The Relationship between Mercury Exposure Indices and Dietary Intake of Fish and Shellfish in Women of Childbearing Age

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Questionnaire Survey
2.3. Analysis of Blood, Hair, and Urine Mercury Concentration
2.4. Statistical Analysis
2.5. Ethics Statement
3. Results
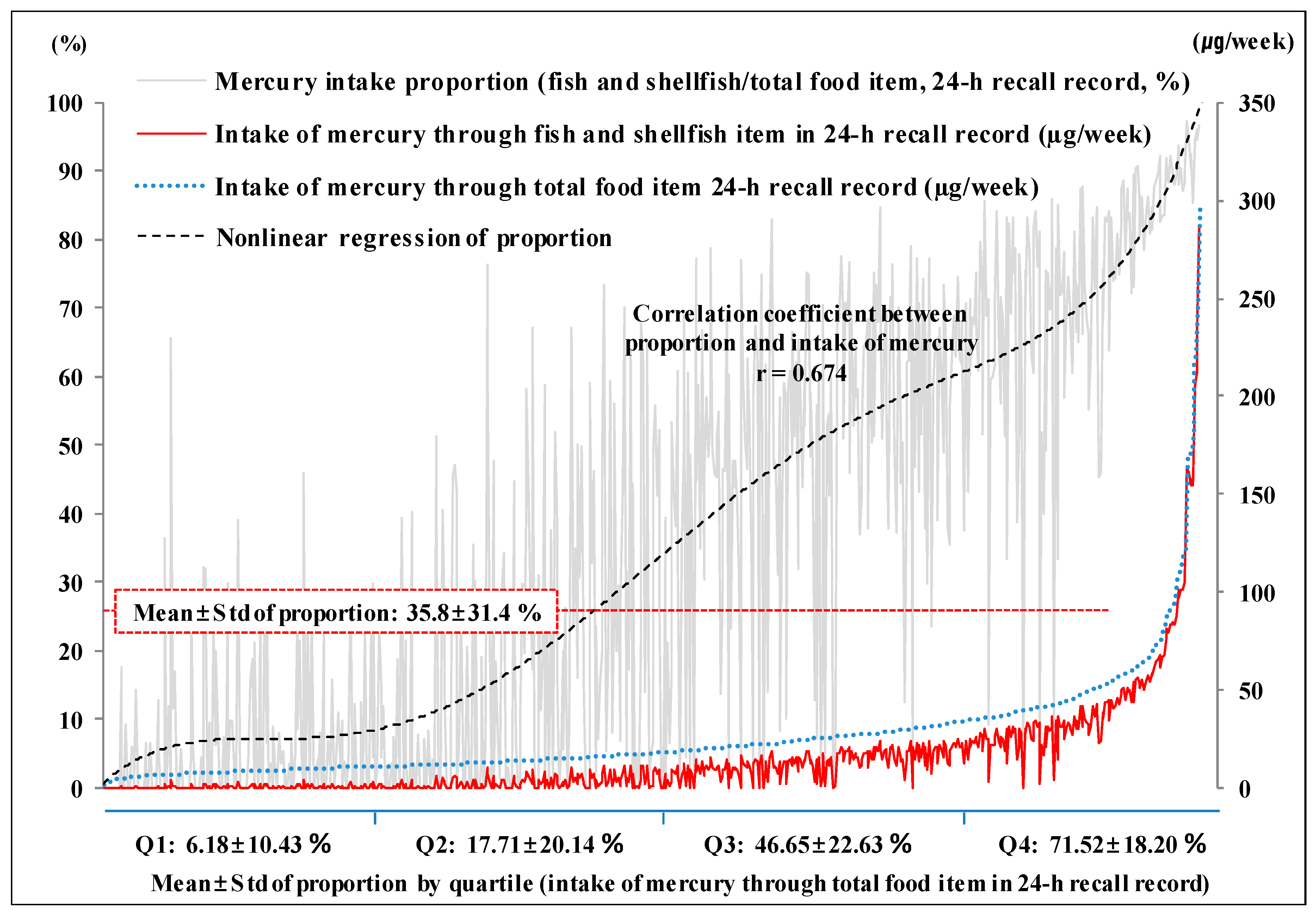
3.1. Mercury Intake through Fish and Shellfish
3.2. Total Blood, Blood Methyl, Hair, and Urine Mercury Concentration
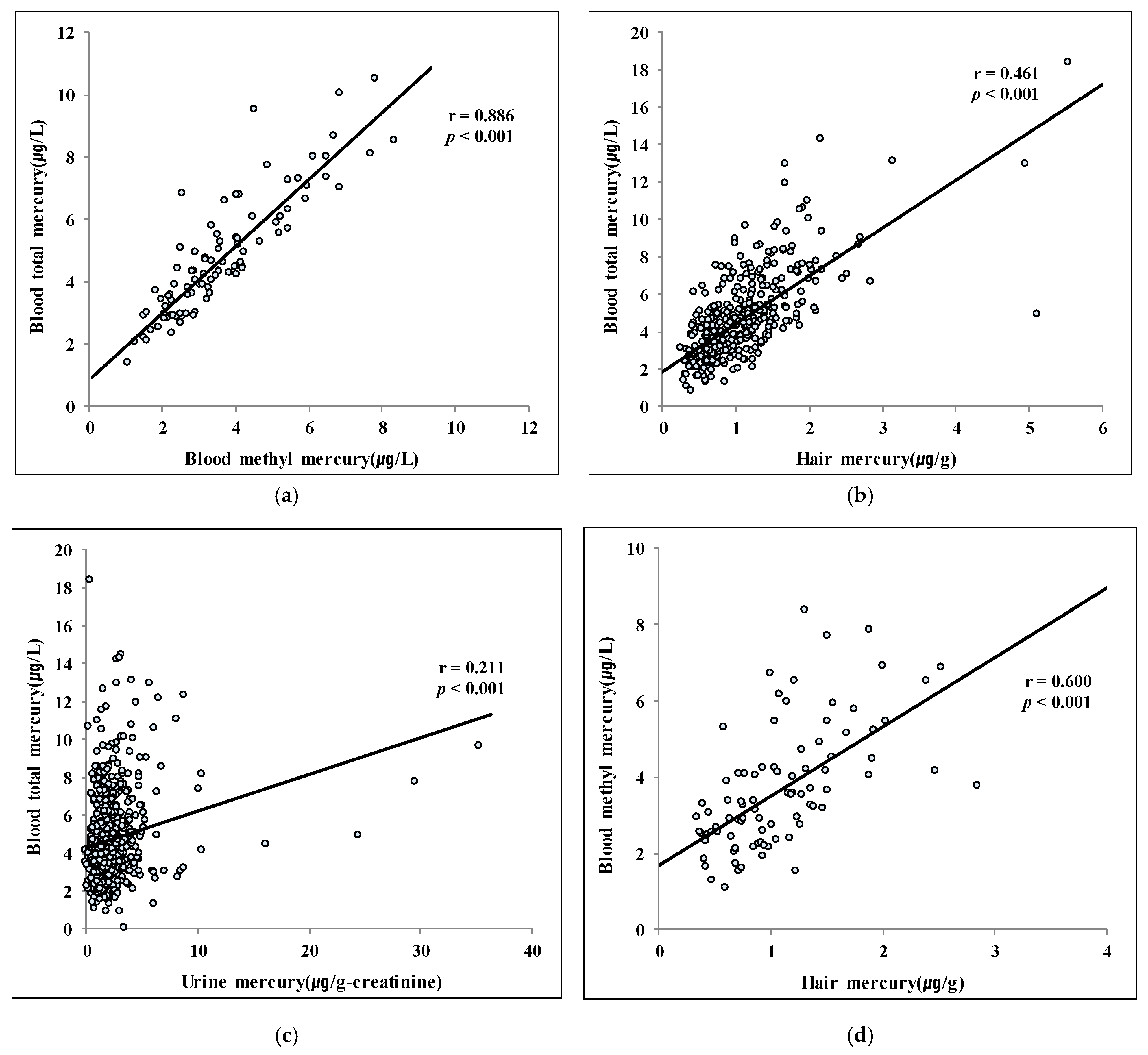
3.3. Correlations among Mercury Concentrations
3.4. Proportion of Blood MeHg/T-Hg Concentrations
3.5. Proportions of Total Blood Mercury Concentrations Exceeding the Standard Criteria
4. Discussion
4.1. Relationship between Seafood Intake and Blood T-Hg Concentration
4.2. Relationship between Seafood Intake and Blood MeHg, Hair Hg, and Urine Hg Concentrations
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kajiwara, Y.; Yasutake, A.; Adachi, T.; Hirayama, K. Methylmercury transport across the placenta via neutral amino acid carrier. Arch. Toxicol. 1996, 70, 310–314. [Google Scholar] [CrossRef]
