Cost-Effectiveness of a Problem-Solving Intervention Aimed to Prevent Sickness Absence among Employees with Common Mental Disorders or Occupational Stress

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
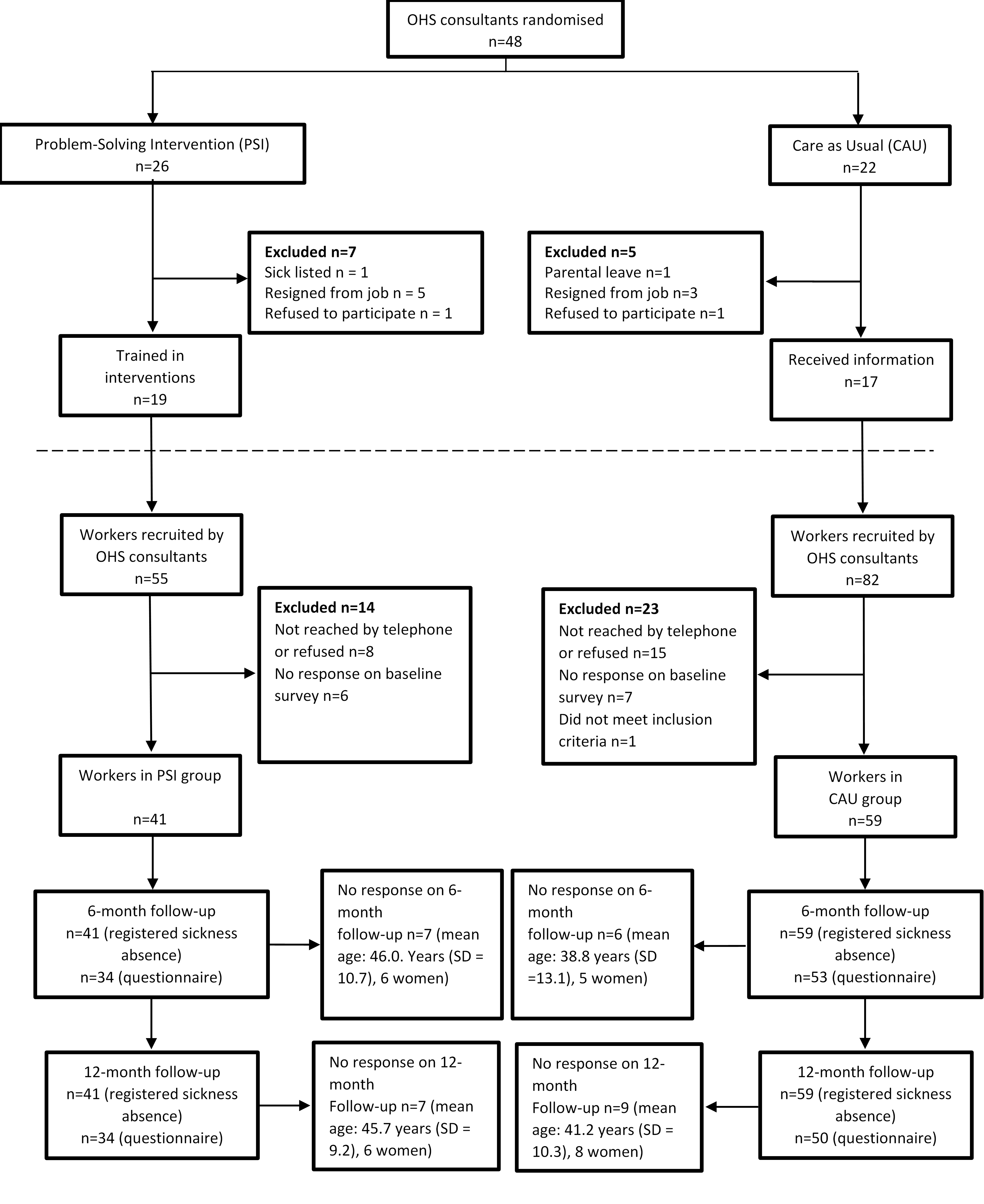
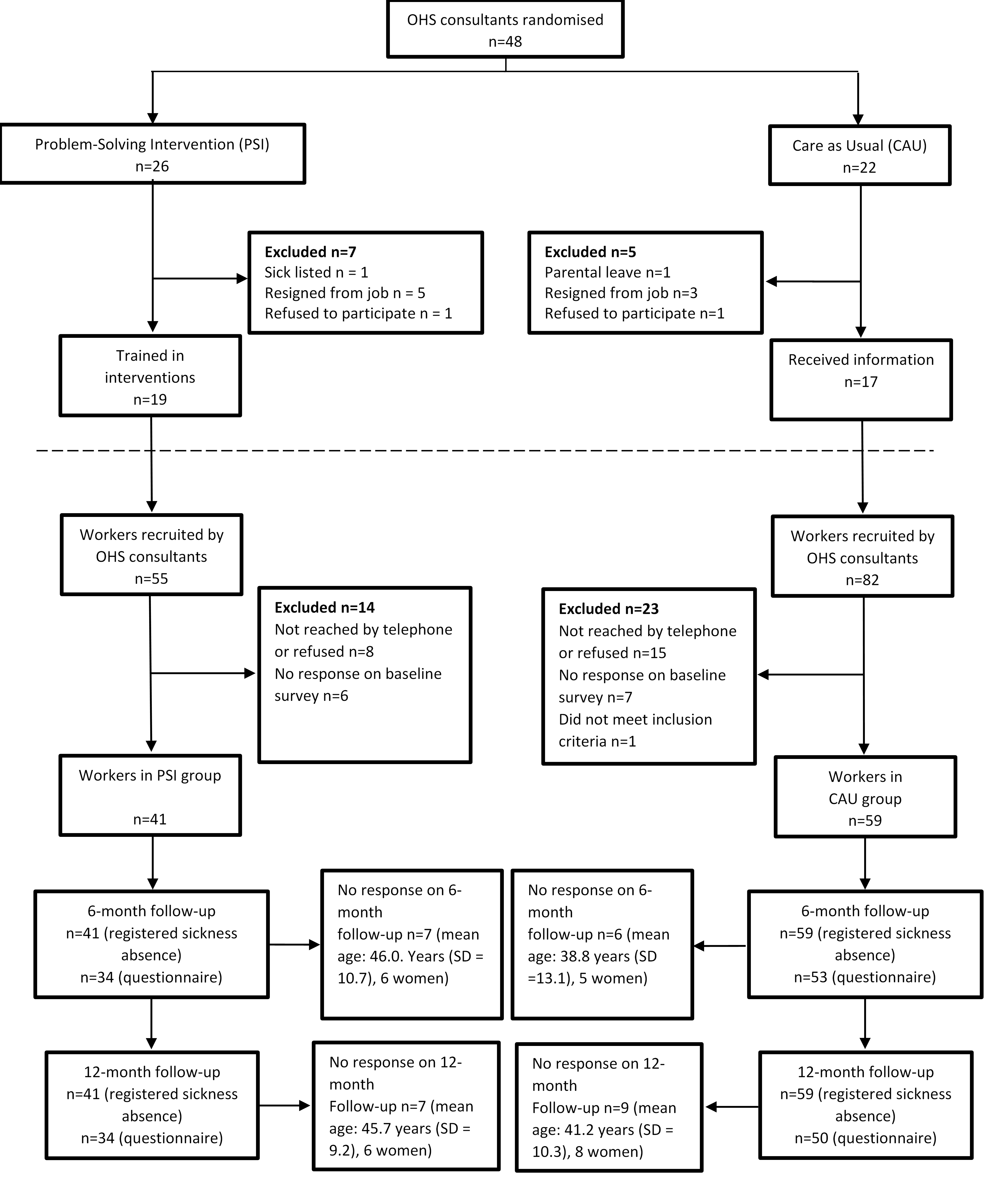
2.1. Study Design and Setting
2.2. Problem-Solving Intervention (PSI)
2.3. Care as Usual
2.4. Data Collection
2.5. Economic Evaluation
2.6. Intervention Cost
2.7. Production Loss
2.8. Data Analysis
2.8.1. Employer Perspective
2.8.2. Societal Perspective
2.8.3. Sensitivity Analysis
3. Results
3.1. Costs for PSI and CAU
3.2. Production Loss
3.3. Cost-Benefit and Cost-Effectiveness Analyses—Employer Perspective
3.4. Sensitivity Analyses
4. Discussion
Methodological Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- OECD/EU. Health at a Glance: Europe 2018: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2018; pp. 1–212. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, K.; Faber, B.; Verbeek, J.H.; Neumeyer-Gromen, A.; Hees, H.L.; Verhoeven, A.C.; van der Feltz-Cornelis, C.M.; Bültmann, U. Interventions to improve return to work in depressed people. Cochrane Database Syst. Rev. 2014, 12, 1–109. [Google Scholar] [CrossRef] [PubMed]
- Volker, D.; Zijlstra-Vlasveld, M.C.; Anema, J.R.; Beekman, A.T.; Brouwers, E.P.; Emons, W.H.; van Lomwel, A.G.C.; van der Feltz-Cornelis, C.M. Effectiveness of a Blended Web-Based Intervention on Return to Work for Sick-Listed Employees With Common Mental Disorders: Results of a Cluster Randomized Controlled Trial. J. Med. Internet Res. 2015, 17, e116. [Google Scholar] [CrossRef] [PubMed]
- Van der Klink, J.J.; Blonk, R.W.; Schene, A.H.; van Dijk, F.J.H. Reducing long term sickness absence by an activating intervention in adjustment disorders: A cluster randomised controlled design. Occup. Environ. Med. 2003, 60, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Arends, I.; Bruinvels, D.J.; Rebergen, D.S.; Nieuwenhuijsen, K.; Madan, I.; Neumeyer-Gromen, A.; Bültmann, U.; Verbeek, J.H. Interventions to facilitate return to work in adults with adjustment disorders. Cochrane Database