The Validity of Connecting Conversations: A Narrative Method to Assess Experienced Quality of Care in Nursing Homes from the Resident’s Perspective

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Connecting Conversations
2.2. Interpretation and Operationalization of Validity for Connecting Conversations
2.3. Setting and Participants
2.3.1. Care Triads
2.3.2. Interviewers
2.4. Data Collection and Procedure
2.4.1. Procedure
2.4.2. Face Validity
2.4.3. Content Validity
2.4.4. Construct Validity
2.5. Data Analysis
2.5.1. Face Validity
2.5.2. Content Validity
2.5.3. Construct Validity
2.6. Ethical Considerations
3. Results
3.1. Face Validity
3.2. Content Validity
3.3. Construct Validity
- Positive segment Resident-Caregiver (triad 008) - Interviewer: “How is the contact between you and Mister Johnson?” Caregiver: “Actually, it is very good. I experience it as being pleasant. He is very grateful that I am there for him and help him.”
- Negative segment Care environment (triad 002) - Interviewer: “Is there anything that could be better?” Resident: “Yes, the care provision. They are busy. They see everything but yeah… And the music is loud. I cannot stand that. Then I often ask if it can be softer.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Ageing and Health: Fact Sheet N°404. Available online: http://www.who.int/mediacentre/factsheets/fs404/en/ (accessed on 6 July 2020).
- Smith, D.B.; Feng, Z. The accumulated challenges of long-term care. Health Aff. 2010, 29, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Sanford, A.M.; Orrell, M.; Tolson, D.; Abbatecola, A.M.; Arai, H.; Bauer, J.M.; Cruz-Jentoft, A.J.; Dong, B.; Ga, H.; Goel, A.; et al. An international definition for “nursing home”. J. Am. Med. Dir. Assoc. 2015, 16, 181–184. [Google Scholar] [CrossRef]
- Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press: Washington, DC, USA, 2001. [Google Scholar] [CrossRef]
- Parasuraman, A.; Zeithaml, V.A.; Berry, L.L. A Conceptual Model of Service Quality and Its Implications for Future Research. J. Mark. 1985, 49, 41–50. [Google Scholar] [CrossRef]
- Goffin, K.; Mitchell, R. Innovation Management: Effective Strategy and Implementation; Macmillan Education UK: London, UK, 2016. [Google Scholar]
- Castle, N.; Ferguson, J. What is nursing home quality and how is it measured? Gerontologist 2010, 50, 426–442. [Google Scholar] [CrossRef] [Green Version]
- OECD/EU. A Good Life in Old Age? OECD Publishing: Paris, France, 2013. [Google Scholar]
- Burke, R.E.; Werner, R.M. Quality measurement and nursing homes: Measuring what matters. BMJ Qual. Amp Saf. 2019, 28, 520–523. [Google Scholar] [CrossRef]
- De Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine: A Practical Guide; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar] [CrossRef]
- Koren, M.J. Person-centered care for nursing home residents: The culture-change movement. Health Aff. 2010, 29, 312–317. [Google Scholar] [CrossRef] [Green Version]
- McCormack, B.; Roberts, T.; Meyer, J.; Morgan, D.; Boscart, V. Appreciating the ’person’ in long-term care. Int. J. Old People Nurs. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Epp, T.D. Person-centred dementia care: A vision to be refined. Can. Alzheimer Dis. Rev. 2003, 5, 14–19. [Google Scholar]
