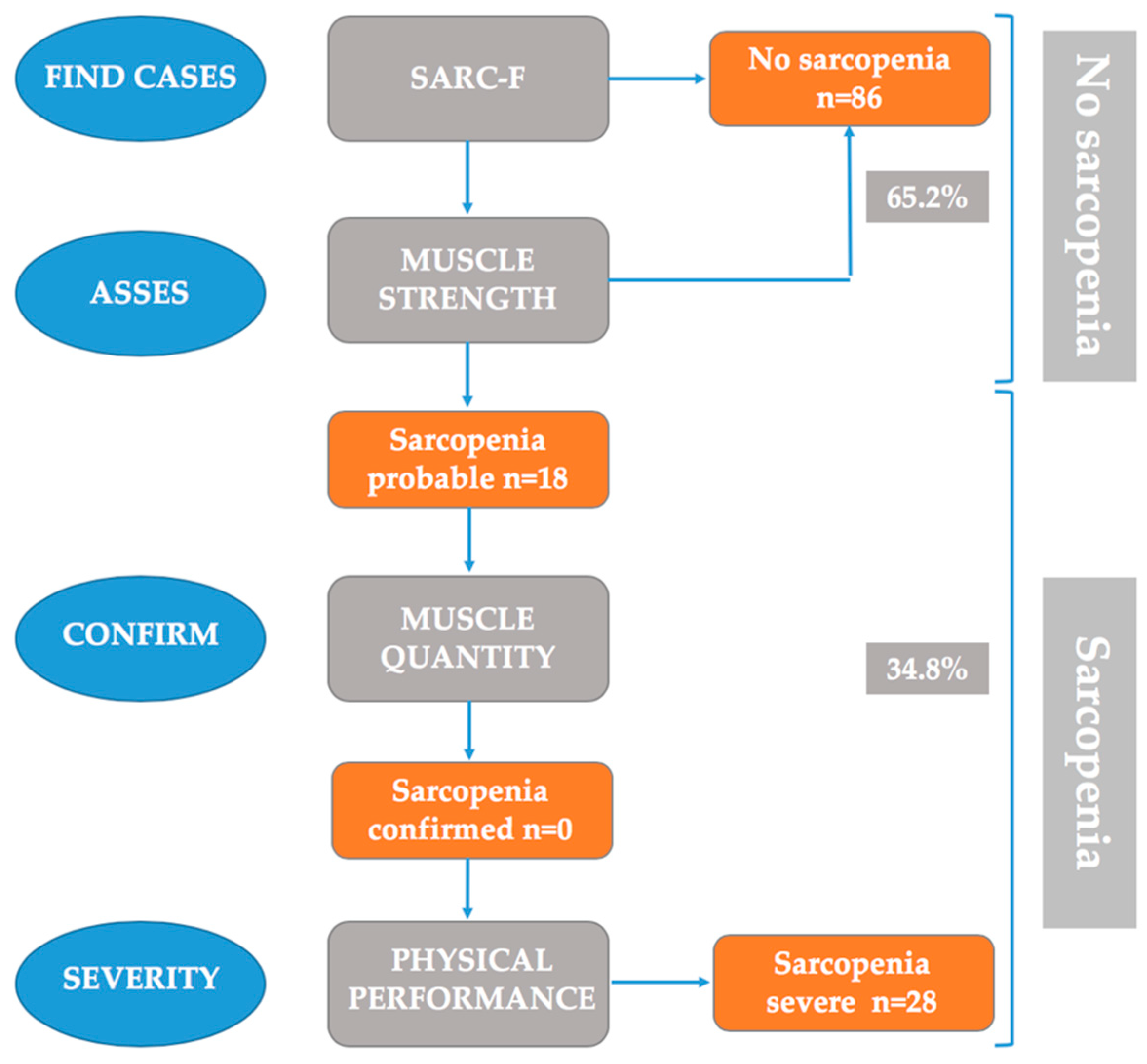
2.3. Sarcopenia Definition
2.4. Measurements
2.5. Sample Size Calculation
2.6. Statistical Analyses
3. Results
3.1. Sample Characteristics
3.2. Differences Based on EWSGOP2 Algorithm’s Application Regarding Study’s Variables
3.3. Derivation of the Regression Equation
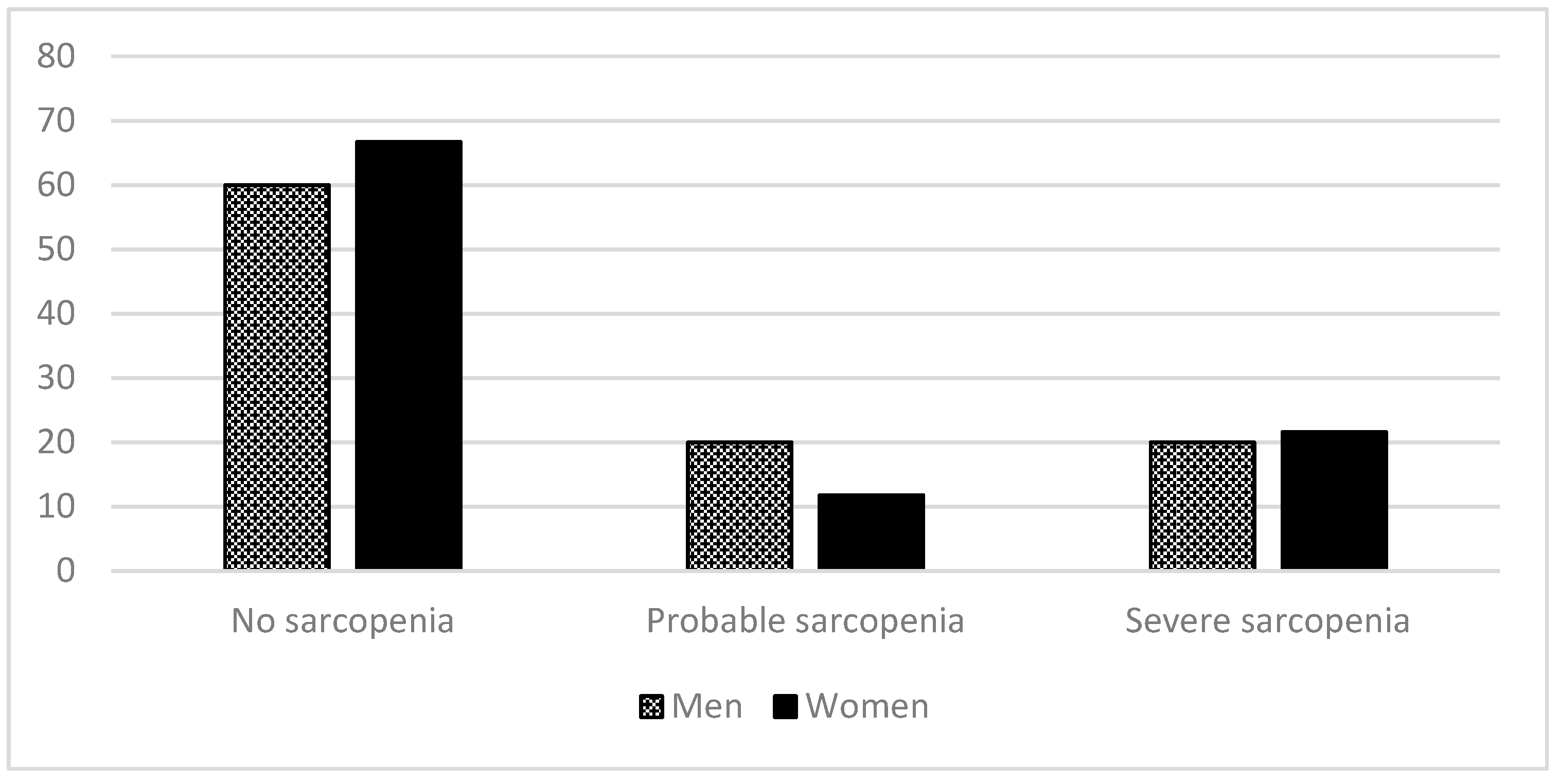
3.4. Prevalence of Sarcopenia by Gender and Age
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations, Department of Economic and Social Affairs. Population Division. World population prospects: The 2017 revision, Key findings and Advance Tables, 2017. Working Paper No. ESA/P/WP/248. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/WPP2017_KeyFindings.pdf (accessed on 24 April 2020).
