The Feasibility of Connecting Conversations: A Narrative Method to Assess Experienced Quality of Care in Nursing Homes from the Resident’s Perspective

 , and
, and
Abstract
:1. Introduction
Theoretical Foundation
2. Materials and Methods
2.1. Connecting Conversations
2.2. Interpretation and Operationalization of Feasibility for Connecting Conversations
2.3. Setting and Participants
2.3.1. Care Triads
2.3.2. Interviewers
2.4. Data-Collection and Procedure
2.4.1. Connecting Conversations
2.4.2. Procedure
2.4.3. Completeness
2.4.4. Protocol Adherence
2.4.5. Interviewer Experiences
2.5. Data-Analysis
2.5.1. Completeness
2.5.2. Protocol Adherence
2.5.3. Interviewer Experiences
2.6. Ethical Considerations
3. Results
3.1. Completeness
3.2. Protocol Adherence
3.3. Interviewer Experiences
3.3.1. In-Depth Attention
3.3.2. Narrative Appreciative Inquiry
3.3.3. Three Perspectives
3.3.4. Learning Network
3.3.5. Commitment
3.3.6. Scheduling
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Conversations

{kind=link}
{kind=link}
{kind=link}
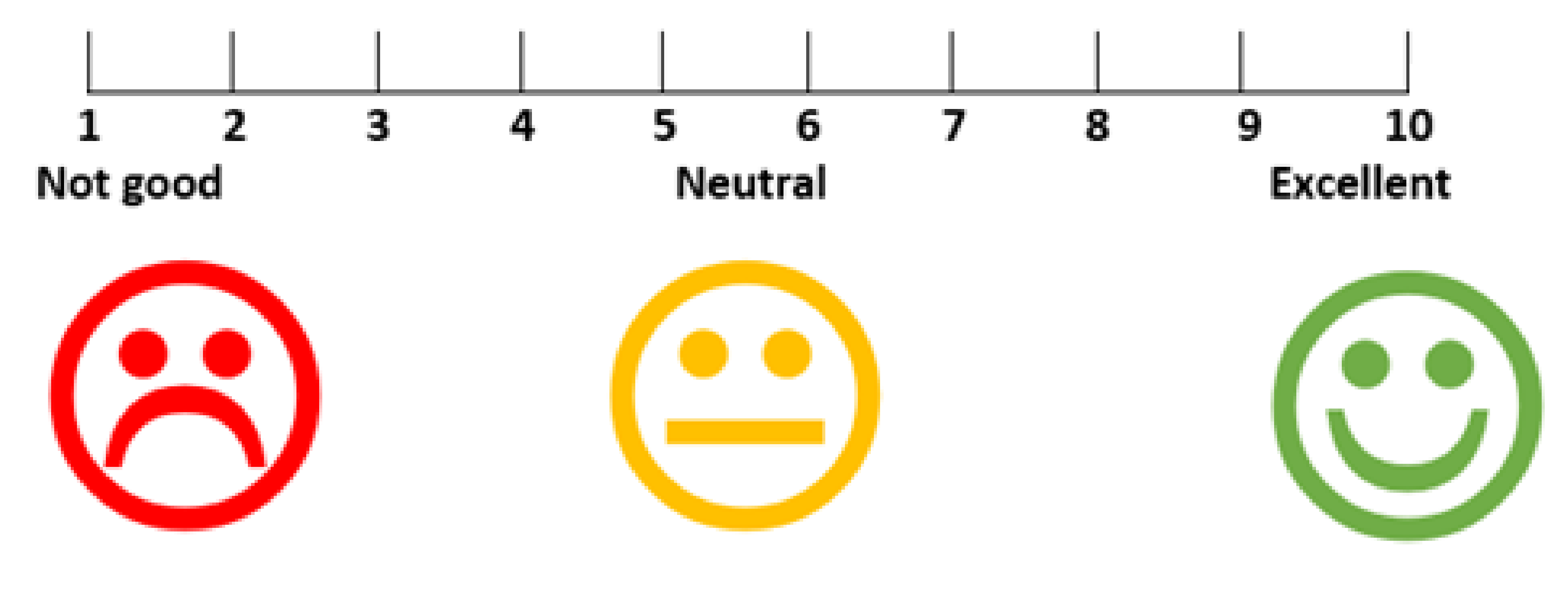
| 1a 1b | On a scale of 1 to 10, how would you grade your life at this moment? What is needed to make that a [grade +1]? |
| 2a 2b | On a scale of 1 to 10, how would you grade the caregivers that are involved with your daily care provision? What is needed to make that a [grade +1]? |
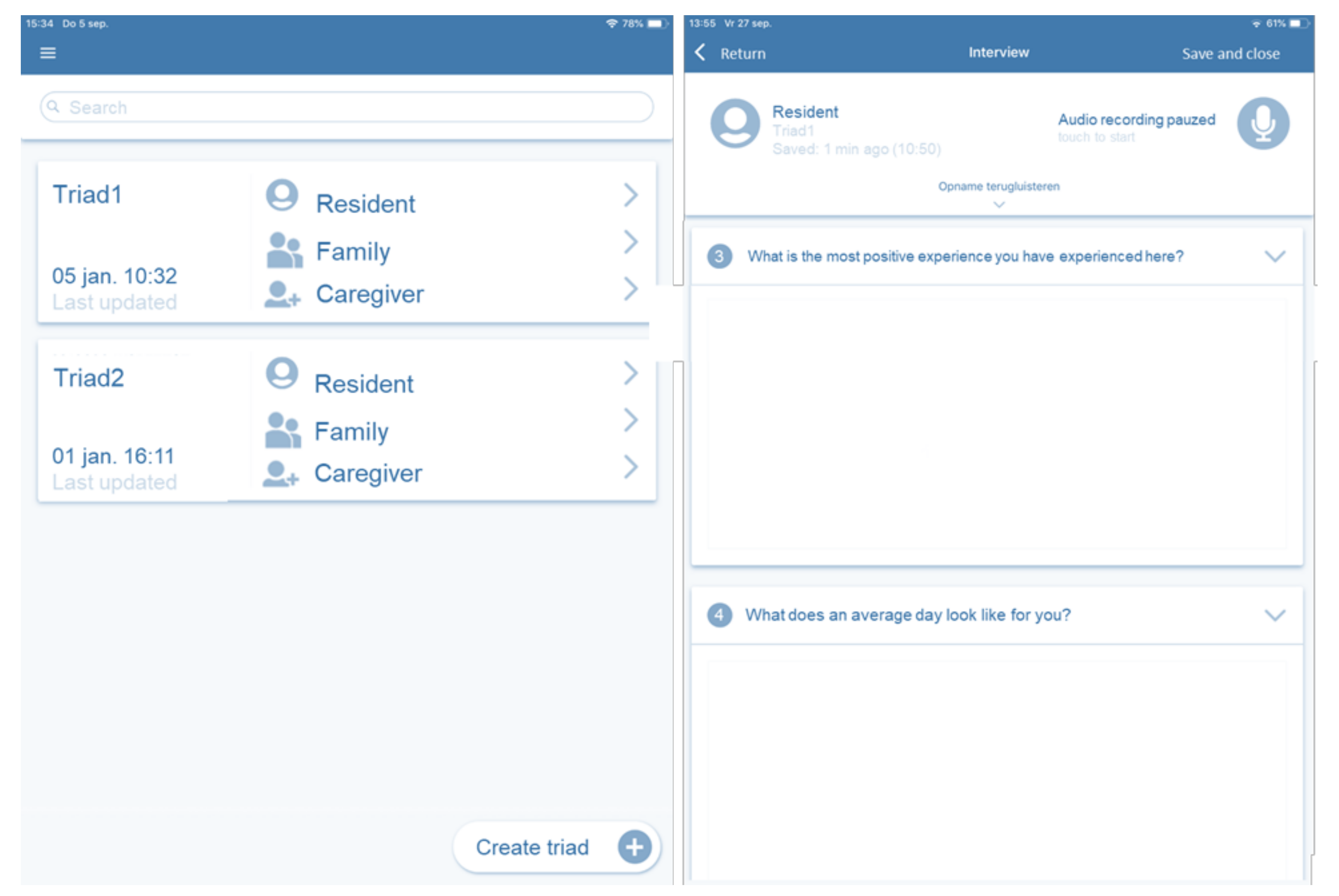
| 3 | What is the most positive experience you have experienced here? |
| 4 | What does an average day look like for you? |
| 5a 5b | What is pleasant about your contact with the caregivers here? What could be different about your contact with the caregivers here? |
| 6a 6b | What is pleasant about your contact with your family? What could be different about your contact with the family here? |
| 7a 7b | What goes well here? What could be done more here? |
| 8 | Is there anything left you would like to share that has not been addressed yet? |
