The Association between Race and Survival among Pediatric Patients with Neuroblastoma in the US between 1973 and 2015

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Main Variables
2.3. Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cunningham, R.M.; Walton, M.A.; Carter, P.M. The major causes of death in children and adolescents in the united states. N. Engl. J. Med. 2018, 379, 2468–2475. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.; DeSantis, C.; Robbins, A.; Kohler, B.; Jemal, A. Childhood and adolescent cancer statistics. CA Cancer J. Clin. 2014, 64, 83–103. [Google Scholar] [CrossRef] [PubMed]
- Moroz, V.; Machin, D.; Faldum, A.; Hero, B.; Iehara, T.; Mosseri, V.; Ladenstein, R.; De Bernardi, B.; Rubie, H.; Berthold, F.; et al. Changes over three decades in outcome and the prognostic influence of age-at-diagnosis in young patients with neuroblastoma: A report from the International Neuroblastoma Risk Group Project. Eur. J. Cancer 2011, 47, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, S. Disparities in cancer outcomes: Lessons learned from children with cancer. Pediatr. Blood Cancer 2011, 56, 994–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pizzo, P.A.; Poplack, D.G. Principles and Practice of Pediatric Oncology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2015. [Google Scholar]
- Friedrich, P.; Itriago, E.; Rodriguez-Galindo, C.; Ribeiro, K. Racial and Ethnic Disparities in the Incidence of Pediatric Extracranial Embryonal Tumors. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [PubMed]
- Lanier, A.P.; Holck, P.; Ehrsam Day, G.; Key, C. Childhood cancer among Alaska natives. Pediatrics 2003, 112, e396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henderson, T.O.; Bhatia, S.; Pinto, N.; London, W.B.; McGrady, P.; Crotty, C.; Sun, C.L.; Cohn, S.L. Racial and ethnic disparities in risk and survival in children with neuroblastoma: A children’s oncology group study. J. Clin. Oncol. 2011, 29, 76–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linabery, A.M.; Ross, J.A. Childhood and adolescent cancer survival in the US by race and ethnicity for the diagnostic period 1975–1999. Cancer 2008, 113, 2575–2596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, K.A.; Aplenc, R.; Bagatell, R. Survival by race among children with extracranial solid tumors in the united states between 1985 and 2005. Pediatr. Blood Cancer 2011, 56, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Pui, C.H.; Pei, D.; Pappo, A.S.; Howard, S.C.; Cheng, C.; Sandlund, J.T.; Furman, W.L.; Ribeiro, R.C.; Spunt, S.L.; Rubnitz, J.E.; et al. Treatment outcomes in black and white children with cancer: Results from the SEER database and St Jude children’s research hospital, 1992 through 2007. J. Clin. Oncol. 2012, 30, 2005–2012. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Meng, Y. A prognostic nomogram for neuroblastoma in children. PeerJ 2019, 11, e7316. [Google Scholar] [CrossRef] [PubMed]
- Gamazon, E.R.; Pinto, N.; Konkashbaev, A.; Im, H.K.; Diskin, S.J.; London, W.B.; Maris, J.M.; Dolan, M.E.; Cox, N.J.; Cohn, S.L. Trans-population analysis of genetic mechanisms of ethnic disparities in neuroblastoma survival. J. Natl. Cancer Inst. 2013, 105, 302–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiNicola, W.; Movassaghi, N.; Leikin, S. Prognosis in Black children with neuroblastoma. Cancer 1975, 36, 1151–1153. [Google Scholar] [CrossRef]
- National Institutes of Health. SEER Program Overview. 2018. Available online: https://seer.cancer.gov/about/factsheets/SEER_Overview.pdf (accessed on 22 January 2019).
