Perceived Discrimination, Psychological Distress and Cardiovascular Risk in Migrants in Spain

 ,
,  ,
,
Abstract
:1. Introduction
1.1. Perceived Discrimination and Cardiovascular Risk
1.2. Health, Psychological Distress and Cardiovascular Risk
1.3. Sociodemographic Variables and Cardiovascular Risk
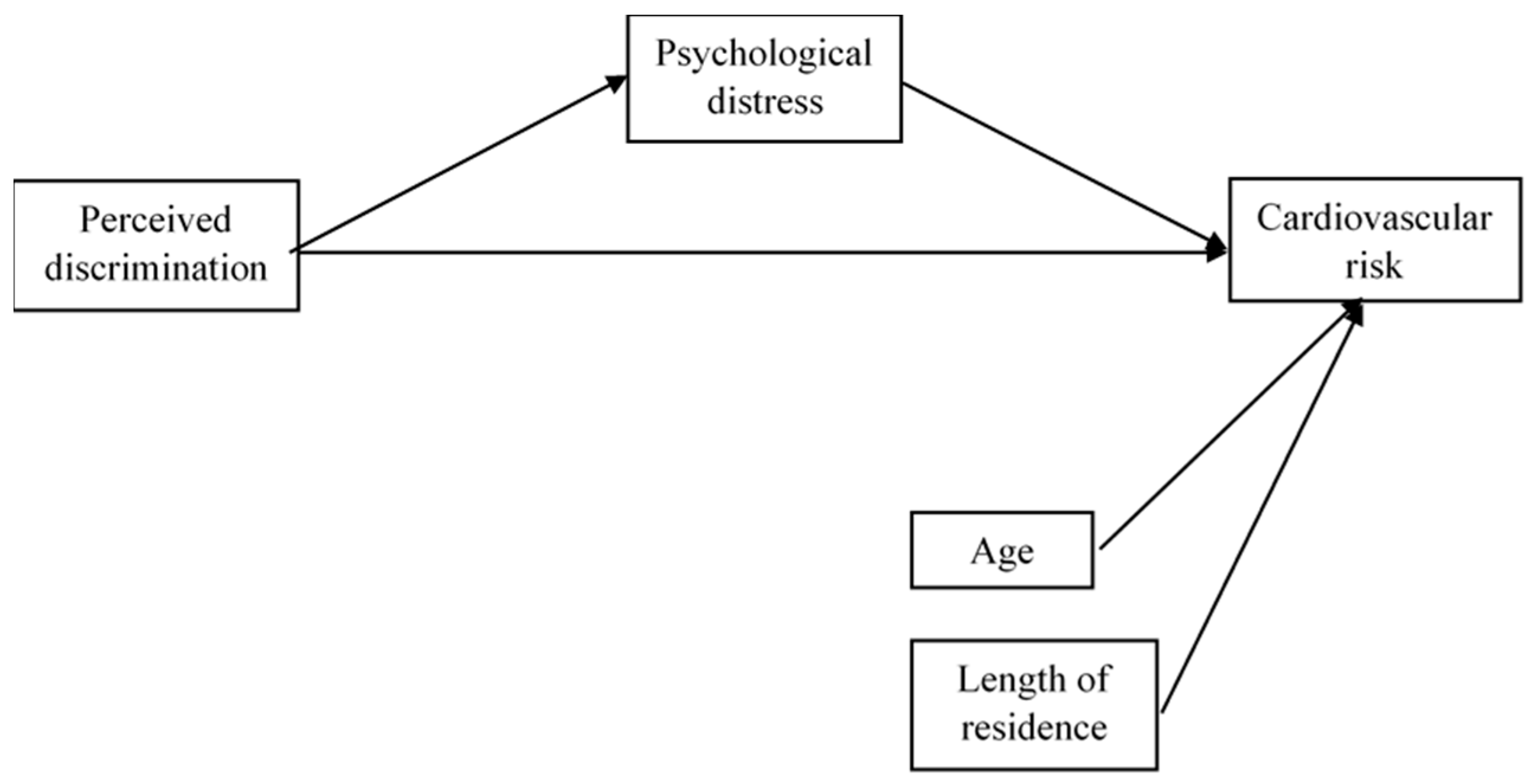
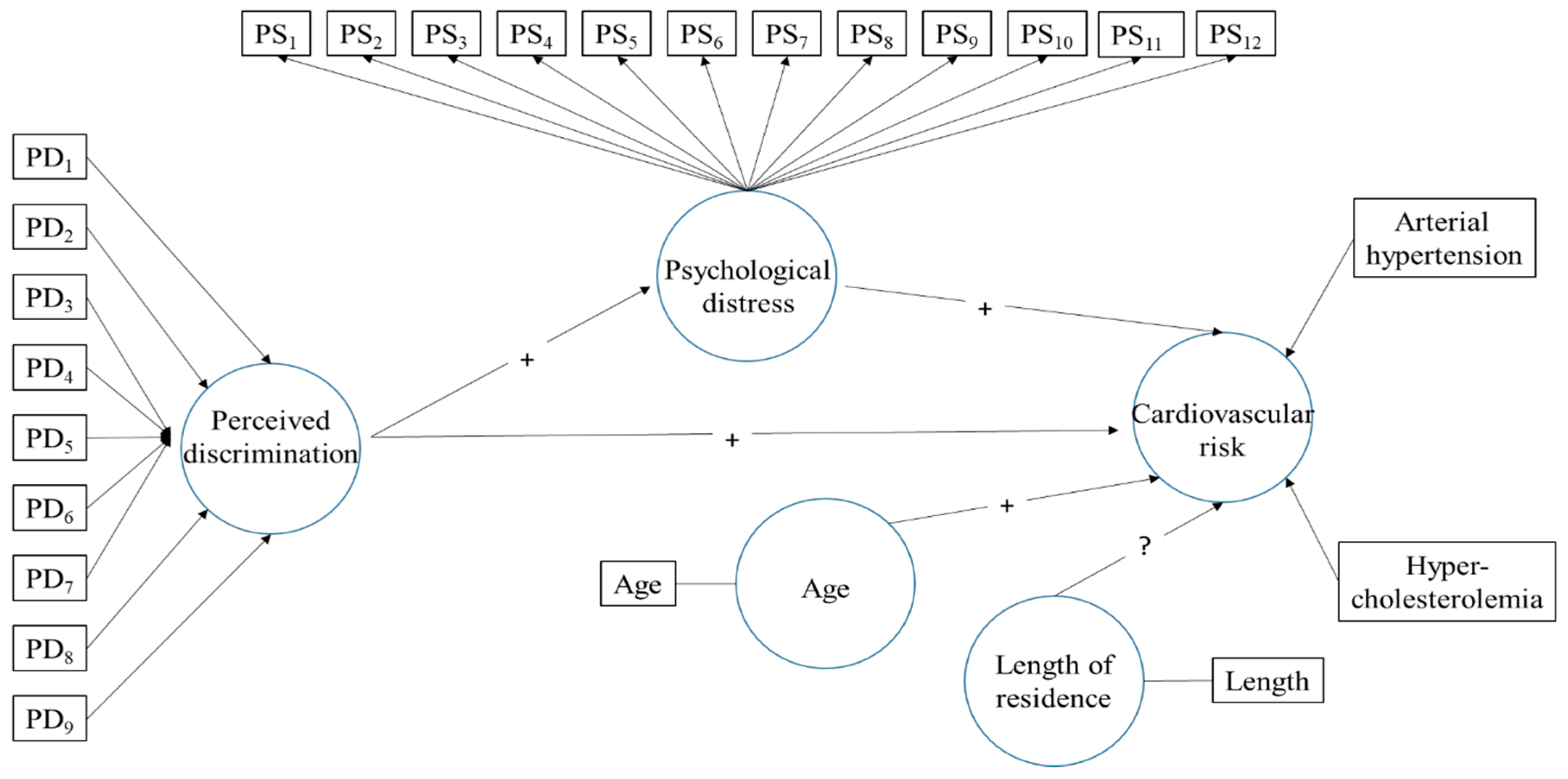
1.4. Present Study
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Data Analysis
3. Results
4. Discussion
4.1. Future Lines of Research
4.2. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kotseva, K.; Wood, D.; De Bacquer, D.; De Backer, G.; Rydén, L.; Jennings, C.; Gyberg, V.; Amouyel, P.; Bruthans, J.; Conde, A.C.; et al. EUROASPIRE IV: A European Society of Cardiology survey on the lifestyle, risk factor and therapeutic management of coronary patients from 24 European countries. Eur. J. Prev. Cardiol. 2015, 23, 636–648. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, J.W.; Whelton Seamus, P.; Blumenthal, R.S. 38—Dyslipidemia. In Hypertension: A Companion to Braunwald’s Heart Disease; Bakris, G.L., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 353–360. Available online: http://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/pii/B978032342973300038X (accessed on 10 May 2020).