| Probing questions | Why? What is going well? What could be done more? How did that make you feel? Can you give an example? |

Care Triads Recruitment
Appendix A.2. Registration
- signing informed consent;
- collecting participant demographics;
- presenting semi-structured questions and suggestions for probing questions;
- typing summative answers to each question;
- audio recording and replaying of conversations;
- viewing collected data through a web portal.

Appendix A.3. Training
Appendix A.4. Certificate
Appendix A.5. Learning Network
Appendix A.6. Analysis
- (1)
- the questions asked;
- (2)
- summative answer resident;
- (3)
- summative answer family;
- (4)
- summative answer caregiver.
| Q2. On a scale of 1 to 10, how would you grade the caregivers that are involved with your daily care provision? | “9, because they do everything they can. It’s just those girls have little time. But they need to see residents within a certain time and cannot just sit around with you.” | “Insufficient, because in her opinion very many care providers do not treat her as a person, but as a thing that needs to be dressed quickly.” | “8, because the wishes of the client are met, for example breakfast in bed and care is provided later.” |
Appendix A.7. Report
| 1 | Core Principles of Connecting Conversations |
|---|---|
| 2 | Details on how many conversations were performed in which ward |
| 3 | To what degree were there many similarities or differences between the resident, family and caregiver within each triad? |
| 4 | What is going well on the ward? (discover) |
| 5 | Quotes supporting results on Section 4 |
| 6 | What could be done more frequently on the ward? (dream) |
| 7 | Quotes supporting results on Section 5 |
| 8 | Discussion asking attendees what they think of the results, what they can learn from the results and what they are going to do with the results? |
References
- World Health Organisation. Ageing and Health: Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 6 July 2020).