- Gray, D.G. A physiologically based pharmacokinetic model for methyl mercury in the pregnant rat and fetus. Toxicol. Appl. Pharmacol. 1995, 132, 91–102. [Google Scholar] [CrossRef] [PubMed]
- National Research Council. Toxicological Effects of Methylmercury; National Academies Press: Washington, DC, USA, 2000.
- Inouye, M.; Kajiwara, Y. Developmental disturbances of the fetal brain in guinea-pigs caused by methylmercury. Arch. Toxicol. 1988, 62, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, H.; Mitani, K.; Kodama, K.; Nakata, T. Placental transfer of heavy metals in normal pregnant Japanese women. Arch. Environ. Health Int. J. 1984, 39, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Keating, M.H.; Mahaffey, K.; Schoeny, R.; Rice, G.; Bullock, O. Mercury Study Report to Congress; Executive Summary; Environmental Protection Agency: Research Triangle Park, NC, USA, 1997; Volume 1.
- Poulin, J.; Gibb, H.; Prüss-Üstün, A.; World Health Organization. Mercury: Assessing the Environmental Burden of Disease at National and Local Levels; WHO: Geneva, Switzerland, 2008.
- Korea Ministry of Food and Drug Safety. Dietary Intake and Risk Assessment of Contaminants in Korea Foods; Korea Ministry of Food and Drug Safety: Cheongju-si, Korea, 2009.