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; De Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics—2017 Update: A Report From the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, M.T.; Koinis-Mitchell, D. Black immigrants and school engagement: Perceptions of discrimination, ethnic identity, and American identity. J. Black Psychol. 2014, 40, 520–538. [Google Scholar] [CrossRef]
- Lebrón, A.M.W.; Schulz, A.J.; Mentz, G.B.; Reyes, A.G.; Gamboa, C.; Israel, B.A.; Viruell-Fuentes, E.A.; House, J.S. Impact of change over time in self-reported discrimination on blood pressure: Implications for inequities in cardiovascular risk for a multi-racial urban community. Ethn. Heal. 2018, 25, 323–341. [Google Scholar] [CrossRef]
- Chilunga, F.P.; Boateng, D.; Henneman, P.; Beune, E.; Requena-Méndez, A.; Meeks, K.A.; Smeeth, L.; Addo, J.; Bahendeka, S.; Danquah, I.; et al. Perceived discrimination and stressful life events are associated with cardiovascular risk score in migrant and non-migrant populations: The RODAM study. Int. J. Cardiol. 2019, 286, 169–174. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Vable, A.M.; Glymour, M.M.; Allen, A.M. Discrimination in health care and biomarkers of cardiometabolic risk in U.S. adults. SSM Popul. Heal. 2019, 7, 100306–101006. [Google Scholar] [CrossRef]
- Havranek, E.P.; Mujahid, M.S.; Barr, D.A.; Blair, I.V.; Cohen, M.S.; Cruz-Flores, S.; Smith, G.D.; Himmelfarb, C.D.; Lauer, M.S.; Lockwood, D.W.; et al. Social Determinants of Risk and Outcomes for Cardiovascular Disease. Circulation 2015, 132, 873–898. [Google Scholar] [CrossRef] [Green Version]
- Ikram, U.Z.; Malmusi, D.; Juel, K.; Rey, G.; Kunst, A.E. Association between Integration Policies and Immigrants’ Mortality: An Explorative Study across Three European Countries. PLoS ONE 2015, 10, e0129916. [Google Scholar] [CrossRef]
- Bécares, L.; Shaw, R.J.; Nazroo, J.; Stafford, M.; Albor, C.; Atkin, K.; Kiernan, K.; Wilkinson, R.; Pickett, K. Ethnic Density Effects on Physical Morbidity, Mortality, and Health Behaviors: A Systematic Review of the Literature. Am. J. Public Heal. 2012, 102, e33–e66. [Google Scholar] [CrossRef]
- Hadgekiss, E.; Renzaho, A. The physical health status, service utilization and barriers to access care for asylum seekers residing in the community: A systematic review of the literature. Austr. Health Rev. 2014, 38, 142–159. [Google Scholar] [CrossRef]
- Kavian, F.; Mehta, K.; Willis, E.; Mwanri, L.; Ward, P.R.; Booth, S. Migration, Stress and the Challenges of Accessing Food: An Exploratory Study of the Experience of Recent Afghan Women Refugees in Adelaide, Australia. Int. J. Environ. Res. Public Heal. 2020, 17, 1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Escamilla, R.; Garcia, J.; Song, D. Health care access among Hispanic immigrants: ¿Alguien está escuchando? (Is anybody listening?). Napa Bull. 2010, 34, 47–67. [Google Scholar] [CrossRef] [Green Version]
- Son, E.; Moring, N.S.; Igdalsky, L.; Parish, S.L. Navigating the health-care system in community: Perspectives from Asian immigrant parents of children with special health-care needs. J. Child. Heal. Care 2018, 22, 251–268. [Google Scholar] [CrossRef] [PubMed]
- Tegegne, M.A. Linguistic Integration and Immigrant Health: The Longitudinal Effects of Interethnic Social Capital. J. Heal. Soc. Behav. 2018, 59, 215–230. [Google Scholar] [CrossRef] [PubMed]
- Zallman, L.; Himmelstein, D.H.; Woolhandler, S.; Bor, D.H.; Ayanian, J.Z.; Wilper, A.P.; McCormick, D. Undiagnosed and Uncontrolled Hypertension and Hyperlipidemia among Immigrants in the US. J. Immigr. Minor. Heal. 2012, 15, 858–865. [Google Scholar] [CrossRef] [Green Version]
- Levin-Zamir, D.; Leung, A.Y.; Dodson, S.; Rowlands, G. Health literacy in selected populations: Individuals, families, and communities from the international and cultural perspective. Inf. Serv. Use 2017, 37, 131–151. [Google Scholar] [CrossRef] [Green Version]
- Lorini, C.; Caini, S.; Ierardi, F.; Bachini, L.; Gemmi, F.; Bonaccorsi, G. Health Literacy as a Shared Capacity: Does the Health Literacy of a Country Influence the Health Disparities among Immigrants? Int. J. Environ. Res. Public Heal. 2020, 17, 1149. [Google Scholar] [CrossRef] [Green Version]
- Han, W.; Siegel, J.; Zhang, L. The response to rural-to-urban migration and other life stressors in shanghai: Effects on physical and psychological well-being among parents of young children. Asian Am. J. Psychol. 2017, 8, 248–258. [Google Scholar] [CrossRef]
- Garcini, L.M.; Murray, K.E.; Zhou, A.; Klonoff, E.A.; Myers, M.G.; Elder, J.P. Mental Health of Undocumented Immigrant Adults in the United States: A Systematic Review of Methodology and Findings. J. Immigr. Refug. Stud. 2016, 14, 1–25. [Google Scholar] [CrossRef]
- Rosenthal, T. The effect of migration on hypertension and other cardiovascular risk factors: A review. J. Am. Soc. Hypertens. 2014, 8, 171–191. [Google Scholar] [CrossRef]
- Agyei, B.; Nicolaou, M.; Boateng, L.; Dijkshoorn, H.; Born, B.J.H.V.D.; Agyemang, C. Relationship between psychosocial stress and hypertension among Ghanaians in Amsterdam, the Netherlands—The GHAIA study. BMC Public Heal. 2014, 14, 692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Severino, P.; Mariani, M.V.; Maraone, A.; Piro, A.; Ceccacci, A.; Tarsitani, L.; Maestrini, V.; Mancone, M.; LaValle, C.; Pasquini, M.; et al. Triggers for Atrial Fibrillation: The Role of Anxiety. Cardiol. Res. Pr. 2019, 2019, 1208505–1208515. [Google Scholar] [CrossRef] [PubMed]
- GBD 2013 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet Lond. 2015, 386, 2287.
