Is Lockdown Bad for Social Anxiety in COVID-19 Regions?: A National Study in The SOR Perspective


Abstract
:1. Introduction
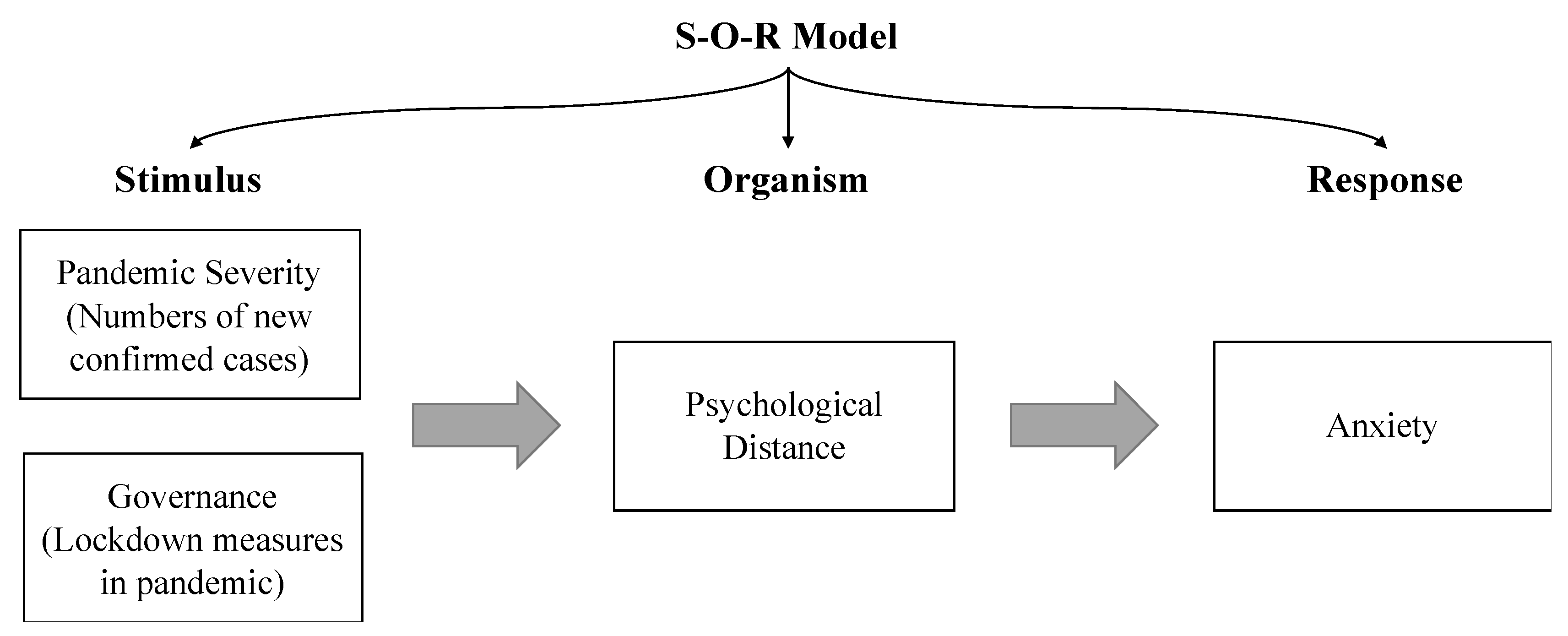
2. Conceptual Model and Hypothesis
2.1. Pandemic Severity and Social Anxiety
2.2. Psychological Distance and Social Anxiety
2.3. Lockdown, Psychological Distance, and Anxiety
3. Materials and Methods
3.1. Participants
3.2. Measures
4. Results
4.1. Descriptive Information
4.2. Pandemic Severity Impacts Anxiety Through Psychological Distancing
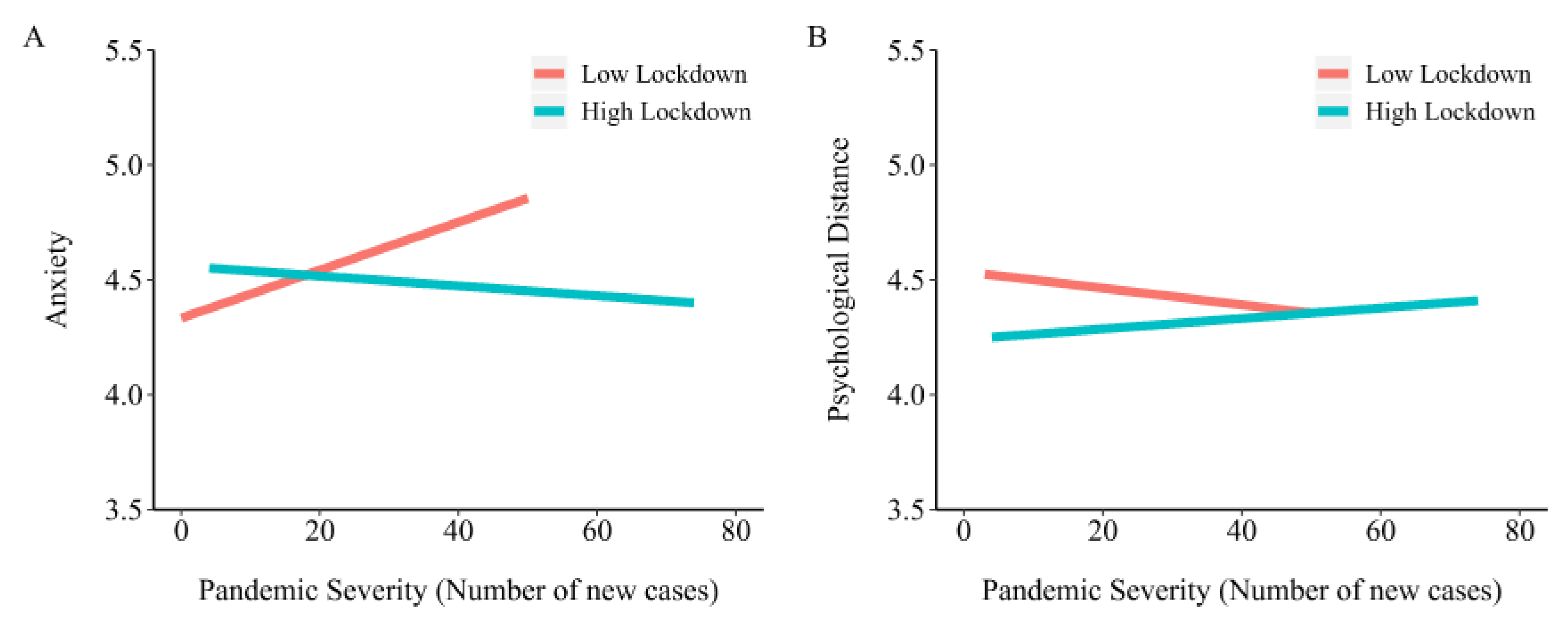
4.3. Lockdown Buffers Pandemic by Moderating Psychological Distance Against Anxiety
5. Discussion
5.1. The SOR Model Explains How Pandemic Impacts Emotions
5.2. Evidence for the Psychological Effects of Lockdown in the Pandemic Region
5.3. Social Psychological Problems in Epidemic Governance
5.4. Practical Implications
5.5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lau, H.; Khosrawipour, V.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J. Travel Med. 2020, 27, taaa037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peto, J.; Alwan, N.A.; Godfrey, K.M.; Burgess, R.A.; Hunter, D.J.; Riboli, E.; Romer, P. Universal weekly testing as the UK COVID-19 lockdown exit strategy. Lancet 2020, 395, 1420–1421. [Google Scholar] [CrossRef]
- Zanin, G.M.; Gentile, E.; Parisi, A.; Spasiano, D. A Preliminary Evaluation of the Public Risk Perception Related to the COVID-19 Health Emergency in Italy. Int. J. Environ. Res. Public Health 2020, 17, 3024. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.J.; Wessely, S. The psychological effects of quarantining a city. BMJ 2020, 368, m313. [Google Scholar] [CrossRef] [Green Version]
- Bergeron, S.L.; Sanchez, A.L. Media effects on students during SARS outbreak. Emerg. Infect. Dis. 2005, 11, 732. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.J.; Amlôt, R.; Page, L.A.; Wessely, S. Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: Cross sectional telephone survey. BMJ 2009, 339, b2651. [Google Scholar] [CrossRef] [Green Version]
- Wong, T.W.; Gao, Y.; Tam, W.W.S. Anxiety among university students during the SARS epidemic in Hong Kong. Stress Health: J. Int. Soc. Investig. Stress 2007, 23, 31–35. [Google Scholar] [CrossRef]
- McGrath, J.W. The biological impact of social responses to the AIDS epidemic. Med Anthropol. 1993, 15, 63–79. [Google Scholar] [CrossRef]
