The Cost of Inflammatory Bowel Disease Management Matches with Clinical Course: A Single Outpatient Centre Analysis

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Patient Cohort
2.3. Care Resources Estimation
- general information: national tax code, age, disease location, therapies (conventional/biological);
- biological drugs (Adalimumab/Infliximab), number of days for therapy administration;
- number of assistance services provided for each year (hospitalization, laboratory tests, instrumental diagnostic examinations and outpatient visits);
- number of working days lost for all welfare service tasks related to disease management for each year.
2.4. Statistics
3. Results
3.1. Clinical and Demographic Data
3.2. Direct and Indirect Costs in 2014
- Conventional therapy: the 58.2% accounted for CD and the 41.8% for UC;
- Biological therapy: the 66.4% accounted for CD and the 33.6% for UC.
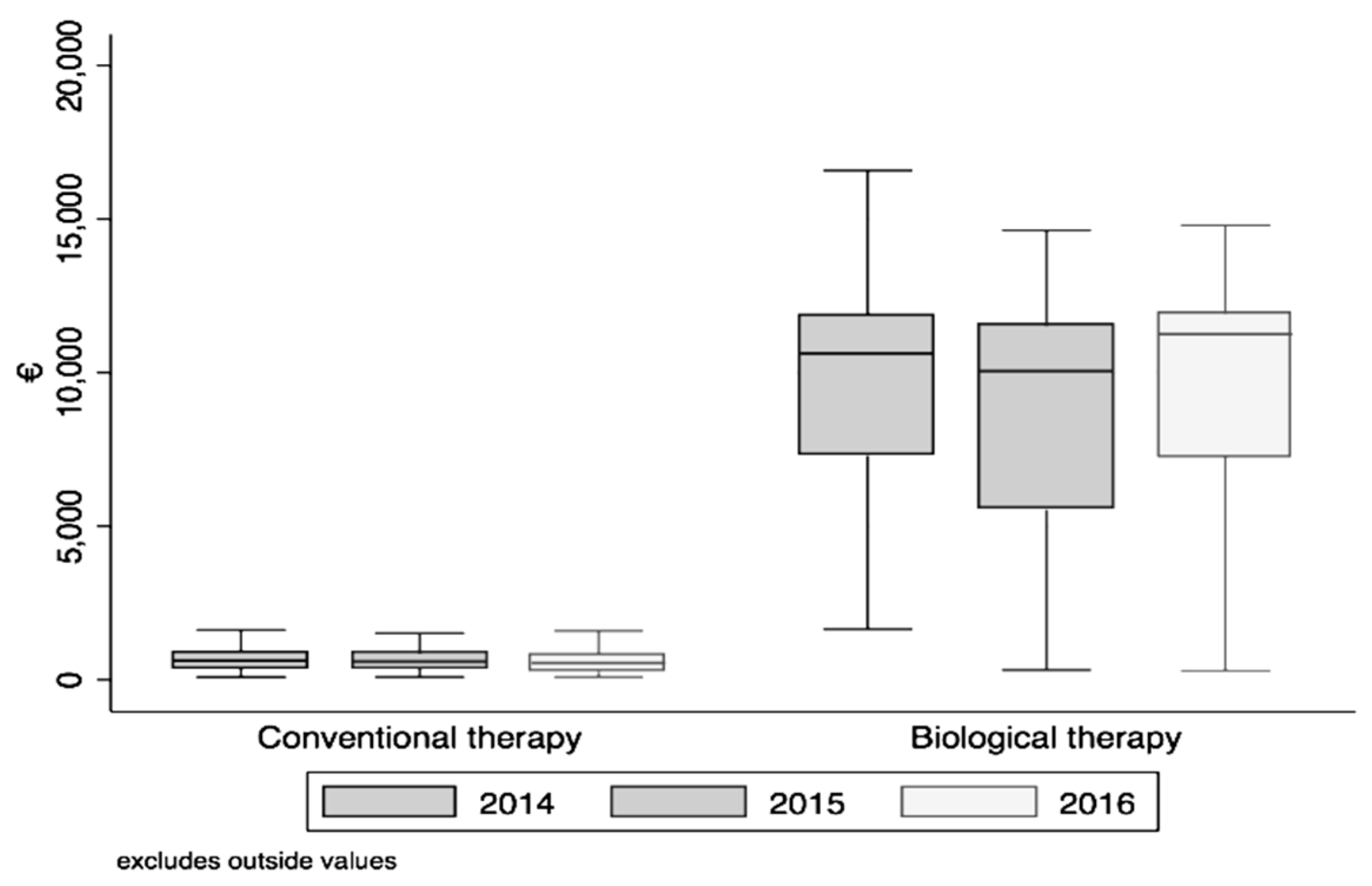
3.3. Cost Estimation in 2014–2016 Follow-Up
- cost for each year (January 2014–December 2016) (Fr = 901.0; p < 0.001);
- costs in the whole three-year period (2014–2016) between the subjects undergoing biological (Fr = 145.8; p < 0.001) and conventional therapy (Fr = 587.8; p = 0.001).