- Bauer, J.M.; Kaise, M.J.; Sieber, C.C. Sarcopenia in nursing home residents. J. Am. Med. Dir. Assoc. 2008, 9, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zúñiga, C.; Arai, H.; Boirie, Y.; Chen, L.K.; Fielding, R.A.; Martin, F.C.; Michel, J.P.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Malafarina, V.; Uriz-Otano, F.; Gil-Guerrero, L. Nutritional assessment and treatment of sarcopenia. Rev. Esp. Geriatr. Gerontol. 2013, 48, 153–154. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. European Working Group on Sarcopenia in Older People. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–414. [Google Scholar] [CrossRef] [Green Version]
- Witham, M.D.; Stott, D.J. A new dawn for sarcopenia. Age Ageing 2019, 48, 2–3. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Lauretani, F.; Russo, C.R.; Bandinelli, S.; Cavazzini, C.; di Iorio, A.; Corsi, A.M.; Rantanen, T.; Guralnik, J.M.; Ferrucci, L. Age-associated changes in skeletal muscles and their effect on mobility: An operational diagnosis of sarcopenia. J. Appl. Physiol. 2003, 95, 1851e60. [Google Scholar] [CrossRef]
- Luppa, M.; Luck, T.; Weyerer, S.; König, H.H.; Brähler, E.; Riedel-Heller, S.G. Prediction of institutionalization in the elderly. A systematic review. Age Ageing 2010, 39, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Marzetti, E.; Calvani, R.; Tosato, M.; Cesari, M.; di Bari, M.; Cherubini, A.; Collamati, A.; d’Angelo, E.; Pahor, M.; Bernabei, R.; et al. Sarcopenia: An overview. Aging Clin. Exp. Res. 2017, 29, 11–17. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Cesari, M.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; Salini, S.; Sisto, A.; Picca, A.; et al. Sarcopenia: An overview on current definitions, diagnosis and treatment. Curr. Protein Pept. Sci. 2018, 19, 633–638. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Landi, F.; Topinková, E.; Michel, J.P. Understanding sarcopenia as a geriatric syndrome. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Silva, T.A.A.; Frisoli Junior, A.; Pinheiro, M.M.; Szejnfeld, V.L. Sarcopenia and aging: Etiological aspects and therapeutic options. Rev. Bras. Reumatol. 2006, 46, 391–397. [Google Scholar]
- Bahat, G.; Yilmaz, O.; Oren, M.M.; Karan, M.A.; Reginster, J.Y.; Bruyère, O.; Beaudart, C. Cross-cultural adaptation and validation of the SARC-F to assess sarcopenia: Methodological report from European Union Geriatric Medicine Society Sarcopenia Special Interest Group. Eur. Geriatr. Med. 2018, 9, 23–28. [Google Scholar] [CrossRef]
- Bravo-José, P.; Moreno, E.; Espert, M.; Romeu, M.; Martínez, P.; Navarro, C. Prevalence of sarcopenia and associated factors in institutionalised older adult patients. Clin. Nutr. ESPEN 2018, 27, 113–119. [Google Scholar] [CrossRef]
- Rodríguez-Rejón, A.I.; Artacho, R.; Puerta, A.; Zúñiga, A.; Ruiz-López, M.D. Diagnosis of sarcopenia in long-term care homes for the ederly: The sensitivity and specificity of two simplified algorithms with respect to the EWGSOP Consensus. J. Nutr. Health Aging 2018, 22, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Kurosawa, Y.; Hara, K.; Tohara, H.; Namiki, C.; Chantaramanee, A.; Nakane, A.; Nagakawa, K.; Yamaguchi, K.; Yoshimi, K.; Furuya, J.; et al. Calf circumference is a useful index for assessing dysphagia. Tohoku J. Exp. Med. 2019, 248, 201–208. [Google Scholar] [CrossRef] [Green Version]