- Severino, P.; Netti, L.; Mariani, M.V.; Maraone, A.; D’Amato, A.; Scarpati, R.; Infusino, F.; Pucci, M.; LaValle, C.; Maestrini, V.; et al. Prevention of Cardiovascular Disease: Screening for Magnesium Deficiency. Cardiol. Res. Pr. 2019, 2019, 4874921–48749310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qu, X.; Jin, F.; Hao, Y.; Li, H.; Tang, T.; Wang, H.; Yan, W.; Dai, K. Magnesium and the Risk of Cardiovascular Events: A Meta-Analysis of Prospective Cohort Studies. PLoS ONE 2013, 8, e57720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, B.J.; Rucklidge, J.J.; Romijn, A.; McLeod, K. The Emerging Field of Nutritional Mental Health. Clin. Psychol. Sci. 2015, 3, 964–980. [Google Scholar] [CrossRef] [Green Version]
- Miller, G.E.; Cole, S.W. Clustering of Depression and Inflammation in Adolescents Previously Exposed to Childhood Adversity. Biol. Psychiatry 2012, 72, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Brummett, B.; Babyak, M.A.; Siegler, I.C.; Shanahan, M.; Harris, K.M.; Elder, G.H.; Williams, R.B. Systolic blood pressure, socioeconomic status, and biobehavioral risk factors in a nationally representative US young adult sample. Hypertension 2011, 58, 161–166. [Google Scholar] [CrossRef]
- Commodore-Mensah, Y.; Matthie, N.; Wells, J.; Dunbar, S.B.; Himmelfarb, C.D.; Cooper, L.A.; Chandler, R.D. African Americans, African Immigrants, and Afro-Caribbeans Differ in Social Determinants of Hypertension and Diabetes: Evidence from the National Health Interview Survey. J. Racial Ethn. Heal. Disparities 2017, 5, 995–1002. [Google Scholar] [CrossRef]
- Agyemang, C.; Bindraban, N.; Mairuhu, G.; Van Montfrans, G.; Koopmans, R.; Stronks, K. Prevalence, awareness, treatment, and control of hypertension among Black Surinamese, South Asian Surinamese and White Dutch in Amsterdam, The Netherlands: The SUNSET study. J. Hypertens. 2005, 23, 1971–1977. [Google Scholar] [CrossRef]
- Mars, N.; Gen, F.; Koskela, J.T.; Ripatti, P.; Kiiskinen, T.; Havulinna, A.S.; Lindbohm, J.V.; Ahola-Olli, A.; Kurki, M.; Karjalainen, J.; et al. Polygenic and clinical risk scores and their impact on age at onset and prediction of cardiometabolic diseases and common cancers. Nat. Med. 2020, 26, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Bernabe-Ortiz, A.; Benziger, C.P.; Gilman, R.H.; Smeeth, L.; Miranda, J.J. Sex Differences in Risk Factors for Cardiovascular Disease: The PERU MIGRANT Study. PLoS ONE 2012, 7, e35127. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N.; Smith, K.; Naishadham, D.; Hartman, C.; Barbeau, E.M. Experiences of discrimination: Validity and reliability of a self-report measure for population health research on racism and health. Soc. Sci. Med. 2005, 61, 1576–1596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González, I.C.V.; Arboleda, C.Z.; Roldan, L.F.R. Propiedades psicométricas del Cuestionario de Salud General de Goldberg GHQ-12 en una institución hospitalaria de la ciudad de Medellín. Av. Psicol. Latinoam. 2013, 31, 532–545. [Google Scholar]
- 2019. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176951&menu=ultiDatos&idp=1254735572981 (accessed on 1 April 2020).
- Ringle, C.M.; Wende, S.; Becker, J.M. SmartPLS 3, Boenningstedt: SmartPLS GmbH. 2015. Available online: http://www.smartpls.com (accessed on 1 April 2020).
