Comparison of Patients’ Perceived Quality of Primary Care Between Urban and Rural Community Health Centers in Guangdong, China

Abstract
:1. Introduction
2. Methods
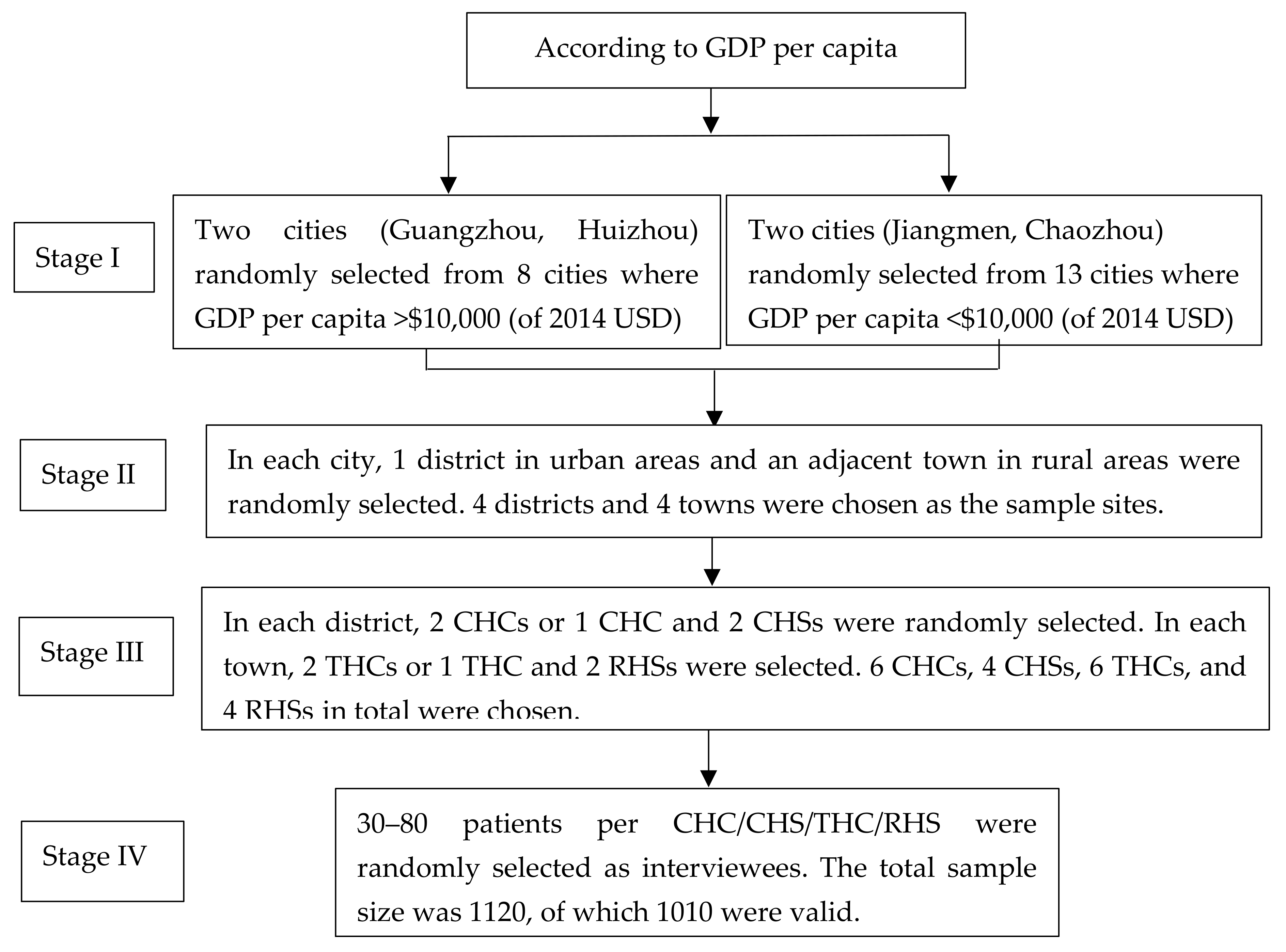
2.1. Study Site
2.2. Study Design and Participants
2.3. Data Collection
2.4. Data Analysis
2.5. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Starfield, B. Is primary care essential? Lancet 1994, 344, 1129–1133. [Google Scholar] [CrossRef]
- World Health Organization. The World Health Report 2008: Primary Health Care Now More Than Ever. Available online: http://www.who.int/whr/2008/en/index.html (accessed on 5 December 2008).