Syst. Rev. 2012, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Axén, I.; Björk Brämberg, E.; Vaez, M.; Lundin, A.; Bergström, G. Interventions for common mental disorders in the occupational health service: A systematic review with a narrative synthesis. Int. Arch. Occup. Environ. Health 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cullen, K.L.; Irvin, E.; Collie, A.; Clay, F.; Gensby, U.; Jennings, P.A.; Hogg-Johnson, S.; Kristman, V.; Laberge, M.; McKenzie, D.; et al. Effectiveness of workplace interventions in return-to-work for musculoskeletal, pain-related and mental health conditions: An update of the evidence and messages for practitioners. J. Occup. Rehabil. 2018, 28, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keus van de Poll, M.; Nybergh, L.; Lornudd, C.; Hagberg, J.; Bodin, L.; Kwak, L.; Jensen, I.; Lohela-Karlsson, M.; Torgén, M.; Bergström, G. Preventing sickness absence among employees with common mental disorders or stress-related symptoms at work: A cluster randomised controlled trial of a problem-solving-based intervention conducted by the Occupational Health Services. Occup. Environ. Med. 2020, 77, 454–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlson, B.; Jönsson, P.; Pålsson, B.; Åbjörnsson, G.; Malmberg, B.; Larsson, B.; Österberg, K. Return to work after a workplace-oriented intervention for patients on sick-leave for burnout-a prospective controlled study. BMC Public Health 2010, 10, 301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Oostrom, S.H.; van Mechelen, W.; Terluin, B.; de Vet, H.C.W.; Anema, J.R. A participatory workplace intervention for employees with distress and lost time: A feasibility evaluation within a randomized controlled trial. J. Occup. Rehabil. 2009, 19, 212–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes, 4th ed.; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Van Dongen, J.M.; van Wier, M.F.; Tompa, E.; Bongers, P.M.; van der Beek, A.J.; van Tulder, M.W.; Bosmans, J.E. Trial-based economic evaluations in occupational health: Principles, methods, and recommendations. J. Occup. Environ. Med. 2014, 56, 