- Feinberg, L.F.; Whitlatch, C.J. Are persons with cognitive impairment able to state consistent choices? Gerontologist 2001, 41, 374–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Vlaev, I.; King, D.; Mayer, E.; Darzi, A.; Dolan, P. Subjective well-being and the measurement of quality in healthcare. Soc. Sci. Med. 2013, 99, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Sion, K.Y.J.; Haex, R.; Verbeek, H.; Zwakhalen, S.M.G.; Odekerken-Schröder, G.; Schols, J.M.G.A.; Hamers, J.P.H. Experienced Quality of Post-Acute and Long-Term Care from the Care Recipient’s Perspective–A Conceptual Framework. J. Am. Med. Dir. Assoc. 2019, 20, 1386–1390. [Google Scholar] [CrossRef] [PubMed]
- Duffy, J.R.; Hoskins, L.M. The Quality-Caring Model: Blending dual paradigms. ANS. Adv. Nurs. Sci. 2003, 26, 77–88. [Google Scholar] [CrossRef]
- Soklaridis, S.; Ravitz, P.; Nevo, G.A.; Lieff, S. Relationship-centred care in health: A 20-year scoping review. Patient Exp. J. 2016, 3, 130–145. [Google Scholar] [CrossRef] [Green Version]
- Sion, K.Y.J.; Verbeek, H.; de Boer, B.; Zwakhalen, S.M.G.; Odekerken-Schröder, G.; Schols, J.M.G.A.; Hamers, J.P.H. How to assess experienced quality of care in nursing homes from the client’s perspective: Results of a qualitative study. BMC Geriatr. 2020, 20, 67. [Google Scholar] [CrossRef] [PubMed]
- Nolan, M.R.; Davies, S.; Brown, J.; Keady, J.; Nolan, J. Beyond person-centred care: A new vision for gerontological nursing. J. Clin. Nurs. 2004, 13, 45–53. [Google Scholar] [CrossRef] [PubMed]
- LaVela, S.L.; Gallan, A.S. Evaluation and measurement of patient experience. Patient Exp. J. 2014, 1, 36. [Google Scholar]
- Kingsley, C.; Patel, S. Patient-reported outcome measures and patient-reported experience measures. BJA Educ. 2017, 17, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Sangl, J.; Buchanan, J.; Cosenza, C.; Bernard, S.; Keller, S.; Mitchell, N.; Brown, J.; Castle, N.; Sekscenski, E.; Larwood, D. The development of a CAHPS instrument for Nursing Home Residents (NHCAHPS). J. Aging Soc. Policy 2007, 19, 63–82. [Google Scholar] [CrossRef]
- Triemstra, M.; Winters, S.; Kool, R.B.; Wiegers, T.A. Measuring client experiences in long-term care in the Netherlands: A pilot study with the Consumer Quality Index Long-term Care. BMC Health Serv. Res. 2010, 10, 95. [Google Scholar] [CrossRef] [Green Version]
- Weldring, T.; Smith, S.M. Patient-reported outcomes (PROs) and patient-reported outcome measures (PROMs). Health Serv. Insights 2013, 6, 61. [Google Scholar]
- Reichheld, F.F. The one number you need to grow. Harv. Bus. Rev. 2003, 81, 46–54, 124. [Google Scholar] [PubMed]
- Bangerter, L.R.; Abbott, K.; Heid, A.; Eshraghi, K.; Van Haitsma, K. Using spontaneous commentary of nursing home residents to develop resident-centered measurement tools: A case study. Geriatr. Nurs. 2017, 38, 548–550. [Google Scholar] [CrossRef] [PubMed]
- Finucane, M.L.; Martino, S.C.; Parker, A.M.; Schlesinger, M.; Grob, R.; Cerully, J.L.; Rybowski, L.; Shaller, D. A framework for conceptualizing how narratives from health-care consumers might improve or impede the use of information about provider quality. Patient Exp. J. 2018, 5, 15–26. [Google Scholar] [CrossRef]
- Martino, S.C.; Shaller, D.; Schlesinger, M.; Parker, A.M.; Rybowski, L.; Grob, R.; Cerully, J.L.; Finucane, M.L. CAHPS and Comments: How Closed-Ended Survey Questions and Narrative Accounts Interact in the Assessment of Patient Experience. J. Patient Exp. 2017, 4, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, M.; Grob, R.; Shaller, D.; Martino, S.C.; Parker, A.M.; Finucane, M.L.; Cerully, J.L.; Rybowski, L. Taking Patients’ Narratives about Clinicians from Anecdote to Science. N. Engl. J. Med. 2015, 373, 675–679. [Google Scholar] [CrossRef]