- Tufan, A.; Bahat, G.; Ozkaya, H.; Taşcıoğlu, D.; Tufan, F.; Saka, B.; Akin, S.; Karan, M.A. Low skeletal muscle mass index is associated with function and nutritional status in residents in a Turkish nursing home. Aging Male 2016, 19, 182–186. [Google Scholar] [CrossRef]
- Shiraishi, A.; Yoshimura, Y.; Wakabayashi, H.; Tsuji, Y. Prevalence of stroke-related sarcopenia and its association with poor oral status in post-acute stroke patients: Implications for oral sarcopenia. Clin. Nutr. 2018, 37, 204–207. [Google Scholar] [CrossRef]
- Lobo, A.; Saz, P.; Marcos, G.; Día, J.L.; de la Cámara, C.; Ventura, T.; Morales Asín, F.; Pascual, L.F.; Montañés, J.A.; Aznar, S.; et al. Revalidación y normalización del Mini-Examen Cognoscitivo (primera versión en castellano del Mini-Mental Status Examination) en la población general geriátrica. Med. Clin. 1999, 112, 767–774. [Google Scholar]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: A symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J. Cachexia Sarcopenia Muscle 2016, 7, 28–36. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Benzeval, M.; Deary, I.J.; Dennison, E.M.; Der, G.; Gale, C.R.; Inskip, H.M.; Jagger, C.; et al. Grip strength across the life course: Normative data from twelve British studies. PLoS ONE 2014, 9, e113637. [Google Scholar] [CrossRef] [Green Version]
- Landi, F.; Liperoti, R.; Fusco, D.; Mastropaolo, S.; Quattrociocchi, D.; Proia, A.; Russo, A.; Bernabei, R.; Onder, G. Prevalence and Risk Factors of Sarcopenia Among Nursing Home Older Residents. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2012, 67, 48–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sergi, G.; de Rui, M.; Veronese, N.; Bolzetta, F.; Berton, L.; Carraro, G.; Bano, G.; Coin, A.; Manzato, E.; Perissinotto, E. Assessing appendicular skeletal muscle mass with bioelectrical impedance analysis in free-living Caucasian older adults. Clin. Nutr. 2015, 34, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Working group on functional outcome measures for clinical trials. Functional outcomes for clinical trials in frail older persons: Time to be moving. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 160–164. [Google Scholar] [CrossRef] [Green Version]
- Studenski, S.; Perera, S.; Patel, K. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Batzan, J.J.; Pérez del Molino, J.; Alarcón, T.; San Cristobal, E.; Izquierdo, G.; Manzarbeitia, J. Indice de Barthel: Instrumento válido para la valoración funcional de pacientes con enfermedad cerebrovascular. Rev. Esp. Geriatr. Gerontol. 1993, 28, 32–40. [Google Scholar]