- Kim, H.-Y.; Kim, S.-Y.; Lee, J.-H.; Jang, Y.-M.; Lee, M.-S.; Park, J.-S.; Lee, K.-H.; Kim, J.-C. Monitoring of Heavy Metals in Fishes in Korea-As, Cd, Cu. Pb, Mn, Zn, Total Hg. Korean J. Food Sci. Technol. 2007, 39, 353–359. [Google Scholar]
- Kwon, H.; Kim, B.; Park, S.; Lee, J.; Park, M.; Lee, M. Research on the harmful heavy metals of seafood in the Busan area. Annu. Rep. Busan Metrop. City Inst. Health Environ. 2010, 20, 44–52. [Google Scholar]
- Hursh, J.B.; Clarkson, T.W.; Cherian, M.G.; Vostal, J.J.; Mallie, R.V. Clearance of mercury (Hg-197, Hg-203) vapor inhaled by human subjects. Arch. Environ. Health Int. J. 1976, 31, 302–309. [Google Scholar] [CrossRef]
- Smith, P.; Langolf, G.; Goldberg, J. Effect of occupational exposure to elemental mercury on short term memory. Occup. Environ. Med. 1983, 40, 413–419. [Google Scholar] [CrossRef] [Green Version]
- Morcillo, M.A.; Santamaria, J. Whole-body retention, and urinary and fecal excretion of mercury after subchronic oral exposure to mercuric chloride in rats. BioMetals 1995, 8, 301–308. [Google Scholar] [CrossRef]
- Samuels, E.; Heick, H.; McLaine, P.; Farant, J. A case of accidental inorganic mercury poisoning. J. Anal. Toxicol. 1982, 6, 120–122. [Google Scholar] [CrossRef]
- Cherian, M.G.; Hursh, J.B.; Clarkson, T.W.; Allen, J. Radioactive mercury distribution in biological fluids and excretion in human subjects after inhalation of mercury vapor. Arch. Environ. Health Int. J. 1978, 33, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Mahaffey, K.R.; Mergler, D. Blood levels of total and organic mercury in residents of the upper St. Lawrence River basin, Quebec: Association with age, gender, and fish consumption. Environ. Res. 1998, 77, 104–114. [Google Scholar] [CrossRef]
- Grandjean, P.; Weihe, P.; Jørgensen, P.; Clarkson, T.; Cernichiari, E.; Viderø, T. Impact of maternal seafood diet on fetal exposure to mercury, selenium, and lead. Arch. Environ. Health Int. J. 1992, 47, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Hansen, J.C.; Tarp, U.; Bohm, J. Prenatal exposure to methyl mercury among Greenlandic polar Inuits. Arch. Environ. Health Int. J. 1990, 45, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Oskarsson, A.; Schütz, A.; Skerfving, S.; Hallén, I.P.; Ohlin, B.; Lagerkvist, B.J. Total and inorganic mercury in breast milk and blood in relation to fish consumption and amalgam fillings in lactating women. Arch. Environ. Health Int. J. 1996, 51, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Aks, S.E.; Erickson, T.; Branches, F.J.; Naleway, C.; Chou, H.-N.; Levy, P.; Hryhorczuk, D. Fractional mercury levels in Brazilian gold refiners and miners. J. Toxicol. Clin. Toxicol. 1995, 33, 1–10. [Google Scholar] [CrossRef]
- Lee, K.E.; Hong, Y.S.; Kim, D.S.; Han, M.S.; Yu, B.C.; Kim, Y.W.; Roh, M.S.; Lee, H.J.; Lee, J.W.; Kwak, J.Y. Mercury concentrations of maternal and umbilical cord blood in Korean pregnant women: Preliminary study. Korean J. Occup. Environ. Med. 2007, 19, 268–275. [Google Scholar] [CrossRef]
- Cernichiari, E.; Brewer, R.; Myers, G.J.; Marsh, D.O.; Lapham, L.W.; Cox, C.; Shamlaye, C.F.; Berlin, M.; Davidson, P.; Clarkson, T.W. Monitoring methylmercury during pregnancy: Maternal hair predicts fetal brain exposure. Neurotoxicology 1995, 16, 705–710. [Google Scholar]
- Suzuki, T.; Hongo, T.; Yoshinaga, J.; Imai, H.; Nakazawa, M.; Matsuo, N.; Akagi, H. The hair-organ relationship in mercury concentration in contemporary Japanese. Arch. Environ. Health Int. J. 1993, 48, 221–229. [Google Scholar] [CrossRef]
- World Health Organization. Methyl Mercury; WHO: Geneva, Switzerland, 1990; Volume 101.
- World Health Organization. Inorganic Mercury; WHO: Geneva, Switzerland, 1991; Volume 101.
- Kim, B.G.; Jo, E.M.; Kim, G.Y.; Kim, D.S.; Kim, Y.M.; Kim, R.B.; Suh, B.S.; Hong, Y.S. Analysis of methylmercury concentration in the blood of Koreans by using cold vapor atomic fluorescence spectrophotometry. Ann. Lab. Med. 2012, 32, 31–37. [Google Scholar] [CrossRef]
- U.S. Environmental Prdotection Agency. Method 7473, Mercury in Solids and Solutions by Thermal Decomposition, Amalgamation, and Atomic Absorption Spectrometry; U.S. Government Printing Office: Washington, DC, USA, 2000.
- U.S. Environmental Protection Agency. Method 1630, Methyl Mercury in Water by Distillation, Aqueous Ethylation, Purge and Trap, and Cold Vapor Atomic Fluorescence Spectrometry; U.S. Government Printing Office: Washington, DC, USA, 2001.
- Korea Centers for Disease Control Prevention. Korea Health Statistics 2007–2011: Korea National Health and Nutrition Examination Survey (KNHANES IV, V); Korea Centers for Disease Control and Prevention Cheongwon: Cheongju-si, Korea, 2012.