- Heliker, D.M. A Narrative Approach to Quality Care in Long-Term Care Facilities. J. Holist. Nurs. 1997, 15, 68–81. [Google Scholar] [CrossRef]
- Hsu, M.Y.; McCormack, B. Using narrative inquiry with older people to inform practice and service developments. J. Clin. Nurs. 2012, 21, 841–849. [Google Scholar] [CrossRef]
- Lincoln, Y.S.; Guba, Y.S.L.E.G.; Guba, E.G. Naturalistic Inquiry; SAGE Publications: Thousand Oaks, CA, USA, 1985. [Google Scholar]
- Merriam, S.B. Qualitative Research and Case Study Applications in Education. Revised and Expanded from “Case Study Research in Education”; ERIC: Bristol, UK, 1998. [Google Scholar]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; De Vet, H.C.W. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J. Clin. Epidemiol. 2010, 63, 737–745. [Google Scholar] [CrossRef] [Green Version]
- Zohrabi, M. Mixed Method Research: Instruments, Validity, Reliability and Reporting Findings. Theory Pract. Lang. Stud. 2013, 3. [Google Scholar] [CrossRef]
- Clandinin, D.J.; Connelly, F.M. Narrative Inquiry: Experience and Story in Qualitative Research; Jossey-Bass: San Francisco, CA, USA, 2000; pp. 251–307. [Google Scholar]
- Overcash, J.A. Narrative research: A review of methodology and relevance to clinical practice. Crit. Rev. Oncol. Hematol. 2003, 48, 179–184. [Google Scholar] [CrossRef]
- Sitzia, J. How valid and reliable are patient satisfaction data? An analysis of 195 studies. Int. J. Qual. Health Care 1999, 11, 319–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimberlin, C.L.; Winterstein, A.G. Validity and reliability of measurement instruments used in research. Am. J. Health Syst. Pharm. 2008, 65, 2276–2284. [Google Scholar] [CrossRef] [PubMed]
- Zorginstituut Nederland. Kwaliteitskader Verpleeghuiszorg Samen Leren En Verbeteren; Zorginstituut Nederland: Diemen, The Netherlands, 2017; pp. 1–41. [Google Scholar]
- Triemstra, M.F.A. Literatuurstudie En Overzicht Van Instrumenten Kwaliteit Van Leven En Zorg Meten; Ministerie van Volksgezondheid, Welzijn en Sport: Utrecht, The Netherland, 2017. [Google Scholar]
- Schrieks, M. Waaier Cliëntervaringseinstrumenten 2017–2019; VGN: Utrecht, The Netherlands, 2017. [Google Scholar]
- Sion, K.Y.J.; Verbeek, H.; De Vries, E.; Zwakhalen, S.M.G.; Odekerken-Schröder, G.; Schols, J.M.G.A.; Hamers, J.P.H. The Feasibility of Connecting Conversations: A Narrative Method to Assess Experienced Quality of Care in Nursing Homes from the Resident’s Perspective. Int. J. Environ. Res. Public Health 2020, 17, 5118. [Google Scholar]
- Beach, M.C.; Inui, T. Relationship-centered care. A constructive reframing. J. Gen. Intern. Med. 2006, 21, S3–S8. [Google Scholar] [CrossRef]
- Verbeek, H.; Zwakhalen, S.M.G.; Schols, J.; Kempen, G.; Hamers, J.P.H. The Living Lab in Ageing and Long-Term Care: A Sustainable Model for Translational Research Improving Quality of Life, Quality of Care and Quality of Work. J. Nutr. Health Aging 2020, 24, 43–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huls, M.; Rooij, S.E.; Diepstraten, A.; Koopmans, R.; Helmich, E. Learning to care for older patients: Hospitals and nursing homes as learning environments. Med. Educ. 2015, 49, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- MAXQDA, Software for Qualitative Data Analysis; VERBI Software–Consult–Sozialforschung GmbH: Berlin, Germany, 1989.