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM), 2nd ed.; Sage Publications Inc.: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Bak-Klimek, A.; Karatzias, T.; Elliott, L.; MacLean, R. The Determinants of Well-Being Among International Economic Immigrants: A Systematic Literature Review and Meta-Analysis. Appl. Res. Qual. Life 2014, 10, 161–188. [Google Scholar] [CrossRef] [Green Version]
- García-Cid, A.; Hombrados-Mendieta, I.; Gómez-Jacinto, L.; García, M.D.L.O.P.; Millán-Franco, M. Apoyo social, resiliencia y región de origen en la salud mental y la satisfacción vital de los inmigrantes. Univ. Psychol. 2018, 16, 1–14. [Google Scholar] [CrossRef]
- Guruge, S.; Thomson, M.S.; George, U.; Chaze, F. Social support, social conflict, and immigrant women’s mental health in a Canadian context: A scoping review. J. Psychiatr. Ment. Heal. Nurs. 2015, 22, 655–667. [Google Scholar] [CrossRef]
- Hombrados-Mendieta, I.; Millán-Franco, M.; Gómez-Jacinto, L.; Gonzalez-Castro, F.; Martos-Méndez, M.J.; García-Cid, A. Positive Influences of Social Support on Sense of Community, Life Satisfaction and the Health of Immigrants in Spain. Front. Psychol. 2019, 10, 10. [Google Scholar] [CrossRef]
- Millán-Franco, M.; Gómez-Jacinto, L.; Hombrados-Mendieta, I.; García-Cid, A. Las redes de apoyo social online y offline en los inmigrantes de Málaga (España). Migracion. Publ. Inst. Univ. Estud. Sobre Migr. 2019, 47, 119–149. [Google Scholar] [CrossRef]
- Fox, R.S.; Carnethon, M.R.; Gallo, L.C.; Wiley, J.F.; Isasi, C.R.; Daviglus, M.L.; Cai, J.; Davis, S.M.; Giachello, A.L.; Gonzalez, P.; et al. Perceived Discrimination and Cardiometabolic Risk Among US Hispanics/Latinos in the HCHS/SOL Sociocultural Ancillary Study. Int. J. Behav. Med. 2019, 26, 331–342. [Google Scholar] [CrossRef]
- Wagner, J.; Tennen, H.; Feinn, R.; Osborn, C. Self-reported discrimination, diabetes distress, and continuous blood glucose in women with type 2 diabetes. J. Immigr. Minor. Heal. 2015, 17, 566–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolezsar, C.M.; McGrath, J.J.; Herzig, A.J.M.; Miller, S.B. Perceived racial discrimination and hypertension: A comprehensive systematic review. Heal. Psychol. 2014, 33, 20–34. [Google Scholar] [CrossRef] [PubMed]
- McClure, H.H.; Snodgrass, J.J.; Martinez, C.R.; Squires, E.C.; Jiménez, R.A.; Isiordia, L.E.; Eddy, J.M.; McDade, T.W.; Small, J. Stress, Place, and Allostatic Load Among Mexican Immigrant Farmworkers in Oregon. J. Immigr. Minor. Heal. 2015, 17, 1518–1525. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Denier, N.; Wang, J.S.-H.; Kaushal, N. Unhealthy assimilation or persistent health advantage? A longitudinal analysis of immigrant health in the United States. Soc. Sci. Med. 2017, 195, 105–114. [Google Scholar] [CrossRef] [Green Version]
- Commodore-Mensah, Y.; Ukonu, N.; Obisesan, O.; Aboagye, J.K.; Agyemang, C.; Reilly, C.M.; Dunbar, S.B.; Okosun, I.S. Length of Residence in the United States is Associated With a Higher Prevalence of Cardiometabolic Risk Factors in Immigrants: A Contemporary Analysis of the National Health Interview Survey. J. Am. Hear. Assoc. 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Lê-Scherban, F.; Albrecht, S.S.; Bertoni, A.G.; Kandula, N.; Mehta, N.; Roux, A.V.D. Immigrant status and cardiovascular risk over time: Results from the Multi-Ethnic Study of Atherosclerosis. Ann. Epidemiol. 2016, 26, 429–435. [Google Scholar] [CrossRef] [Green Version]
- Zemrak, F.; Ambale-Venkatesh, B.; Captur, G.; Chrispin, J.; Chamera, E.; Habibi, M.; Nazarian, S.A.; Mohiddin, S.; Moon, J.C.E.; Petersen, S.; et al. Left Atrial Structure in Relationship to Age, Sex, Ethnicity, and Cardiovascular Risk Factors: MESA (Multi-Ethnic Study of Atherosclerosis). Circ. Cardiovasc. Imaging 2017, 10, 005379. [Google Scholar] [CrossRef] [Green Version]
- Urzúa, A.; Basabe, N.; Pizarro, J.J.; Ferrer-Urbina, R. Afrontamiento del estrés por aculturación: Inmigrantes latinos en Chile. Univ. Psychol. 2018, 16, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Pucci, G.; Alcidi, R.; Tap, L.; Battista, F.; Mattace-Raso, F.; Schillaci, G. Sex- and gender-related prevalence, cardiovascular risk and therapeutic approach in metabolic syndrome: A review of the literature. Pharmacol. Res. 2017, 120, 34–42. [Google Scholar] [CrossRef]