- You, C.H.; Kim, B.G.; Jo, E.M.; Kim, G.Y.; Yu, B.C.; Hong, M.G.; Kim, D.S.; Hong, Y.S. The relationship between the fish consumption and blood total/methyl-mercury concentration of costal area in Korea. Neurotoxicology 2012, 33, 676–682. [Google Scholar] [CrossRef]
- U.S. Centers for Disease Control and Prevention. Fourth National Report on Human Exposure to Environmental Chemicals, Updated Tables, January 2019; Department of Health and Human Services, Centers for Disease Control and Prevention: Georgia, GA, USA, 2019.
- Statistics Canada. Canadian Health Measures Survey: Cycle 2 Data Tables, 2009 to 2011; Statistics Canada: Ottawa, ON, Canada, 2012.
- Becker, K.; Kaus, S.; Krause, C.; Lepom, P.; Schulz, C.; Seiwert, M.; Seifert, B. German Environmental Survey 1998 (GerES III): Environmental pollutants in blood of the German population. Int. J. Hyg. Environ. Health 2002, 205, 297–308. [Google Scholar] [CrossRef]
- Sakamoto, M.; Kaneoka, T.; Murata, K.; Nakai, K.; Satoh, H.; Akagi, H. Correlations between mercury concentrations in umbilical cord tissue and other biomarkers of fetal exposure to methylmercury in the Japanese population. Environ. Res. 2007, 103, 106–111. [Google Scholar] [CrossRef]
- Hightower, J.M.; O’Hare, A.; Hernandez, G.T. Blood mercury reporting in NHANES: Identifying Asian, Pacific Islander, Native American, and multiracial groups. Environ. Health Perspect. 2006, 114, 173–175. [Google Scholar] [CrossRef] [Green Version]
- Karouna-Renier, N.K.; Rao, K.R.; Lanza, J.J.; Rivers, S.D.; Wilson, P.A.; Hodges, D.K.; Levine, K.E.; Ross, G.T. Mercury levels and fish consumption practices in women of child-bearing age in the Florida Panhandle. Environ. Res. 2008, 108, 320–326. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Rimm, E.B. Fish intake, contaminants, and human health: Evaluating the risks and the benefits. JAMA 2006, 296, 1885–1899. [Google Scholar] [CrossRef] [Green Version]
- Grandjean, P.; Weihe, P.; White, R.F.; Debes, F. Cognitive performance of children prenatally exposed to “safe” levels of methylmercury. Environ. Res. 1998, 77, 165–172. [Google Scholar] [CrossRef]
- Schober, S.E.; Sinks, T.H.; Jones, R.L.; Bolger, P.M.; McDowell, M.; Osterloh, J.; Garrett, E.S.; Canady, R.A.; Dillon, C.F.; Sun, Y.; et al. Blood mercury levels in US children and women of childbearing age, 1999–2000. JAMA 2003, 289, 1667–1674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrissette, J.; Takser, L.; St-Amour, G.; Smargiassi, A.; Lafond, J.; Mergler, D. Temporal variation of blood and hair mercury levels in pregnancy in relation to fish consumption history in a population living along the St. Lawrence River. Environ. Res. 2004, 95, 363–374. [Google Scholar] [CrossRef]
- Järup, L. Hazards of Heavy Metal Contamination. Br. Med. Bull. 2003, 68, 167–182. [Google Scholar] [CrossRef] [Green Version]
- Mahaffey, K.R.; Clickner, R.P.; Bodurow, C.C. Blood organic mercury and dietary mercury intake: National Health and Nutrition Examination Survey, 1999 and 2000. Environ. Health Perspect. 2004, 112, 562–570. [Google Scholar] [CrossRef] [Green Version]
- McKelvey, W.; Gwynn, R.C.; Jeffery, N.; Kass, D.; Thorpe, L.E.; Garg, R.K.; Palmer, C.D.; Parsons, P.J. A biomonitoring study of lead, cadmium, and mercury in the blood of New York city adults. Environ. Health Perspect. 2007, 115, 1435–1441. [Google Scholar] [CrossRef]
- Kim, E.H.; Kim, I.K.; Kwon, J.Y.; Kim, S.W.; Park, Y.W. The effect of fish consumption on blood mercury levels of pregnant women. Yonsei Med. J. 2006, 47, 626–633. [Google Scholar] [CrossRef] [Green Version]
- Vahter, M.; Åkesson, A.; Lind, B.; Björs, U.; Schütz, A.; Berglund, M. Longitudinal study of methylmercury and inorganic mercury in blood and urine of pregnant and lactating women, as well as in umbilical cord blood. Environ. Res. 2000, 84, 186–194. [Google Scholar] [CrossRef] [Green Version]
- Björnberg, K.A.; Vahter, M.; Grawé, K.P.; Berglund, M. Methyl mercury exposure in Swedish women with high fish consumption. Sci. Total Environ. 2005, 341, 45–52. [Google Scholar] [CrossRef]
- Allen, B.C.; Eric Hack, C.; Clewell, H.J. Use of Markov Chain Monte Carlo analysis with a physiologically-based pharmacokinetic model of methylmercury to estimate exposures in US women of childbearing age. Risk Anal. Int. J. 2007, 27, 947–959. [Google Scholar] [CrossRef]
- U.S. Environmental Protection Agency. Methylmercury Reference Dose for Chronic Oral Exposure. U.S. Environmental Protection Agency, Integrated Risk Information System (IRIS). Available online: http://www.epa.gov/iris/subst/0073.htm (accessed on 22 April 2004).