- Corp, I. IBM SPSS Statistics for Windows; Version 25; IBM Corp.: Armonk, NY, USA, 2017. [Google Scholar]
- Black, B.S.; Rabins, P.V.; Sugarman, J.; Karlawish, J.H. Seeking assent and respecting dissent in dementia research. Am. J. Geriatr. Psychiatry 2010, 18, 77–85. [Google Scholar] [CrossRef] [Green Version]
- Holloway, I.; Freshwater, D. Vulnerable story telling: Narrative research in nursing. J. Res. Nurs. 2007, 12, 703–711. [Google Scholar] [CrossRef]
- Van Nie-Visser, N.C.; Schols, J.M.; Meesterberends, E.; Lohrmann, C.; Meijers, J.M.; Halfens, R.J. An international prevalence measurement of care problems: Study protocol. J. Adv. Nurs. 2013, 69, e18–e29. [Google Scholar] [CrossRef]
- Rahman, A.N.; Applebaum, R.A. The Nursing Home Minimum Data Set Assessment Instrument: Manifest Functions and Unintended Consequences—Past, Present, and Future. Gerontologist 2009, 49, 727–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wanous, J.P.; Reichers, A.E.; Hudy, M.J. Overall job satisfaction: How good are single-item measures? J. Appl. Psychol. 1997, 82, 247. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.A.; Issel, L.M.; McDaniel, R.R., Jr. Nursing homes as complex adaptive systems: Relationship between management practice and resident outcomes. Nurs. Res. 2003, 52, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Bedard, M.; Squire, L.; Minthorn-Biggs, M.-B.; Molloy, D.W.; Dubois, S.; O’Donnell, M.; Lever, J.A. Validity of Self-Reports in Dementia Research. Clin. Gerontol. 2003, 26, 155–163. [Google Scholar] [CrossRef]
- Applebaum, R.; Uman, C.; Straker, J. Capturing the voices of consumers in long-term care: If you ask them they will tell. Consum. Voice Choice Long Term Care 2006, 127–140. [Google Scholar]
- Milte, R.; Huynh, E.; Ratcliffe, J. Assessing quality of care in nursing homes using discrete choice experiments: How does the level of cognitive functioning impact upon older people’s preferences? Soc. Sci. Med. 2019, 238, 112466. [Google Scholar] [CrossRef]
- Cahill, S.; Diaz-Ponce, A.M. I hate having nobody here. I’d like to know where they all are: Can qualitative research detect differences in quality of life among nursing home residents with different levels of cognitive impairment? Aging Ment. Health 2011, 15, 562–572. [Google Scholar] [CrossRef]
- Whitlatch, C.J. Including the person with dementia in family care-giving research. Aging Ment. Health 2001, 5, S20–S22. [Google Scholar] [CrossRef]
- Stans, S.E.; Dalemans, R.; De Witte, L.; Beurskens, A. Challenges in the communication between ‘communication vulnerable’ people and their social environment: An exploratory qualitative study. Patient Educ. Couns. 2013, 92, 302–312. [Google Scholar] [CrossRef]
- Curyto, K.J.; Van Haitsma, K.; Vriesman, D.K. Direct observation of behavior: A review of current measures for use with older adults with dementia. Res. Gerontol. Nurs. 2008, 1, 52–76. [Google Scholar] [CrossRef]
- Mohammad, S.M.; Turney, P.D. Crowdsourcing a word–emotion association lexicon. Comput. Intell. 2013, 29, 436–465. [Google Scholar] [CrossRef] [Green Version]