- Sims, M.; Diez-Roux, A.V.; Dudley, A.; Gebreab, S.; Wyatt, S.B.; Bruce, M.A.; James, S.A.; Robinson, J.C.; Williams, D.R.; Taylor, H.A. Perceived Discrimination and Hypertension Among African Americans in the Jackson Heart Study. Am. J. Public Heal. 2012, 102, S258–S265. [Google Scholar] [CrossRef]
- Williams, D.R.; Collins, C. Racial residential segregation: A fundamental cause of racial disparities in health. Public Health Reports 2016. [Google Scholar] [CrossRef]
- Albright, A.L.; Gregg, E.W. Preventing type 2 diabetes in communities across the U.S.: The National Diabetes Prevention Program. Am. J. Prev. Med. 2013, 44, S346–S351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukherjea, A.; Morgan, P.A.; Snowden, L.R.; Ling, P.M.; Ivey, S.L. Social and cultural influences on tobacco-related health disparities among South Asians in the USA. Tob. Control. 2011, 21, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Kokab, F.; Greenfield, S.; Lindenmeyer, A.; Sidhu, M.; Tait, L.; Gill, P. The experience and influence of social support and social dynamics on cardiovascular disease prevention in migrant Pakistani communities: A qualitative synthesis. Patient Educ. Couns. 2018, 101, 619–630. [Google Scholar] [CrossRef] [Green Version]
- Chun, K.M.; Chesla, C.A.; Kwan, C.M. “So We Adapt Step by Step”: Acculturation experiences affecting diabetes management and perceived health for Chinese American immigrants. Soc. Sci. Med. 2010, 72, 256–264. [Google Scholar] [CrossRef] [Green Version]
- Beune, E.A.; Haafkens, J.; Agyemang, C.E.; Bindels, P.J. Inhibitors and enablers of physical activity in multiethnic hypertensive patients: Qualitative study. J. Hum. Hypertens. 2009, 24, 280–290. [Google Scholar] [CrossRef]
- Zlotnick, C.; Goldblatt, H.; Shadmi, E.; Birenbaum-Carmeli, D.; Taychaw, O. A qualitative study assessing cardiovascular risk factors: The accumulative stressors influencing societal integration of teenage African immigrants. BMC Public Heal. 2015, 15, 785. [Google Scholar] [CrossRef] [Green Version]
- Alegría, M.; Alvarez, K.; DiMarzio, K. Immigration and Mental Health. Curr. Epidemiol. Rep. 2017, 4, 145–155. [Google Scholar] [CrossRef]
- Salinero-Fort, M.A.; Gómez-Campelo, P.; Bragado-Álvarez, C.; Abánades-Herranz, J.C.; Jiménez-García, R.; De Burgos-Lunar, C. Health-Related Quality of Life of Latin-American Immigrants and Spanish-Born Attended in Spanish Primary Health Care: Socio-Demographic and Psychosocial Factors. PLoS ONE 2015, 10, e0122318. [Google Scholar] [CrossRef]
- Fernández, I.; Silván-Ferrero, P.; Molero, F.; Gaviria, E.; Garcia-Ael, C. Perceived Discrimination and Well-Being in Romanian Immigrants: The Role of Social Support. J. Happiness Stud. 2014, 16, 857–870. [Google Scholar] [CrossRef]
- Salinas, J.J.; Abdelbary, B.; Rentfro, A.; Fisher-Hoch, S.; McCormick, J.B. Cardiovascular Disease Risk Among the Mexican American Population in the Texas-Mexico Border Region, by Age and Length of Residence in United States. Prev. Chronic Dis. 2014, 11, 130253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatt, J.M.; Alexander, R.; Emond, A.; Foster, K.; Hadfield, K.; Mason-Jones, A.; Reid, S.; Theron, L.; Ungar, M.; Wouldes, T.A.; et al. Trauma, Resilience, and Mental Health in Migrant and Non-Migrant Youth: An International Cross-Sectional Study Across Six Countries. Front. Psychol. 2020, 10, 997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giordano, F.; Cipolla, A.; Ragnoli, F.; Bruno, F.B. Transit Migration and Trauma: The Detrimental Effect of Interpersonal Trauma on Syrian Children in Transit in Italy. Psychol. Inj. Law 2019, 12, 76–87. [Google Scholar] [CrossRef]
- Official College of Psychologists. Guidance for Psychological Intervention with Immigrants and Refugees; Cop Madrid: Madrid, Spain, 2016. [Google Scholar]
- Constant, A.F. The healthy immigrant paradox and health convergence. CESifo Working Paper Series No. 6692. 2017. Available online: https://ssrn.com/abstract=3074307 (accessed on 1 April 2020).