- Weihe, P.; Grandjean, P.; Debes, F.; White, R. Health implications for Faroe Islanders of heavy metals and PCBs from pilot whales. Sci. Total Environ. 1996, 186, 141–148. [Google Scholar] [CrossRef]
- Grandjean, P.; Weihe, P.; White, R.F.; Debes, F.; Araki, S.; Yokoyama, K.; Murata, K.; Sørensen, N.; Dahl, R.; Jørgensen, P.J. Cognitive deficit in 7-year-old children with prenatal exposure to methylmercury. Neurotoxicol. Teratol. 1997, 19, 417–428. [Google Scholar] [CrossRef]
- Huang, L.S.; Cox, C.; Myers, G.J.; Davidson, P.W.; Cernichiari, E.; Shamlaye, C.F.; Sloane-Reeves, J.; Clarkson, T.W. Exploring nonlinear association between prenatal methylmercury exposure from fish consumption and child development: Evaluation of the Seychelles Child Development Study nine-year data using semiparametric additive models. Environ. Res. 2005, 97, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.S.; Myers, G.J.; Davidson, P.W.; Cox, C.; Xiao, F.; Thurston, S.W.; Cernichiari, E.; Shamlaye, C.F.; Sloane-Reeves, J.; Georger, L. Is susceptibility to prenatal methylmercury exposure from fish consumption non-homogeneous? Tree-structured analysis for the Seychelles Child Development Study. Neurotoxicology 2007, 28, 1237–1244. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.S.; Lee, E.J.; Bae, S.H.; Ohtsuka, R.; Suzuki, T. Mercury concentrations in pregnant women’s hair in the Seoul area. Korean J. Environ. Health 1992, 18, 105–111. [Google Scholar]
- Song, M.; Cho, T.; Jeon, H.; Kim, J.; Son, B. A study on mercury concentration in the hair of university students in Jeon-nam area. J. Environ. Health Sci. 2009, 35, 287–294. [Google Scholar]
- Eun, J.K.; Lee, W.S. Mercury contents of human scalp hair by the consumption pattern in fish. J. Environ. Sanit. Eng. 2000, 15, 8–14. [Google Scholar]
- Kim, S.A.; Jeon, C.K.; Paek, D.M. Hair mercury concentrations of children and mothers in Korea: Implication for exposure and evaluation. Sci. Total Environ. 2008, 402, 36–42. [Google Scholar] [CrossRef]
- Agusa, T.; Kunito, T.; Iwata, H.; Monirith, I.; Tana, T.S.; Subramanian, A.; Tanabe, S. Mercury contamination in human hair and fish from Cambodia: Levels, specific accumulation and risk assessment. Environ. Pollut. 2005, 134, 79–86. [Google Scholar] [CrossRef]
- Akira, Y.; Miyuki, M.; Masako, Y.; Noriyuki, H. Current Hair Mercury Levels in Japanese for Estimation of Methylmercury Exposure. J. Health Sci. 2004, 50, 120–125. [Google Scholar] [CrossRef] [Green Version]
- Díez, S.; Montuori, P.; Pagano, A.; Sarnacchiaro, P.; Bayona, J.M.; Triassi, M. Hair mercury levels in an urban population from southern Italy: Fish consumption as a determinant of exposure. Environ. Int. 2008, 34, 162–167. [Google Scholar] [CrossRef]
- Dolbec, J.; Mergler, D.; Larribe, F.; Roulet, M.; Lebel, J.; Lucotte, M. Sequential analysis of hair mercury levels in relation to fish diet of an Amazonian population, Brazil. Sci. Total Environ. 2001, 271, 87–97. [Google Scholar] [CrossRef]
- Gerstenberger, S.L.; Tavris, D.R.; Hansen, L.K.; Pratt-Shelley, J.; Dellinger, J.A. Concentrations of blood and hair mercury and serum PCBs in an Ojibwa population that consumes Great Lakes region fish. J. Toxicol. Clin. Toxicol. 1997, 35, 377–386. [Google Scholar] [CrossRef]
- Holsbeek, L.; Das, H.; Joiris, C. Mercury in human hair and relation to fish consumption in Bangladesh. Sci. Total Environ. 1996, 186, 181–188. [Google Scholar] [CrossRef]
- Malm, O.; Branches, F.J.P.; Akagi, H.; Castro, M.B.; Pfeiffer, W.C.; Harada, M.; Bastos, W.R.; Kato, H. Mercury and methylmercury in fish and human hair from the Tapajós river basin, Brazil. Sci. Total Environ. 1995, 175, 141–150. [Google Scholar] [CrossRef]