- Madruga, F.; Castellote, F.J.; Serrano, F.; Pizarro, A.; Luengo, C.; Jiménez, E.F. Índice de Katz y escala de Barthel como indicadores de respuesta funcional en el anciano. Rev. Esp. Geriatr. Gerontol. 1992, 27, 130. [Google Scholar]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Berkman, L.F.; Leo-Summers, L.; Horwitz, R.I. Emotional support and survival after myocardial infarction. A prospective, population-based study of the elderly. Ann. Intern. Med. 1992, 117, 1003–1009. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Rejón, A.I.; Ruiz-López, M.D.; Artacho Martín-Lagos, R. Diagnóstico y prevalencia de sarcopenia en residencias de mayores: EWGSOP2 frente al EWGSOP1. Nutr. Hosp. 2019, 36, 1074–1080. [Google Scholar] [CrossRef] [Green Version]
- Woo, J.; Leung, J.; Morley, J.E. Validating the SARC-F: A suitable community screening tool for sarcopenia? JAMDA 2014, 15, 630–634. [Google Scholar] [CrossRef]
- Ida, S.; Murata, K.; Nakadachi, D.; Ishihara, Y.; Imataka, K.; Uchida, A.; Monguchi, K.; Kaneko, R.; Fujiwara, R.; Takahashi, H. Development of a Japanese version of the SARC-F for diabetic patients: An examination of reliability and validity. Aging Clin. Exp. Res. 2017, 29, 935–942. [Google Scholar] [CrossRef]
- Parra-Rodríguez, L.; Szlejf, C.; García-González, A.I.; Malmstrom, T.K.; Cruz-Arenas, E.; Rosas-Carrasco, O. Cross-cultural adaptation and validation of the Spanish-language version of the SARC-F to assess sarcopenia in Mexican community-dwelling older adults. J. Am. Med. Dir. Assoc. 2016, 17, 1142e1146. [Google Scholar] [CrossRef]
- Wu, T.Y.; Liaw, C.K.; Chen, F.C.; Kuo, K.L.; Chie, W.C.; Yang, R.S. Sarcopenia screened with SARC-F questionnaire is associated with quality of life and 4-year mortality. J. Am. Med. Dir. Assoc. 2016, 17, 1129e1135. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Peters, K.W.; Shardell, M.D.; McLean, R.R.; Dam, T.T.L.; Kenny, A.M.; Fragala, M.S.; Harris, T.B.; Kiel, D.P.; Guralnik, J.M.; et al. Cutpoints for low appendicular lean mass that identify older adults with clinically significant weakness. J Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 567–575. [Google Scholar] [CrossRef] [Green Version]
- Gould, H.; Brennan, S.L.; Kotowicz, M.A.; Nicholson, G.C.; Pasco, J.A. Total and appendicular lean mass reference ranges for Australian men and women: The geelong osteoporosis study. Calcif. Tissue Int. 2014, 94, 363–372. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- Frisoli, A.; Chaves, P.H.; McNeill Ingham, S.J.; Fried, L.P. Severe osteopenia and osteoporosis, sarcopenia, and frailty status in community-dwelling older women: Results from the women’s health and aging study (WHAS) II. Bone 2011, 48, 952–957. [Google Scholar] [CrossRef]
- Sanada, K.; Miyachi, M.; Tanimoto, M.; Yamamoto, K.; Murakami, H.; Okumura, S.; Gando, Y.; Suzuki, K.; Tabata, I.; Higuchi, M. A cross-sectional study of sarcopenia in Japanese men and women: Reference values and association with cardiovascular risk factors. Eur. J. App. Physiol. 2010, 110, 57–65. [Google Scholar] [CrossRef]
- Kim, K.M.; Jang, H.C.; Lim, S. Differences among skeletal muscle mass indices derived from height-, weight-, and body mass index-adjusted models in assessing sarcopenia. Korean J. Intern. Med. 2016, 31, 643–650. [Google Scholar] [CrossRef] [Green Version]
- Beaudart, C.; Rolland, Y.; Cruz-Jentoft, A.J.; Bauer, J.M.; Sieber, C.; Cooper, C.; Al-Daghri, N.; Araujo de Carvalho, I.; Bautmans, I.; Bernabei, R.; et al. Assessment of muscle function and physical performance in daily clinical practice. Calcif. Tissue Int. 2019, 105, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons Is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Liu, Y.; Zuo, Y.; Tang, H. Sarcopenia for predicting falls and hospitalization in community-dwelling older adults: EWGSOP versus EWGSOP2. Sci. Rep. 2019, 9, 17636. [Google Scholar] [CrossRef]
- Vieira, E.R.; Palmer, R.C.; Chaves, P.H. Prevention falls in older living in the community. BMJ 2016, 353, i1419. [Google Scholar] [CrossRef] [Green Version]
- Vellas, B.J.; Guigoz, Y.; Garry, P.J.; Albarede, J.L. (Eds.) The Mini Nutritional Assessment: MNA, 3rd ed.; Serdi Publishing: Paris, France, 1997. [Google Scholar]
- Rolfson, D.B.; Majumdar, S.R.; Tsuyuki, R.T.; Tahir, A.; Rockwood, K. Validity and reliability of the Edmonton Frail Scale. Age Ageing 2006, 35, 526–529. [Google Scholar] [CrossRef] [Green Version]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.Y.; Bruyère, O. Health outcomes of sarcopenia: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Rodríguez, D.; Marco, E.; Miralles, R.; Guillén-Solà, A.; Vázquez-Ibar, O.; Escalada, F.; Muniesa, J. Does gait speed contribute to sarcopenia case-finding in a postacute rehabilitation setting? Arch. Gerontol. Geriatr. 2015, 61, 176–181. [Google Scholar] [CrossRef]
- Landi, F.; Cruz-Jentoft, A.J.; Liperoti, R.; Russo, A.; Giovannini, A.; Tosato, M.; Capoluongo, E.; Bernabei, R.; Onder, G. Sarcopenia and mortality risk in frail older persons aged 80 years and older: Results from ilSIRENTE study. Age Ageing 2013, 42, 203–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Rejón, A.I.; Ruiz-López, M.D.; Wanden-Berghe, C.; Artacho, R. Prevalence and diagnosis of sarcopenia in residential facilities: A systematic review. Adv. Nutr. 2019, 10, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvà, A.; Serra-Rexach, J.A.; Artaza, I.; Formiga, F.; Rojano, I.; Luque, X.; Cuesta, F.; López-Soto, A.; Masanés, F.; Ruiz, D.; et al. Prevalence of sarcopenia in Spanish nursing homes: Comparison of the results of the ELLI study with other populations. Rev. Esp. Geriatr. Gerontol. 2016, 51, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Smoliner, C.; Sieber, C.C.; Wirth, R. Prevalence of sarcopenia in geriatric hospitalized patients. J. Am. Med. Dir. Assoc. 2014, 15, 267e72. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total (n = 132) | Men (n = 30) | Women (n = 102) | p-Value a |
|---|---|---|---|---|
| Anthropometrics | ||||
| Age (years) | 82.03 ± 8.25 | 78.70 ± 8.73 | 83.00 ± 7.88 | 0.11 |
| (80.61–83.45) | (75.44–81.96) | (81.46–84.56) | ||
| Weight (kg) | 66.66 ± 13.45 | 75.98 ± 12.60 | 63.92 ± 12.47 | <0.001 † |
| (64.34–68.97) | (71.28–80.69) | (61.47–66.37) | ||
| Height (cm) | 154.02 ± 9.08 | 165.05 ± 8.00 | 150.77 ± 6.46 | <0.001 † |
| (152.46–155.58) | (162.07–168.04) | (149.50–152.04) | ||
| BMI (kg/m2) | 28.06 ± 4.89 | 27.92 ± 3.83 | 28.10 ± 5.17 | 0.831 |
| (27.22–28.90) | (26.49–29.35) | (27.09–29.11) | ||
| EWSGOP2 algorithm | ||||
| SARC-F (0–10 score) | 3.95 ± 2.59 | 3.63 ± 2.77 | 4.04 ± 2.54 | 0.453 |
| (3.50–4.39) | (2.60–4.67) | (3.54–4.54) | ||
| Grip strength (kg) | 18.77 ± 7.82 | 26.85 ± 9.89 | 16.39 ± 5.10 | <0.001 † |
| (17.42–20.11) | (23.16–30.55) | (15.39–17.39) | ||
| ASM (kg) | 15.10 ± 3.48 | 19.63 ± 3.14 | 13.84 ± 2.33 | <0.001 † |
| (14.50–15.71) | (18.41–20.85) | (13.38–14.30) | ||
| ASMI (kg/m2) | 6.32 ± 0.98 | 7.20 ± 0.83 | 6.07 ± 0.87 | <0.001 † |
| (6.15–6.49) | (6.87–7.52) | (5.90–6.24) | ||
| Gait speed (m/s) | 0.56 ± 0.27 | 0.57 ± 0.29 | 0.56 ± 0.27 | 0.797 |
| (0.51–0.61) | (0.46–0.68) | (0.50–0.61) | ||
| SPPB (0–12 score) | 5.27 ± 2.99 | 6.17 ± 2.84 | 5.00 ± 2.99 | 0.06 |
| (4.75–5.78) | (5.11–7.23) | (4.41–5.59) | ||
| Study’s variables | ||||
| Barthel Index (0–100 score) | 77.95 ± 19.07 | 79.00 ± 22.87 | 77.65 ± 17.92 | 0.767 |
| (74.67–81.24) | (70.46–87.54) | (74.13–81.17) | ||
| Barthel Index classification | 0.064 | |||
| Independent (100) | 23 (17.4%) | 9 (30%) | 14 (13.8%) | |
| Mild dependence (91–99) | 11 (8.3%) | 3 (10%) | 8 (7.8%) | |
| Moderate dependence (61–90) | 76 (57.6%) | 11 (36.7%) | 65 (63.7%) | |
| Severe dependence (21–60) | 20 (15.2%) | 7 (23.3%) | 13 (12.7%) | |
| Total dependency (0–20) | 2 (1.5%) | 0 (0%) | 2 (2.0%) | |
| Abbreviated Charlson’s | 1.70 ± 1.33 | 2.27 ± 1.34 | 1.53 ± 1.29 | <0.01 * |
| Comorbidity Index (0–10) | (1.47–1.93) | (1.77–2.77) | (1.28–1.78) | |
| Modified abbreviated Charlson’s Comorbidity Index b | 0.027 * | |||
| No comorbidity | 66 (50%) | 10 (33.3%) | 56 (55.5%) | |
| Low comorbidity | 35 (26.5%) | 8 (26.7%) | 27 (26.7%) | |
| High comorbidity | 30 (22.7%) | 12 (40.0%) | 18 (17.8%) | |
| Medication (n) | 8.67 ± 4.37 | 9.00 ± 4.59 | 8.58 ± 4.32 | 0.644 |
| (7.92–9.43) | (7.29–10.71) | (7.73–9.43) | ||
| Hospitalisation stays (n) | 0.24 ± 0.59 | 0.23 ± 0.50 | 0.25 ± 0.62 | 0.924 |
| (0.14–0.34) | (0.05–0.42) | (0.12–0.37) | ||
| Falls (n) | 1.13 ± 2.08 | 0.93 ± 1.48 | 1.19 ± 2.22 | 0.56 |
| (0.77–1.49) | (0.38–1.49) | (0.75–1.62) | ||
| Modified falls (%) c | 0.773 | |||
| No falls | 65 (49.2%) | 15 (50%) | 50 (49%) | |
| 1–2 falls | 59 (44.7%) | 14 (46.7%) | 45 (44%) | |
| ≥3 falls | 8 (6.1%) | 1 (3.3%) | 7 (7%) |
| Variables | EWSOP2 Algorithm | Mean ± SD | F | df | df (error) | p-Value | η2 |
|---|---|---|---|---|---|---|---|
| Barthel Index (0–100 score) | NS | 83.26 ± 16.90 | 10.992 | 2 | 129 | <0.001 † | 0.146 |
| PS | 67.78 ± 18.96 | ||||||
| SS | 68.21 ± 19.54 | ||||||
| Abbreviated Charlson’s Comorbidity Index (0–10) | NS | 1.42 ± 1.30 | 6.054 | 2 | 129 | 0.003 † | 0.086 |
| PS | 2.06 ± 1.26 | ||||||
| SS | 2.32 ± 1.25 | ||||||
| Medication (n) | NS | 8.43 ± 4.57 | 0.561 | 2 | 129 | 0.572 | 0.009 |
| PS | 9.61 ± 4.07 | ||||||
| SS | 8.82 ± 3.94 | ||||||
| Hospitalisation stays (n) | NS | 0.17 ± 0.47 | 1.876 | 2 | 129 | 0.157 | 0.028 |