- World Health Organisation. World Report on Ageing and Health; World Health Organization: Luxembourgh, Luxembourgh, 2015. [Google Scholar]
- Sanford, A.M.; Orrell, M.; Tolson, D.; Abbatecola, A.M.; Arai, H.; Bauer, J.M.; Cruz-Jentoft, A.J.; Dong, B.; Ga, H.; Goel, A.; et al. An international definition for “nursing home”. J. Am. Med. Dir. Assoc. 2015, 16, 181–184. [Google Scholar] [CrossRef] [PubMed]
- OECD/EU. A Good Life in Old Age? OECD Publishing: Paris, France, 2013. [Google Scholar]
- Miller, S.C.; Miller, E.A.; Jung, H.Y.; Sterns, S.; Clark, M.; Mor, V. Nursing home organizational change: The “Culture Change” movement as viewed by long-term care specialists. Med. Care Res. Rev. MCRR 2010, 67, 65s–81s. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, S.; Shier, V.; Saliba, D. Transforming nursing home culture: Evidence for practice and policy. Gerontologist 2014, 54 (Suppl. 1), S1–S5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakrem, S.; Vinsnes, A.G.; Seim, A. Residents’ experiences of interpersonal factors in nursing home care: A qualitative study. Int. J. Nurs. Stud. 2011, 48, 1357–1366. [Google Scholar] [CrossRef]
- Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press (US): Washington, DC, USA, 2001. [Google Scholar] [CrossRef]
- Castle, N.; Ferguson, J. What is nursing home quality and how is it measured? Gerontologist 2010, 50, 426–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Nie-Visser, N.C.; Schols, J.M.; Meesterberends, E.; Lohrmann, C.; Meijers, J.M.; Halfens, R.J. An international prevalence measurement of care problems: Study protocol. J. Adv. Nurs. 2013, 69, e18–e29. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.N.; Applebaum, R.A. The Nursing Home Minimum Data Set Assessment Instrument: Manifest Functions and Unintended Consequences—Past, Present, and Future. Gerontologist 2009, 49, 727–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edvardsson, D.; Baxter, R.; Corneliusson, L.; Anderson, R.A.; Beeber, A.; Boas, P.V.; Corazzini, K.; Gordon, A.L.; Hanratty, B.; Jacinto, A.; et al. Advancing Long-Term Care Science Through Using Common Data Elements: Candidate Measures for Care Outcomes of Personhood, Well-Being, and Quality of Life. Gerontol. Geriatr. Med. 2019, 5, 2333721419842672. [Google Scholar] [CrossRef]
- De Roo, M.L.; Leemans, K.; Claessen, S.J.J.; Cohen, J.; Pasman, H.R.W.; Deliens, L.; Francke, A.L. Quality Indicators for Palliative Care: Update of a Systematic Review. J. Pain Symptom Manag. 2013, 46, 556–572. [Google Scholar] [CrossRef] [PubMed]
- Mor, V.; Leone, T.; Maresso, A. Regulating Long-Term Care Quality: An. International Comparison; Cambridge University Press: Cambridge, UK, 2014. [Google Scholar] [CrossRef]
- Clarke, A.; Rao, M. Developing quality indicators to assess quality of care. Qual. Saf. Health Care 2004, 13, 248–249. [Google Scholar] [CrossRef] [Green Version]
- Lewis, R.C.; Booms, B.H. The marketing aspects of service quality. Emerg. Perspect. Serv. Mark. 1983, 65, 99–107. [Google Scholar]
- Voorhees, C.M.; Fombelle, P.W.; Gregoire, Y.; Bone, S.; Gustafsson, A.; Sousa, R.; Walkowiak, T. Service encounters, experiences and the customer journey: Defining the field and a call to expand our lens. J. Bus. Res. 2017, 79, 269–280. [Google Scholar] [CrossRef]
- Lemon, K.N.; Verhoef, P.C. Understanding Customer Experience Throughout the Customer Journey. J. Mark. 2016, 80, 69–96. [Google Scholar] [CrossRef]
- McCormack, B.; Roberts, T.; Meyer, J.; Morgan, D.; Boscart, V. Appreciating the ‘person’ in long-term care. Int. J. Older People Nurs. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Wilberforce, M.; Challis, D.; Davies, L.; Kelly, M.P.; Roberts, C.; Clarkson, P. Person-centredness in the community care of older people: A literature-based concept synthesis. Int. J. Soc. Welf. 2017, 26, 86–98. [Google Scholar] [CrossRef] [Green Version]
- Koren, M.J. Person-centered care for nursing home residents: The culture-change movement. Health Aff. 2010, 29, 312–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duffy, J.R.; Hoskins, L.M. The Quality-Caring Model: Blending dual paradigms. ANS Adv. Nurs. Sci. 2003, 26, 77–88. [Google Scholar] [CrossRef]