- Hutchison, B.; Levesque, J.F.; Strumpf, E.; Coyle, M. Primary Health Care in Canada: Systems in Motion. Milbank Q. 2011, 89, 256–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, L.; Stevens, G.D. The Role of Community Health Centers in Delivering Primary Care to the Underserved: Experiences of the Uninsured and Medicaid Insured. J. Ambul. Care Manag. 2007, 30, 159–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kousgaard, M.B.; Joensen, A.S.; Thorsen, T. The challenges of boundary spanners in supporting inter-organizational collaboration in primary care-a qualitative study of general practitioners in a new role. BMC Fam. Pract. 2015, 16, 17. [Google Scholar] [CrossRef] [Green Version]
- Politzer, R.M.; Yoon, J.; Shi, L.; Hughes, R.G.; Regan, J.; Gaston, M.H. Inequality in America: The Contribution of Health Centers in Reducing and Eliminating Disparities in Access to Care. Med. Care Res. Rev. 2001, 58, 234–248. [Google Scholar] [CrossRef]
- Shi, L.; Starfield, B. Primary Care, Income Inequality, and Self-Rated Health in the United States: A Mixed-Level Analysis. Int. J. Health Serv. 2000, 30, 541–555. [Google Scholar] [CrossRef]
- Hespe, C.; Rychetnik, L.; Peiris, D.; Harris, M. Informing implementation of quality improvement in Australian primary care. BMC Health Serv. Res. 2018, 18, 287. [Google Scholar] [CrossRef] [Green Version]
- Thomas, S.L.; Wakerman, J.; Humphreys, J.S. Ensuring equity of access to primary health care in rural and remote Australia—What core services should be locally available? Int. J. Equity Health 2015, 14, 111. [Google Scholar] [CrossRef] [Green Version]
- Yip, W.; Hsiao, W. China’s health care reform: A tentative assessment. China Econ. Rev. 2009, 20, 613–619. [Google Scholar] [CrossRef]
- Shi, L.; Makinen, M.; Lee, D.C.; Kidane, R.; Blanchet, N.; Liang, H.; Li, J.; Lindelow, M.; Wang, H.; Xie, S.; et al. Integrated care delivery and health care seeking by chronically-ill patients—A case-control study of rural Henan province, China. Int. J. Equity Health 2015, 14, 98. [Google Scholar] [CrossRef] [Green Version]
- Yip, W.C.; Hsiao, W.C.; Chen, W.; Hu, S.; Ma, J.; Maynard, A. Early appraisal of China’s huge and complex health-care reforms. Lancet 2012, 379, 833–842. [Google Scholar] [CrossRef]
- Li, X.; Lu, J.; Hu, S.; Cheng, K.K.; De Maeseneer, J.; Meng, Q.; Mossialos, E.; Xu, D.R.; Yip, W.; Zhang, H.; et al. The primary health-care system in China. Lancet 2017, 390, 2584–2594. [Google Scholar] [CrossRef]