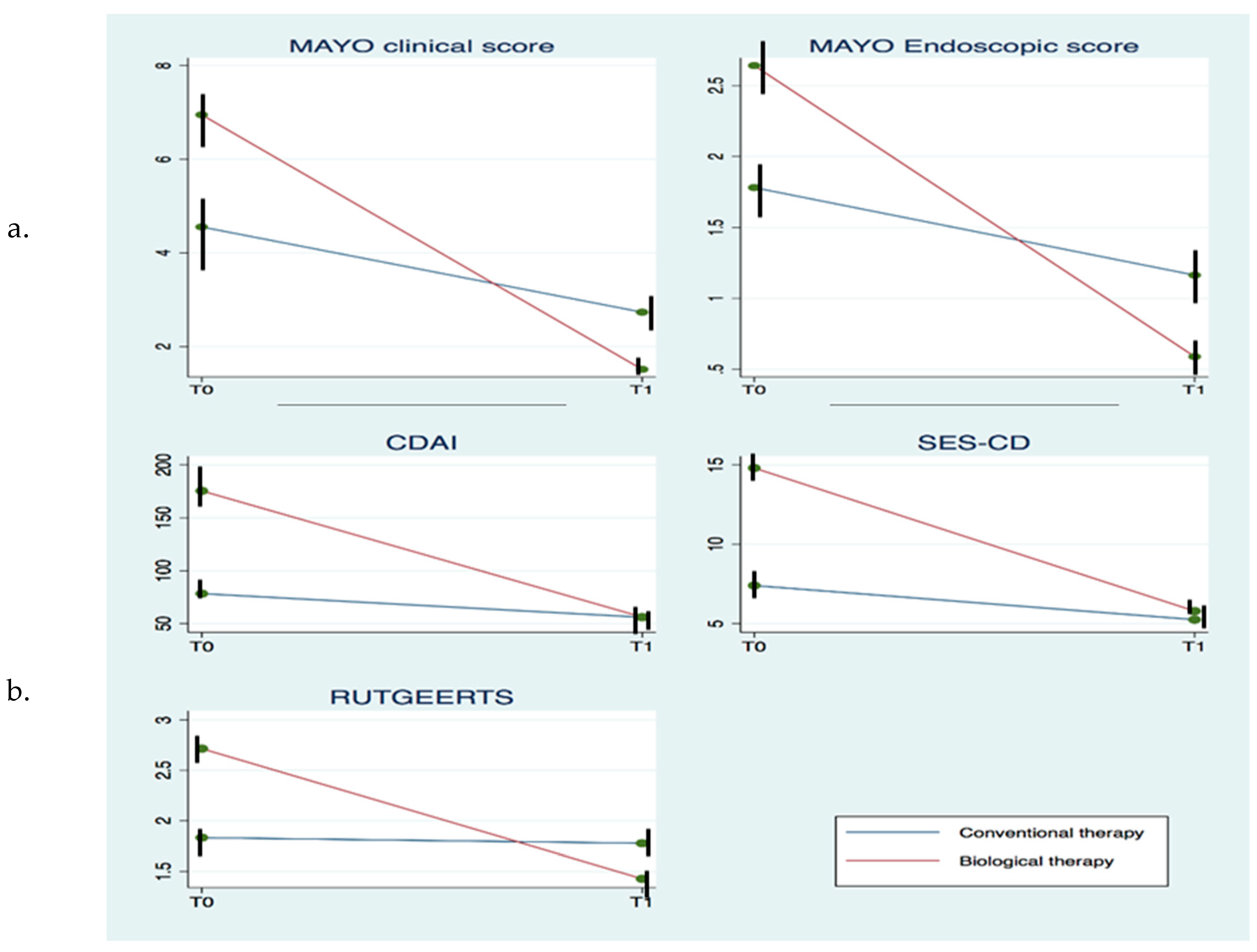
3.4. Disease Activity in 3-Year Follow-Up (2014–2016)
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wallace, K.L.; Zheng, L.-B.; Kanazawa, Y.; Shih, D.Q. Immunopathology of inflammatory bowel disease. World J. Gastroenterol. 2014, 20, 6–21. [Google Scholar] [CrossRef]
- Cosnes, J.; Cattan, S.; Blain, A.; Beaugerie, L.; Carbonnel, F.; Parc, R.; Gendre, J.-P. Long-Term Evolution of Disease Behavior of Crohn’s Disease. Inflamm. Bowel Dis. 2002, 8, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, D.C.; Sandborn, W.J. Inflammatory bowel disease: Clinical aspects and established and evolving therapies. Lancet 2007, 369, 1641–1657. [Google Scholar] [CrossRef]
- Cosnes, J.; Gower-Rousseau, C.; Seksik, P.; Cortot, A. Epidemiology and Natural History of Inflammatory Bowel Diseases. Gastroenterology 2011, 140, 1785–1794.e4. [Google Scholar] [CrossRef] [PubMed]
- Colombel, J.-F.; Rutgeerts, P.; Sandborn, W.J.; Yang, M.; Camez, A.; Pollack, P.F.; Thakkar, R.B.; Robinson, A.M.; Chen, N.; Mulani, P.M.; et al. Adalimumab Induces Deep Remission in Patients With Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2014, 12, 414–422.e5. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, D.C.; Sandborn, W.J. Crohn’s disease. Lancet 2012, 380, 1590–1605. [Google Scholar] [CrossRef] [Green Version]
- Abraham, C.; Cho, J. Inflammatory bowel disease. New Engl. J. Med. 2009, 361, 2066–2078. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Ferrante, M.; Magro, F.; Campbell, S.; Franchimont, D.; Fidder, H.; Strid, H.; Ardizzone, S.; Veereman-Wauters, G.; Chevaux, J.-B.; et al. Results from the 2nd Scientific Workshop of the ECCO (I): Impact of mucosal healing on the course of inflammatory bowel disease. J. Crohns Coliti 2011, 5, 477–483. [Google Scholar] [CrossRef]
- Williet, N.; Sandborn, W.J.; Peyrin–Biroulet, L. Patient-Reported Outcomes as Primary End Points in Clinical Trials of Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2014, 12, 1246–1256.e6. [Google Scholar] [CrossRef]