- Muckle, G.; Ayotte, P.; Dewailly, E.E.; Jacobson, S.W.; Jacobson, J.L. Prenatal exposure of the northern Quebec Inuit infants to environmental contaminants. Environ. Health Perspect. 2001, 109, 1291–1299. [Google Scholar]
- Knobeloch, L.; Anderson, H.A.; Imm, P.; Peters, D.; Smith, A. Fish consumption, advisory awareness, and hair mercury levels among women of childbearing age. Environ. Res. 2005, 97, 220–227. [Google Scholar] [CrossRef] [PubMed]
- McDowell, M.A.; Dillon, C.F.; Osterloh, J.; Bolger, P.M.; Pellizzari, E.; Fernando, R.; Montes de Oca, R.; Schober, S.E.; Sinks, T.; Jones, R.L.; et al. Hair mercury levels in U.S. children and women of childbearing age: Reference range data from NHANES 1999-2000. Environ. Health Perspect. 2004, 112, 1165–1171. [Google Scholar] [CrossRef]
- Björnberg, K.A.; Vahter, M.; Petersson-Grawe, K.; Glynn, A.; Cnattingius, S.; Darnerud, P.O.; Atuma, S.; Aune, M.; Becker, W.; Berglund, M. Methyl mercury and inorganic mercury in Swedish pregnant women and in cord blood: Influence of fish consumption. Environ. Health Perspect. 2003, 111, 637–641. [Google Scholar]
- Lindow, S.W.; Knight, R.; Batty, J.; Haswell, S.J. Maternal and neonatal hair mercury concentrations: The effect of dental amalgam. BJOG 2003, 110, 287–291. [Google Scholar] [CrossRef]
- Korea National Institute of Environmental Research. Korean National Survey of Hazardous Substances in Biological Samples Ⅱ; Korea National Institute of Environmental Research Incheon: Incheon, Korea, 2008. [Google Scholar]
- Kim, D.S.; Ahn, S.C.; Ryu, J.M.; Yu, S.D. Monitoring Study on Exposure Levels of Environmental Pollutants in Residents of a Non-Industrial Area, Korea. Korean J. Environ. Health Sci. 2012, 38. [Google Scholar] [CrossRef] [Green Version]
- Nuttall, K.L. Interpreting mercury in blood and urine of individual patients. Ann. Clin. Lab. Sci. 2004, 34, 235–250. [Google Scholar]
- Mahaffey, K.R. Methylmercury: A new look at the risks. Public Health Rep. 1999, 114, 396–399. [Google Scholar]



{kind=link}
{kind=link}
| Factor | Geometric Mean (95% Confidence Interval) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Blood Total Mercury (µg/L) | Blood Methyl Mercury (µg/L) | Hair Mercury (µg/g) | Urine Mercury (µg/g-creatinine) b | |||||||||
| n | Crude | Adjusted c | n | Crude | Adjusted c | n | Crude | Adjusted c | n | Crude | Adjusted c | |
| Total | 711 | 4.11 (3.90–4.33) | 90 | 3.32 (3.03–3.64) | 359 | 0.97 (0.92–1.03) | 616 | 1.72 (1.61–1.85) | ||||
| Age (y) | ||||||||||||
| 19–29 | 233 | 3.69 (3.49–3.90) | 3.62 (3.21–4.08) | 30 | 2.96 (2.63–3.33) | 2.77 (2.24–3.44) | 114 | 0.84 (0.77–0.93) | 0.79 (0.70–0.89) | 191 | 1.52 (1.36–1.70) | 1.45 (1.24–1.71) |
| 30–39 | 264 | 4.08 (3.61–4.60) | 3.85 (3.49–4.24) | 30 | 3.59 (3.06–4.20) | 3.55 (2.93–4.30) | 123 | 1.06 (0.97–1.16) | 1.00 (0.90–1.11) | 237 | 1.77 (1.54–2.04) | 1.74 (1.53–1.98) |
| 40–49 | 214 | 4.65 (4.36–4.96) | 4.32 (3.87–4.83) | 30 | 3.43 (2.81–4.20) | 3.49 (2.87–4.25) | 122 | 1.02 (0.94–1.12) | 0.97 (0.87–1.08) | 188 | 1.90 (1.73–2.09) | 1.90 (1.65–2.19) |
| p-value | 0.003 | 0.059 | 0.206 | 0.118 | 0.001 | 0.002 | 0.042 | 0.028 | ||||
| Education | ||||||||||||
| High School or Less | 182 | 4.51 (4.20–4.84) | 4.21 (3.72–4.75) | 19 | 3.14 (2.53–3.90) | 3.08 (2.45–3.88) | 91 | 1.02 (0.92–1.12) | 0.93 (0.82–1.05) | 162 | 1.74 (1.43–2.13) | 1.60 (1.37–1.88) |
| University Student | 215 | 3.47 (3.00–4.01) | 3.37 (3.01–3.77) | 26 | 3.49 (2.93–4.16) | 3.41 (2.74–4.24) | 107 | 0.89 (0.79–1.00) | 0.86 (0.77–0.96) | 184 | 1.73 (1.58–1.91) | 1.74 (1.50–2.03) |
