Driving Accidents, Driving Violations, Symptoms of Attention-Deficit-Hyperactivity (ADHD) and Attentional Network Tasks

 ,
, 
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Tools
2.3.1. Demographic Information
2.3.2. Driving-Related Information
2.3.3. Dimensions of Attention-Deficit/Hyperactivity Disorder (ADHD)
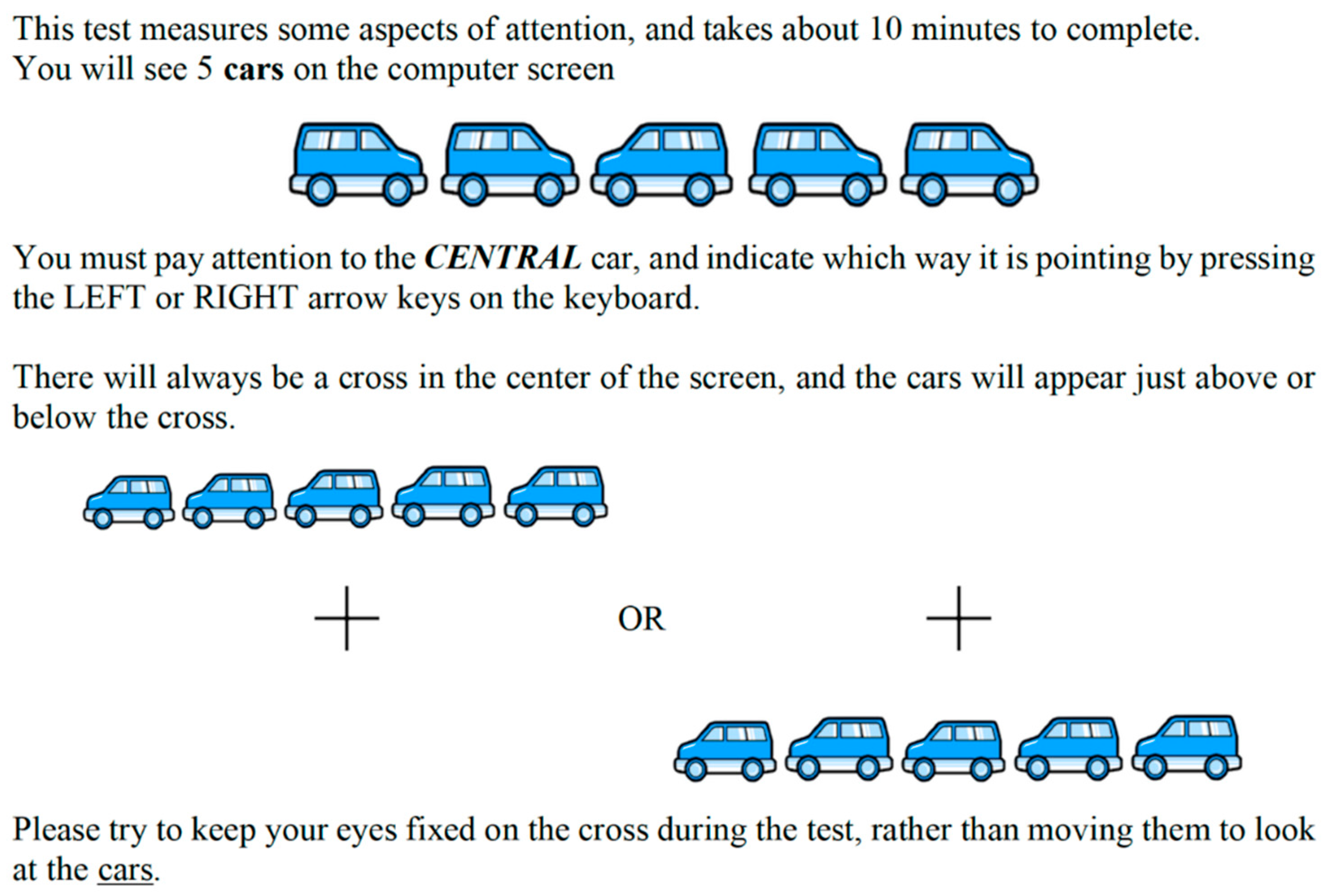
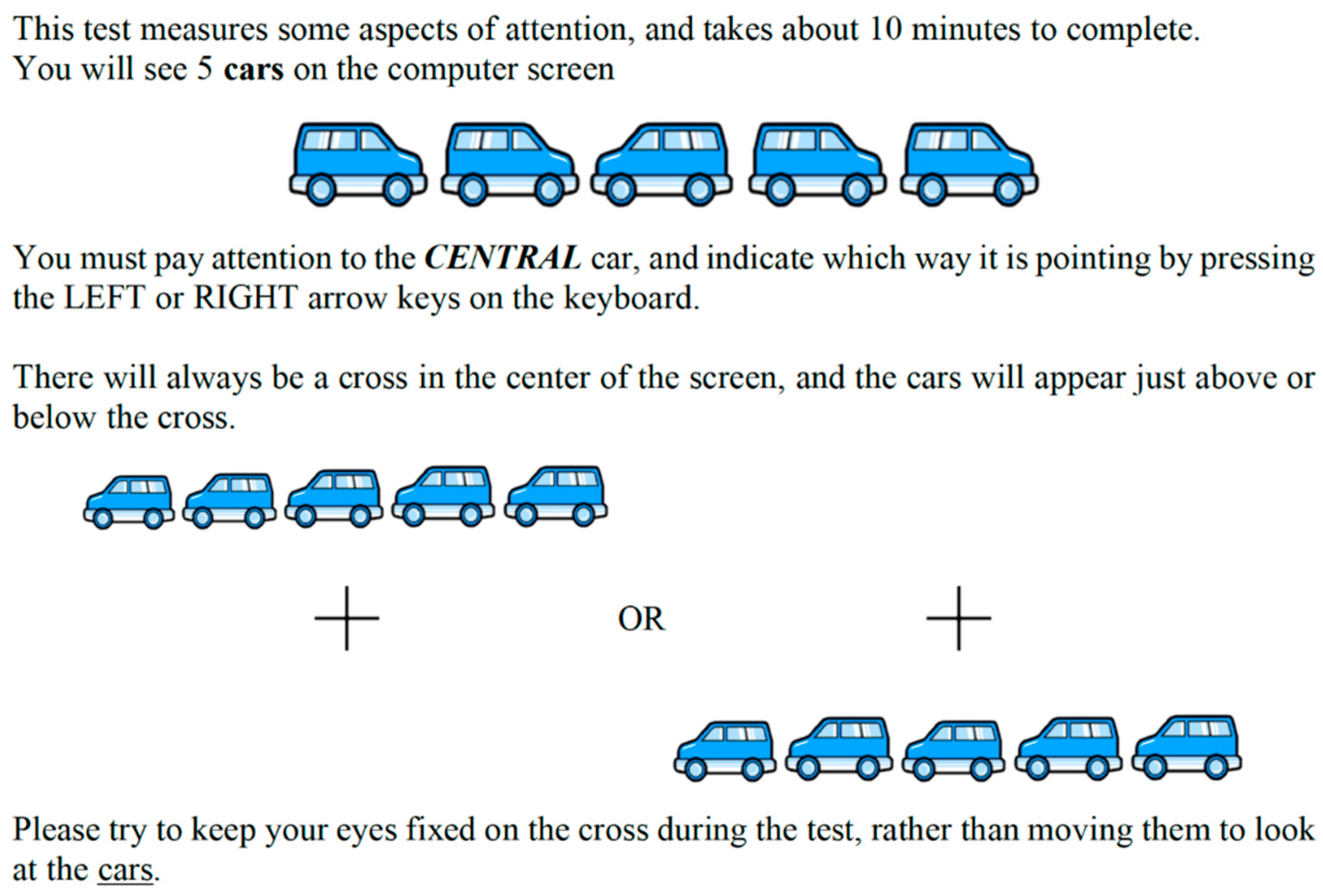
2.3.4. Attention and Perception
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Traffic Accidents, Traffic Violations, Driving Frequency, Driving Experience, and Objective Processing Speed of Attentional Network Tasks
3.3. Symptoms of ADHD and Driving Behavior
3.4. Age and Objectively Assessed Functioning of Attentional Network Tasks
3.5. Self-Reported Symptoms of ADHD and Objective Performance of Attentional Network Tasks
3.6. Age, Self-Reported Symptoms of ADHD, Driving Experience and Driving Frequency, and Objective Performance of Attentional Network Tasks as Predictors of Self-reported Traffic Violations and Traffic Accidents
3.7. Additional Computations; Demographic Information, Driving Behavior, and Cognitive Performance between Traffic Offenders and Traffic Non-Offenders
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Abdoli, N.; Farnia, V.; Delavar, A.; Dortaj, F.; Esmaeili, A.; Farrokhi, N.; Karami, M.; Shakeri, J.; Holsboer-Trachsler, E.; Brand, S. Mental health status, aggression, and poor driving distinguish traffic offenders from non-offenders but health status predicts driving behavior in both groups. Neuropsychiatr. Dis. Treat. 2015, 11, 2063–2070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moradi, S. An epidemiologic survey of pedestrians passed away in traffic accident. J. Leg. Med. 2003, 9, 75–81. [Google Scholar]
- Moradi, S.K.H. Survey of victims of car accidents year 1387. J. Forensic Med. 2009, 15, 21–28. [Google Scholar]
- World Health Organization, W.H.O. Global Status Report on Road Safety 2013: Supporting a Decade of Action; World Health Organization: Geneva, Switzerland, 2013.