- Tourigny, A.; Aubin, M.; Haggerty, J.; Bonin, L.; Morin, D.; Reinharz, D.; Leduc, Y.; St-Pierre, M.; Houle, N.; Giguère, A.; et al. Patients’ perceptions of the quality of care after primary care reform. Can. Fam. Physician 2010, 56, e273–e282. [Google Scholar] [PubMed]
- Hu, R.; Liao, Y.; Du, Z.; Hao, Y.; Liang, H.; Shi, L. Types of health care facilities and the quality of primary care: A study of characteristics and experiences of Chinese patients in Guangdong Province, China. BMC Health Serv. Res. 2016, 16, 335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Center for Health Statistics and Information. An Analysis Report of National Health Services Survey in China, 2013; Peking Union Medical College Press: Peking, China, 2016; pp. 36–41. [Google Scholar]
- Shi, L.; Starfield, B.; Xu, J.; Politzer, R.; Regan, J. Primary care quality: Community health centre and health maintenance organization. South. Med. J. 2003, 96, 787–795. [Google Scholar] [CrossRef] [PubMed]
- D’Avila, O.P.; Pinto, L.F.; Hauser, L.; Gonçalves, M.R.; Harzheim, E. The use of the Primary Care Assessment Tool (PCAT): An integrative review and proposed update. Cienc. Saude Coletiva 2017, 22, 855–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macinko, J.; Almeida, C.; de Sá, P.K. A rapid assessment methodology for the evaluation of primary care organization and performance in Brazil. Health Policy Plan. 2007, 22, 167–177. [Google Scholar] [CrossRef] [Green Version]
- Haggerty, J.L.; Pineault, R.; Beaulieu, M.D.; Brunelle, Y.; Gauthier, J.; Goulet, F.; Rodrigue, J. Room for improvement: Patients’ experiences of primary care in Quebec before major reforms. Can. Fam. Physician 2007, 53, 1057. [Google Scholar]
- Bresick, G.F.; Sayed, A.R.; Le Grange, C.; Bhagwan, S.; Manga, N.; Hellenberg, D. Western Cape Primary Care Assessment Tool (PCAT) study: Measuring primary care organisation and performance in the Western Cape Province, South Africa (2013). Afr. J. Prim. Health Care Fam. Med. 2016, 8, e1–e12. [Google Scholar] [CrossRef]
- Ameh, S.; Gómez-Olivé, F.X.; Kahn, K.; Tollman, S.M.; Klipstein-Grobusch, K. Relationships between structure, process and outcome to assess the quality of integrated chronic disease management in a rural South African setting: Applying a structural equation model. BMC Health Serv. Res. 2017, 17, 229. [Google Scholar] [CrossRef] [Green Version]