- Strong, P. Epidemic psychology: A model. Sociol. Health Illn. 1990, 12, 249–259. [Google Scholar] [CrossRef]
- Zarocostas, J. Violence hinders efforts to stem Haiti cholera epidemic as deaths continue to rise. BMJ Br. Med. J. (Online) 2010, 341, c7259. [Google Scholar] [CrossRef]
- Kim, D.H. ‘How do you feel about a disease?’ The effect of psychological distance towards a disease on health communication. Int. J. Advert. 2019, 38, 139–153. [Google Scholar]
- Chen, Q.; Liang, M.; Li, Y.; Guo, J.; Fei, D.; Wang, L.; He, L.; Sheng, C.; Cai, Y.; Li, X.; et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e15–e16. [Google Scholar] [CrossRef]
- Cao, X.; Sun, J. Exploring the effect of overload on the discontinuous intention of social media users: An SOR perspective. Comput. Hum. Behav. 2018, 81, 10–18. [Google Scholar] [CrossRef]
- Jang, S.S.; Namkung, Y. Perceived quality, emotions, and behavioral intentions: Application of an extended Mehrabian–Russell model to restaurants. J. Bus. Res. 2009, 62, 451–460. [Google Scholar] [CrossRef]
- Folkman, S. The case for positive emotions in the stress process. Anxiety Stress Coping 2008, 21, 3–14. [Google Scholar] [CrossRef]
- Zheng, L.; Lippke, S.; Chen, Y.; Li, D.; Gan, Y. Future orientation buffers depression in daily and specific stress. Psych. J. 2019, 8, 342–352. [Google Scholar] [CrossRef]
- Tausczik, Y.; Faasse, K.; Pennebaker, J.W.; Petrie, K.J. Public anxiety and information seeking following the H1N1 outbreak: Blogs, newspaper articles, and Wikipedia visits. Health Commun. 2012, 27, 179–185. [Google Scholar] [CrossRef]
- Quah, S.R.; Hin-Peng, L. Crisis prevention and management during SARS outbreak, Singapore. Emerg. Infect. Dis. 2004, 10, 364. [Google Scholar] [CrossRef]
- Bults, M.; Beaujean, D.J.; de Zwart, O.; Kok, G.; van Empelen, P.; van Steenbergen, J.E.; Richardus, J.H.; Voeten, H.A. Perceived risk, anxiety, and behavioural responses of the general public during the early phase of the Influenza A (H1N1) pandemic in the Netherlands: Results of three consecutive online surveys. BMC Public Health 2011, 11, 2. [Google Scholar] [CrossRef] [Green Version]
- Liberman, N.; Trope, Y. Traversing psychological distance. Trends Cogn. Sci. 2014, 18, 364–369. [Google Scholar] [CrossRef]
- Trope, Y.; Liberman, N. Construal-level theory of psychological distance. Psychol. Rev. 2010, 117, 440–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trope, Y.; Liberman, N.; Wakslak, C. Construal levels and psychological distance: Effects on representation, prediction, evaluation, and behavior. J. Consum. Psychol. 2007, 17, 83–95. [Google Scholar] [CrossRef] [Green Version]