- Colombel, J.-F.; Rutgeerts, P.; Reinisch, W.; Esser, D.; Wang, Y.; Lang, Y.; Marano, C.W.; Strauss, R.; Oddens, B.J.; Feagan, B.G.; et al. Early Mucosal Healing with Infliximab Is Associated with Improved Long-term Clinical Outcomes in Ulcerative Colitis. Gastroenterology 2011, 141, 1194–1201. [Google Scholar] [CrossRef]
- Gomes, P.; du Boulay, C.; Smith, C.L.; Holdstock, G. Relationship between disease activity indices and colonoscopic findings in patients with colonic inflammatory bowel disease. Gut 1986, 27, 92–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peyrin-Biroulet, L.; Reinisch, W.; Colombel, J.-F.; Mantzaris, G.J.; Kornbluth, A.; Diamond, R.; Rutgeerts, P.; Tang, L.K.; Cornillie, F.J.; Sandborn, W.J. Clinical disease activity, C-reactive protein normalisation and mucosal healing in Crohn’s disease in the SONIC trial. Gut 2013, 63, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Rutgeerts, P.; Sandborn, W.J.; Feagan, B.G.; Reinisch, W.; Olson, A.; Johanns, J.; Travers, S.; Rachmilewitz, D.; Hanauer, S.B.; Lichtenstein, G.R.; et al. Infliximab for Induction and Maintenance Therapy for Ulcerative Colitis. New Engl. J. Med. 2005, 353, 2462–2476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lichtenstein, G.R.; Feagan, B.G.; Cohen, R.D.; Salzberg, B.A.; Diamond, R.H.; Chen, D.M.; Pritchard, M.L.; Sandborn, W.J. Serious Infections and Mortality in Association with Therapies for Crohn’s Disease: TREAT Registry. Clin. Gastroenterol. Hepatol. 2006, 4, 621–630. [Google Scholar] [CrossRef]
- Osterman, M.T.; Sandborn, W.J.; Colombel, J.-F.; Peyrin-Biroulet, L.; Robinson, A.M.; Zhou, Q.; Lewis, J.D. Crohn’s Disease Activity and Concomitant Immunosuppressants Affect the Risk of Serious and Opportunistic Infections in Patients Treated with Adalimumab. Am. J. Gastroenterol. 2016, 111, 1806–1815. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.P.; Cabanilla, L.A.; Wu, E.Q.; Mulani, P.M.; Chao, J. The costs of Crohn’s disease in the United States and other Western countries: A systematic review. Curr. Med Res. Opin. 2007, 24, 319–328. [Google Scholar] [CrossRef]