563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tompa, E.; Verbeek, J.; van Tulder, M.; de Boer, A. Developing guidelines for good practice in the economic evaluation of occupational safety and health interventions. Scand. J. Work Environ. Health 2010, 36, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Hamberg-van Reenen, H.H.; Proper, K.I.; van den Berg, M. Worksite mental health interventions: A systematic review of economic evaluations. Occup. Environ. Med. 2012, 69, 837–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Björk Brämberg, E.; Nyman, T.; Kwak, L.; Alipour, A.; Bergström, G.; Schäfer Elinder, L.; Hermansson, U.; Jensen, I. Development of evidence-based practice in occupational health services in Sweden. A 3-year follow-up of attitudes, barriers and facilitators. Int. Arch. Occup. Environ. Health 2017, 90, 335–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergström, G.; Lohela-Karlsson, M.; Kwak, L.; Bodin, L.; Jensen, I.; Torgén, M.; Nybergh, L. Preventing sickness absenteeism among employees with common mental disorders or stress-related symptoms at work: Design of a cluster randomized controlled trial of a problem-solving based intervention versus care-as-usual conducted at the Occupational Health Services. BMC Public Health 2017, 17, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Nezu, A.M.; Nezu, C.M.; D’Zurilla, T. Problem-Solving Therapy: A Treatment Manual; Springer Publishing Company: New York, NY, USA, 2012. [Google Scholar]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aboagye, E.; Karlsson, M.L.; Hagberg, J.; Jensen, I. Cost-effectiveness of early interventions for non-specific low back pain: A randomized controlled study investigating medical yoga, exercise therapy and self-care advice. J. Rehabil. Med. 2015, 47, 167–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohela-Karlsson, M.; Bergström, G.; Björklund, C.; Hagberg, J.; Jensen, I. Measuring production loss due to health and work environment problems: Construct validity and implications. J. Occup. Environ. Med. 2013, 55, 1475–1483. [Google Scholar] [CrossRef] [PubMed]