| University Graduate | 314 | 4.36 (4.16–4.58) | 4.25 (3.86–4.67) | 45 | 3.30 (2.89–3.76) | 3.27 (2.76–3.88) | 161 | 1.01 (0.94–1.08) | 0.96 (0.87–1.05) | 270 | 1.71 (1.56–1.86) | 1.72 (1.52–1.95) |
| p-value | <0.001 | 0.001 | 0.722 | 0.791 | 0.102 | 0.229 | 0.963 | 0.669 | ||||
| Income (KRW 10,000) | ||||||||||||
| ≤199 | 186 | 4.09 (3.85–4.35) | 3.93 (3.50–4.40) | 20 | 3.30 (2.70–4.03) | 3.52 (2.81–4.40) | 90 | 0.98 (0.90–1.08) | 0.94 (0.84–1.05) | 159 | 1.97 (1.76–2.21) | 1.98 (1.71–2.30) |
| 200–299 | 147 | 4.11 (3.78–4.47) | 3.94 (3.48–4.47) | 16 | 2.78 (2.18–3.54) | 2.72 (2.11–3.50) | 69 | 0.99 (0.87–1.12) | 0.91 (0.80–1.04) | 123 | 1.72 (1.52–1.93) | 1.65 (1.40–1.95) |
| 300–399 | 150 | 4.37 (4.05–4.72) | 4.06 (3.58–4.60) | 21 | 3.53 (2.92–4.26) | 3.39 (2.72–4.22) | 75 | 0.93 (0.82–1.05) | 0.87 (0.77–0.99) | 132 | 1.49 (1.19–1.88) | 1.43 (1.21–1.68) |
| ≥400 | 190 | 4.04 (3.43–4.76) | 3.75 (3.33–4.23) | 28 | 3.50 (2.92–4.18) | 3.45 (2.83–4.19) | 107 | 1.01 (0.91–1.12) | 0.93 (0.83–1.05) | 167 | 1.81 (1.63–2.01) | 1.73 (1.48–2.03) |
| p-value | 0.781 | 0.795 | 0.339 | 0.324 | 0.774 | 0.794 | 0.057 | 0.018 | ||||
| Drinking Status | ||||||||||||
| Current Drinker | 443 | 4.11 (3.80–4.44) | 4.08 (3.80–4.39) | 53 | 3.19 (2.82–3.60) | 3.19 (2.79–3.64) | 223 | 0.99 (0.92–1.06) | 0.96 (0.90–1.04) | 379 | 1.75 (1.59–1.94) | 1.78 (1.62–1.96) |
| Past Drinker | 69 | 3.75 (3.37–4.17) | 3.62 (3.04–4.32) | 10 | 3.54 (2.70–4.64) | 3.24 (2.36–4.43) | 35 | 0.90 (0.77–1.06) | 0.85 (0.71–1.01) | 63 | 1.79 (1.48–2.17) | 1.71 (1.36–2.15) |
| Non Drinker | 199 | 4.24 (3.97–4.53) | 4.07 (3.67–4.52) | 27 | 3.50 (2.92–4.20) | 3.34 (2.75–4.05) | 101 | 0.98 (0.88–1.08) | 0.94 (0.84–1.04) | 174 | 1.64 (1.48–1.81) | 1.58 (1.38–1.82) |
| p-value | 0.466 | 0.451 | 0.594 | 0.926 | 0.640 | 0.390 | 0.666 | 0.378 | ||||
| Amalgam Treatment | ||||||||||||
| Absence | 272 | 3.82 (3.38–4.30) | 3.63 (3.29–4.02) | 37 | 3.32 (2.87–3.83) | 3.22 (2.69–3.86) | 144 | 0.90 (0.83–0.97) | 0.84 (0.76–0.93) | 238 | 1.72 (1.57–1.88) | 1.68 (1.47–1.91) |
| Presence | 439 | 4.30 (4.12–4.48) | 4.23 (3.88–4.60) | 53 | 3.32 (2.94–3.75) | 3.28 (2.81–3.84) | 215 | 1.03 (0.96–1.11) | 0.99 (0.91–1.08) | 378 | 1.73 (1.56–1.91) | 1.70 (1.52–1.90) |
| p-value | 0.031 | 0.009 | 0.999 | 0.848 | 0.014 | 0.004 | 0.944 | 0.882 | ||||
| Mercury Exposure through Fish and Shellfish a | ||||||||||||
| Low (≤ 663 µg/y) | 237 | 3.84 (3.62–4.07) | 3.68 (3.32–4.09) | 26 | 3.20 (2.70–3.80) | 3.06 (2.48–3.77) | 119 | 0.94 (0.85–1.03) | 0.89 (0.80–0.99) | 201 | 1.67 (1.50–1.85) | 1.67 (1.45–1.93) |
| Middle (664–1294 µg/y) | 237 | 4.31 (4.07–4.55) | 4.08 (3.67–4.53) | 37 | 3.21 (2.76–3.74) | 3.12 (2.59–3.76) | 121 | 1.00 (0.91–1.10) | 0.93 (0.84–1.03) | 208 | 1.92 (1.74–2.11) | 1.86 (1.63–2.14) |
| High (≥ 1295 µg/y) | 237 | 4.19 (3.66–4.80) | 4.01 (3.59–4.47) | 27 | 3.58 (3.02–4.25) | 3.60 (2.95–4.40) | 119 | 0.99 (0.90–1.08) | 0.92 (0.83–1.03) | 207 | 1.60 (1.37–1.87) | 1.54 (1.34–1.78) |
| p-value | 0.183 | 0.281 | 0.553 | 0.394 | 0.583 | 0.739 | 0.553 | 0.101 | ||||
| Factor | Arithmetic Means of Proportion (95% Confidence Interval) | ||
|---|---|---|---|
| n | Crude | Adjusted b | |
| Total | 90 | 76.51 (73.62–79.39) | |
| Age (y) | |||
| 19–29 | 30 | 77.35 (72.24–82.46) | 78.67 (72.19–85.16) |
| 30–39 | 30 | 78.07 (72.45–83.69) | 79.58 (73.79–85.37) |
| 40–49 | 30 | 74.10 (69.36–78.84) | 76.82 (70.88–82.75) |
| p-value | 0.499 | 0.771 | |
| Education (y) | |||
| High School or Less | 19 | 74.34 (68.58–80.10) | 78.05 (71.08–85.01) |
| University Student | 26 | 80.40 (74.26–86.55) | 81.88 (75.30–88.47) |
| University Graduate | 45 | 75.17 (71.11–79.22) | 75.14 (69.96–80.32) |
| p-value | 0.229 | 0.217 | |
| Income (KRW 10,000) | |||