- Pinto, N.R.; Applebaum, M.A.; Volchenboum, S.L.; Matthay, K.K.; London, W.B.; Ambros, P.F.; Nakagawara, A.; Berthold, F.; Schleiermacher, G.; Park, J.R.; et al. Advances in risk classification and treatment strategies for neuroblastoma. J. Clin. Oncol. 2015, 33, 3008–3017. [Google Scholar] [CrossRef] [PubMed]
- Stata Corp, LP. Stata Statistical Software: Release 15; StataCorp LP: College Station, TX, USA, 2017. [Google Scholar]
- Kehm, R.D.; Spector, L.G.; Poynter, J.N.; Vock, D.M.; Altekruse, S.F.; Osypuk, T.L. Does socioeconomic status account for racial and ethnic disparities in childhood cancer survival? Cancer 2018, 124, 4090–4097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coldman, A.J.; Fryer, C.; Elwood, J.M.; Sonley, M.J. Neuroblastoma: Influence of age at diagnosis, stage, tumor site, and sex on prognosis. Cancer 1980, 46, 1896–1901. [Google Scholar] [CrossRef]
- Vo, K.T.; Matthay, K.K.; Neuhaus, J.; London, W.B.; Hero, B.; Ambros, P.F.; Nakagawara, A.; Miniati, D.; Wheeler, K.; Pearson, A.D.; et al. Clinical, biologic, and prognostic differences on the basis of primary tumor site in neuroblastoma: A report from the international neuroblastoma risk group project. J. Clin. Oncol. 2014, 32, 3169. [Google Scholar] [CrossRef] [PubMed]
- Duggan, M.A.; Anderson, W.F.; Altekruse, S.; Penberthy, L.; Sherman, M.E. The surveillance, epidemiology and end results (SEER) program and pathology: Towards strengthening the critical relationship. Am. J. Surg. Pathol. 2016, 40, e94. [Google Scholar] [CrossRef] [PubMed]
- London, W.B.; Castleberry, R.P.; Matthay, K.K.; Look, A.T.; Seeger, B.; Shimada, H.; Thorner, P.; Brodeur, G.; Maris, J.M.; Reynolds, C.P.; et al. Evidence for an age cut-off greater than 365 days for neuroblastoma risk group stratification in the Children’s Oncology Group. J. Clin. Oncol. 2005, 23, 6459–6465. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | White (n = 1680) | Black (n = 274) | API a (n = 165) | p-Value | |||
|---|---|---|---|---|---|---|---|
| % (n) | % (n) | % (n) | (n) | ||||
| Age (years) | 0.001 | ||||||
| <1 | 43.1 | −724 | 29.6 | −81 | 43.6 | −72 | |
| 1–4 | 46.5 | −781 | 55.8 | −153 | 45.5 | −75 | |
| 5–17 | 10.4 | −175 | 14.6 | −40 | 10.9 | −18 | |
| Gender | 0.661 | ||||||
| Male | 54.6 | −917 | 52.6 | −144 | 57 | −94 | |
| Female | 45.4 | −763 | 47.5 | −130 | 43 | −71 | |
| Ethnicity | <0.001 | ||||||
| Hispanic | 11.3 | −190 | 2.55 | −7 | 4.2 | −7 | |
| Non-Hispanic | 89 | −1490 | 97.5 | −267 | 95.8 | −158 | |
| Stage | 0.415 | ||||||
| Localized | 10.7 | −180 | 9.5 | −26 | 10.3 | −17 | |