- Montazeri, A. Road-traffic-related mortality in Iran: A descriptive study. Public Health 2004, 118, 110–113. [Google Scholar] [CrossRef]
- Zangooei Dovom, H.; Shafahi, Y.; Zangooei Dovom, M. Fatal accident distribution by age, gender and head injury, and death probability at accident scene in Mashhad, Iran, 2006–2009. Int. J. Inj. Control. Saf. Promot. 2013, 20, 121–133. [Google Scholar] [CrossRef]
- Mohajerani, S.H.; Asghari, S. Pattern of mid-facial fractures in Tehran, Iran. Dent. Traumatol. 2011, 27, 131–134. [Google Scholar] [CrossRef]
- Motamedi, M.H.; Dadgar, E.; Ebrahimi, A.; Shirani, G.; Haghighat, A.; Jamalpour, M.R. Pattern of maxillofacial fractures: A 5-year analysis of 8,818 patients. J. Trauma Acute Care Surg. 2014, 77, 630–634. [Google Scholar] [CrossRef]
- Zargar, M.; Khaji, A.; Karbakhsh, M.; Zarei, M.R. Epidemiology study of facial injuries during a 13 month of trauma registry in Tehran. Indian J. Med. Sci. 2004, 58, 109–114. [Google Scholar]
- Abdoli, N.; Bahmani, D.S.; Farnia, V.; Alikhani, M.; Golshani, S.; Holsboer-Trachsler, E.; Brand, S. Among substance-abusing traffic offenders, poor sleep and poor general health predict lower driving skills but not slower reaction times. Psychol. Res. Behav. Manag. 2018, 11, 557–566. [Google Scholar] [CrossRef] [Green Version]
- Reason, J.; Manstead, A.; Stradling, S.; Baxter, J.; Campbell, K. Errors and violations on the roads: A real distinction? Ergonomics 1990, 33, 1315–1332. [Google Scholar] [CrossRef] [PubMed]
- Hole, G.J. The Psychology of Driving; Psychology Press: New York, NY, USA, 2014. [Google Scholar]
- López-Ramón, M.F.; Castro, C.; Roca, J.; Ledesma, R.; Lupiañez, J. Attentional networks functioning, age, and attentional lapses while driving. Traffic Inj. Prev. 2011, 12, 518–528. [Google Scholar] [CrossRef]
- Fan, J.; McCandliss, B.D.; Sommer, T.; Raz, A.; Posner, M.I. Testing the efficiency and independence of attentional networks. J. Cogn. Neurosci. 2002, 14, 340–347. [Google Scholar] [CrossRef]
- Petersen, S.E.; Posner, M.I. The attention system of the human brain: 20 years after. Annu. Rev. Neurosci. 2012, 35, 73–89. [Google Scholar] [CrossRef] [Green Version]
- Posner, M.I.; Petersen, S.E. The attention system of the human brain. Annu. Rev. Neurosci. 1990, 13, 25–42. [Google Scholar] [CrossRef]
- Sternberg, R.J. Cognitive Psychology, 7th ed.; CENGAGE Learning: Boston, MA, USA, 2017. [Google Scholar]
- Weaver, B.; Bedard, M.; McAuliffe, J.; Parkkari, M. Using the Attention Network Test to predict driving test scores. Accid. Anal. Prev. 2009, 41, 76–83. [Google Scholar] [CrossRef]
- Choi, H.; Kasko, J.; Feng, J. An Attention Assessment for Informing Older Drivers’ Crash Risks in Various Hazardous Situations. Gerontologist 2019, 59, 112–123. [Google Scholar] [CrossRef]
- Jongen, S.; Vuurman, E.; Ramaekers, J.G.; Vermeeren, A. Comparing the effects of oxazepam and diazepam in actual highway driving and neurocognitive test performance: A validation study. Psychopharmacology 2018, 235, 1283–1294. [Google Scholar] [CrossRef] [Green Version]
- Jongen, S.; Perrier, J.; Vuurman, E.F.; Ramaekers, J.G.; Vermeeren, A. Sensitivity and validity of psychometric tests for assessing driving impairment: Effects of sleep deprivation. PLoS ONE 2015, 10, e0117045. [Google Scholar] [CrossRef]