- Lau, A.L.D.; Chi, I.; Cummins, R.A.; Lee, T.M.C.; Chou, K.-L.; Chung, L.W.M. The SARS (Severe Acute Respiratory Syndrome) pandemic in Hong Kong: Effects on the subjective wellbeing of elderly and younger people. Aging Ment. Health 2008, 12, 746–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- BBC. Sierra Leone begins Ebola Lockdown; BBC: London, UK, 2014. [Google Scholar]
- Gostin, L.O.; Friedman, E.A. Ebola: A crisis in global health leadership. Lancet 2014, 384, 1323–1325. [Google Scholar] [CrossRef] [Green Version]
- Gostin, L.O.; Friedman, E.A. A retrospective and prospective analysis of the west African Ebola virus disease epidemic: Robust national health systems at the foundation and an empowered WHO at the apex. Lancet 2015, 385, 1902–1909. [Google Scholar] [CrossRef] [Green Version]
- Peak, C.M.; Wesolowski, A.; Erbach-Schoenberg, E.Z.; Tatem, A.J.; Wetter, E.; Lu, X.; Power, D.; Weidman-Grunewald, E.; Ramos, S.; Moritz, S.; et al. Population mobility reductions associated with travel restrictions during the Ebola epidemic in Sierra Leone: Use of mobile phone data. Int. J. Epidemiol. 2018, 47, 1562–1570. [Google Scholar] [CrossRef]
- Liao, Q.; Cowling, B.J.; Lam, W.W.T.; Ng, D.M.W.; Fielding, R. Anxiety, worry and cognitive risk estimate in relation to protective behaviors during the 2009 influenza A/H1N1 pandemic in Hong Kong: Ten cross-sectional surveys. BMC Infect. Dis. 2014, 14, 169. [Google Scholar] [CrossRef] [Green Version]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen Psychiatr 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: New York, NY, USA, 1984. [Google Scholar]
- Yen, M.-Y.; Chiu, A.W.-H.; Schwartz, J.; King, C.-C.; Lin, Y.E.; Chang, S.-C.; Armstrong, D.; Hsueh, P.-R. From SARS in 2003 to H1N1 in 2009: Lessons learned from Taiwan in preparation for the next pandemic. J. Hosp. Infect. 2014, 87, 185–193. [Google Scholar] [CrossRef]
- Yen, M.-Y.; Schwartz, J.; Hsueh, P.-R.; Chiu, A.W.-H.; Armstrong, D. Traffic control bundling is essential for protecting healthcare workers and controlling the 2014 Ebola epidemic. Clin. Infect. Dis. 2015, 60, 823–825. [Google Scholar] [CrossRef] [Green Version]