- Aoki, T.; Inoue, M.; Nakayama, T. Development and validation of the Japanese version of Primary Care Assessment Tool. Fam. Pract. 2016, 33, 112–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Choi, Y.J.; Sung, N.J.; Kim, S.Y.; Chung, S.H.; Kim, J.; Jeon, T.H.; Park, H.K. Korean Primary Care Research Group: Development of the Korean primary care assessment tool—Measuring user experience: Tests of data quality and measurement performance. Int. J. Qual. Health Care 2009, 21, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Mei, J.; Liang, Y.; Shi, L.; Zhao, J.; Wang, Y.; Kuang, L. The Development and Validation of a Rapid Assessment Tool of Primary Care in China. BioMed Res. Int. 2016, 2016, 6019603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.; Shi, L.; Lebrun, L.A.; Zhou, X.; Liu, J.; Wang, H. Development of the Chinese primary care assessment tool: Data quality and measurement properties. Int. J. Qual. Health Care 2013, 25, 92–105. [Google Scholar] [CrossRef] [Green Version]
- Zou, Y.; Zhang, X.; Hao, Y.; Shi, L.; Hu, R. General practitioners versus other physicians in the quality of primary care: A cross-sectional study in Guangdong Province, China. BMC Fam. Pract. 2015, 16, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, C.; Kuang, L.; Li, L.; Liang, Y.; Mei, J.; Li, L. Equity in patient experiences of primary care in community health centres using primary care assessment tool: A comparison of rural-to-urban migrants and urban locals in Guangdong, China. Int. J. Equity Health 2018, 17, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, S.; Shi, L.; Zeng, J.; Chen, W.; Ling, L. Comparison of Primary Care Experiences in Village Clinics with Different Ownership Models in Guangdong Province, China. PLoS ONE 2017, 12, e0169241. [Google Scholar] [CrossRef]
- Wang, W.; Maitland, E.; Nicholas, S.; Loban, E.; Haggerty, J. Comparison of patient perceived primary care quality in public clinics, public hospitals and private clinics in rural China. Int. J. Equity Health 2017, 16, 176. [Google Scholar] [CrossRef] [Green Version]
- Zeng, J.; Shi, L.; Zou, X.; Chen, W.; Ling, L. Rural-to-Urban Migrants’ Experiences with Primary Care under Different Types of Medical Institutions in Guangzhou, China. PLoS ONE 2015, 10, e0140922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, L.; Lee, D.C.; Liang, H.; Zhang, L.; Makinen, M.; Blanchet, N.; Kidane, R.; Lindelow, M.; Wang, H.; Wu, S. Community health centres and primary care access and quality for chronically-ill patients—A case-comparison study of urban Guangdong Province, China. Int. J. Equity Health 2015, 14, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Z.; Liao, Y.; Chen, C.C.; Hao, Y.; Hu, R. Usual source of care and the quality of primary care: A survey of patients in Guangdong province, China. Int. J. Equity Health 2015, 14, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuang, L.; Liang, Y.; Mei, J.; Zhao, J.; Wang, Y.; Liang, H.; Shi, L. Family practice and the quality of primary care: A study of Chinese patients in Guangdong Province. Fam. Pract. 