- De Smedt, T.; Daelemans, W. “Vreselijk Mooi!” (Terribly Beautiful): A Subjectivity Lexicon for Dutch Adjectives. In Proceedings of the Eighth Internaitonal Conference on Language Resources and Evaluation, Istanbul, Turkey, 23–25 May 2012; pp. 3568–3572. [Google Scholar]
- Downing, S.M. Validity: On the meaningful interpretation of assessment data. Med. Educ. 2003, 37, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Altheide, D.L.; Johnson, J.M. Criteria for Assessing Interpretive Validity in Qualitative Research. In Handbook of Qualitative Research; Sage Publications Inc.: Thousand Oaks, CA, USA, 1994; pp. 485–499. [Google Scholar]
- Tuval-Mashiach, R. Raising the curtain: The importance of transparency in qualitative research. Qual. Psychol. 2017, 4, 126–138. [Google Scholar] [CrossRef]


{kind=link}
| Concept | Definition | Operationalization for Connecting Conversations | Analysis |
|---|---|---|---|
| 1. Face validity | The degree to which a narrative assessment method looks as though it is an adequate reflection of the construct to be measured [35] | The degree to which experts, interviewers and client representatives judged Connecting Conversations actually assesses residents’ experienced quality of care in nursing homes | Three separate group discussions in which evaluations by key stakeholders, client representatives, and trained interviewers were interpreted |
| 2. Content validity | The degree to which a narrative assessment method adequately represents the construct under study [35] | The degree to which Connecting Conversations has a sample of questions that covers the full concept of residents’ experienced quality of care as defined by the INDEXQUAL framework | Analyzed whether transcripts could be coded with the themes from the INDEXQUAL framework of experienced quality of long-term care for one full triad per interviewer |
| 3. Construct validity | The degree to which the stories of a narrative assessment method are consistent with hypotheses, e.g., with regard to internal relationships, relationships with scores of other assessment methods, or differences between relevant groups [35] | The degree to which data collected with Connecting Conversations can be interpreted as ratings of experienced quality of care, varying from negative to positive | Analyzed the %-positively coded segments per transcript for one full triad per interviewer. Hereafter, compared %-positive to the actors within a triad and between triads |
| The degree to which results from Connecting Conversations are similar to results from the Net Promoter Score (NPS), assessing residents’ loyalty/satisfaction | The %-positive coded segments were compared to the NPS score for all full triads of one nursing home scoring high and one scoring low on the NPS score |
| Theme | Sub-Theme | Interpretation |
|---|---|---|
| Context | Nursing home | What are the characteristics of the nursing home? |
| Person | Who was and who is the resident? | |
| Expectations | Expectations | What did the R–F–C expect from the nursing home care? |
| Word-of-mouth | What did the R–F–C hear from others about nursing home care? | |
| Personal needs | What needs does the resident have? (sense of security, belonging, continuity, purpose, achievement, significance) | |