- Zamani Sani, S.H.; Sadeghi-Bazargani, H.; Fathirezaie, Z.; Hadidi, Y.; Brand, S. Higher symptoms of attention-deficit/hyperactivity disorders (ADHD) and younger age were associated with faster visual perception, but not with lower traffic violations. Transp. Res. Part F Traffic Psychol. Behav. 2019, 66, 419–429. [Google Scholar] [CrossRef]
- Gershon, P.; Ben-Asher, N.; Shinar, D. Attention and search conspicuity of motorcycles as a function of their visual context. Accid. Anal. Prev. 2012, 44, 97–103. [Google Scholar] [CrossRef]
- Zhang, T.; Chan, A.H.S.; Ba, Y.; Zhang, W. Situational driving anger, driving performance and allocation of visual attention. Transp. Res. Part F Traffic Psychol. Behav. 2016, 42, 376–388. [Google Scholar] [CrossRef]
- Pierce, R.S.; Andersen, G.J. The effects of age and workload on 3D spatial attention in dual-task driving. Accid. Anal. Prev. 2014, 67, 96–104. [Google Scholar] [CrossRef] [Green Version]
- Arexis, M.; Maquestiaux, F.; Gaspelin, N.; Ruthruff, E.; Didierjean, A. Attentional capture in driving displays. Br. J. Psychol. 2017, 108, 259–275. [Google Scholar] [CrossRef]
- Choi, H.; Geden, M.; Feng, J. More visual mind wandering occurrence during visual task performance: Modality of the concurrent task affects how the mind wanders. PLoS ONE 2017, 12, e0189667. [Google Scholar] [CrossRef] [Green Version]
- Zheng, X.; Yang, Y.; Easa, S.; Lin, W.; Cherchi, E. The effect of leftward bias on visual attention for driving tasks. Transp. Res. Part F Traffic Psychol. Behav. 2020, 70, 199–207. [Google Scholar] [CrossRef]
- Hosking, S.G.; Young, K.L.; Regan, M.A. The effects of text messaging on young drivers. Hum. Factors 2009, 51, 582–592. [Google Scholar] [CrossRef] [Green Version]
- Salmon, P.M.; Young, K.L.; Regan, M.A. Distraction ‘on the buses’: A novel framework of ergonomics methods for identifying sources and effects of bus driver distraction. Appl. Ergon. 2011, 42, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Atchley, P.; Tran, A.V.; Salehinejad, M.A. Constructing a publically available distracted driving database and research tool. Accid. Anal. Prev. 2017, 99, 306–311. [Google Scholar] [CrossRef]
- Atwood, J.; Guo, F.; Fitch, G.; Dingus, T.A. The driver-level crash risk associated with daily cellphone use and cellphone use while driving. Accid. Anal. Prev. 2018, 119, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Dingus, T.A.; Guo, F.; Lee, S.; Antin, J.F.; Perez, M.; Buchanan-King, M.; Hankey, J. Driver crash risk factors and prevalence evaluation using naturalistic driving data. Proc. Natl. Acad. Sci. USA 2016, 113, 2636–2641. [Google Scholar] [CrossRef] [Green Version]
- Larsen, L.; Kines, P. Multidisciplinary in-depth investigations of head-on and left-turn road collisions. Accid. Anal. Prev. 2002, 34, 367–380. [Google Scholar] [CrossRef]
- Sagberg, F.; Bjornskau, T. Hazard perception and driving experience among novice drivers. Accid. Anal. Prev. 2006, 38, 407–414. [Google Scholar] [CrossRef]
- Ericson, J.M.; Parr, S.A.; Beck, M.R.; Wolshon, B. Compensating for failed attention while driving. Transp. Res. Part F Traffic Psychol. Behav. 2017, 45, 65–74. [Google Scholar] [CrossRef]
- Dekkers, T.J.; Popma, A.; Agelink van Rentergem, J.A.; Bexkens, A.; Huizenga, H.M. Risky decision making in Attention-Deficit/Hyperactivity Disorder: A meta-regression analysis. Clin. Psychol. Rev. 2016, 45, 1–16. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 5th Edition: DSM 5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Polanczyk, C.A.; de Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef]