| ≤199 | 20 | 77.52 (70.50–84.55) | 80.21 (73.44–86.97) |
| 200–299 | 16 | 72.06 (65.76–78.36) | 74.81 (67.19–82.43) |
| 300–399 | 21 | 75.54 (68.38–82.70) | 77.15 (70.53–83.77) |
| ≥400 | 28 | 78.99 (74.37–83.61) | 81.26 (75.34–87.19) |
| p-value | 0.425 | 0.457 | |
| Drinking Status | |||
| Current Drinker | 53 | 74.61 (70.76–78.47) | 72.95 (68.92–76.99) |
| Past Drinker | 10 | 83.13 (74.42–91.83) | 82.10 (72.62–91.58) |
| Non Drinker | 27 | 77.77 (72.41–83.12) | 80.02 (74.15–85.89) |
| p-value | 0.173 | 0.051 | |
| Amalgam Treatment | |||
| Absence | 37 | 73.92 (69.51–78.33) | 76.87 (71.38–82.36) |
| Presence | 53 | 78.31 (74.45–82.17) | 79.84 (75.11–84.58) |
| p-value | 0.138 | 0.348 | |
| Mercury Exposure through Fish and Shellfish a | |||
| Low (≤ 663 µg/y) | 26 | 75.70 (70.88–80.52) | 76.30 (69.96–82.63) |
| Middle (664–1294 µg/y) | 37 | 75.64 (69.77–81.51) | 77.54 (71.53–83.55) |
| High (≥ 1295 µg/y) | 27 | 77.70 (72.87–82.54) | 81.24 (75.56–86.91) |
| p-value | 0.793 | 0.386 | |
| Factor | Proportion (95% Confidence Interval) | ||
|---|---|---|---|
| n | ≥5.0 (HBM-I) | ≥5.8 (EPA) | |
| Total | 711 | 34.18 (30.68–37.67) | 23.63 (20.50–26.76) |
| Age (y) | |||
| 19–29 | 233 | 21.03 (15.76–26.30) | 14.16 (9.65–18.67) |
| 30–39 | 264 | 37.50 (31.62–43.38) | 26.52 (21.16–31.87) |
| 40–49 | 214 | 44.39 (37.68–51.10) | 30.37 (24.16–36.58) |
| p-value | <0.001 | <0.001 | |
| Education (y) | |||
| High School or Less | 182 | 40.66 (33.46–47.86) | 28.57 (21.95–35.20) |
| University Student | 215 | 27.44 (21.43–33.45) | 17.21 (12.12–22.30) |
| University Graduate | 314 | 35.03 (29.73–40.34) | 25.16 (20.33–29.99) |
| p-value | 0.020 | 0.020 | |
| Income (KRW 10,000) | |||
| ≤199 | 186 | 29.03 (22.45–35.62) | 18.28 (12.67–23.89) |
| 200–299 | 147 | 34.69 (26.91–42.48) | 27.21 (19.93–34.49) |
| 300–399 | 150 | 38.67 (30.78–46.55) | 28.00 (20.73–35.27) |
| ≥400 | 190 | 38.95 (31.95–45.94) | 25.79 (19.51–32.07) |
| p-value | 0.167 | 0.131 | |
| Drinking Status | |||
| Current Drinker | 443 | 34.54 (30.09–38.98) | 23.93 (19.94–27.92) |
| Past Drinker | 69 | 21.74 (11.76–31.72) | 11.59 (3.85–19.34) |
| Non Drinker | 199 | 37.69 (30.90–44.48) | 27.14 (20.90–33.37) |
| p-value | 0.053 | 0.031 | |
| Amalgam Treatment | |||
| Absence | 272 | 30.88 (25.36–36.41) | 20.96 (16.09–25.82) |
| Presence | 439 | 36.22 (31.71–40.73) | 25.28 (21.20–29.37) |
| p-value | 0.145 | 0.187 | |
| Mercury Exposure through Fish and Shellfish a | |||
| Low (≤ 663 µg/y) | 237 | 27.85 (22.10–33.60) | 17.72 (12.82–22.62) |
| Middle (664–1294 µg/y) | 237 | 35.86 (29.71–42.02) | 25.74 (20.13–31.34) |
| High (≥ 1295 µg/y) | 237 | 38.82 (32.57–45.07) | 27.43 (21.70–33.15) |
| p-value | 0.034 | 0.029 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, J.-w.; Kim, B.-g.; Hong, Y.-s. The Relationship between Mercury Exposure Indices and Dietary Intake of Fish and Shellfish in Women of Childbearing Age. Int. J. Environ. Res. Public Health 2020, 17, 4907. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134907
Seo J-w, Kim B-g, Hong Y-s. The Relationship between Mercury Exposure Indices and Dietary Intake of Fish and Shellfish in Women of Childbearing Age. International Journal of Environmental Research and Public Health. 2020; 17(13):4907. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134907
Chicago/Turabian StyleSeo, Jeong-wook, Byoung-gwon Kim, and Young-seoub Hong. 2020. "The Relationship between Mercury Exposure Indices and Dietary Intake of Fish and Shellfish in Women of Childbearing Age" International Journal of Environmental Research and Public Health 17, no. 13: 4907. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134907