- SCB. Genomsnittlig Månadslön Efter Sektor (Mean Monthly Wages per Sector). Available online: https://www.scb.se/hitta-statistik/statistik-efter-amne/arbetsmarknad/loner-och-arbetskostnader/lonestrukturstatistik-hela-ekonomin/pong/tabell-och-diagram/genomsnittlig-manadslon-efter-sektor/ (accessed on 18 February 2020).
- Sveriges Riksbank. Månadsgenomsnitt Valutakurser (Mean Exchange Rate per Month). Available online: https://www.riksbank.se/sv/statistik/sok-rantor--valutakurser/manadsgenomsnitt-valutakurser/?y=2015&m=12&s=Comma&f=m (accessed on 16 March 2020).
- Skatteverket. Arbetsgivaravgifter (General Payroll Tax). Available online: https://www.skatteverket.se/foretagochorganisationer/arbetsgivare/arbetsgivaravgifterochskatteavdrag/arbetsgivaravgifter.4.233f91f71260075abe8800020817.html (accessed on 18 February 2020).
- Försäkringskassan. Social Insurance in Figures, Stockholm. 2019. Available online: https://www.forsakringskassan.se/wps/wcm/connect/cec4cea8-1d6c-4895-b442-bc3b64735b09/socialforsakringen-i-siffror-2019-engelsk.pdf?MOD=AJPERES&CVID= (accessed on 4 June 2020).
- SCB. Konsumentprisindex (Consumer Price Index). Available online: https://www.scb.se/hitta-statistik/statistik-efter-amne/priser-och-konsumtion/konsumentprisindex/konsumentprisindex-kpi/pong/tabell-och-diagram/konsumentprisindex-kpi/kpi-faststallda-tal-1980100/ (accessed on 18 February 2020).
- Ekberg, K.; Bernfort, L.; Persson, J. 472 Employer accommodations and productivity loss for long-term sick-listed workers before, during and after sick-leave. Occup. Environ. Med. 2018, 75, A548. [Google Scholar] [CrossRef] [Green Version]
- Lötters, F.; Meerding, W.J.; Burdorf, A. Reduced productivity after sickness absence due to musculoskeletal disorders and its relation to health outcomes. Scand. J. Work Environ. Health 2005, 31, 367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UWV. Werknemer en Loondoorbetaling (Employee and Continued Payment of Wages). Available online: https://www.uwv.nl/werkgevers/werknemer-is-ziek/loondoorbetaling/werknemer-is-ziek-loon-doorbetalen/detail/loon-doorbetalen-tijdens-ziekte/loon-doorbetalen-in-het-tweede-ziektejaar (accessed on 20 May 2020).