| Past experiences | What prior experiences did the R–F–C have with care? | |
| Experiences | Experiences (daily routine) | What does an average day of the resident look like? |
| Relationship-centered care | How are the relationships in the nursing home? (more general than themes below) | |
| ● Resident–Family | How is the relationship between R–F? | |
| ● Resident–Caregiver | How is the relationship between R–C? | |
| ● Family–Caregiver | How is the relationship between F–C? | |
| Care environment | How is the subjective nursing home environment experienced? | |
| Experienced quality of care | Perceived care services | What happened during a specific experience? |
| Perceived care outcomes | How is the resident’s health status? | |
| Satisfaction | How did it make the R–F–C feel? |
| Interviewers (N = 16) | |
|---|---|
| Mean age in years (SD) | 40 (11) |
| % Female | 14 (88) |
| Occupation | |
| Nurse (%) | 10 (63) |
| Policy advisor (%) | 3 (19) |
| Nurse aid (%) | 1 (6) |
| Psychologist (%) 1 | 1 (6) |
| Health scientist (%) 1 | 1 (6) |
| Mean contracted hours per week (SD) | 32.3 (5.2) |
| Mean years working experience (SD) | 13.8 (9.7) |
| Concept | Interpretation Connecting Conversations | Main findings |
|---|---|---|
| 1. Face validity | The degree to which experts, interviewers, and client representatives judged Connecting Conversations truly assesses residents’ experienced quality of care in nursing homes | Key stakeholders (n = 7), interviewers (n = 16), and client representatives (n = 10) evaluated the design of and questions asked with Connecting Conversations to be the right formula to assess experienced quality of care in nursing homes from the resident’s perspective |
| 2. Content validity | The degree to which Connecting Conversations has an appropriate sample of questions to cover the full concept of residents’ experienced quality of care as defined by the INDEXQUAL framework | All themes and sub-themes from the INDEXQUAL framework were present in the 11 randomly selected triads. Word-of-mouth was seldom identified |
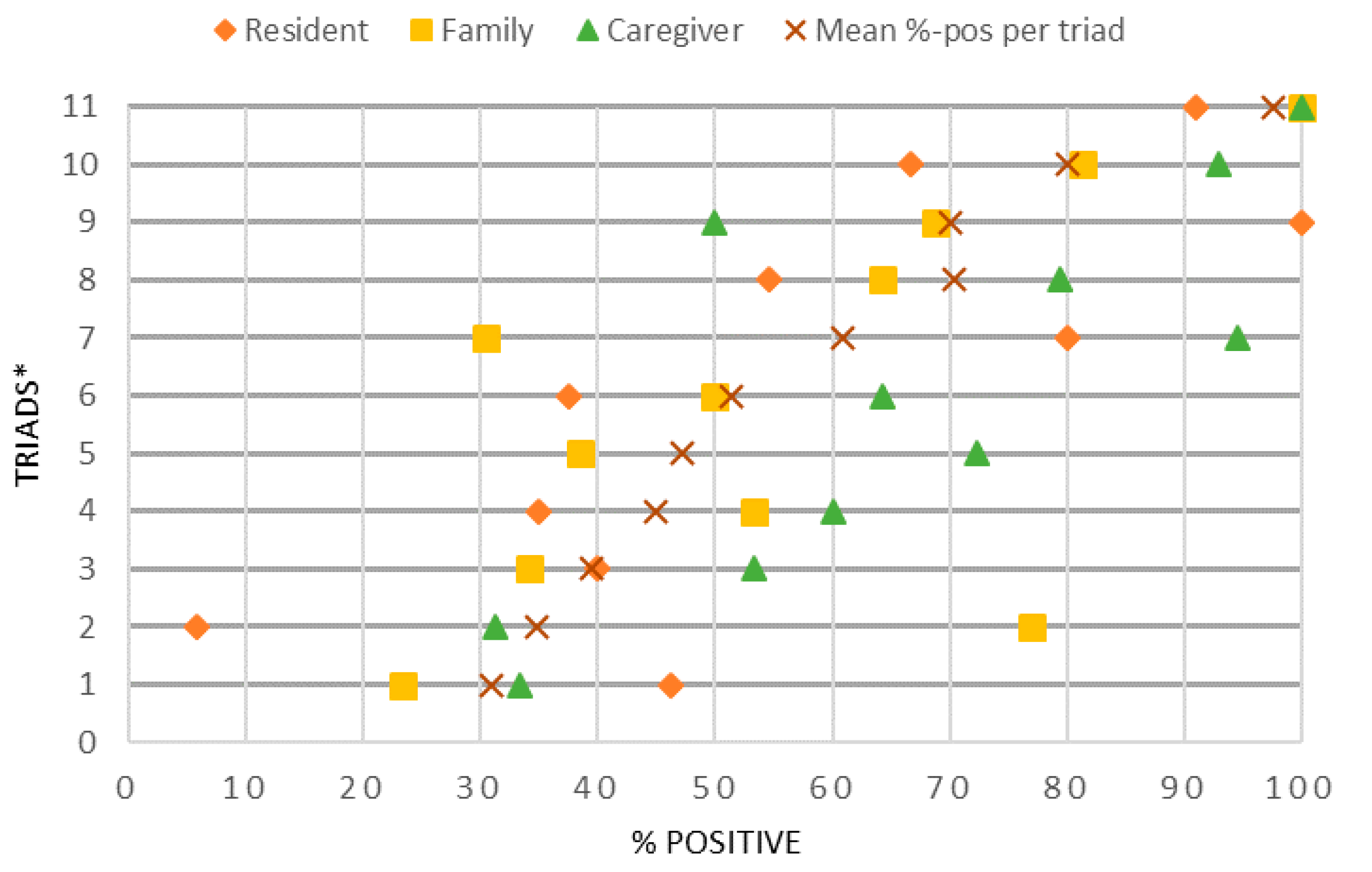
| 3. Construct validity | The degree to which data collected with Connecting Conversations can be interpreted as true ratings of experienced quality of care. Thus, there is a variety in conversations from being not positive to very positive | %-positive ranged between and within triads ● Residents, 6% * to 100% positive ● Family, 23% to 100% positive ● Caregivers, 31% to 100% |
| The degree to which results from Connecting Conversations are similar to results from the Net Promoter Score (NPS), assessing residents’ loyalty/satisfaction | A nursing home scoring low on the NPS also scored a lower %-positive compared to a nursing home scoring high on the NPS, showing a general tendency There was insufficient data for a correlation analysis |
| Theme | Sub-Theme | R | F | C | Quote |
|---|---|---|---|---|---|
| Context | Nursing home |  |  | | “It is eventually small-scale living.” (F) |
| Person |  | | | “She always enjoys to talk.” (C)“I am used to speaking dialect and that is what I feel comfortable with.” (R) | |