- Polanczyk, C.A.; Willcutt, E.G.; Salum, G.A.; Kieling, C.; Rohde, L.A. ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. Int. J. Epidemiol. 2014, 43, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child. Psychol. Psychiatry Allied Discip. 2015, 56, 345–365. [Google Scholar] [CrossRef]
- Caci, H.M.; Morin, A.J.; Tran, A. Prevalence and correlates of attention deficit hyperactivity disorder in adults from a French community sample. J. Nerv. Ment. Dis. 2014, 202, 324–332. [Google Scholar] [CrossRef] [Green Version]
- Caye, A.; Rocha, T.B.; Anselmi, L.; Murray, J.; Menezes, A.M.; Barros, F.C.; Goncalves, H.; Wehrmeister, F.; Jensen, C.M.; Steinhausen, H.C.; et al. Attention-Deficit/Hyperactivity Disorder Trajectories From Childhood to Young Adulthood: Evidence From a Birth Cohort Supporting a Late-onset Syndrome. JAMA Psychiatry 2016. [Google Scholar] [CrossRef] [Green Version]
- Instanes, J.T.; Klungsoyr, K.; Halmoy, A.; Fasmer, O.B.; Haavik, J. Adult ADHD and Comorbid Somatic Disease: A Systematic Literature Review. J. Atten. Disord. 2018, 22, 203–228. [Google Scholar] [CrossRef] [Green Version]
- Agnew-Blais, J.C.; Polanczyk, G.V.; Danese, A.; Wertz, J.; Moffitt, T.E.; Arseneault, L. Evaluation of the Persistence, Remission, and Emergence of Attention-Deficit/Hyperactivity Disorder in Young Adulthood. JAMA Psychiatry 2016, 73, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Moffitt, T.E.; Houts, R.; Asherson, P.; Belsky, D.W.; Corcoran, D.L.; Hammerle, M.; Harrington, H.; Hogan, S.; Meier, M.H.; Polanczyk, G.V.; et al. Is Adult ADHD a Childhood-Onset Neurodevelopmental Disorder? Evidence From a Four-Decade Longitudinal Cohort Study. Am. J. Psychiatry 2015, 172, 967–977. [Google Scholar] [CrossRef] [PubMed]
- Asherson, P.; Buitelaar, J.; Faraone, S.V.; Rohde, L.A. Adult attention-deficit hyperactivity disorder: Key conceptual issues. Lancet Psychiatry 2016, 3, 568–578. [Google Scholar] [CrossRef] [Green Version]
- Hechtman, L.; Swanson, J.M.; Sibley, M.H.; Stehli, A.; Owens, E.B.; Mitchell, J.T.; Arnold, L.E.; Molina, B.S.G.; Hinshaw, S.P.; Jensen, P.S.; et al. Functional Adult Outcomes 16 Years After Childhood Diagnosis of Attention-Deficit/Hyperactivity Disorder: MTA Results. J. Am. Acad. Child. Adolesc. Psychiatry 2016, 55, 945–952.e942. [Google Scholar] [CrossRef] [Green Version]
- Buss, D.M. Evoutionary Psychology: The New Science of the Mind, 6th ed.; Routledge: New York, NY, USA, 2019. [Google Scholar]
- Stevens, A.; Price, J. Evolutionary Psychiatry: A New Beginning; Routledge: New York, NY, USA; Taylor & Francis Group: London, UK, 2000. [Google Scholar]
- González-Carpio Hernández, G.; Serrano Selva, J.P. Medication and creativity in Attention Deficit Hyperactivity Disorder (ADHD). Psicothema 2016, 28, 20–25. [Google Scholar] [CrossRef]
- Gvirts, H.Z.; Mayseless, N.; Segev, A.; Lewis, D.Y.; Feffer, K.; Barnea, Y.; Bloch, Y.; Shamay-Tsoory, S.G. Novelty-seeking trait predicts the effect of methylphenidate on creativity. J. Psychopharmacol. 2017, 31, 599–605. [Google Scholar] [CrossRef]
- Fuermaier, A.B.; Tucha, L.; Evans, B.L.; Koerts, J.; de Waard, D.; Brookhuis, K.; Aschenbrenner, S.; Thome, J.; Lange, K.W.; Tucha, O. Driving and attention deficit hyperactivity disorder. J. Neural Transm. 2017, 124, 55–67. [Google Scholar] [CrossRef] [Green Version]