- Beach, M.C.; Inui, T. Relationship-centered care. A constructive reframing. J. Gen. Intern. Med. 2006, 21 (Suppl. 1), S3–S8. [Google Scholar] [CrossRef]
- Gummesson, E. Extending the service-dominant logic: From customer centricity to balanced centricity. J. Acad. Mark. Sci. 2008, 36, 15–17. [Google Scholar] [CrossRef]
- Nolan, M.; Brown, J.; Davies, S.; Nolan, J.; Keady, J. The Senses Framework: Improving Care for Older People through A Relationship-Centred Approach; Getting Research into Practice (GRiP) Report No 2.; University of Sheffield: Sheffield, UK, 2006. [Google Scholar]
- OECD. Ministerial Statement: The Next Generation of Health Reforms; OECD Publishing: Paris, France, 2017. [Google Scholar]
- Nadash, P.; Hefele, J.; Wang, J.; Barooah, A. Nursing home satisfaction measures: What is their relationship to quality? Innov. Aging 2017, 1, 542. [Google Scholar] [CrossRef]
- Corazzini, K.N.; Anderson, R.A.; Bowers, B.J.; Chu, C.H.; Edvardsson, D.; Fagertun, A.; Gordon, A.L.; Leung, A.Y.M.; McGilton, K.S.; Meyer, J.E.; et al. Toward Common Data Elements for International Research in Long-term Care Homes: Advancing Person-Centered Care. J. Am. Med. Dir. Assoc. 2019, 20, 598–603. [Google Scholar] [CrossRef]
- Kellett, U. Searching for new possibilities to care: A qualitative analysis of family caring involvement in nursing homes. Nurs. Inq. 1999, 6, 9–16. [Google Scholar] [CrossRef] [PubMed]
- McGilton, K.S.; Boscart, V.M. Close care provider-resident relationships in long-term care environments. J. Clin. Nurs. 2007, 16, 2149–2157. [Google Scholar] [CrossRef] [PubMed]
- Zorginstituut Nederland. Kwaliteitskader Verpleeghuiszorg Samen Leren en Verbeteren; Zorginstituut Nederland: Diemen, The Netherlands, 2017; pp. 1–41. [Google Scholar]
- Curyto, K.J.; Van Haitsma, K.; Vriesman, D.K. Direct observation of behavior: A review of current measures for use with older adults with dementia. Res. Gerontol. Nurs. 2008, 1, 52–76. [Google Scholar] [CrossRef] [PubMed]
- Weldring, T.; Smith, S.M.S. Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health Serv. Insights 2013, 6, 61–68. [Google Scholar] [CrossRef]
- Zuidgeest, M.; Delnoij, D.M.J.; Luijkx, K.G.; de Boer, D.; Westert, G.P. Patients’ experiences of the quality of long-term care among the elderly: Comparing scores over time. BMC Health Serv. Res. 2012, 12, 26. [Google Scholar] [CrossRef] [Green Version]
- LaVela, S.L.; Gallan, A.S. Evaluation and measurement of patient experience. Patient Exp. J. 2014, 1, 28–36. [Google Scholar]
- Kenyon, G.; Randall, W. Introduction. J. Aging Stud. 2015, 34, 143–145. [Google Scholar] [CrossRef]
- Heliker, D.M. A Narrative Approach to Quality Care in Long-Term Care Facilities. J. Holist. Nurs. 1997, 15, 68–81. [Google Scholar] [CrossRef]
- Finucane, M.L.; Martino, S.C.; Parker, A.M.; Schlesinger, M.; Grob, R.; Cerully, J.L.; Rybowski, L.; Shaller, D. A framework for conceptualizing how narratives from health-care consumers might improve or impede the use of information about provider quality. Patient Exp. J. 2018, 5, 15–26. [Google Scholar] [CrossRef]
- Beswick, N. Determination of the inter-rater reliability of the Edmonton Narrative Norms Instrument. In Department of Speech Pathology and Audiology; Unpublished Project Report; Universiy of Alberta: Alberta, Canada, 2008. [Google Scholar]
- Bettmann, J.E.; Lundahl, B.W. Tell me a story: A review of narrative assessments for preschoolers. Child. Adolesc. Soc. Work J. 2007, 24, 455–475. [Google Scholar] [CrossRef]
- Hendriks, L.; Veerbeek, M.A.; Volker, D.; Veenendaal, L.; Willemse, B.M. Life review therapy for older adults with depressive symptoms in general practice: Results of a pilot evaluation. Int. Psychogeriatr. 2019, 31, 1801–1808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, R.N. The Life Review: An Interpretation of Reminiscence in the Aged. Psychiatry 1963, 26, 65–76. [Google Scholar] [CrossRef]
- De Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine: A Practical Guide; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar] [CrossRef]