| Regional | 18.3 | −308 | 17.2 | −47 | 14 | −23 | |
| Distant | 40.6 | −682 | 37.2 | −102 | 44.9 | −74 | |
| Unstaged/Unknown | 30.4 | −510 | 36 | −99 | 31 | −51 | |
| Site | 0.004 | ||||||
| Adrenal | 40.6 | −682 | 40.5 | −111 | 53.9 | −89 | |
| Non-Adrenal | 59.4 | −998 | 59.5 | −163 | 46.1 | −76 | |
| Year | 0.001 | ||||||
| 1973–1999 | 59.5 | −999 | 52.6 | −144 | 46.7 | −77 | |
| 2000–2004 | 13.3 | −223 | 12.8 | −35 | 12.7 | −21 | |
| 2005–2015 | 27.3 | −458 | 34.7 | −95 | 40.6 | −67 | |
| Characteristics | Unadjusted | Adjusted |
|---|---|---|
| HR a (95% CI b) | HR (95% CI) | |
| Race | ||
| White | Ref.c | Ref. |
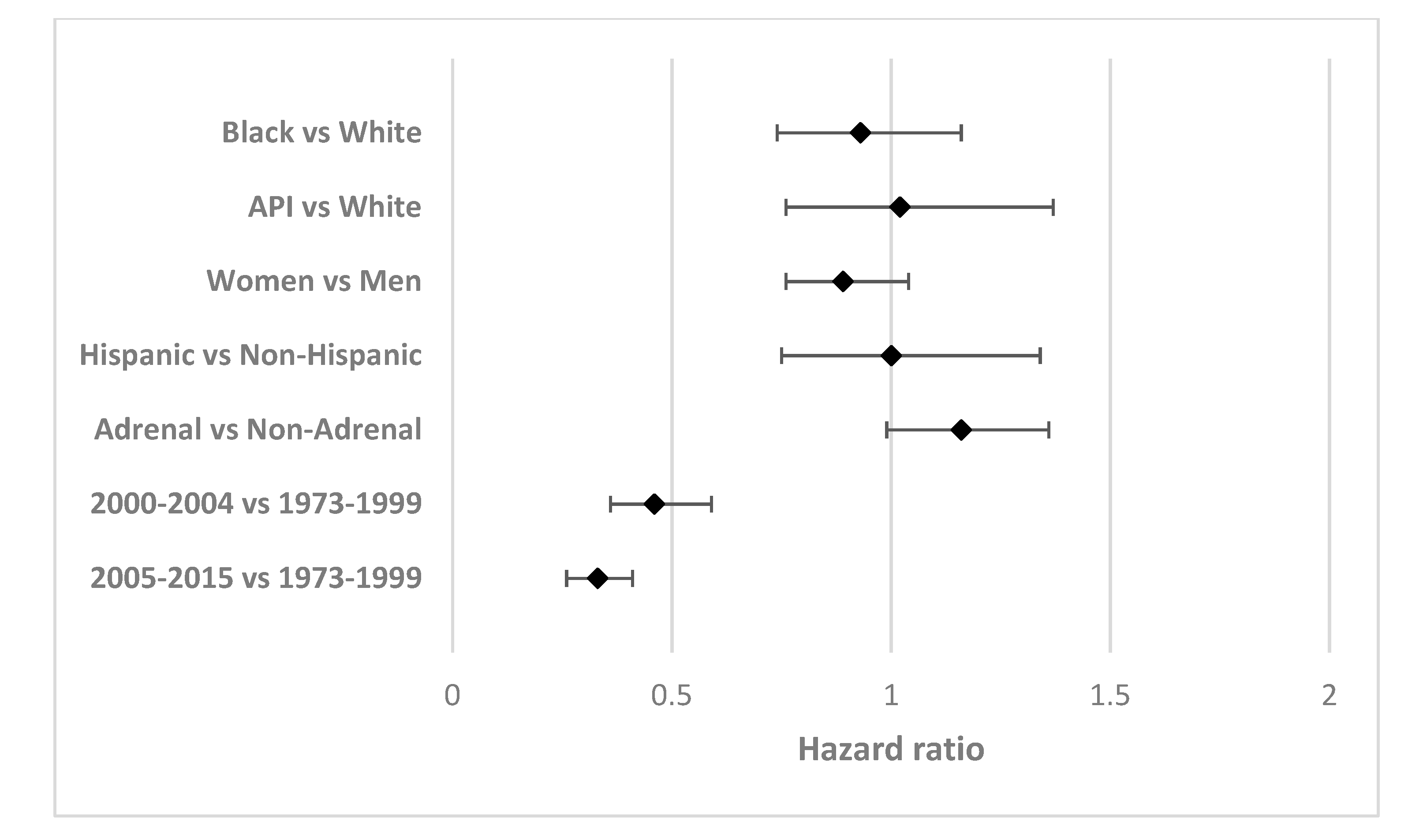
| Black | 1.04 (0.83–1.30) | 0.93 (0.74–1.16) |
| API d | 1.02 (0.76–1.35) | 1.02 (0.76–1.37) |
| Age | ||
| <1 years | Ref. | Ref. |
| 1–4 years | 6.65 (5.22–8.47) | 5.92 (4.64–7.56) |
| 5–17 years | 8.57 (6.49–11.31) | 7.29 (5.51–9.66) |
| Sex | ||
| Male | Ref. | Ref. |
| Female | 0.86 (0.74–1.00) | 0.89 (0.76–1.04) |
| Ethnicity | ||
| Non-Hispanic | Ref. | Ref. |
| Hispanic | 0.77 (0.58–1.02) | 1.00 (0.75–1.34) |
| Stage | ||
| Localized | Ref. | Ref. |
| Regional | 3.63 (1.91–6.88) | 3.06 (1.61–5.80) |
| Distant | 13.45 (7.39–24.50) | 9.03 (4.94–16.49) |
| Unstaged/Unknown | 7.78 (4.24–14.29) | 7.32 (3.97–13.51) |
| Site | ||
| Non-Adrenal | Ref. | Ref. |
| Adrenal | 1.37 (1.18–1.59) | 1.16 (0.99–1.36) |
| Year | ||
| 1973–1999 | Ref. | Ref. |
| 2000–2004 | 0.51 (0.40–0.65) | 0.46 (0.36–0.59) |
| 2005–2015 | 0.39 (0.31–0.48) | 0.33 (0.26–0.41) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farouk, F.S.; Viqar, O.A.; Sheikh, Z.; Castro, G.; Barengo, N.C. The Association between Race and Survival among Pediatric Patients with Neuroblastoma in the US between 1973 and 2015. Int. J. Environ. Res. Public Health 2020, 17, 5119. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145119
Farouk FS, Viqar OA, Sheikh Z, Castro G, Barengo NC. The Association between Race and Survival among Pediatric Patients with Neuroblastoma in the US between 1973 and 2015. International Journal of Environmental Research and Public Health. 2020; 17(14):5119. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145119
Chicago/Turabian StyleFarouk, Farouk S., Omar A. Viqar, Zaid Sheikh, Grettel Castro, and Noël C. Barengo. 2020. "The Association between Race and Survival among Pediatric Patients with Neuroblastoma in the US between 1973 and 2015" International Journal of Environmental Research and Public Health 17, no. 14: 5119. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145119