2015, 32, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Chung, R.Y.; Wei, X.; Mou, J.; Wong, S.Y.; Wong, M.C.; Zhang, D.; Zhang, Y.; Griffiths, S. Comparison of perceived quality amongst migrant and local patients using primary health care delivered by community health centres in Shenzhen, China. BMC Fam. Pract. 2014, 15, 76. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.H.; Wong, S.Y.; Wong, M.C.; Wang, J.J.; Wei, X.L.; Li, D.K.; Tang, J.L.; Griffiths, S.M. Attributes of primary care in community health centres in China and implications for equitable care: A cross-sectional measurement of patients’ experiences. QJM 2015, 108, 549–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, S.Y.; Kung, K.; Griffiths, S.M.; Carthy, T.; Wong, M.C.; Lo, S.V.; Chung, V.C.; Goggins, W.B.; Starfield, B. Comparison of primary care experiences among adults in general outpatient clinics and private general practice clinics in Hong Kong. BMC Public Health 2010, 10, 397. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Li, H.; Yang, N.; Wong, S.Y.; Owolabi, O.; Xu, J.; Shi, L.; Tang, J.; Li, D.; Griffiths, S.M. Comparing quality of public primary care between Hong Kong and Shanghai using validated patient assessment tools. PLoS ONE 2015, 10, e0121269. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | All Participants n = 1010 (100.0) | CHC/CHS n = 405 (%) | THC/RHS n = 605 (%) | χ2 | p-Value |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 412 (40.79) | 134 (33.09) | 278 (45.95) | 16.62 | <0.001 |
| Female | 598 (59.21) | 271 (66.91) | 327 (54.05) | ||
| Age | |||||
| 18–34 | 72 (7.13) | 22 (5.43) | 50 (8.26) | 13.07 | 0.011 |
| 35–49 | 123 (12.18) | 36 (8.89) | 87 (14.38) | ||
| 50–64 | 336 (33.27) | 137 (33.83) | 199 (32.89) | ||
| ≥65 | 479 (47.42) | 210 (51.85) | 269 (44.47) | ||
| Marital status | |||||
| Married | 840 (83.17) | 328 (80.99) | 512 (84.63) | 2.30 | 0.130 |
| Unmarried (single/divorced/windowed) | 170 (16.83) | 77 (19.01) | 93 (15.37) | ||
| Education background | |||||
| Primary school and below | 492 (48.71) | 148 (36.54) | 344 (56.86) | 42.81 | <0.001 |
| Middle school | 433 (42.87) | 208 (51.36) | 225 (37.19) | ||
| College degree and above | 85 (8.42) | 49 (12.10) | 36 (5.95) | ||
| The income of family monthly (of 2014 USD) | |||||
| <$495.9 | 706 (69.90) | 208 (51.36) | 498 (82.31) | 112.99 | <0.001 |
| $495.9–$1157.0 | 253 (25.05) | 169 (41.73) | 84 (13.88) | ||