- van der Valk, M.E.; Mangen, M.-J.J.; Leenders, M.; Dijkstra, G.; van Bodegraven, A.A.; Fidder, H.H.; de Jong, D.J.; Pierik, M.; van der Woude, C.J.; Romberg-Camps, M.J.L.; et al. Healthcare costs of inflammatory bowel disease have shifted from hospitalisation and surgery towards anti-TNFα therapy: Results from the COIN study. Gut 2012, 63, 72–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bähler, C.; Schoepfer, A.M.; Vavricka, S.R.; Brüngger, B.; Reich, O. Chronic comorbidities associated with inflammatory bowel disease. Eur. J. Gastroenterol. Hepatol. 2017, 29, 916–925. [Google Scholar] [CrossRef] [PubMed]
- Severs, M.; Oldenburg, B.; A van Bodegraven, A.; Siersema, P.D.; Mangen, M.-J.J. The Economic Impact of the Introduction of Biosimilars in Inflammatory Bowel Disease. J. Crohns Coliti 2016, 11, 289–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomollón, F.; Dignass, A.; Annese, V.; Tilg, H.; van Assche, G.; Lindsay, J.O.; Peyrin-Biroulet, L.; Cullen, G.J.; Daperno, M.; Kucharzik, T.; et al. 3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 1: Diagnosis and Medical Management. J. Crohns Coliti 2016, 11, 3–25. [Google Scholar] [CrossRef] [Green Version]
- Harbord, M.; Eliakim, R.; Bettenworth, D.; Karmiris, K.; Katsanos, K.; Kopylov, U.; Kucharzik, T.; Molnar, T.; Raine, T.; Sebastian, S.; et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 2: Current Management. J. Crohns Coliti 2017, 11, 769–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FIMMG Bari—Sist Puglia: Aggiornamento del Nomenclatore Tariffario e Catalogo Unico Regionale. Available online: https://fimmg.bari.it/articoli/0CAAA (accessed on 9 May 2020).
- Gazzetta Ufficiale. Available online: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=2005-10-13&atto.codiceRedazionale=005G0233&elenco30giorni=false (accessed on 10 May 2020).
- Petryszyn, P.; Witczak, I. Costs in inflammatory bowel diseases. Gastroenterol. Rev. 2016, 11, 6–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burger, D.; Travis, S. Conventional Medical Management of Inflammatory Bowel Disease. Gastroenterology 2011, 140, 1827–1837.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odes, S.; Vardi, H.; Friger, M.; Wolters, F.; Russel, M.G.; Riis, L.; Munkholm, P.; Politi, P.; Tsianos, E.; Clofent, J.; et al. Cost Analysis and Cost Determinants in a European Inflammatory Bowel Disease Inception Cohort With 10 Years of Follow-up Evaluation. Gastroenterology 2006, 131, 719–728. [Google Scholar] [CrossRef]
- Bassi, A.; Dodd, S.; Williamson, P.; Bodger, K. Cost of illness of inflammatory bowel disease in the UK: A single centre retrospective study. Gut 2004, 53, 1471–1478. [Google Scholar] [CrossRef]
- Burisch, J.; Vardi, H.; Pedersen, N.; Brinar, M.; Cukovic-Cavka, S.; Kaimakliotis, I.; Duricova, D.; Bortlík, M.; Shonová, O.; Vind, I.; et al. Costs and Resource Utilization for Diagnosis and Treatment During the Initial Year in a European Inflammatory Bowel Disease Inception Cohort. Inflamm. Bowel Dis. 2015, 21, 121–131. [Google Scholar] [CrossRef]
- Gibson, P.R.; Weston, A.R.; Shann, A.; Florin, T.H.J.; Lawrance, I.C.; Macrae, F.A.; Radford-Smith, G. Relationship between disease severity, quality of life and health-care resource use in a cross-section of Australian patients with Crohn’s disease. J. Gastroenterol. Hepatol. 2007, 22, 1306–1312. [Google Scholar] [CrossRef]
- Odes, S. How expensive is inflammatory bowel disease? A critical analysis. World J. Gastroenterol. 2008, 14, 6641–6647. [Google Scholar] [CrossRef]
- Feagan, B.G.; Vreeland, M.G.; Larson, L.R.; Bala, M.V. Annual cost of care for Crohn’s disease: A payor perspective. Am. J. Gastroenterol. 2000, 95, 1955–1960. [Google Scholar] [CrossRef]
- Hay, J.W.; Hay, A.R. Inflammatory Bowel Disease. J. Clin. Gastroenterol. 1992, 14, 309–317. [Google Scholar] [CrossRef]
- Bodger, K. Cost effectiveness of treatments for inflammatory bowel disease. Pharmacoeconomics 2011, 29, 387–401. [Google Scholar] [CrossRef] [PubMed]
- Targownik, L.E.; Benchimol, E.I.; Witt, J.; Bernstein, C.N.; Singh, H.; Lix, L.; Tennakoon, A.; Zubieta, A.A.; Coward, S.; Jones, J.; et al. The Effect of Initiation of Anti-TNF Therapy on the Subsequent Direct Health Care Costs of Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2019, 25, 1718–1728. [Google Scholar] [CrossRef] [PubMed]
- Blumenstein, I.; Bock, H.; Weber, C.; Rambow, A.; Tacke, W.; Kihn, R.; Pfaff, R.; Orlemann, S.; Schaeffer, R.; Schröder, O.; et al. Health care and cost of medication for inflammatory bowel disease in the Rhein-Main region, Germany: A multicenter, prospective, internet-based study. Inflamm. Bowel Dis. 2008, 14, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Aniwan, S.; Harmsen, W.S.; Tremaine, W.J.; Lightner, A.L.; Faubion, W.A. Update on the Natural Course of Fistulizing Perianal Crohn’s Disease in a Population-Based Cohort. Inflamm. Bowel Dis. 2018, 25, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- Jackson, B.D.; Con, D.; Gorelik, A.; Liew, D.; Knowles, S.R.; de Cruz, P. Examination of the relationship between disease activity and patient-reported outcome measures in an inflammatory bowel disease cohort. Intern. Med. J. 2018, 48, 1234–1241. [Google Scholar] [CrossRef]
- Principi, M.; Losurdo, G.; la Fortezza, R.F.; Lopolito, P.; Lovero, R.; Grillo, S.; Bringiotti, R.; Ierardi, E.; di Leo, A. Does Infliximab Short Infusion have a Beneficial Impact on the Quality of Life in Patients with Inflammatory Bowel Diseases? A Single Centre Prospective Evaluation. J. Gastrointest. Liver Dis. 2015, 24, 165–170. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Crohn’s Disease | ||
|---|---|---|
| Conventional therapy | Biological therapy | |
| L1 | 74.9% | 57.3% |
| L2 | 12.9% | 12.0% |
| L3 | 12.2% | 30.7% |
| B1 | 86.6% | 66.7% |
| B2 | 13.4% | 32.0% |
| B3 | 0.0% | 1.3% |
| Ulcerativa Colitis | ||
| Conventional therapy | Biological therapy | |
| Proctitis | 34.7% | 23.7% |
| Proctosigmoiditis | 43.3% | 29.0% |
| Left colitis | 7.0% | 2.6% |
| Pancolitis | 15.0% | 44.7% |
| DIRECT COSTS | |||
|---|---|---|---|
| Conventional Therapy | Biological Therapy | Total | |
| Instrumental diagnostic procedures | 89.3 ± 186.2 (0.0–1106.3) | 197.3 ± 296.8 (0.0–1816.9) | 119.0 ± 227.0 (0.0–1816.9) |
| Outpatient visits | 24.5 ± 23.7 (0.0–198.2) | 54.4 ± 70.0 (0.0–339.6) | 32.7 ± 43.7 (0.0–339.6) |
| Laboratory tests | 89.9 ± 102.2 (0.0–580.6) | 201.0 ± 157.6 (0.0–623.8) | 120.3 ± 129.6 (0.0–623.8) |
| Hospitalizations | 84.9 ± 654.6 (0.0–6318.0) | 462.5 ± 2241.7 (0.0–16,079.0) | 189.5 ± 1311.9 (0.0–16,079.0) |
| Drugs | 318.2 ± 218.4 (23.3–1264.7) | 8179.1 ± 3421.2 (571.2–14,831.9) | 2355.5 ± 3865.4 (24.3–14,831.9) |
| INDIRECT COSTS | |||
| Lost Working Days | Conventional Therapy | Biological Therapy | Total |
| Drug administration | 0.0 ± 0.0 (0.0–0.0) | 75.6 ± 112.4 (0.0–371.4) | 20.9 ± 67.9 (0.0–371.4) |
| Instrumental diagnostic | 24.7 ± 39.2 (0.0–232.2) | 46.0 ± 46.2 (0.0–185.7) | 30.6 ± 42.3 (0.0–232.2) |
| Outpatient visits | 56.1 ± 53.2 (0.0–417.9) | 119.4 ± 157.7 (0.0–882.2) | 73.4 ± 97.9 (0.0–882.2) |
| Laboratory tests | 54.5 ± 62.5 (0.0–417.9) | 127.4 ± 93.8 (0.0–325.0) | 74.4 ± 79.3 (0.0–417.9) |
| Hospitalizations | 8.5 ± 59.0 (0.0–417.9) | 33.3 ± 149.2 (0.0–1253.6) | 15.3 ± 93.6 (0.0–1253.6) |
| Year | 2014 | 2015 | 2016 |
|---|---|---|---|
| Infliximab | |||
| Instrumental diagnostic | 146.1 ± 301.3 (0.0–1816.9) | 161.6 ± 768.4 (0.0–5764.0) | 73.2 ± 186.4 (0.0–1200.0) |
| Outpatient visits | 73.3 ± 90.4 (0.0–339.6) | 74.1 ± 87.7 (0.0–377.2) | 56.4 ± 85.3 (0.0–474.0) |
| Laboratory tests | 222.9 ± 168.9 (0.0–623.8) | 260.2 ± 296.1 (0.0–1280.7) | 220.9 ± 227.9 (0.0–878.7) |
| Hospitalizations | 55.6 ± 304.2 (0.0–2014.0) | 283.5 ± 1422.6 (0.0–9477.0) | 0.0 ± 0.0 (0.0–0.0) |
| Total direct costs | 500.7 ± 578.6 (0.0–3143.1) | 788.4 ± 1712.9 (0.0–9950.5) | 350.5 ± 364.5 (0.0–1492.5) |
| Adalimumab | |||
| Instrumental diagnostic | 248.5 ± 285.7 (0.0–908.5) | 142.3 ± 226.9 (0.0–961.3) | 175.5 ± 277.6 (0.0–1526.1) |
| Outpatient visits | 36.3 ± 33.9 (0.0–181.0) | 34.3 ± 46.8 (0.0–295.2) | 40.0 ± 49.8 (0.0–215.7) |
| Laboratory tests | 179.4 ± 143.9 (0.0–551.3) | 125.5 ± 137.8 (0.0–770.2) | 145.2 ± 114.7 (0.0–421.1) |
| Hospitalizations | 862.3 ± 3103.4 (0.0–16,079.0) | 82.9 ± 501.1 (0.0–3645.0) | 18.7 ± 141.5 (0.0–1068.0) |
| Total direct costs | 1344.1 ± 3113.7 (0.0–16,458.8) | 385.1 ± 571.1 (0.0–3836.7) | 379.5 ± 367.7 (0.0–1858.2) |
| Total | |||
| Instrumental diagnostic | 197.3 ± 296.8 (0.0–1816.9) | 151.9 ± 561.9 (0.0–5764.0) | 124.8 ± 241.3 (0.0–1526.1) |
| Outpatient visits | 54.4 ± 70.0 (0.0–339.6) | 54.0 ± 72.6 (0.0–377.2) | 48.1 ± 69.9 (0.0–474.0) |
| Laboratory tests | 201.0 ± 157.6 (0.0–623.8) | 191.6 ± 238.2 (0.0–1280.7) | 182.7 ± 183.1 (0.0–878.7) |
| Hospitalizations | 462.5 ± 2241.7 (0.0–16,079.0) | 182.3 ± 1062.8 (0.0–9477.0) | 9.5 ± 100.5 (0.0–1068.0) |
| Total direct costs | 926.2 ± 2278.4 (0.0–16,458.8) | 583.2 ± 1277.9 (0.0–9950.5) | 365.1 ± 364.8 (0.0–1858.2) |
| Infliximab | Adalimumab | z | p | |
|---|---|---|---|---|
| 2014 | 8364.5 ± 3209.1 (1652.0–16,581.5) | 10,648.6 ± 4317.6 (2134.1–28,429.0) | 3.8 | <0.001 |
| 2015 | 8214.9 ± 4261.3 (320.4–25,432.0) | 9182 ± 3568.9 (1290.2–12,519.8) | 1.8 | 0.075 |
| 2016 | 8555.8 ± 3820.7 (263.5–14,807.1) | 10,253.8 ± 3494.1 (1024.3–13,577.3) | 2.6 | 0.009 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Principi, M.; Labarile, N.; Bianchi, F.P.; Contaldo, A.; Tafuri, S.; Ierardi, E.; Di Leo, A. The Cost of Inflammatory Bowel Disease Management Matches with Clinical Course: A Single Outpatient Centre Analysis. Int. J. Environ. Res. Public Health 2020, 17, 4549. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124549
Principi M, Labarile N, Bianchi FP, Contaldo A, Tafuri S, Ierardi E, Di Leo A. The Cost of Inflammatory Bowel Disease Management Matches with Clinical Course: A Single Outpatient Centre Analysis. International Journal of Environmental Research and Public Health. 2020; 17(12):4549. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124549
Chicago/Turabian StylePrincipi, Mariabeatrice, Nunzia Labarile, Francesco Paolo Bianchi, Antonella Contaldo, Silvio Tafuri, Enzo Ierardi, and Alfredo Di Leo. 2020. "The Cost of Inflammatory Bowel Disease Management Matches with Clinical Course: A Single Outpatient Centre Analysis" International Journal of Environmental Research and Public Health 17, no. 12: 4549. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124549