- Borrell, C.; Muntaner, C.; Gil-González, D.; Artazcoz, L.; Rodríguez-Sanz, M.; Rohlfs, I.; Pérez, A.K.; García-Calvente, M.; Villegas, R.; Álvarez-Dardet, C. Perceived discrimination and health by gender, social class, and country of birth in a Southern European country. Prev. Med. 2010, 50, 86–92. [Google Scholar] [CrossRef]
- Sevillano, V.; Basabe, N.; Bobowik, M.; Aierdi, X. Health-related quality of life, ethnicity and perceived discrimination among immigrants and natives in Spain. Ethn. Heal. 2013, 19, 178–197. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Latent Variable | Indicators | Loadings | t Value | p Value | 95% Confidence Interval | Indicator Reliability | Items | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Psychological Distress | PS1 | 0.373 | 11.631 | 0.000 | 0.309 | 0.434 | 0.139 | Have you been able to concentrate well? |
| PS2 | 0.690 | 35.421 | 0.000 | 0.649 | 0.726 | 0.476 | Have your concerns made you lose much sleep? | |
| PS3 | 0.619 | 26.545 | 0.000 | 0.569 | 0.662 | 0.383 | Have you felt you are leading a useless life? | |
| PS4 | 0.628 | 27.596 | 0.000 | 0.581 | 0.670 | 0.394 | Have you felt unable to make decisions? | |
| PS5 | 0.578 | 26.044 | 0.000 | 0.532 | 0.619 | 0.334 | Have you felt constantly stressed and under tension? | |
| PS6 | 0.586 | 24.595 | 0.000 | 0.536 | 0.630 | 0.343 | Have you had the feeling of not being able to overcome difficulties? | |
| PS7 | 0.463 | 16.082 | 0.000 | 0.406 | 0.517 | 0.214 | Have you been able to enjoy everyday activities? | |
| PS8 | 0.647 | 33.321 | 0.000 | 0.606 | 0.682 | 0.418 | Have you been able to face your problems appropriately? | |
| PS9 | 0.689 | 40.245 | 0.000 | 0.653 | 0.721 | 0.475 | Have you felt unhappy or depressed? | |
| PS10 | 0.584 | 25.032 | 0.000 | 0.536 | 0.628 | 0.341 | Have you lost confidence in yourself? | |
| PS11 | 0.571 | 23.887 | 0.000 | 0.521 | 0.615 | 0.326 | Have you felt like a useless person? | |
| PS12 | 0.743 | 49.599 | 0.000 | 0.711 | 0.770 | 0.552 | Do you feel reasonably happy considering all circumstances? | |
| AVE = 0.370 | 34.953 | 0.000 | 0.349 | 0.391 | ||||
| Composite Reliability = 0.873 | 164.924 | 0.000 | 0.862 | 0.883 | ||||
| Rho A = 0.858 | 128.750 | 0.000 | 0.845 | 0.871 | ||||
| Cronbach’s Alpha = 0.844 | 121.381 | 0.000 | 0.830 | 0.857 | ||||
| Formative Constructs | Formative Indicators | Outer Weights | Outer Loadings | t Value | p Value | 95% Confidence Interval | Items | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Perceived Discrimination | PD1 | 0.340 | 0.771 | 3.625 | 0.000 | 0.149 | 0.510 | Work environment (access to work, salary, promotion, training, dismissal, balancing work and family life) |
| PD2 | 0.410 | 0.812 | 4.273 | 0.000 | 0.212 | 0.585 | Access to public services (education, health care, subsidies, means of transport) | |
| PD3 | 0.085 | 0.649 | 0.915 | 0.360 | −0.099 | 0.271 | Attention and treatment from the Public Administration (citizen’s assistance offices, information, civil servants) | |
| PD4 | 0.049 | 0.536 | 0.548 | 0.584 | −0.131 | 0.223 | Treatment by the police | |
| PD5 | 0.138 | 0.676 | 1.452 | 0.147 | −0.052 | 0.320 | Access to housing | |
| PD6 | 0.250 | 0.672 | 2.676 | 0.007 | 0.060 | 0.425 | At shops, bars and other private services | |
| PD7 | −0.062 | 0.243 | 0.524 | 0.600 | −0.294 | 0.174 | In your family (from your partner) | |
| PD8 | 0.040 | 0.292 | 0.360 | 0.719 | −0.177 | 0.248 | In your family (from someone who is not your partner) | |
| PD9 | 0.048 | 0.645 | 0.501 | 0.617 | −0.141 | 0.237 | In the street, treatment from people | |
| Cardiovascular Risk | Hypertension | 0.686 | 0.822 | 11.600 | 0.000 | 0.564 | 0.794 | Arterial hypertension |
| Cholesterol | 0.586 | 0.745 | 8.956 | 0.000 | 0.452 | 0.707 | Hypercholesterolemia | |
| Effects | Path Coefficients | t Value | p Value | 95% Confidence Intervals | Significance (p < 0.05)? ** | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Total | ||||||
| Direct effect | ||||||
| Perceived Discrimination → Psychological Distresss | 0.363 | 13.701 | 0.000 | 0.320 | 0.423 * | Yes |
| Perceived Discrimination → Cardiovascular Risk | 0.134 | 4.272 | 0.000 | 0.074 | 0.198 * | Yes |
| Psychological Distresss → Cardiovascular Risk | 0.118 | 4.353 | 0.000 | 0.063 | 0.171 * | Yes |
| Age → Cardiovascular Risk | 0.275 | 10.607 | 0.000 | 0.223 | 0.324 * | Yes |
| Length of Residence → Cardiovascular Risk | 0.020 | 0.611 | 0.541 | −0.044 | 0.084 | No |