- De La Fuente, A.; Xia, S.; Branch, C.; Li, X. A review of attention-deficit/hyperactivity disorder from the perspective of brain networks. Front. Hum. Neurosci. 2013, 7, 192. [Google Scholar] [CrossRef] [Green Version]
- Oberlin, B.G.; Alford, J.L.; Marrocco, R.T. Normal attention orienting but abnormal stimulus alerting and conflict effect in combined subtype of ADHD. Behav. Brain. Res. 2005, 165, 1–11. [Google Scholar] [CrossRef]
- Willcutt, E.G.; Doyle, A.E.; Nigg, J.T.; Faraone, S.V.; Pennington, B.F. Validity of the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic review. Biol. Psychiatry 2005, 57, 1336–1346. [Google Scholar] [CrossRef]
- Schachar, R.; Mota, V.L.; Logan, G.D.; Tannock, R.; Klim, P. Confirmation of an inhibitory control deficit in attention-deficit/hyperactivity disorder. J. Abnorm. Child. Psychol. 2000, 28, 227–235. [Google Scholar] [CrossRef]
- Johnson, K.A.; Robertson, I.H.; Barry, E.; Mulligan, A.; Dáibhis, A.; Daly, M.; Watchorn, A.; Gill, M.; Bellgrove, M.A. Impaired conflict resolution and alerting in children with ADHD: Evidence from the Attention Network Task (ANT). J. Child. Psychol. Ppsychiatry Allied Discip. 2008, 49, 1339–1347. [Google Scholar] [CrossRef] [PubMed]
- Aduen, P.A.; Kofler, M.J.; Cox, D.J.; Sarver, D.E.; Lunsford, E. Motor vehicle driving in high incidence psychiatric disability: Comparison of drivers with ADHD, depression, and no known psychopathology. J. Psychiatr. Res. 2015, 64, 59–66. [Google Scholar] [CrossRef]
- Ankem, G.; Klauer, C.; Ollendick, T.; Dingus, T.; Guo, F. 2343—How Risky Are ADHD Teen Drivers? Analysis of ADHD Teen Drivers Using Naturalistic Driving Data. J. Transp. Health 2018, 9, S13. [Google Scholar] [CrossRef]
- Barkley, R.A.; Cox, D. A review of driving risks and impairments associated with attention-deficit/hyperactivity disorder and the effects of stimulant medication on driving performance. J. Saf. Res. 2007, 38, 113–128. [Google Scholar] [CrossRef]
- Thorslund, B.; Lidestam, B. 2037—Effects of ADHD on Driving Behaviour and Attention. J. Transp. Health 2017, 5, S77. [Google Scholar] [CrossRef]
- Sobanski, E.; Bruggemann, D.; Alm, B.; Kern, S.; Philipsen, A.; Schmalzried, H.; Hesslinger, B.; Waschkowski, H.; Rietschel, M. Subtype differences in adults with attention-deficit/hyperactivity disorder (ADHD) with regard to ADHD-symptoms, psychiatric comorbidity and psychosocial adjustment. Eur. Psychiatry 2008, 23, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Adamo, N.; Del Giovane, C.; Mohr-Jensen, C.; Hayes, A.J.; Carucci, S.; Atkinson, L.Z.; Tessari, L.; Banaschewski, T.; Coghill, D.; et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: A systematic review and network meta-analysis. Lancet Psychiatry 2018, 5, 727–738. [Google Scholar] [CrossRef] [Green Version]
- Vaa, T. ADHD and relative risk of accidents in road traffic: A meta-analysis. Accid. Anal. Prev. 2014, 62, 415–425. [Google Scholar] [CrossRef] [Green Version]
- Barkley, R.A.; Guevremont, D.C.; Anastopoulos, A.D.; DuPaul, G.J.; Shelton, T.L. Driving-related risks and outcomes of attention deficit hyperactivity disorder in adolescents and young adults: A 3- to 5-year follow-up survey. Pediatrics 1993, 92, 212–218. [Google Scholar]