- Cao, B.; Li, X.-W.; Mao, Y.; Wang, J.; Lu, H.-Z.; Chen, Y.-S.; Liang, Z.-A.; Liang, L.; Zhang, S.-J.; Zhang, B.; et al. Clinical features of the initial cases of 2009 pandemic influenza A (H1N1) virus infection in China. N. Engl. J. Med. 2009, 361, 2507–2517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, N.M.; Cummings, D.A.T.; Fraser, C.; Cajka, J.C.; Cooley, P.C.; Burke, D.S. Strategies for mitigating an influenza pandemic. Nature 2006, 442, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Longini, I.M.; Nizam, A.; Xu, S.; Ungchusak, K.; Hanshaoworakul, W.; Cummings, D.A.T.; Halloran, M.E. Containing pandemic influenza at the source. Science 2005, 309, 1083–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, R.E.; Kuehn, M.M.; Duckworth, A.L.; Kross, E.; Ayduk, Ö. Focusing on the future from afar: Self-distancing from future stressors facilitates adaptive coping. Emotion 2019, 19, 903–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumeister, R.F.; Vohs, K.D.; DeWall, C.N.; Zhang, L. How emotion shapes behavior: Feedback, anticipation, and reflection, rather than direct causation. Personal. Soc. Psychol. Rev. 2007, 11, 167–203. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, F.; Zhu, C.; Wang, Z. Willingness to Self-Isolate When Facing a Pandemic Risk: Model, Empirical Test, and Policy Recommendations. Int. J. Environ. Res. Public Health 2020, 17, 197. [Google Scholar] [CrossRef] [Green Version]
- Becks, L.; Milinski, M. Extortion strategies resist disciplining when higher competitiveness is rewarded with extra gain. Nat. Commun. 2019, 10, 783. [Google Scholar] [CrossRef]
- Kim, T.-H. Infections Climb in South Korea as World Fights Virus; ABC News: New York, NY, USA, 2020. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Mean/Categories | Total No. |
|---|---|---|
| Age | 30.64 ± 9.19 | 1847 |
| Gender | Males | 767 |
| Females | 1080 | |
| Education | High school | 257 |
| Junior college | 465 | |
| Bachelor | 868 | |
| Master or PhD | 257 | |
| Income | <1999 | 423 |
| 2000–3999 | 430 | |
| 4000–5999 | 423 | |
| 6000–9999 | 332 | |
| 10,000–14,999 | 156 | |
| 15,000–19,999 | 40 | |
| >20,000 | 43 | |
| Psychological Distance | 4.43 ± 2.03 | |
| Anxiety | 4.41 ± 1.05 | |
| Pandemic Severity | 174.15 ± 563.68 | |
| Lockdown | 3.71 ± 1.76 |
| Variables | Model 1 | Model 2 | Model 3 | Model 4 | Model 5a | Model 5b |
|---|---|---|---|---|---|---|
| Anxiety | Anxiety | Anxiety | Anxiety | Anxiety | PD | |