- Triemstra, M.F.A. Literatuurstudie en Overzicht van Instrumenten Kwaliteit van Leven en Zorg Meten; Ministerie van Volksgezondheid; Welzijn en Sport: Utrecht, The Netherlands, 2017. [Google Scholar]
- Sion, K.Y.J.; Haex, R.; Verbeek, H.; Zwakhalen, S.M.G.; Odekerken-Schröder, G.; Schols, J.M.G.A.; Hamers, J.P.H. Experienced Quality of Post-Acute and Long-Term Care From the Care Recipient’s Perspective—A Conceptual Framework. J. Am. Med. Dir. Assoc. 2019, 20, 1386–1390. [Google Scholar] [CrossRef]
- Sion, K.Y.J.; Verbeek, H.; de Boer, B.; Zwakhalen, S.M.G.; Odekerken-Schröder, G.; Schols, J.M.G.A.; Hamers, J.P.H. How to assess experienced quality of care in nursing homes from the client’s perspective: Results of a qualitative study. BMC Geriatr. 2020, 20, 67. [Google Scholar] [CrossRef]
- Sion, K.Y.J.; Verbeek, H.; Aarts, S.; Zwakhalen, S.M.G.; Odekerken-Schröder, G.; Schols, J.M.G.A.; Hamers, J.P.H. The Validity of Connecting Conversations: A Narrative Method to Assess Experienced Quality of Care in Nursing Homes from the Resident’s Perspective. Int. J. Environ. Res. Public Health 2020, 17, 5100. [Google Scholar] [CrossRef]
- Soklaridis, S.; Ravitz, P.; Nevo, G.A.; Lieff, S. Relationship-centred care in health: A 20-year scoping review. Patient Exp. J. 2016, 3, 130–145. [Google Scholar] [CrossRef] [Green Version]
- Nolan, M.R.; Davies, S.; Brown, J.; Keady, J.; Nolan, J. Beyond person-centred care: A new vision for gerontological nursing. J. Clin. Nurs. 2004, 13, 45–53. [Google Scholar] [CrossRef]
- Cooperrider, D.; Srivastva, S. Appreciative Inquiry in Organizational Life. Res. Organ. Chang. Dev. 1987, 1, 129–169. [Google Scholar]
- Cooperrider, D.L.; Whitney, D.K.; Stavros, J.M. Appreciative Inquiry Handbook; Lakeshore Communications Inc: Bedford Heights, OH, USA, 2003. [Google Scholar]
- Dewar, B.; MacBride, T. Developing caring conversations in care homes: An appreciative inquiry. Health Soc. Care Community 2017, 25, 1375–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beauchamp, J.M.; Glessner, T.M. Appreciative Inquiry Promotes Nursing Culture Change. Clin. Nurse Spec. 2006, 20, 82. [Google Scholar] [CrossRef]
- Wenger, E. Communities of Practice: Learning, Meaning, and Identity; Cambridge University Press: Cambridge, UK, 1998. [Google Scholar] [CrossRef]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, H.; Zwakhalen, S.M.G.; Schols, J.M.G.A.; Kempen, G.I.J.M.; Hamers, J.P.H. The Living Lab in Ageing and Long-Term Care: A Sustainable Model for Translational Research Improving Quality of Life, Quality of Care and Quality of Work. J. Nutr. Health Aging 2019, 24, 43–47. [Google Scholar] [CrossRef] [Green Version]
- Nickerson, R.S. Confirmation Bias: A Ubiquitous Phenomenon in Many Guises. Rev. Gen. Psychol. 1998, 2, 175–220. [Google Scholar] [CrossRef]
- DeMarrais, K.B.; Lapan, S.D., IV. Qualitative Interview Studies: Learning Through Experience. In Foundations for Research: Methods of Inquiry in Education and the Social Sciences; L. Erlbaum Associates: Mahwah, NJ, USA, 2004. [Google Scholar]
- MAXQDA. Software for Qualitative Data Analysis; VERBI Software—Consult—Sozialforschung GmbH: Berlin, Germany, 1989–2020. [Google Scholar]
- Black, B.S.; Rabins, P.V.; Sugarman, J.; Karlawish, J.H. Seeking assent and respecting dissent in dementia research. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2010, 18, 77–85. [Google Scholar] [CrossRef] [Green Version]
- Villar, F.; Serrat, R. Changing the culture of long-term care through narrative care: Individual, interpersonal, and institutional dimensions. J. Aging Stud. 2017, 40, 44–48. [Google Scholar] [CrossRef]
- Meerveld, E.V.; Vos, F.S.M.; Bos, E.H.; Jansen, Y.J.F.M. Meerwaarde van een Lerend Netwerk, Casus National Inzetbaarheidsplan; TNO: Hoofddorp, The Netherlands, 2014. [Google Scholar]
- Boyd, E.M.; Fales, A.W. Reflective Learning: Key to Learning from Experience. J. Humanist. Psychol. 1983, 23, 99–117. [Google Scholar] [CrossRef]
- Magnussen, I.-L.; Alteren, J.; Bondas, T. Appreciative inquiry in a Norwegian nursing home: A unifying and maturing process to forward new knowledge and new practice. Int. J. Qual. Stud. Health Well Being 2019, 14, 1559437. [Google Scholar] [CrossRef]