| Indirect effect | ||||||
| Perceived Discrimination → Psychological Distresss → Cardiovascular Risk | 0.043 | 4.027 | 0.000 | 0.023 | 0.065 * | Yes |
| Africa | ||||||
| Direct effect | ||||||
| Perceived Discrimination → Psychological Distresss | 0.385 | 9.616 | 0.000 | 0.334 | 0.491 * | Yes |
| Perceived Discrimination → Cardiovascular Risk | 0.127 | 2.221 | 0.026 | 0.024 | 0.248 * | Yes |
| Psychological Distresss → Cardiovascular Risk | 0.107 | 2.141 | 0.032 | 0.004 | 0.200 * | Yes |
| Age → Cardiovascular Risk | 0.293 | 6.328 | 0.000 | 0.197 | 0.380 * | Yes |
| Length of Residence → Cardiovascular Risk | −0.030 | 0.505 | 0.614 | −0.141 | 0.086 | No |
| Indirect effect | ||||||
| Perceived Discrimination → Psychological Distresss → Cardiovascular Risk | 0.041 | 1.973 | 0.048 | 0.002 | 0.085 * | Yes |
| Latin America | ||||||
| Direct effect | ||||||
| Perceived Discrimination → Psychological Distresss | 0.377 | 8.707 | 0.000 | 0.310 | 0.479 * | Yes |
| Perceived Discrimination → Cardiovascular Risk | 0.213 | 3.453 | 0.001 | 0.093 | 0.333 * | Yes |
| Psychological Distresss → Cardiovascular Risk | 0.116 | 2.569 | 0.010 | 0.025 | 0.198 * | Yes |
| Age → Cardiovascular Risk | 0.290 | 6.808 | 0.000 | 0.206 | 0.370 * | Yes |
| Length of Residence → Cardiovascular Risk | 0.148 | 2.869 | 0.004 | 0.041 | 0.245 * | Yes |
| Indirect effect | ||||||
| Perceived Discrimination → Psychological Distresss → Cardiovascular Risk | 0.044 | 2.283 | 0.022 | 0.010 | 0.085 * | Yes |
| Europe | ||||||
| Direct effect | ||||||
| Perceived Discrimination → Psychological Distresss | 0.395 | 7.274 | 0.000 | 0.301 | 0.516 * | Yes |
| Perceived Discrimination → Cardiovascular Risk | 0.112 | 1.269 | 0.204 | −0.054 | 0.286 | No |
| Psychological Distresss → Cardiovascular Risk | 0.109 | 2.022 | 0.043 | 0.000 | 0.210 | No |
| Age → Cardiovascular Risk | 0.254 | 4.997 | 0.000 | 0.149 | 0.348 * | Yes |
| Length of Residence → Cardiovascular Risk | −0.052 | 1.072 | 0.284 | −0.145 | 0.048 | No |
| Indirect effect | ||||||
| Perceived Discrimination → Psychological Distresss → Cardiovascular Risk | 0.043 | 1.894 | 0.058 | 0.000 | 0.090 | No |
| Women | ||||||
| Direct effect | ||||||
| Perceived Discrimination → Psychological Distresss | 0.341 | 8.346 | 0.000 | 0.272 | 0.432 * | Yes |
| Perceived Discrimination → Cardiovascular Risk | 0.186 | 3.413 | 0.001 | 0.085 | 0.303 * | Yes |
| Psychological Distresss → Cardiovascular Risk | 0.116 | 3.300 | 0.001 | 0.044 | 0.184 * | Yes |
| Age → Cardiovascular Risk | 0.258 | 7.052 | 0.000 | 0.185 | 0.328 * | Yes |
| Length of Residence → Cardiovascular Risk | −0.029 | 0.621 | 0.535 | −0.117 | 0.067 | No |
| Indirect effect | ||||||
| Perceived Discrimination → Psychological Distresss → Cardiovascular Risk | 0.040 | 2.952 | 0.003 | 0.015 | 0.068 * | Yes |
| Men | ||||||
| Direct effect | ||||||
| Perceived Discrimination → Psychological Distresss | 0.404 | 11.498 | 0.000 | 0.354 | 0.491 * | Yes |
| Perceived Discrimination → Cardiovascular Risk | 0.067 | 1.439 | 0.150 | −0.023 | 0.163 | No |
| Psychological Distresss → Cardiovascular Risk | 0.143 | 3.218 | 0.001 | 0.052 | 0.226 * | Yes |
| Age → Cardiovascular Risk | 0.293 | 8.051 | 0.000 | 0.220 | 0.363 * | Yes |
| Length of Residence → Cardiovascular Risk | 0.066 | 1.420 | 0.156 | −0.023 | 0.159 | No |
| Indirect effect | ||||||
| Perceived Discrimination → Psychological Distresss → Cardiovascular Risk | 0.058 | 2.969 | 0.003 | 0.022 | 0.098 * | Yes |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martos-Méndez, M.J.; García-Cid, A.; Gómez-Jacinto, L.; Hombrados-Mendieta, I. Perceived Discrimination, Psychological Distress and Cardiovascular Risk in Migrants in Spain. Int. J. Environ. Res. Public Health 2020, 17, 4601. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124601
Martos-Méndez MJ, García-Cid A, Gómez-Jacinto L, Hombrados-Mendieta I. Perceived Discrimination, Psychological Distress and Cardiovascular Risk in Migrants in Spain. International Journal of Environmental Research and Public Health. 2020; 17(12):4601. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124601
Chicago/Turabian StyleMartos-Méndez, María José, Alba García-Cid, Luis Gómez-Jacinto, and Isabel Hombrados-Mendieta. 2020. "Perceived Discrimination, Psychological Distress and Cardiovascular Risk in Migrants in Spain" International Journal of Environmental Research and Public Health 17, no. 12: 4601. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124601