{kind=link}
| Sociodemographic Characteristics | PSI (n = 41) | CAU (n = 59) | |||
|---|---|---|---|---|---|
| Age, years, m (sd) | 42.7 | (10.4) | 44.0 | (9.6) | |
| Female, n (%) | 37 | (90) | 43 | (73) | |
| Children, n (%) | 23 | (56) | 39 | (66) | |
| Education level, n (%) | |||||
| Prim./sec. education | 14 | (34) | 20 | (34) | |
| Higher education/university | 27 | (66) | 39 | (66) | |
| Ordinary working hours | |||||
| Full time (40 h/week) | 31 | (76) | 52 | (88) | |
| Part time (< 40 h/week) | 10 | (24) | 7 | (12) | |
| Employer, n (%) | |||||
| Municipality, county, state 1 | 38 | (93) | 39 | (66) | |
| Private business | 3 | (7) | 20 | (34) | |
| Profession, n (%) | |||||
| Teacher | 9 | (22) | 2 | (3) | |
| manager | 2 | (5) | 8 | (14) | |
| Assistant nurse | 4 | (10) | 5 | (8) | |
| nurse | 3 | (7) | 6 | (10) | |
| IT-architect/system development/test leader | 1 | (2) | 4 | (7) | |
| Administrative (executive) official | 2 | (5) | 2 | (3) | |
| Caretaker/personal assistant | 2 | (5) | 2 | (3) | |
| Client support | 0 | (0) | 4 | (7) | |
| Other 2 | 18 | (44) | 26 | (45) | |
| Registered sickness absence, n (%) | |||||
| No sickness absence | 20 | (49) | 31 | (53) | |
| Sickness absence | 21 | (51) | 28 | (47) | |
| % Production loss due to ill health | 62 | (28) | 65 | (24) | |
| PSI n = 26 | CAU n = 22 | |
|---|---|---|
| Female | 21 (80.8) | 19 (86.4) |
| Male | 5 (19.2) | 3 (13.6) |
| Nurses and ergonomists | 16 (61.5) | 17 (77.3) |
| Behavioral scientists and psychologists | 8 (30.8) | 4 (18.2) |
| Physician | 2 (7.7) | 1 (4.5) |
| Attending the Meeting | Duration in Minutes (Approx.) | Location | ||
|---|---|---|---|---|
| PSI | ||||
| Step 1 | OHS consultant and manager | 30 | phone | |
| Step 2 | OHS consultant and employee | 90 | OHS | |
| Step 3 | OHS consultant, employee and employer | 60 | OHS | |
| CAU | ||||
| Units 1 and 2 | ||||
| Step 1 | OHS consultant and manager | 30 | Phone | |
| Step 2 | OHS consultant and employee | 120 * | OHS | |
| Step 3 | OHS consultant, employee and manager | 60 * | OHS | |
| Unit 3 | ||||
| Step 1 | OHS consultant, employee and manager | 60 | OHS | |
| Step 2 | OHS consultant and employee | 120–210 ** | OHS | |
| Unit 4 | ||||
| Step 1 | OHS consultant and manager | 30 | phone | |
| Step 2 | OHS consultant, manager and employee | 90 | OHS | |
| PSI | 95% CI | CAU | 95% CI | |||
|---|---|---|---|---|---|---|
| Component | Lower; Upper | Lower; Upper | ||||
| Employer’s perspective | ||||||
| Intervention Costs | ||||||
| Intervention | 405 | 393; 418 | 445 | 426; 463 | ||
| Travel time | 62 | 52; 72 | 64 | 54; 75 | ||
| Total | 467 | 445; 489 | 509 | 481; 537 | ||
| Sickness absence Costs | ||||||
| Long-term sickness absence 1 | 1358 | 878; 1838 | 1647 | 1218; 2077 | ||
| Short-term sickness absence 2 | 1876 | 1246; 2506 | 1310 | 797; 1823 | ||
| Total | 3234 | 2498; 3970 | 2957 | 2306; 3609 | ||
| Presenteeism costs | ||||||
| Production loss due to ill health | 16,101 | 13,577; 18,625 | 13,942 | 11,576; 16,308 | ||