- NCHR&D. Quality of Life in Care Homes: A Review of the Literature; Help the Aged: London, UK, 2007. [Google Scholar]
- Dewar, B.; Nolan, M. Caring about caring: Developing a model to implement compassionate relationship centred care in an older people care setting. Int. J. Nurs. Stud. 2013, 50, 1247–1258. [Google Scholar] [CrossRef]
- Anderson, R.A.; Issel, L.M.; McDaniel, R.R., Jr. Nursing homes as complex adaptive systems: Relationship between management practice and resident outcomes. Nurs. Res. 2003, 52, 12–21. [Google Scholar] [CrossRef]
- Woo, K.; Milworm, G.; Dowding, D. Characteristics of quality improvement champions in nursing homes: A systematic review with implications for evidence-based practice. Worldviews Evid. Based Nurs. 2017, 14, 440–446. [Google Scholar] [CrossRef]
- Backman, A.; Sjögren, K.; Lindkvist, M.; Lövheim, H.; Edvardsson, D. Towards person-centredness in aged care—Exploring the impact of leadership. J. Nurs. Manag. 2016, 24, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Stiegler, A.; Biedinger, N. Interviewer Skills and Training. GESIS Surv. Guidel. 2016, 1–8. [Google Scholar] [CrossRef]
- Merriam, S.B. Qualitative Research and Case Study Applications in Education. Revised and Expanded from “Case Study Research in Education; Jossey-Bass: San Francisco, CA, USA, 1998. [Google Scholar]
- Clandinin, D.J.; Connelly, F.M. Narrative Inquiry: Experience and Story in Qualitative Research; Jossey-Bass: San Francisco, CA, USA, 2000. [Google Scholar]
- Chang, S.J. Lived Experiences of Nursing Home Residents in Korea. Asian Nurs. Res. 2013, 7, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Chuang, Y.H.; Abbey, J.A.; Yeh, Y.C.; Tseng, I.J.; Liu, M.F. As they see it: A qualitative study of how older residents in nursing homes perceive their care needs. Collegian 2015, 22, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Drageset, J.; Haugan, G.; Tranvag, O. Crucial aspects promoting meaning and purpose in life: Perceptions of nursing home residents. BMC Geriatr. 2017, 17, 254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, H.; Paliadelis, P. Older peoples’ experiences of living in a residential aged care facility in Australia. Australas. J. Ageing 2016, 35, E6–E10. [Google Scholar] [CrossRef]
- Applebaum, R.; Uman, C.; Straker, J. Capturing the voices of consumers in long-term care: If you ask them they will tell. In Consumer Voice and Choice in Long-Term Care; Springer Publishing Company: New York, NY, USA, 2006; pp. 127–140. [Google Scholar]
- Milte, R.; Huynh, E.; Ratcliffe, J. Assessing quality of care in nursing homes using discrete choice experiments: How does the level of cognitive functioning impact upon older people’s preferences? Soc. Sci. Med. 2019, 238, 112466. [Google Scholar] [CrossRef]
- De Boer, B.; Beerens, H.C.; Zwakhalen, S.M.; Tan, F.E.; Hamers, J.P.; Verbeek, H. Daily lives of residents with dementia in nursing homes: Development of the Maastricht electronic daily life observation tool. Int. Psychogeriatr. 2016, 28, 1333–1343. [Google Scholar] [CrossRef]
- Brooker, D. Dementia Care Mapping. In Principles and Practice of Geriatric Psychiatry; John Wiley & Sons, Ltd: West Sussex, UK, 2010. [Google Scholar] [CrossRef]
- Brooker, D.; La Fontaine, J.; De Vries, K.; Latham, I. The development of PIECE-dem: Focussing on the experience of care for people living with advanced dementia. Br. Psychol. Soc. Clin. Psychol. Forum 2013, 250, 38–46. [Google Scholar]
- Bohlmeijer, E.; Kenyon, G.; Randall, W. Toward a Narrative Turn in Health Care. In Storying Later Life: Issues, Investigations, and Interventions in Narrative Gerontology; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Usai, A.; Pironti, M.; Mital, M.; Mejri, C.A. Knowledge discovery out of text data: A systematic review via text mining. J. Knowl. Manag. 2018, 22, 1471–1488. [Google Scholar] [CrossRef] [Green Version]