- Ortega, R.; Lopez, V.; Carrasco, X.; Anllo-Vento, L.; Aboitiz, F. Exogenous orienting of visual-spatial attention in ADHD children. Brain Res. 2013, 1493, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Turkan, B.N.; Amado, S.; Ercan, E.S.; Percinel, I. Comparison of change detection performance and visual search patterns among children with/without ADHD: Evidence from eye movements. Res. Dev. Disabil. 2016, 49–50, 205–215. [Google Scholar] [CrossRef]
- Laasonen, M.; Salomaa, J.; Cousineau, D.; Leppamaki, S.; Tani, P.; Hokkanen, L.; Dye, M. Project DyAdd: Visual attention in adult dyslexia and ADHD. Brain Cogn. 2012, 80, 311–327. [Google Scholar] [CrossRef]
- Philip, P.; Micoulaud-Franchi, J.A.; Lagarde, E.; Taillard, J.; Canel, A.; Sagaspe, P.; Bioulac, S. Attention Deficit Hyperactivity Disorder Symptoms, Sleepiness and Accidental Risk in 36140 Regularly Registered Highway Drivers. PLoS ONE 2015, 10, e0138004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vance, D.E.; Fazeli, P.L.; Ball, D.A.; Slater, L.Z.; Ross, L.A. Cognitive functioning and driving simulator performance in middle-aged and older adults with HIV. J. Assoc. Nurses AIDS Care 2014, 25, e11–e26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro, C.; Padilla, J.L.; Doncel, P.; Garcia-Fernandez, P.; Ventsislavova, P.; Eisman, E.; Crundall, D. How are distractibility and hazard prediction in driving related? Role of driving experience as moderating factor. Appl. Ergon. 2019, 81, 102886. [Google Scholar] [CrossRef] [PubMed]
- Crundall, D. Hazard prediction discriminates between novice and experienced drivers. Accid. Anal. Prev. 2016, 86, 47–58. [Google Scholar] [CrossRef] [Green Version]
- Zhang, T.; Chan, A.H. The association between driving anger and driving outcomes: A meta-analysis of evidence from the past twenty years. Accid. Anal. Prev. 2016, 90, 50–62. [Google Scholar] [CrossRef]
- Green, J.G.; DeYoung, G.; Wogan, M.E.; Wolf, E.J.; Lane, K.L.; Adler, L.A. Evidence for the reliability and preliminary validity of the Adult ADHD Self-Report Scale v1.1 (ASRS v1.1) Screener in an adolescent community sample. Int. J. Methods Psychiatr. Res. 2018, e1751. [Google Scholar] [CrossRef] [Green Version]
- Ustun, B.; Adler, L.A.; Rudin, C.; Faraone, S.V.; Spencer, T.J.; Berglund, P.; Gruber, M.J.; Kessler, R.C. The World Health Organization Adult Attention-Deficit/Hyperactivity Disorder Self-Report Screening Scale for DSM-5. JAMA Psychiatry 2017, 74, 520–526. [Google Scholar] [CrossRef] [Green Version]
- Roca, J.; Castro, C.; López-Ramón, M.F.; Lupiáñez, J. Measuring vigilance while assessing the functioning of the three attentional networks: The ANTI-Vigilance task. J. Neurosci. Methods 2011, 198, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Yerkes, R.M.; Dodson, J.D. The relation of strength of stimulus to rapidity of habit-formation. J. Comp. Neurol. Psychol. 1908, 18, 459–482. [Google Scholar] [CrossRef] [Green Version]
- Abdoli, N.; Farnia, V.; Delavar, A.; Esmaeili, A.; Dortaj, F.; Farrokhi, N.; Karami, M.; Shakeri, J.; Holsboer-Trachsler, E.; Brand, S. Poor mental health status and aggression are associated with poor driving behavior among male traffic offenders. Neuropsychiatr. Dis. Treat. 2015, 11, 2071–2078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yordanova, J.; Albrecht, B.; Uebel, H.; Kirov, R.; Banaschewski, T.; Rothenberger, A.; Kolev, V. Independent oscillatory patterns determine performance fluctuations in children with attention deficit/hyperactivity disorder. Brain 2011, 134, 1740–1750. [Google Scholar] [CrossRef] [Green Version]