| Total cost for production loss 3 | 19,335 | 16,920; 21,750 | 16,900 | 14,391; 19,408 | ||
| Societal perspective | ||||||
| Intervention Costs | ||||||
| Intervention | 446 | 446; 447 | 494 | 477; 511 | ||
| Travel time | 95 | 95; 95 | 101 | 94; 107 | ||
| Total | 541 | 541; 542 | 594 | 572; 617 | ||
| Sickness absence costs | ||||||
| Long-term sickness absence 4 | 16,409 | 9372; 23,445 | 24,622 | 17,160; 32,084 | ||
| Short-term sickness absence 2 | 2280 | 1514; 3045 | 1592 | 968; 2216 | ||
| Total | 18,688 | 11,712; 25,665 | 26,214 | 18,874; 33,554 | ||
| Presenteeism costs | ||||||
| Production loss due to ill health | 16,101 | 13,577; 18,625 | 13,942 | 11,576; 16,308 | ||
| Total cost for production loss 3 | 34,789 | 27,551; 42,027 | 40,156 | 33,205; 47,107 | ||
| C * | E * | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| CAU | PSI | CAU | PSI | ΔC | ΔE | ICER | NMB | ||
| CBA | employer | 508 | 467 | 16,892 | 19,342 | 41 | −2450 | −2409 | |
| society | 594 | 541 | 40,178 | 34,701 | 53 | 5477 | 5530 | ||
| CEA | employer | 15,780 | 18,430 | 93 | 65 | −2650 | 28 | −95 | |
| society | 16,109 | 18,930 | 93 | 65 | −2821 | 28 | −101 | ||
| C | E | ΔC | ΔE | ICER | NMB | ||||
|---|---|---|---|---|---|---|---|---|---|
| CAU | PSI | CAU | PSI | ||||||
| Sens.analysis 1 1 | |||||||||
| CBA | employer | 509 | 467 | 2957 | 3225 | 42 | −268 | −226 | |
| society | 595 | 541 | 26,306 | 18,712 | 54 | 7594 | 7648 | ||
| CEA | employer | 1820 | 2348 | 93 | 65 | −528 | 28 | −19 | |
| society | 2189 | 2824 | 93 | 65 | −635 | 28 | −23 | ||
| Sens.analysis 2 2 | |||||||||
| CBA | employer | 509 | 467 | 1647 | 1358 | 42 | 289 | 331 | |
| society | 594 | 541 | 24,605 | 16,358 | 53 | 8247 | 8300 | ||
| CEA | employer | 509 | 467 | 93 | 65 | 42 | 28 | 1.5 | |
| society | 594 | 541 | 93 | 65 | 53 | 28 | 1.9 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keus Van De Poll, M.; Bergström, G.; Jensen, I.; Nybergh, L.; Kwak, L.; Lornudd, C.; Lohela-Karlsson, M. Cost-Effectiveness of a Problem-Solving Intervention Aimed to Prevent Sickness Absence among Employees with Common Mental Disorders or Occupational Stress. Int. J. Environ. Res. Public Health 2020, 17, 5234. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145234
Keus Van De Poll M, Bergström G, Jensen I, Nybergh L, Kwak L, Lornudd C, Lohela-Karlsson M. Cost-Effectiveness of a Problem-Solving Intervention Aimed to Prevent Sickness Absence among Employees with Common Mental Disorders or Occupational Stress. International Journal of Environmental Research and Public Health. 2020; 17(14):5234. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145234
Chicago/Turabian StyleKeus Van De Poll, Marijke, Gunnar Bergström, Irene Jensen, Lotta Nybergh, Lydia Kwak, Caroline Lornudd, and Malin Lohela-Karlsson. 2020. "Cost-Effectiveness of a Problem-Solving Intervention Aimed to Prevent Sickness Absence among Employees with Common Mental Disorders or Occupational Stress" International Journal of Environmental Research and Public Health 17, no. 14: 5234. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145234