- Safran, D.G.; Miller, W.; Beckman, H. Organizational dimensions of relationship-centered care theory, evidence, and practice. J. Gen. Intern. Med. 2006, 21, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Van Achterberg, T.; Schoonhoven, L.; Grol, R. Nursing implementation science: How evidence-based nursing requires evidence-based implementation. J. Nurs. Scholarsh. Off. Publ. Sigma Tau Int. Honor Soc. Nurs. 2008, 40, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Christie, H.L.; Martin, J.L.; Connor, J.; Tange, H.J.; Verhey, F.R.J.; de Vugt, M.E.; Orrell, M. eHealth interventions to support caregivers of people with dementia may be proven effective, but are they implementation-ready? Internet Interv. 2019, 18, 100260. [Google Scholar] [CrossRef]
- Flanagan, J.C. The critical incident technique. Psychol. Bull. 1954, 51, 327–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serrat, O. The Critical Incident Technique. In Knowledge Solutions: Tools, Methods, and Approaches to Drive Organizational Performance; Springer Singapore: Singapore, 2017; pp. 1077–1083. [Google Scholar] [CrossRef] [Green Version]
- Wilber, K. An integral theory of consciousness. J. Conscious. Stud. 1997, 4, 71–92. [Google Scholar]
- Bradley, S.P.; Nolan, R.L. Sense and Respond: Capturing Value in the Network Era; Harvard Business School Press: Boston, MA, USA, 1998. [Google Scholar]

| Element | Main Description |
|---|---|
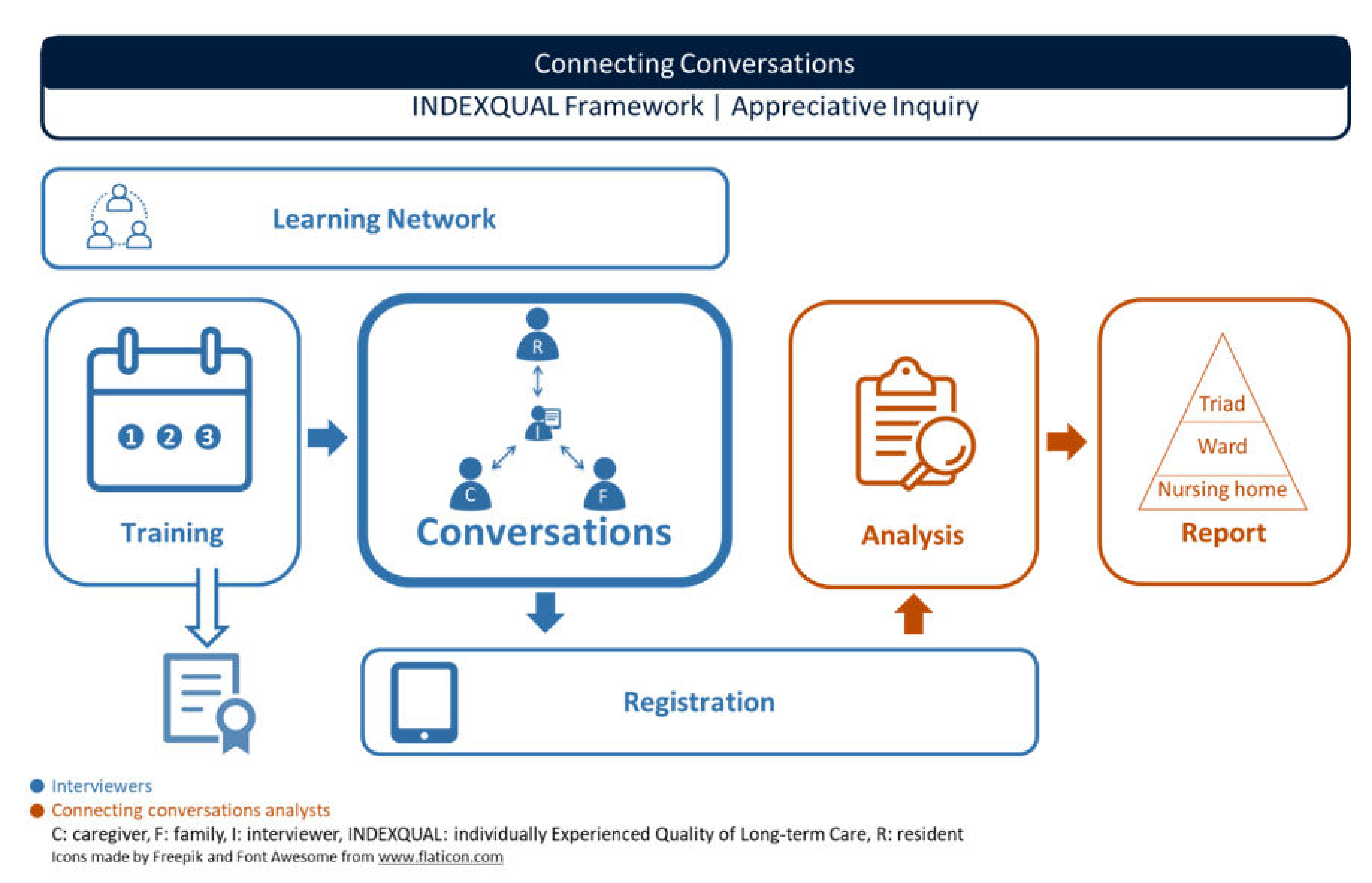
| Training | Interviewers need to follow a mandatory three-day (3 h/day) training to assure the quality and reliability of performing and registering Connecting Conversations. The training focusses on connecting, practicing and sharing experiences, and has adopted an appreciative inquiry approach. Successful attendance results in a certificate. |
| Conversations | Semi-structured questions are asked in separate conversation with a resident, family member and professional caregiver of that resident, who each answer from the resident’s perspective. Questions are based on the INDEXQUAL framework and are formulated from an appreciative inquiry approach. Main topics: resident’s life, satisfaction with care provision, most positive experience, description of an average day in the nursing home and relationships between the resident, family and caregiver. |
| Registration | The Connecting Conversations app supports interviewers to perform, register and view the conversations. Main features app: documenting informed consent, participant demographics, summative answers, audio recording and viewing collected data. |
| Learning network | The learning network provides a platform for interviewers in which they can learn from and with each other through continuous interaction [54]. Interviewers from different care organizations follow the training together and perform conversations in each other’s care organizations, thus not where they themselves are employed. This provides for independent interviewers and the opportunity for interviewers to learn from daily practices in another nursing home environment. |
| Analysis | The written texts, as reported in the app, are analyzed by two researchers with content analysis [55]. |
| Report | The analyzed data are presented on ward level in a factsheet with supporting ‘quotes’. Additional reports on triad and nursing home level can be delivered upon request. |
| Feasibility Concept | Definition | Operationalization for Connecting Conversations
| Analysis |
|---|---|---|---|
| Completeness | Extent to which Connecting Conversations was completed as planned | All planned triads were randomly selected and completed in the learning network as planned Interviewers completed the training and all planned conversations
|
|
| Protocol adherence | Extent to which the conversations were performed as planned | All interviewers followed the Connecting Conversations’ protocol as taught during the training.
|
|
| Interviewer experiences | Interviewers’ satisfaction with Connecting Conversations and experienced facilitators and barriers | All interviewers evaluated all components of Connecting Conversations: training, scheduling conversations, performing conversations and registering conversations.