| Expectations | Expectations | | | | “What is being organized here, I have been totally amazed. I did not expect that.” (F) |
| Word-of-mouth | | “Her husband also has that. They all think it is too busy.” (F) | |||
| Personal need | | | | “But, close by, that is precisely what I long for. That I really live in my own village. And that is very important to me.” (R) | |
| Past experiences | |  | | “I also think through the years, she used to live elsewhere. The family therefore has certain expectations of care that cannot always be achieved.” (C) | |
| Experiences | Experiences (daily routine) | | | | “In the evening she usually goes to bed on time, because she has dialysis and then she has to be downstairs at 7.30 a.m.” (F) |
| Relationship-centered care |  | | | “The contact with the people from the other neighborhood here…she really misses that connection.” (C) | |
| Resident–Family | | | | “It’s nice every time they visit.” (R) | |
| Resident–Caregiver | | | | “She likes all staff, so a 10.” (F) | |
| Family–Caregiver | | | “Yes, actually good too; the daughter is also the first contact person.” (C) | ||
| Care environment | | | | “Because, they don’t always have time for us.” (R) | |
| Experienced quality of care | Perceived care services |  | | | “Yes, you are looked after, but that is all. You have to nag the entire week because you don’t have absorbent products and then suddenly there are six packs on the rack.” (R) |
| Perceived care outcomes | | | | “She always used to love to read, but reading is not possible anymore.” (F) | |
| Satisfaction | | | | “Sometimes a bit annoyed.” (C) |
1–7 | 8–26 | 27–37 | 38–62 | 63–150 coded segments.| Measure | Nursing Home A | Nursing Home B | ||
|---|---|---|---|---|
| Score | n | Score | n | |
| NPS score (residents) | 34 | 38 | −50 | 16 |
| % Positive Connecting Conversations (residents) | 62% | 4 | 49% | 3 |
| % Positive Connecting Conversations (triads R–F–C) | 72% | 12 | 57% | 9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sion, K.; Verbeek, H.; Aarts, S.; Zwakhalen, S.; Odekerken-Schröder, G.; Schols, J.; Hamers, J. The Validity of Connecting Conversations: A Narrative Method to Assess Experienced Quality of Care in Nursing Homes from the Resident’s Perspective. Int. J. Environ. Res. Public Health 2020, 17, 5100. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145100
Sion K, Verbeek H, Aarts S, Zwakhalen S, Odekerken-Schröder G, Schols J, Hamers J. The Validity of Connecting Conversations: A Narrative Method to Assess Experienced Quality of Care in Nursing Homes from the Resident’s Perspective. International Journal of Environmental Research and Public Health. 2020; 17(14):5100. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145100
Chicago/Turabian StyleSion, Katya, Hilde Verbeek, Sil Aarts, Sandra Zwakhalen, Gaby Odekerken-Schröder, Jos Schols, and Jan Hamers. 2020. "The Validity of Connecting Conversations: A Narrative Method to Assess Experienced Quality of Care in Nursing Homes from the Resident’s Perspective" International Journal of Environmental Research and Public Health 17, no. 14: 5100. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145100