Association between Health Problems and Turnover Intention in Shift Work Nurses: Health Problem Clustering



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Measurements
2.3.1. Demographic and Job-Related Characteristics
2.3.2. Turnover Intention
2.3.3. Health Problems
Sleep Disturbance
Fatigue
Depression
2.4. Statistical Analysis
2.5. Ethical Consideration
3. Results
3.1. Demographic and Job-Related Characteristics
3.2. Prevalence and Association between Single Health Problems and Turnover Intention
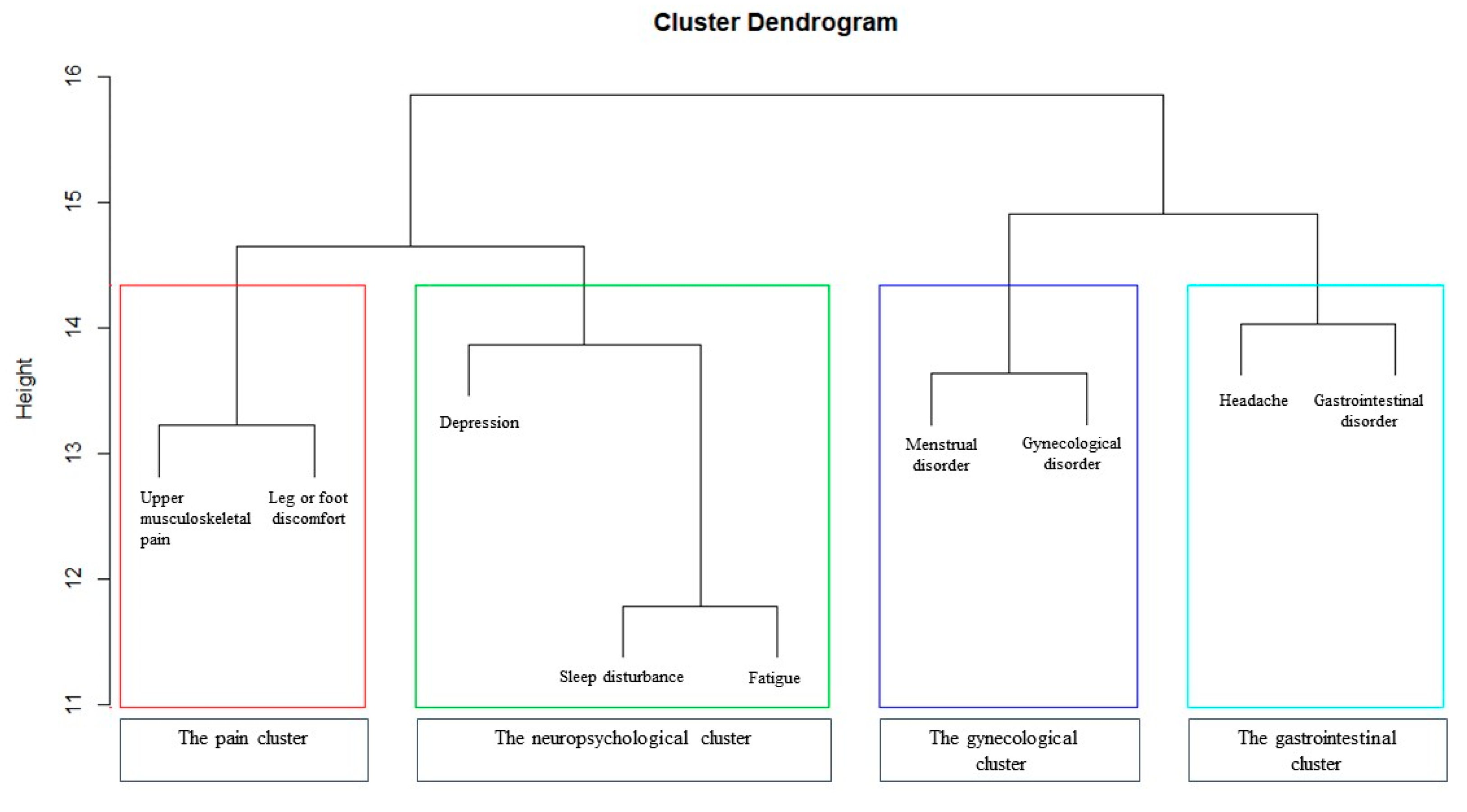
3.3. Hierarchical Clustering of Health Problems
3.4. Prevalence and Association between Clusters of Health Problems and Turnover Intention
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kecklund, G.; Axelsson, J. Health consequences of shift work and insufficient sleep. BMJ 2016, 355, i5210. [Google Scholar] [CrossRef] [PubMed]
- Letvak, S. We cannot ignore nurses’ health anymore: A synthesis of the literature on evidence-based strategies to improve nurse health. Nurs. Adm. Q. 2013, 37, 295–308. [Google Scholar] [CrossRef] [PubMed]
- Hayward, D.; Bungay, V.; Wolff, A.C.; MacDonald, V. A qualitative study of experienced nurses’ voluntary turnover: Learning from their perspectives. J. Clin. Nurs. 2016, 25, 1336–1345. [Google Scholar] [CrossRef]
- Duffield, C.M.; Roche, M.A.; Homer, C.; Buchan, J.; Dimitrelis, S. A comparative review of nurse turnover rates and costs across countries. J. Adv. Nurs. 2014, 70, 2703–2712. [Google Scholar] [CrossRef]
- Korea Hospital Nurse Association. Survey on the Status of Hospital Nursing Staffing; Korea Hospital Nurse Association: Seoul, Korea, 2018. [Google Scholar]
- Yeom, E.Y.; Jeong, G.S.; Kim, K.A. Influencing Factors on Presenteeism of Clinical Nurses. Korean J. Occup. Health Nurs. 2015, 24, 302–312. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Jung, M. Presenteeism and absenteeism according to health problems on nurses. J. Korean Acad. Community Health Nurs. 2008, 19, 459–468. [Google Scholar]
- Yoshida, M.; Miki, A. Factors Related to Presenteeism in Young and Middle-aged Nurses. J. Occup. Health 2018, 60, 31–40. [Google Scholar] [CrossRef] [Green Version]
- Yassi, A.; Lockhart, K. Work-relatedness of low back pain in nursing personnel: A systematic review. Int. J. Occup. Environ. Health 2013, 19, 223–244. [Google Scholar] [CrossRef]
- Abdul Rahman, H.; Abdul-Mumin, K.; Naing, L. Psychosocial Work Stressors, Work Fatigue, and Musculoskeletal Disorders: Comparison between Emergency and Critical Care Nurses in Brunei Public Hospitals. Asian Nurs. Res. 2017, 11, 13–18. [Google Scholar] [CrossRef] [Green Version]
- Wong, H.; Wong, M.C.S.; Wong, S.Y.S.; Lee, A. The association between shift duty and abnormal eating behavior among nurses working in a major hospital: A cross-sectional study. Int. J. Nurs. Stud. 2010, 47, 1021–1027. [Google Scholar] [CrossRef]