| Deductive coding of interviewer experiences, categorized into elements that were appreciated and that were considered challenging |
| Care Triads | Total | Field-Testing Cycle 1 | Field-Testing Cycle 2 |
|---|---|---|---|
| Planned conversations n | |||
| → Total | 405 | 240 | 165 |
| → Triads R-F-C | 135 | 80 | 55 |
| Performed conversations n (%) | |||
| → Total | 275 (68) 3 | 149 (62) 5 | 126 (76) 7 |
| → Resident (R) | 89 (66) | 46 (58) | 43 (78) |
| → Family (F) | 83 (61) | 46 (58) | 37 (67) |
| → Caregiver (C) | 103 (76) | 57 (71) | 46 (84) |
| → Total triads/dyads | 103 (76) | 57 (71) | 46 (84) |
| → Full triads R-F-C | 68 (50) 4 | 34 (43) 6 | 34 (60) 8 |
| → F-C combination 1 | 14 (10) | 11 (14) | 3 (5) |
| → R-C combination | 20 (15) | 11 (14) | 9 (16) |
| → Full triads missing | 32 (24) | 23 (29) | 9 (16) |
| Mean/Median minutes conversations (range) | |||
| → Total | 19/17 (3–79) | 18/15 (3–54) | 21/18 (4–79) |
| → Resident (R) | 21/17 (4–79) | 18/14 (6–54) | 24/22 (4–79) |
| → Family (F) | 21/19 (6–48) | 21/22 (6–39) | 21/18 (7–48) |
| → Caregiver (C) | 17/14 (3–55) | 15/14 (3–41) | 19/16 (4–55) |
| Interviewers’ characteristics | |||
| Total interviewers n | 35 | 16 | 19 |
| Mean age in years (SD) | 40 (11) | 40 (11) | 42 (11) |
| Females (%) | 31 (89) | 14 (88) | 17 (89) |
| Occupation n (%) | |||
| → Nurse | 10 (29) | 6 (38) | 4 (21) |
| → Baccalaureate-educated nurse | 9 (26) | 4 (25) | 5 (26) |
| → Policy advisor | 5 (14) | 3 (19) | 2 (11) |
| → Care manager | 2 (6) | 0 | 2 (11) |
| → Recreational coach | 2 (6) | 0 | 2 (11) |
| → Psychologist 2 | 3 (9) | 1 (6) | 2 (11) |
| → Health scientist 2 | 2 (6) | 1 (6) | 1 (5) |
| → Nurse aid | 1 (3) | 1 (6) | 0 |
| → Complaints officer | 1 (3) | 0 | 1 (5) |
| Mean contracted hours per week (SD) | 32.4 (5.2) | 32.3 (5.2) | 32.6 (5.3) |
| Mean years working experience (SD) | 13.1 (11.0) | 13.8 (9.7) | 12.4 (12.1) |
| Training attendance all 3 days n (%) | 30 (86) | 13 (81) | 17 (89) |
| Training attendance 2 out of 3 days n (%) | 5 (14) | 3 (19) | 2 (11) |
| Total | Resident (R) | Family (F) | Caregiver (C) | |
|---|---|---|---|---|
| N = 125 | N = 36 | N = 38 | N = 51 | |
| Question 1 quality of life n (%) | 107 (86) | 24 (67) | 36 (95) | 47 (92) |
| Question 2 satisfaction caregivers n (%) | 113 (90) | 29 (81) | 34 (89) | 50 (98) |
| Question 3 most positive n (%) | 116 (93) | 30 (83) | 36 (95) | 50 (98) |
| Question 4 average day n (%) | 113 (90) | 26 (72) | 37 (97) | 50 (98) |
| Question 5 relationships n (%) 2 | 102 (82) | 24 (67) | 34 (89) | 44 (86) |
| Question 6 relationships n (%) 3 | 106 (85) | 25 (69) | 33 (87) | 48 (94) |
| Average questions asked % | 88 | 73 | 92 | 94 |
| All six questions asked n (%) | 79 (63) | 14 (39) | 28 (74) | 37 (73) |
| Four or five questions asked n (%) | 30 (24) | 10 (28) | 8 (21) | 14 (27) |
| Less than four questions asked n (%) | 14 (11) | 12 (33) | 2 (5)4 | 0 |
| Probing questions n (%) | 124 (99) | 36 (100) | 37 (97) | 51 (100) |
| Paraphrasing n (%) | 86 (69) | 22 (61) | 29 (76) | 35 (69) |
| ≥50% responder words spoken n (%) | 108 (86) | 23 (64) | 37 (97) | 50 (98) |
| Facilitators | Reason Why Important | |
|---|---|---|
| Vision | Adopt an appreciative inquiry approach when introducing, implementing and embedding Connecting Conversations into the nursing home | To enhance commitment and enthusiasm; and set an example of the method’s positive impact: ‘practice what you preach’ |
| Have a clear purpose for what the results will be used | To decide on the magnitude of the assessment and the format of the report(s) | |
| Prerequisites | Random selection of triads on a ward | To avoid selection bias |
| Assure interviewers have conversations elsewhere than where they are employed (external interviewers) | To enhance the learning network and provide respondents a safe environment to share their stories | |
| Provide sufficient time for training, conversations and the learning network | To ensure quality of the conducted conversations | |
| Assign a contact person in the nursing home who is responsible for facilitating the visiting interviewer (scheduling conversations; informing residents, family and staff on the ward) | To enhance completeness and to create a safe environment for the visiting interviewer | |
| Performance | Make an effort to have conversations with each selected resident, regardless of his or her (cognitive) health status | To embrace an inclusive approach, in which residents are provided with self-determination |
| Think in solutions when scheduling conversations, for example by allowing full-time employed family to have the conversation by phone or during evening hours | To embrace an inclusive and appreciative approach |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sion, K.; Verbeek, H.; de Vries, E.; Zwakhalen, S.; Odekerken-Schröder, G.; Schols, J.; Hamers, J. The Feasibility of Connecting Conversations: A Narrative Method to Assess Experienced Quality of Care in Nursing Homes from the Resident’s Perspective. Int. J. Environ. Res. Public Health 2020, 17, 5118. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145118
Sion K, Verbeek H, de Vries E, Zwakhalen S, Odekerken-Schröder G, Schols J, Hamers J. The Feasibility of Connecting Conversations: A Narrative Method to Assess Experienced Quality of Care in Nursing Homes from the Resident’s Perspective. International Journal of Environmental Research and Public Health. 2020; 17(14):5118. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145118
Chicago/Turabian StyleSion, Katya, Hilde Verbeek, Erica de Vries, Sandra Zwakhalen, Gaby Odekerken-Schröder, Jos Schols, and Jan Hamers. 2020. "The Feasibility of Connecting Conversations: A Narrative Method to Assess Experienced Quality of Care in Nursing Homes from the Resident’s Perspective" International Journal of Environmental Research and Public Health 17, no. 14: 5118. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145118