- Burwell, S.J.; Makeig, S.; Iacono, W.G.; Malone, S.M. Reduced premovement positivity during the stimulus-response interval precedes errors: Using single-trial and regression ERPs to understand performance deficits in ADHD. Psychophysiology 2019, e13392. [Google Scholar] [CrossRef]
- Diaz-Roman, A.; Mitchell, R.; Cortese, S. Sleep in adults with ADHD: Systematic review and meta-analysis of subjective and objective studies. Neurosci. Biobehav. Rev. 2018, 89, 61–71. [Google Scholar] [CrossRef]
- Husain, S.F.; Yu, R.; Tang, T.B.; Tam, W.W.; Tran, B.; Quek, T.T.; Hwang, S.H.; Chang, C.W.; Ho, C.S.; Ho, R.C. Validating a functional near-infrared spectroscopy diagnostic paradigm for Major Depressive Disorder. Sci. Rep. 2020, 10, 9740. [Google Scholar] [CrossRef]

{kind=link}
| Dimensions | ||||||||
|---|---|---|---|---|---|---|---|---|
| Dimensions | Age | Accidents | At-Fault Accidents | Traffic Violations | Driving Frequency 1 | Driving Experience | ADHD | M (SD) |
| Age | - | 0.06 | 0.09 | −0.32 ** | - | - | −0.05 | 31.37 (9.75) |
| Accidents | - | - | 0.69 ** | 0.31 ** | - | - | 0.15 * | 1.20 (1.68) |
| At-fault accidents | - | - | - | 0.19 ** | - | - | 0.16 * | 0.53 (1.04) |
| Traffic violations | - | - | - | - | - | - | 0.45 *** | 35.28 (9.78) |
| ADHD | - | - | - | - | - | - | - | 1.85 (1.39) |
| Driving frequency 1 | 0.09 | 0.09 | 0.07 | 0.06 | - | - | 0.01 | 1.58 (1.13) |
| Driving experience | 0.82 ** | 0.18 ** | 0.12 | −0.17 ** | 0.20 ** | - | −0.04 | 9.30 (7.81) |
| Attentional network tasks | 0.16 | −0.06 | −0.03 | −0.30 ** | 0.05 | 0.32 ** | −0.07 | 56.59 (20.13) |
| Alerting | 0.06 | 0.01 | 0.01 | −0.05 | 0.08 | 0.09 | −0.10 | 37.89 (30.56) |
| Orienting | 0.06 | −0.04 | 0.07 | −0.04 | 0.04 | 0.04 | −0.04 | 45.54 (33.67) |
| Executive function | 0.08 | −0.5 | −0.11 | −0.13 * | 0.09 | 0.12 | −0.04 | 86.35 (38.84) |
| Correct answers (%) | −0.12 | −0.03 | −0.04 | −0.08 | 0.04 | −0.18 | 0.03 | 95.32 (4.67) |
| Incorrect answers (%) | 0.12 | 0.04 | 0.03 | 0.07 | −0.04 | 0.18 | −0.03 | 4.67 (5.25) |
| Dimension | Variables | Coefficient | Standard Error | Coefficient β | T | p | R | R2 | Durbin-Watson Coefficient |
|---|---|---|---|---|---|---|---|---|---|
| Violations | Intercept | 53.96 | 3.40 | - | 15.86 | 0.0001 | 0.557 | 0.310 | 2.119 |
| Attentional network tasks score | −0.015 | 0.005 | −0.176 | −3.031 | 0.003 | ||||
| Symptoms of ADHD | 2.164 | 0.334 | 0.336 | 6.479 | 0.0001 | ||||
| Age | −0.223 | 0.054 | −0.242 | −4.158 | 0.0001 | ||||
| Driving frequency | 3.981 | 0.754 | 0.275 | 5.277 | 0.0001 | ||||
| Excluded variables | Driving experience, Alertness, Orientation, Executive function (all t’s < 1.4, all p’s > 0.14) | ||||||||
| Accidents | Intercept | 2.077 | 0.505 | - | 4.114 | 0.0001 | 0.319 | 0.102 | 1.987 |
| Symptoms of ADHD | 0.176 | 0.073 | 0.145 | 2.421 | 0.016 | ||||
| Age | −0.042 | 0.018 | −0.236 | −2.313 | 0.022 | ||||
| Driving experience | 0.076 | 0.023 | 0.343 | 3.312 | 0.001 | ||||
| Driving frequency | 0.435 | 0.169 | 0.159 | 2.582 | 0.010 | ||||
| Excluded variables | Attentional network task score, Alertness, Orientation, Executive function (all t’s < 1.0, all p’s > 0.16) | ||||||||
| t | Df | p | Mean Difference | Std. