Association between Surrounding Greenness and Mortality: An Ecological Study in Taiwan

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cause of Death
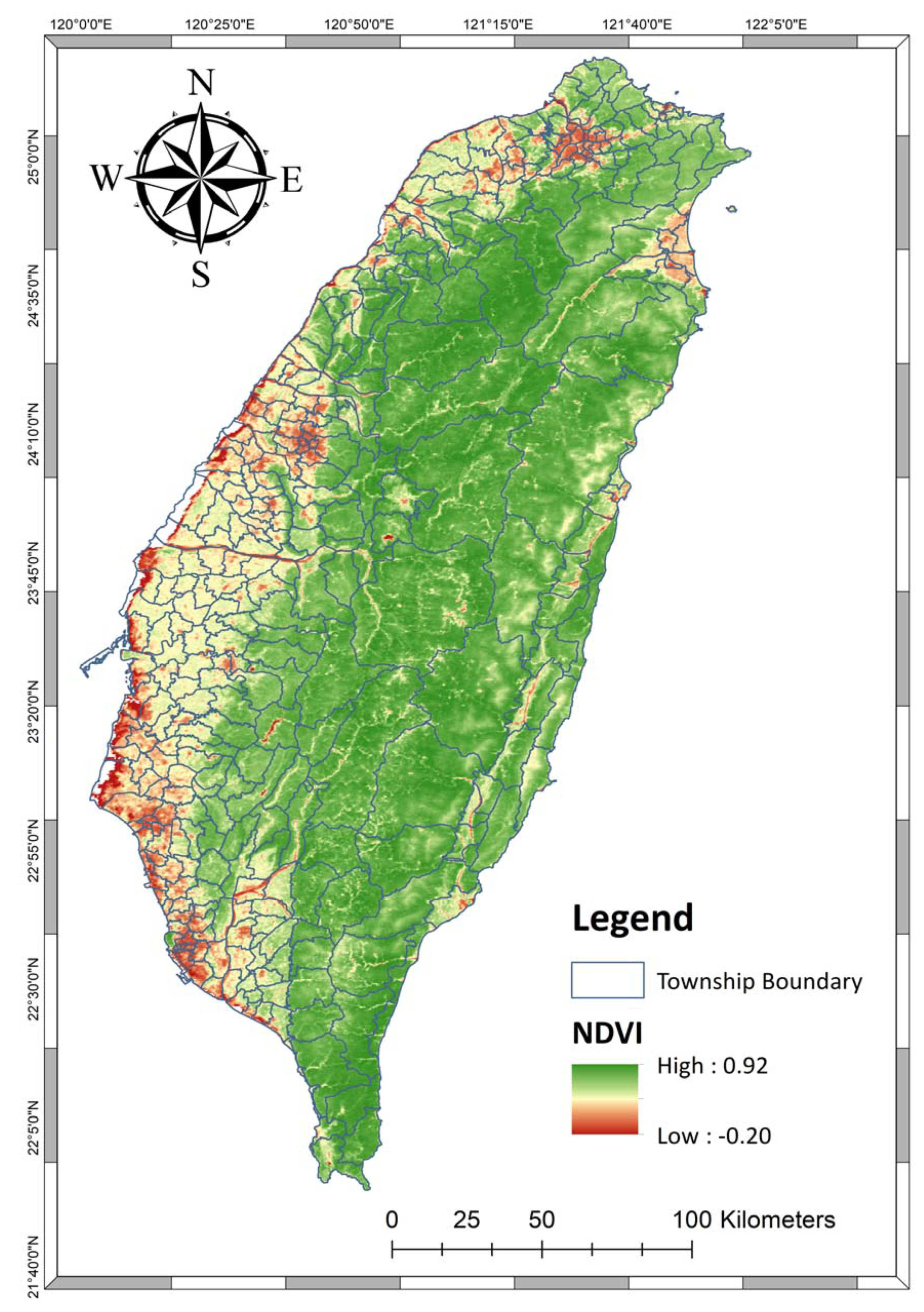
2.2. Index of Surrounding Greenness
2.3. Information of Covariates
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- DALYs, G.B.D.; Collaborators, H. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef] [Green Version]
- Disease, G.B.D.; Injury, I.; Prevalence, C. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Fong, K.C.; Hart, J.E.; James, P. A review of epidemiologic studies on greenness and health: Updated literature through 2017. Curr. Environ. Health Rep. 2018, 5, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crouse, D.L.; Pinault, L.; Balram, A.; Brauer, M.; Burnett, R.T.; Martin, R.V.; van Donkelaar, A.; Villeneuve, P.J.; Weichenthal, S. Complex relationships between greenness, air pollution, and mortality in a population-based Canadian cohort. Environ. Int. 2019, 128, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Yitshak-Sade, M.; James, P.; Kloog, I.; Hart, E.J.; Schwartz, D.J.; Laden, F.; Lane, J.K.; Fabian, P.M.; Fong, C.K.; Zanobetti, A. Neighborhood greenness attenuates the adverse effect of PM2.5 on cardiovascular mortality in neighborhoods of lower socioeconomic status. Int. J. Environ. Res. Public Health 2019, 16, 814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, S.; Sarkar, C.; Kumari, S.; James, P.; Cao, W.; Lee, R.S.; Tian, L.; Webster, C. Air pollution associated respiratory mortality risk alleviated by residential greenness in the Chinese Elderly Health Service Cohort. Environ. Res. 2020, 183, 109139. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef] [Green Version]
- Pereira, G.; Foster, S.; Martin, K.; Christian, H.; Boruff, B.J.; Knuiman, M.; Giles-Corti, B. The association between neighborhood greenness and cardiovascular disease: An observational study. BMC Public Health 2012, 12, 466. [Google Scholar] [CrossRef] [Green Version]
- James, P.; Hart, J.E.; Banay, R.F.; Laden, F. Exposure to greenness and mortality in a nationwide prospective cohort study of women. Environ. Health Perspect. 2016, 124, 1344–1352. [Google Scholar] [CrossRef] [Green Version]
- Iyer, H.S.; Valeri, L.; James, P.; Chen, J.T.; Hart, J.E.; Laden, F.; Holmes, M.D.; Rebbeck, T.R. The contribution of residential greenness to mortality among men with prostate cancer: A registry-based cohort study of Black and White men. Environ. Epidemiol. 2020, 4, e087. [Google Scholar] [CrossRef] [Green Version]
- Vienneau, D.; de Hoogh, K.; Faeh, D.; Kaufmann, M.; Wunderli, J.M.; Roosli, M.; Group, S.N.C.S. More than clean air and tranquillity: Residential green is independently associated with decreasing mortality. Environ. Int. 2017, 108, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Crouse, D.L.; Pinault, L.; Balram, A.; Hystad, P.; Peters, P.A.; Chen, H.; van Donkelaar, A.; Martin, R.V.; Menard, R.; Robichaud, A.; et al. Urban greenness and mortality in Canada’s largest cities: A national cohort study. Lancet Planet. Health 2017, 1, e289–e297. [Google Scholar] [CrossRef]
- Orioli, R.; Antonucci, C.; Scortichini, M.; Cerza, F.; Marando, F.; Ancona, C.; Manes, F.; Davoli, M.; Michelozzi, P.; Forastiere, F.; et al. Exposure to residential greenness as a predictor of cause-specific mortality and stroke incidence in the rome longitudinal study. Environ. Health Perspect. 2019, 127, 27002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, J.S.; Zhu, A.; Bai, C.; Wu, C.D.; Yan, L.; Tang, S.; Zeng, Y.; James, P. Residential greenness and mortality in oldest-old women and men in China: A longitudinal cohort study. Lancet Planet. Health 2019, 3, e17–e25. [Google Scholar] [CrossRef] [Green Version]
- Ji, J.S.; Zhu, A.; Lv, Y.; Shi, X. Interaction between residential greenness and air pollution mortality: Analysis of the Chinese Longitudinal Healthy Longevity Survey. Lancet Planet. Health 2020, 4, e107–e115. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Kim, H.; Lee, J.T. Interactions between ambient air particles and greenness on cause-specific mortality in seven korean metropolitan cities, 2008–2016. Int. J. Environ. Res. Public Health 2019, 16, 1866. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.D.; Zeng, Y.T.; Lung, S.C. A hybrid kriging/land-use regression model to assess PM2.5 spatial-temporal variability. Sci. Total Environ. 2018, 645, 1456–1464. [Google Scholar] [CrossRef]
- Richardson, E.A.; Mitchell, R. Gender differences in relationships between urban green space and health in the United Kingdom. Soc. Sci. Med. 2010, 71, 568–575. [Google Scholar] [CrossRef] [Green Version]
- Richardson, E.; Pearce, J.; Mitchell, R.; Day, P.; Kingham, S. The association between green space and cause-specific mortality in urban New Zealand: An ecological analysis of green space utility. BMC Public Health 2010, 10, 240. [Google Scholar] [CrossRef] [Green Version]
- Richardson, J.; Goss, Z.; Pratt, A.; Sharman, J.; Tighe, M. Building HIA approaches into strategies for green space use: An example from Plymouth’s (UK) Stepping Stones to Nature project. Health Promot. Int. 2013, 28, 502–511. [Google Scholar] [CrossRef] [Green Version]
- Richardson, E.A.; Mitchell, R.; Hartig, T.; de Vries, S.; Astell-Burt, T.; Frumkin, H. Green cities and health: A question of scale? J. Epidemiol. Community Health 2012, 66, 160–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, Y.; Wang, Y.; Yu, H.; Zhang, Y.; Xiang, F.; Yang, Y.; Yang, Y.; Li, L.; Dong, S.; Yang, D.; et al. Geographical variation in lung cancer risk associated with road traffics in Jiading District, Shanghai. Sci. Total Environ. 2019, 652, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Rivas, I.; Basagana, X.; Alvarez-Pedrerol, M.; Su, J.; De Castro Pascual, M.; Amato, F.; Jerret, M.; Querol, X.; Sunyer, J.; et al. The association between greenness and traffic-related air pollution at schools. Sci. Total Environ. 2015, 523, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Nowak, D.J.; Crane, D.E.; Stevens, J.C. Air pollution removal by urban trees and shrubs in the United States. Urban For. Urban Green. 2006, 4, 115–123. [Google Scholar] [CrossRef]
- Lafortezza, R.; Carrus, G.; Sanesi, G.; Davies, C. Benefits and well-being perceived by people visiting green spaces in periods of heat stress. Urban For. Urban Green. 2009, 8, 97–108. [Google Scholar] [CrossRef]
- Gidlöf-Gunnarsson, A.; Öhrström, E. Noise and well-being in urban residential environments: The potential role of perceived availability to nearby green areas. Landsc. Urban Plan. 2007, 83, 115–126. [Google Scholar] [CrossRef]
- Li, Q. Effect of forest bathing trips on human immune function. Environ. Health Prev. Med. 2010, 15, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across Japan. Environ. Health Prev. Med. 2010, 15, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Tsunetsugu, Y.; Park, B.J.; Miyazaki, Y. Trends in research related to "Shinrin-yoku" (taking in the forest atmosphere or forest bathing) in Japan. Environ. Health Prev. Med. 2010, 15, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Mao, G.X.; Cao, Y.B.; Lan, X.G.; He, Z.H.; Chen, Z.M.; Wang, Y.Z.; Hu, X.L.; Lv, Y.D.; Wang, G.F.; Yan, J. Therapeutic effect of forest bathing on human hypertension in the elderly. J. Cardiol. 2012, 60, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Mao, G.X.; Lan, X.G.; Cao, Y.B.; Chen, Z.M.; He, Z.H.; Lv, Y.D.; Wang, Y.Z.; Hu, X.L.; Wang, G.F.; Yan, J. Effects of short-term forest bathing on human health in a broad-leaved evergreen forest in Zhejiang Province, China. Biomed. Environ. Sci. 2012, 25, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.S.; Lim, Y.-R.; Lee, K.; Lee, J.; Lee, J.H.; Lee, I.-S. Terpenes from forests and human health. Toxicol. Res. 2017, 33, 97–106. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Seasonal Mean (SD) a |
|---|---|
| Number of Deaths per 100,000 people | |
| All Cause | 96.09 (93.63) |
| Cardiovascular | 21.91 (21.76) |
| Respiratory | 9.42 (9.87) |
| Lung Cancer | 5.89 (6.61) |
| Sex Ratio (Male/Female) | 107.74 (8.11) |
| Income (thousands of NTD) | 712.79 (166.03) |
| Age Structure (%) | |
| 0–14 | 14.97 (3.07) |
| 15–64 | 71.86 (2.97) |
| >64 | 13.17 (4.21) |
| Index of Greenness | |
| NDVI | 0.51 (0.17) |
| Area of Forest (%) | 30.1 (30.8) |
| Area of Park (%) | 1.17 (2.99) |
| Air Pollutants (μg/m3) | |
| PM2.5 | 27.61 (11.27) |
| NOX | 22.72 (8.62) |
| Precipitation (mm) | 601.9 (530.78) |
| Temperature (°C) | 22.5 (4.08) |
| All-Cause d | Cardiovascular d | Respiratory d | Lung Cancer d | |
|---|---|---|---|---|
| Model 1 a | 0.901 ¶ (0.862, 0.941) | 0.892 ‡ (0.817, 0.975) | 0.721 ¶ (0.632, 0.824) | 0.871 (0.735, 1.032) |
| Model 2 b | 0.896 ¶ (0.857, 0.936) | 0.887 # (0.812, 0.97) | 0.695 ¶ (0.608, 0.795) | 0.866 (0.731, 1.026) |
| Model 3 c | 0.900 ¶ (0.86, 0.94) | 0.892 ‡ (0.816, 0.975) | 0.699 ¶ (0.611, 0.799) | 0.884 (0.746, 1.048) |
| All-Cause a | Cardiovascular a | Respiratory a | Lung Cancer a | |
|---|---|---|---|---|
| Sex Ratio (Male/female) | ||||
| <107.3 | 0.877 ¶ (0.828, 0.928) | 0.893 (0.797, 1.002) | 0.759 # (0.640, 0.901) | 0.843 (0.683, 1.040) |
| ≥107.3 | 0.929 * (0.865, 0.997) | 0.882 (0.767, 1.014) | 0.683 ¶ (0.557, 0.836) | 0.889 (0.682, 1.158) |
| Age 15–64 | ||||
| <71.9% | 0.924 ‡ (0.865, 0.987) | 0.874 ‡ (0.767, 0.996) | 0.661 ¶ (0.545, 0.801) | 0.818 (0.638, 1.048) |
| ≥71.9% | 0.876 ¶ (0.824, 0.931) | 0.892 (0.789, 1.008) | 0.767 # (0.639, 0.921) | 0.831 (0.662, 1.043) |
| Annual Household Income, NTD | ||||
| <668,701 | 0.954 (0.889, 1.025) | 0.882 (0.766, 1.016) | 0.739 (0.602, 0.908) | 0.757 (0.581, 0.987) |
| ≥668,701 | 0.871 (0.822, 0.922) | 0.881 (0.785, 0.988) | 0.733 (0.618, 0.871) | 0.899 (0.729, 1.108) |
| Area | ||||
| Rural | 0.923 (0.867, 0.982) | 0.863 (0.763, 0.976) | 0.733 (0.612, 0.879) | 0.83 (0.651, 1.057) |
| Urban | 0.861 (0.806, 0.919) | 0.903 (0.791, 1.030) | 0.72 (0.590, 0.879) | 0.981 (0.771, 1.247) |
| Greenness Index | All-Cause a | Cardiovascular a | Respiratory a | Lung Cancer a |
|---|---|---|---|---|
| NDVI | 0.901 ¶ (0.862, 0.941) | 0.892 ‡ (0.817, 0.975) | 0.721 ¶ (0.632, 0.824) | 0.871 (0.735, 1.032) |
| Forest Area (%) | 0.883 ¶ (0.866, 0.900) | 0.898 ¶ (0.880, 0.917) | 0.903 ¶ (0.883, 0.923) | 0.884 ¶ (0.864, 0.904) |
| Forest or Park Area (%) | 0.884 ¶ (0.867, 0.901) | 0.898 ¶ (0.88, 0.917) | 0.903 ¶ (0.883, 0.923) | 0.885 ¶ (0.865, 0.905) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.-Y.; Wu, C.-D.; Chang, Y.-T.; Chern, Y.-R.; Lung, S.-C.C.; Su, H.-J.; Pan, W.-C. Association between Surrounding Greenness and Mortality: An Ecological Study in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 4525. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124525
Lee H-Y, Wu C-D, Chang Y-T, Chern Y-R, Lung S-CC, Su H-J, Pan W-C. Association between Surrounding Greenness and Mortality: An Ecological Study in Taiwan. International Journal of Environmental Research and Public Health. 2020; 17(12):4525. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124525
Chicago/Turabian StyleLee, Hsiao-Yun, Chih-Da Wu, Yi-Tsai Chang, Yinq-Rong Chern, Shih-Chun Candice Lung, Huey-Jen Su, and Wen-Chi Pan. 2020. "Association between Surrounding Greenness and Mortality: An Ecological Study in Taiwan" International Journal of Environmental Research and Public Health 17, no. 12: 4525. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124525