| Sex | 0.23 ** (0.04) | 0.23 ** (0.05) | 0.22 ** (0.04) | 0.22 ** (0.05) | 0.22 ** (0.04) | −0.06 (0.06) |
| Age | 0.01 (0.01) | 0.01 (0.01) | 0.01 (0.01) | 0.01 (0.01) | 0.01 (0.01) | 0.01 (0.01) |
| Education | 0.08 ** (0.03) | 0.08 ** (0.03) | 0.06 * (0.03) | 0.06 * (0.03) | 0.06 * (0.03) | −0.11 ** (0.03) |
| Income | −0.01 (0.02) | −0.01 (0.02) | −0.01 (0.02) | −0.01 (0.02) | −0.01 (0.02) | 0.01 (0.01) |
| PS | 0.06 (0.01) | 0.04 ** (0.01) | 0.04 (0.02) | 0.04 (0.02) | −0.12 ** (0.01) | |
| PD | −0.17 ** (0.02) | −0.17 ** (0.02) | −0.17 ** (0.02) | |||
| △R2 | 0.02 | 0.003 | 0.03 | 0.03 | 0.03 | 0.03 |
| Variables | Model 6 | Model 7 | Model 8 | Model 9 | Model 10a | Model 10b |
|---|---|---|---|---|---|---|
| Anxiety | Anxiety | PD | PD | Anxiety | PD | |
| Sex | 0.20 ** (0.04) | 0.23 ** (0.05) | −0.01 ** (0.05) | −0.01 ** (0.05) | 0.20 ** (0.05) | −0.01 (0.05) |
| Age | 0.01 (0.01) | 0.01 (0.01) | −0.01 (0.01) | −0.01 (0.01) | 0.01 (0.01) | −0.01 (0.01) |
| Education | 0.07 * (0.03) | 0.08 ** (0.03) | −0.10 (0.03) | −0.10 (0.03) | 0.05 (0.03) | −0.10 ** (0.03) |
| Income | −0.03 (0.02) | −0.01 (0.02) | 0.01 ** (0.02) | 0.01 ** (0.02) | −0.02 (0.02) | 0.01 (0.02) |
| PD | −0.18 ** (0.03) | |||||
| Pandemic Severity | 0.04 ** (0.01) | −0.08 (0.07) | −0.12 (0.04) | −0.02 (0.06) | 0.06 (0.04) | −0.02 (0.06) |
| Lockdown | −0.08 + (0.04) | −0.11 (0.05) | 0.08 ** (0.04) | 0.10 ** (0.04) | 0.10 ** (0.04) | |
| PS × LD | −0.11 * (0.05) | 0.10 ** (0.04) | 0.10 ** (0.04) | |||
| △R2 | 0.06 | 0.001 | 0.08 | 0.001 | 0.02 | 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, L.; Miao, M.; Lim, J.; Li, M.; Nie, S.; Zhang, X. Is Lockdown Bad for Social Anxiety in COVID-19 Regions?: A National Study in The SOR Perspective. Int. J. Environ. Res. Public Health 2020, 17, 4561. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124561
Zheng L, Miao M, Lim J, Li M, Nie S, Zhang X. Is Lockdown Bad for Social Anxiety in COVID-19 Regions?: A National Study in The SOR Perspective. International Journal of Environmental Research and Public Health. 2020; 17(12):4561. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124561
Chicago/Turabian StyleZheng, Lei, Miao Miao, JiYoon Lim, Maorui Li, Shu Nie, and Xiaojun Zhang. 2020. "Is Lockdown Bad for Social Anxiety in COVID-19 Regions?: A National Study in The SOR Perspective" International Journal of Environmental Research and Public Health 17, no. 12: 4561. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124561