| PS | 0.44 ± 1.04 | ||||||
| SS | 0.32 ± 0.55 | ||||||
| Falls (n) | NS | 1.07 ± 2.39 | 0.44 | 2 | 129 | 0.65 | 0.007 |
| PS | 1.56 ± 1.72 | ||||||
| SS | 1.04 ± 1.0 |
| Variables | EWSOP2 | χ2 | df | p-Value | Cramer’s V | Kendall’s τ | ||
|---|---|---|---|---|---|---|---|---|
| Algorithm | ||||||||
| NS | PS | SS | ||||||
| Barthel Index classification | 23.941 | 8 | 0.003 † | 0.301 | −0.353 | |||
| Independent (100) | 22 | 1 | 0 | |||||
| Mild dependence (91–99) | 9 | 0 | 2 | |||||
| Moderate dependence (61–90) | 48 | 11 | 17 | |||||
| Severe dependence (21–60) | 6 | 6 | 8 | |||||
| Total dependency (0–20) | 1 | 0 | 1 | |||||
| Mod-Abb-Charlson-Index a | 12.86 | 4 | 0.014 * | 0.222 | 0.285 | |||
| No comorbidity | 52 | 6 | 8 | |||||
| Low comorbidity | 20 | 6 | 9 | |||||
| High comorbidity | 13 | 6 | 11 | |||||
| Modified falls b | 14.87 | 4 | 0.005 † | 0.237 | 0.244 | |||
| No falls | 52 | 5 | 8 | |||||
| 1–2 falls | 28 | 12 | 19 | |||||
| ≥3 falls | 6 | 1 | 1 | |||||
| Variables | B | SE | p | Odd-Ratio | 95% CI |
|---|---|---|---|---|---|
| Age | 0.101 | 0.03 | 0.001 | 1.16 | 1.04–1.17 |
| Barthel’s Index | −0.04 | 0.01 | 0.001 | 0.96 | 0.95–0.98 |
| Abbreviated Charlson’s Comorbility Index | 0.418 | 0.17 | 0.015 | 1.51 | 1.08–2.12 |
| Sarcopenia Subtypes | 65–74 Years | 75–84 Years | ≥85 Years | Total |
|---|---|---|---|---|
| No-sarcopenia (n = 86) | 24.4% (21) | 44.2% (38) | 31.4% (27) | 65.2% |
| Probable sarcopenia (n = 18) | 16.7% (3) | 16.7% (3) | 66.7% (12) | 13.6% |
| Confirmed sarcopenia (n = 0) | 0% | 0% | 0% | 0% |
| Severe sarcopenia (n = 28) | 3.6% (1) | 35.7% (10) | 60.7% (17) | 21.2% |
| n = 132 | 18.9% (25) | 38.6% (51) | 42.4% (56) | 100% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cebrià i Iranzo, M.A.; Arnal-Gómez, A.; Tortosa-Chuliá, M.A.; Balasch-Bernat, M.; Forcano, S.; Sentandreu-Mañó, T.; Tomas, J.M.; Cezón-Serrano, N. Functional and Clinical Characteristics for Predicting Sarcopenia in Institutionalised Older Adults: Identifying Tools for Clinical Screening. Int. J. Environ. Res. Public Health 2020, 17, 4483. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124483
Cebrià i Iranzo MA, Arnal-Gómez A, Tortosa-Chuliá MA, Balasch-Bernat M, Forcano S, Sentandreu-Mañó T, Tomas JM, Cezón-Serrano N. Functional and Clinical Characteristics for Predicting Sarcopenia in Institutionalised Older Adults: Identifying Tools for Clinical Screening. International Journal of Environmental Research and Public Health. 2020; 17(12):4483. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124483
Chicago/Turabian StyleCebrià i Iranzo, Maria A., Anna Arnal-Gómez, Maria A. Tortosa-Chuliá, Mercè Balasch-Bernat, Silvia Forcano, Trinidad Sentandreu-Mañó, Jose M. Tomas, and Natalia Cezón-Serrano. 2020. "Functional and Clinical Characteristics for Predicting Sarcopenia in Institutionalised Older Adults: Identifying Tools for Clinical Screening" International Journal of Environmental Research and Public Health 17, no. 12: 4483. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124483