| ≥$1157.0 | 51 (5.05) | 28 (6.91) | 23 (3.81) | ||
| Medical insurance | |||||
| Have | 988 (97.82) | 397 (98.02) | 591 (97.69) | 3.24 | 0.293 |
| No | 22 (2.18) | 8 (1.98) | 14 (2.31) | ||
| The proportion of medical expenditure to total family expenditures | |||||
| <30% | 853 (84.46) | 334 (82.47) | 519 (85.78) | 3.62 | 0.308 |
| ≥30% | 157 (15.54) | 71 (17.53) | 86 (14.22) | ||
| Self-reported health status | |||||
| Well | 374 (37.03) | 126 (31.11) | 248 (40.99) | 10.91 | 0.004 |
| General | 454 (44.95) | 204 (50.37) | 250 (41.32) | ||
| Bad | 182 (18.02) | 75 (18.52) | 107 (17.69) | ||
| Chronic conditions | |||||
| Yes | 462 (45.74) | 200 (49.38) | 262 (43.31) | 6.89 | 0.122 |
| No | 548 (54.26) | 205 (50.62) | 343 (56.69) | ||
| Walking to the nearest primary care institutions (minutes) | |||||
| <30 | 858 (84.95) | 326 (80.49) | 532 (87.93) | 10.50 | 0.001 |
| ≥30 | 152 (15.05) | 79 (19.51) | 73 (12.07) | ||
| Preferred primary care institutions | |||||
| Yes | 696 (68.91) | 143 (35.31) | 553 (91.40) | 180.82 | <0.001 |
| No | 314 (31.09) | 262 (64.69) | 52 (8.60) | ||
| Number of visiting primary care institutions | |||||
| ≤3 | 428 (42.38) | 146 (36.05) | 282 (46.61) | 14.79 | 0.001 |
| 4–6 | 218 (21.58) | 86 (21.23) | 132 (21.82) | ||
| ≥7 | 364 (36.04) | 173 (42.72) | 191 (31.57) |
| Domain | All participants (n = 1010) | CHC/CHS (n = 405) | THC/RHS (n = 605) | t-Value | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| Mean (SE) | Standardized Score | Mean (SE) | Standardized Score | Mean (SE) | Standardized Score | |||
| Unadjusted | ||||||||
| First contact ** | 7.01 (0.06) | 7.79 | 6.78 (0.98) | 7.53 | 7.16 (0.73) | 7.96 | 3.13 | 0.002 |
| Accessibility ** | 7.77 (0.09) | 6.48 | 6.96 (0.14) | 5.80 | 8.32 (0.12) | 6.93 | 7.42 | <0.001 |
| Ongoing care ** | 7.89 (0.09) | 6.58 | 7.24 (0.14) | 6.03 | 8.31 (0.11) | 6.93 | 6.08 | <0.001 |
| Coordination (Referrals) ** | 10.82 (0.38) | 7.21 | 11.76 (0.61) | 7.84 | 10.13 (0.47) | 6.75 | −2.24 | 0.026 |
| Coordination (Information systems) ** | 6.60 (0.07) | 7.33 | 6.83 (0.13) | 7.59 | 6.44 (0.09) | 7.16 | −2.60 | 0.009 |
| Comprehensiveness (Services available) | 11.49 (0.09) | 7.73 | 11.33 (0.16) | 7.55 | 11.60 (0.12) | 7.73 | 1.40 | 0.163 |
| Comprehensiveness (Services provided) | 9.45 (0.10) | 7.88 | 9.36 (0.15) | 7.80 | 9.51 (0.12) | 7.93 | 0.76 | 0.451 |
| Family centeredness | 5.45 (0.08) | 6.06 | 5.47 (0.12) | 6.08 | 5.44 (0.09) | 6.04 | −0.21 | 0.833 |
| Community orientation ** | 5.35 (0.07) | 5.94 | 4.69 (0.10) | 5.21 | 5.80 (0.09) | 6.44 | 7.85 | <0.001 |