- Kim, O.; Ahn, Y.; Lee, H.Y.; Jang, H.J.; Kim, S.; Lee, J.E.; Jung, H.; Cho, E.; Lim, J.Y.; Kim, M.J.; et al. The Korea Nurses’ Health Study: A Prospective Cohort Study. J. Women’s Health 2017, 26, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Zhai, L.; Zhang, H.; Zhang, D. Sleep Duration and Depression among Adults: A Meta-Analysis of Prospective Studies. Depress. Anxiety 2015, 32, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Caruso, C.C. Negative Impacts of Shiftwork and Long Work Hours. Rehabil. Nurs. 2014, 39, 16–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferri, P.; Guadi, M.; Marcheselli, L.; Balduzzi, S.; Magnani, D.; Di Lorenzo, R. The impact of shift work on the psychological and physical health of nurses in a general hospital: A comparison between rotating night shifts and day shifts. Risk Manag. Healthc. Policy 2016, 9, 203–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.-J.; McGuire, D.B.; Tulman, L.; Barsevick, A.M. Symptom clusters: Concept analysis and clinical implications for cancer nursing. Cancer Nurs. 2005, 28, 270–282. [Google Scholar] [CrossRef]
- Barsevick, A. Defining the Symptom Cluster: How Far Have We Come? Semin. Oncol. Nurs. 2016, 32, 334–350. [Google Scholar] [CrossRef]
- Oyane, N.M.F.; Pallesen, S.; Moen, B.E.; Akerstedt, T.; Bjorvatn, B. Associations Between Night Work and Anxiety, Depression, Insomnia, Sleepiness and Fatigue in a Sample of Norwegian Nurses. PLoS ONE 2013, 8, e70228. [Google Scholar] [CrossRef]
- Tuckett, A.; Henwood, T.; Oliffe, J.L.; Kolbe-Alexander, T.L.; Kim, J.R. A Comparative Study of Australian and New Zealand Male and Female Nurses’ Health. Am. J. Men’s Health 2016, 10, 450–458. [Google Scholar] [CrossRef] [Green Version]
- Meeusen, V.C.; Van Dam, K.; Brown-Mahoney, C.; Van Zundert, A.A.; Knape, H.T. Understanding nurse anesthetists’ intention to leave their job: How burnout and job satisfaction mediate the impact of personality and workplace characteristics. Health Care Manag. Rev. 2011, 36, 155–163. [Google Scholar] [CrossRef]
- Estryn-Behar, D.; van der Heijden, B.; Fry, C.; Hasselhorn, H. Longitudinal Analysis of Personal and Work-Related Factors Associated With Turnover Among Nurses. Nurs. Res. 2010, 59, 166–177. [Google Scholar] [CrossRef]
- Han, K.; Trinkoff, A.M.; Gurses, A.P. Work-related factors, job satisfaction and intent to leave the current job among United States nurses. J. Clin. Nurs. 2015, 24, 3224–3232. [Google Scholar] [CrossRef] [PubMed]
- Turpin, R.S.; Ozminkowski, R.J.; Sharda, C.E.; Collins, J.J.; Berger, M.L.; Billotti, G.M.; Baase, C.M.; Olson, M.J.; Nicholson, S. Reliability and validity of the Stanford Presenteeism Scale. J. Occup. Environ. Med. 2004, 46, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Stolt, M.; Suhonen, R.; Virolainen, P.; Leino-Kilpi, H. Lower extremity musculoskeletal disorders in nurses: A narrative literature review. Scand. J. Public Health 2016, 44, 106–115. [Google Scholar] [CrossRef]
- Cai, S.; Lin, H.; Hu, X.; Cai, Y.; Chen, K.; Cai, W. High fatigue and its associations with health and work related factors among female medical personnel at 54 hospitals in Zhuhai, China. Psychol. Health Med. 2018, 23, 304–316. [Google Scholar] [CrossRef] [PubMed]
- Brandford, A.A.; Reed, D.B. Depression in registered nurses: A state of the science. Workplace Health Saf. 2016, 64, 488–511. [Google Scholar] [CrossRef]
- Kang, W.; Jang, K.-H.; Lim, H.-M.; Ahn, J.-S.; Park, W.-J. The menstrual cycle associated with insomnia in newly employed nurses performing shift work: A 12-month follow-up study. Int. Arch. Occup. Environ. Health 2019, 92, 227–235. [Google Scholar] [CrossRef]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale: Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Dunn, H.; Quinn, L.; Corbridge, S.J.; Eldeirawi, K.; Kapella, M.; Collins, E.G. Cluster analysis in nursing research: An introduction, historical perspective, and future directions. West. J. Nurs. Res. 2018, 40, 1658–1676. [Google Scholar] [CrossRef]
- Clatworthy, J.; Buick, D.; Hankins, M.; Weinman, J.; Horne, R. The use and reporting of cluster analysis in health psychology: A review. Br. J. Health Psychol. 2005, 10, 329–358. [Google Scholar] [CrossRef] [PubMed]
- Brooks, I.; Swailes, S. Analysis of the relationship between nurse influences over flexible working and commitment to nursing. J. Adv. Nurs. 2002, 38, 117–126. [Google Scholar] [CrossRef]
- Milisen, K.; Abraham, I.; Siebens, K.; Darras, E.; Dierckx de Casterlé, B. Work environment and workforce problems: A cross-sectional questionnaire survey of hospital nurses in Belgium. Int. J. Nurs. Stud. 2006, 43, 745–754. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Zhou, H.; Rakofsky, J.; Hu, L.; Liu, T.; Wu, S.; Liu, H.; Liu, Y.; Tang, Y. Intention to leave and associated factors among psychiatric nurses in China: A nationwide cross-sectional study. Int. J. Nurs. Stud. 2019, 94, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Camerino, D.; Conway, P.M.; Estryn-Béhar, M.; Costa, G.; Hasselhorn, H.-M. Age-dependent relationships between work ability, thinking of quitting the job, and actual leaving among Italian nurses: A longitudinal study. Int. J. Nurs. Stud. 2008, 45, 1645–1659. [Google Scholar] [CrossRef]
- Estryn-Béhar, M.; Van der Heijden, B.I.; Ogińska, H.; Camerino, D.; Le Nézet, O.; Conway, P.M.; Fry, C.; Hasselhorn, H.-M. The impact of social work environment, teamwork characteristics, burnout, and personal factors upon intent to leave among European nurses. Med. Care 2007, 45, 939–950. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.S.; Du, P.L.; Huang, I.C. Nurses’ perceptions of severe acute respiratory syndrome: Relationship between commitment and intention to leave nursing. J. Adv. Nurs. 2006, 54, 171–179. [Google Scholar] [CrossRef]
- Liu, Y.; Wu, L.M.; Chou, P.L.; Chen, M.H.; Yang, L.C.; Hsu, H.T. The influence of work-related fatigue, work conditions, and personal characteristics on intent to leave among new nurses. J. Nurs. Scholarsh. 2016, 48, 66–73. [Google Scholar] [CrossRef]
- Richter, K.; Acker, J.; Adam, S.; Niklewski, G. Prevention of fatigue and insomnia in shift workers-a review of non-pharmacological measures. EPMA J. 2016, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Ferris, J. Nursing Fatigue: An Evidence-Based Practice Review for Oncology Nurses. Clin. J. Oncol. Nurs. 2015, 19, 662–664. [Google Scholar] [CrossRef]
- Shimizu, T.; Eto, R.; Horiguchi, I.; Obata, Y.; Feng, Q.; Nagata, S. Relationship between Turnover and Periodic Health Check-Up Data among Japanese Hospital Nurses: A Three-Year Follow-Up Study. J. Occup. Health 2005, 47, 327–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, H.; Lin, Y.; Chang, H.; Wang, S.; Liu, Y.; Lee, H.; Peng, T.; Chang, F. Intensive care unit staff nurses: Predicting factors for career decisions. J. Clin. Nurs. 2008, 17, 1886–1896. [Google Scholar] [CrossRef]
- Hsieh, M.L.; Li, Y.M.; Chang, E.T.; Lai, H.L.; Wang, W.H.; Wang, S.C. Sleep disorder in Taiwanese nurses: A random sample survey. Nurs. Health Sci. 2011, 13, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Ji, X.; Zhou, W.; Liu, J. Sleep problems in shift nurses: A brief review and recommendations at both individual and institutional levels. J. Nurs. Manag. 2019, 27, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Bower, J.E.; Ganz, P.A.; Irwin, M.R.; Kwan, L.; Breen, E.C.; Cole, S.W. Inflammation and behavioral symptoms after breast cancer treatment: Do fatigue, depression, and sleep disturbance share a common underlying mechanism? J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 3517–3522. [Google Scholar] [CrossRef] [Green Version]
- Ho, S.-Y.; Rohan, K.J.; Parent, J.; Tager, F.A.; McKinley, P.S. A longitudinal study of depression, fatigue, and sleep disturbances as a symptom cluster in women with breast cancer. J. Pain Symptom Manag. 2015, 49, 707–715. [Google Scholar] [CrossRef]
- Knutsson, A.; Bøggild, H. Gastrointestinal disorders among shift workers. Scand. J. Work. Environ. Health 2010, 36, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Joung Kim, Y.; Ban, D.J. Prevalence of irritable bowel syndrome, influence of lifestyle factors and bowel habits in Korean college students. Int. J. Nurs. Stud. 2005, 42, 247–254. [Google Scholar] [CrossRef]
- Cho, S.H.; Chun, H.; Lee, H.S.; Lee, S.W.; Shim, K.W.; Lee, J.Y.; Byun, A.R.; Lee, H.Y. The Relationship between Shared Breakfast and Skipping Breakfast with Depression and General Health State in Korean Adults: The 2014 Korea National Health and Nutrition Examination Survey. Korean J. Fam. Pract. 2018, 8, 441–447. [Google Scholar] [CrossRef]
- Lee, S.; Lee, J.; Kwon, Y.; Kim, J.; Sohn, J. Clinical Implications of Associations between Headache and Gastrointestinal Disorders: A Study Using the Hallym Smart Clinical Data Warehouse. Front. Neurol. 2017, 8, 526. [Google Scholar] [CrossRef] [Green Version]
- Aamodt, A.; Stovner, L.; Hagen, K.; Zwart, J. Comorbidity of Headache and Gastrointestinal Complaints. The Head-HUNT Study. Cephalalgia 2008, 28, 144–151. [Google Scholar] [PubMed]
- Welton, J.M.; Decker, M.; Adam, J.; Zone-Smith, L. How far do nurses walk? Medsurg Nurs. 2006, 15, 213–216. [Google Scholar] [PubMed]
- Trinkoff, A.M.; Lipscomb, J.A.; Geiger-Brown, J.; Storr, C.L.; Brady, B.A. Perceived physical demands and reported musculoskeletal problems in registered nurses. Am. J. Prev. Med. 2003, 24, 270–275. [Google Scholar] [CrossRef]
- Carnes, D.; Parsons, S.; Ashby, D.; Breen, A.; Foster, N.; Pincus, T.; Vogel, S.; Underwood, M. Chronic musculoskeletal pain rarely presents in a single body site: Results from a UK population study. Rheumatology 2007, 46, 1168–1170. [Google Scholar] [CrossRef] [Green Version]
- Colditz, G.A.; Hankinson, S.E. The Nurses’ Health Study: Lifestyle and health among women. Nat. Rev. Cancer 2005, 5, 388–396. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Categories | Total | Strong Intent to Stay | Intent to Stay | Intent to Leave | Strong Intent to Leave | χ2 or F | p |
|---|---|---|---|---|---|---|---|---|
| (n = 500, 100.0%) | (n = 53, 10.5%) | (n = 336, 67.2%) | (n = 99, 19.9%) | (n = 12, 2.4%) | ||||
| n (%) or M ± SD | n (%) or M ± SD | n (%) or M ± SD | n (%) or M ± SD | n (%) or M ± SD | ||||
| Age (years) | 26.72 ± 4.20 | 28.77 ± 5.68 | 26.29 ± 3.87 | 27.08 ± 4.31 | 26.58 ± 2.35 | 5.70 | 0.001 * | |
| Education | ≤BSN | 459 (91.8) | 48 (90.6) | 310 (92.3) | 89 (89.9) | 12 (100.0) | 1.74 | 0.626 |
| ≥MSN | 41 (8.2) | 5 (9.4) | 26 (7.7) | 10 (10.1) | 0 (0.0) | |||
| Marital Status | Single | 441 (88.2) | 42 (79.3) | 303 (90.2) | 85 (85.9) | 11 (91.7) | 6.00 | 0.108 |
| Married | 59 (11.8) | 11 (20.7) | 33 (9.8) | 14 (14.1) | 1 (8.3) | |||
| Having Children | Yes | 30 (6.0) | 8 (15.1) | 15 (4.5) | 7 (7.1) | 0 (0.0) | 10.14 | 0.030 * |
| No | 470 (94.0) | 45 (84.9) | 321 (95.5) | 92 (92.9) | 12 (100.0) | |||
| Body Mass Index (kg/m2) | 20.19 ± 2.24 | 20.96 ± 2.36 | 20.19 ± 2.19 | 19.92 ± 2.34 | 18.77 ± 1.22 | 4.24 | 0.006 * | |
| Work Unit | Ward | 366 (73.2) | 41 (77.4) | 239 (71.1) | 76 (76.8) | 10 (83.3) | 4.61 | 0.673 |
| ICU | 109 (21.8) | 8 (15.1) | 79 (23.5) | 20 (20.2) | 2 (16.7) | |||
| DR, ER | 25 (5.0) | 4 (7.5) | 18 (5.4) | 3 (3.0) | 0 (0.0) | |||
| Shift Work Experience (months) | 34.93 ± 42.94 | 58.66 ± 59.97 | 30.84 ± 40.01 | 37.03 ± 39.38 | 27.58 ± 27.80 | 6.83 | <0.001 * | |
| Average Number of Nights Per Month (days) | 6.00 ± 1.26 | 5.62 ± 1.48 | 5.98 ± 1.37 | 6.06 ± 1.16 | 6.13 ± 0.78 | 1.45 | 0.228 | |
| Variables | Total | Adjusted 1 Odds Ratio | 95% CI | p |
|---|---|---|---|---|
| (n = 500, 100.0%) | ||||
| n (%) | ||||
| Upper Musculoskeletal Pain | 412 (82.4) | 1.07 | 0.65–1.74 | 0.775 |
| Leg or Foot Discomfort | 339 (67.8) | 1.69 | 1.12–2.56 | 0.012 * |
| Sleep Disturbance | 312 (62.4) | 1.61 | 1.10–2.37 | 0.013 * |
| Fatigue | 325 (65.0) | 3.4 | 2.21–5.24 | <0.001 * |
| Depression | 207 (41.4) | 1.79 | 1.22–2.62 | 0.002 * |
| Menstrual Disorder | 194 (38.8) | 1.26 | 0.86–1.85 | 0.229 |
| Gynecological Disorder | 36 (7.2) | 0.98 | 0.47–2.01 | 0.959 |
| Headache | 195 (39.0) | 1.2 | 0.82–1.75 | 0.343 |
| Gastrointestinal Disorder | 222 (44.4) | 1.51 | 1.03–2.19 | 0.031 * |
| Cluster | Health Problem | Adjusted 1 | ||||
|---|---|---|---|---|---|---|
| Contents | Number | n (%) | Odds Ratio | 95% CI | p | |
| Pain Cluster | Upper musculoskeletal pain + Leg or foot discomfort | 0 | 37 (7.4) | 1.00 | ||
| 1 | 175 (35.0) | 0.57 | 0.27–1.23 | 0.155 | ||
| 2 | 288 (57.6) | 1.11 | 0.54–2.30 | 0.763 | ||
| Neuropsychological Cluster | Sleep disturbance + Fatigue + Depression | 0 | 99 (19.8) | 1.00 | ||
| 1 | 97 (19.4) | 1.59 | 0.85–2.97 | 0.141 | ||
| 2 | 165 (33.0) | 3.35 | 1.90–5.92 | <0.001 * | ||
| 3 | 139 (27.8) | 5.73 | 3.17–10.33 | <0.001 * | ||
| Gynecological Cluster | Menstrual disorder + Gynecological disorder | 0 | 292 (58.4) | 1.00 | ||
| 1 | 186 (37.2) | 1.22 | 0.83–1.81 | 0.298 | ||
| 2 | 22 (4.4) | 1.21 | 0.48–3.05 | 0.676 | ||
| Gastrointestinal Cluster | Headache + Gastrointestinal disorder | 0 | 193 (38.6) | 1.00 | ||
| 1 | 197 (39.4) | 1.43 | 0.94–2.19 | 0.092 | ||
| 2 | 110 (22.0) | 1.60 | 0.98–2.64 | 0.060 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ki, J.; Ryu, J.; Baek, J.; Huh, I.; Choi-Kwon, S. Association between Health Problems and Turnover Intention in Shift Work Nurses: Health Problem Clustering. Int. J. Environ. Res. Public Health 2020, 17, 4532. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124532
Ki J, Ryu J, Baek J, Huh I, Choi-Kwon S. Association between Health Problems and Turnover Intention in Shift Work Nurses: Health Problem Clustering. International Journal of Environmental Research and Public Health. 2020; 17(12):4532. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124532
Chicago/Turabian StyleKi, Jison, Jaegeum Ryu, Jihyun Baek, Iksoo Huh, and Smi Choi-Kwon. 2020. "Association between Health Problems and Turnover Intention in Shift Work Nurses: Health Problem Clustering" International Journal of Environmental Research and Public Health 17, no. 12: 4532. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124532