| Culturally competent | 9.75 (0.07) | 8.13 | 9.63 (0.11) | 8.03 | 9.83 (0.09) | 8.19 | 1.43 | 0.152 |
| Total scores ** | 70.70 (0.47) | 73.65 | 68.32 (0.73) | 71.17 | 72.41 (0.59) | 75.43 | 4.37 | <0.001 |
| Adjusted | ||||||||
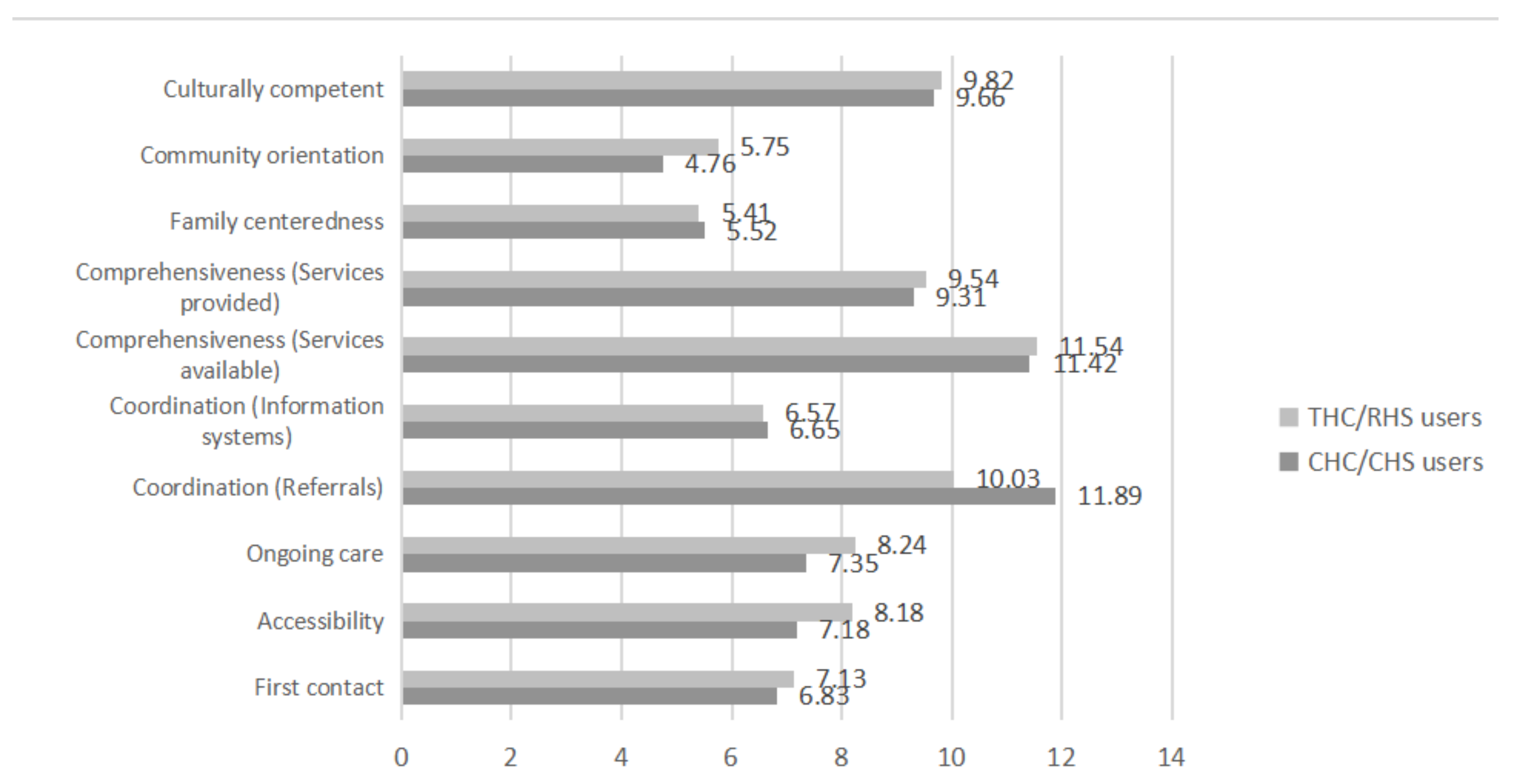
| First contact ** | 6.98 (0.06) | 7.76 | 6.83 (0.09) | 7.59 | 7.13 (0.08) | 7.92 | 5.47 | 0.024 |
| Accessibility ** | 7.68 (0.09) | 6.40 | 7.18 (0.15) | 5.98 | 8.18 (0.12) | 6.82 | 25.56 | <0.001 |
| Ongoing care ** | 7.80 (0.09) | 6.50 | 7.35 (0.14) | 6.13 | 8.24 (0.11) | 6.87 | 22.99 | <0.001 |
| Coordination (Referrals) ** | 10.91 (0.38) | 7.27 | 11.89 (0.59) | 7.93 | 10.03 (0.53) | 6.69 | 5.71 | 0.017 |
| Coordination (Information systems) | 6.61 (0.08) | 7.34 | 6.65 (0.12) | 7.39 | 6.57 (0.10) | 7.30 | 0.26 | 0.608 |
| Comprehensiveness (Services available) | 11.48 (0.09) | 7.65 | 11.42 (0.15) | 7.61 | 11.54 (0.12) | 7.69 | 0.30 | 0.587 |
| Comprehensiveness (Services provided) | 9.43 (0.10) | 7.86 | 9.31 (0.16) | 7.76 | 9.54 (0.13) | 7.95 | 1.22 | 0.271 |
| Family centeredness | 5.47 (0.08) | 6.08 | 5.52 (0.12) | 6.13 | 5.41 (0.10) | 6.01 | 0.48 | 0.493 |
| Community orientation ** | 5.26 (0.07) | 5.84 | 4.76 (0.12) | 5.29 | 5.75 (0.09) | 6.39 | 40.78 | <0.001 |
| Culturally competent | 6.74 (0.07) | 7.49 | 6.74 (0.11) | 7.49 | 6.74 (0.09) | 7.49 | 0.16 | 0.983 |
| Total scores ** | 67.76 (0.45) | 70.58 | 65.43 (0.71) | 68.16 | 69.32 (0.58) | 72.21 | 18.14 | 0.001 |
| Variables | Model I | Model II | Model III | Model IV | ||||
|---|---|---|---|---|---|---|---|---|
| β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | |
| Medical institution type | ||||||||
| THC/RHS (ref) | ||||||||
| CHC/CHS | −2.17 (−3.34, −0.61) | <0.001 | −1.19 (−2.91, −0.11) | 0.005 | −2.55 (−4.96, −1.23) | <0.001 | −3.58 (−7.69, −1.12) | <0.001 |
| Gender | ||||||||
| Male (ref) | ||||||||
| Female | −0.23 (−1.08, 0.71) | 0.783 | −0.25 (−1.10, 0.60) | 0.798 | 0.46 (−0.37, 1.18) | 0.650 | ||
| Age | ||||||||
| 18–34 (ref) | ||||||||
| 35–49 | 0.17 (−0.52, 0.76) | 0.877 | 0.99 (−0.60, 2.58) | 0.613 | 1.21 (−0.32, 2.88) | 0.332 | ||
| 50–64 | −1.02 (−3.18, 1.71) | 0.582 | −1.41 (−2.24, 0.53) | 0.365 | −0.86 (−3.07, 1.87) | 0.814 | ||
| ≥65 | −0.05 (−0.67, 0.81) | 0.886 | −0.38 (−1.55, 1.45) | 0.756 | −0.38 (−1.92, 1.39) | 0.806 | ||
| Marital status | ||||||||
| Married (ref) | ||||||||
| Unmarried (single/divorced/windowed) | −1.77 (−4.52, −0.21) | 0.063 | −2.77 (−5.22, −0.23) | 0.076 | −1.49 (−3.85, 0.86) | 0.208 | ||
| Education background | ||||||||
| Primary school and below (ref) | ||||||||
| Middle school | −1.32 (−3.22, 0.51) | 0.122 | −1.34 (−3.23, 0.52) | 0.133 | −0.46 (−1.77, 2.39) | 0.206 | ||
| College degree and above | −6.61 (−10.07, −1.27) | 0.001 | −5.45 (−9.12, −2.44) | 0.001 | −3.89 (−8.51, 0.71) | 0.001 | ||
| The income of family monthly (of 2014 USD) | ||||||||
| <$495.9 (ref) | ||||||||
| $495.9–$1157.0 | −0.81 (−1.97, 1.12) | 0.383 | −1.28 (−3.25, 0.91) | 0.208 | −1.10 (−3.13, 0.97) | 0.290 | ||
| ≥$1157.0 | −2.41 (−5.23, −1.03) | 0.065 | −2.76 (−4.98, −1.34) | 0.178 | −2.88 (−6.68, 1.53) | 0.353 | ||
| Self-reported health status | ||||||||
| Well (ref) | ||||||||
| General | −0.09 (−0.53, 0.46) | 0.893 | −0.21 (−1.92, 0.76) | 0.488 | ||||
| Bad | −2.46 (−5.24, 0.11) | 0.071 | −2.11 (−5.78, −0.15) | 0.191 | ||||
| Chronic conditions | ||||||||
| Yes (ref) | ||||||||
| No | −4.61 (−9.23, −1.24) | <0.001 | −3.52 (−5.32, −1.69) | <0.001 | ||||
| Medical insurance | ||||||||
| Have (ref) | ||||||||
| No | −2.16 (−4.53, 1.21) | 0.657 | −2.87 (−6.33, 1.42) | 0.511 | ||||
| The proportion of medical expenditure to total family expenditures | ||||||||
| <30% (ref) | ||||||||
| ≥30% | 0.37 (−0.07, 1.54) | 0.689 | 0.92 (−0.38, 2.32) | 0.564 | ||||
| Walking to the nearest primary care institutions (minutes) | ||||||||
| <30 (ref) | ||||||||
| ≥30 | −0.59 (−1.07, 0.89) | 0.643 | ||||||
| Preferred primary care institutions | ||||||||
| Yes (ref) | ||||||||
| No | −6.64 (−9.76, −3.52) | <0.001 | ||||||
| Number of visiting primary care institutions | ||||||||
| ≤3 (ref) | ||||||||
| 4–6 | 1.55 (−0.57, 3.66) | 0.1524 | ||||||
| ≥7 | 4.01 (1.66, 6.34) | 0.002 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, A.; Feng, S.; Zhang, L.; Shi, L. Comparison of Patients’ Perceived Quality of Primary Care Between Urban and Rural Community Health Centers in Guangdong, China. Int. J. Environ. Res. Public Health 2020, 17, 4898. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134898
Chen A, Feng S, Zhang L, Shi L. Comparison of Patients’ Perceived Quality of Primary Care Between Urban and Rural Community Health Centers in Guangdong, China. International Journal of Environmental Research and Public Health. 2020; 17(13):4898. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134898
Chicago/Turabian StyleChen, Aiyun, Shanshan Feng, Liang Zhang, and Leiyu Shi. 2020. "Comparison of Patients’ Perceived Quality of Primary Care Between Urban and Rural Community Health Centers in Guangdong, China" International Journal of Environmental Research and Public Health 17, no. 13: 4898. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134898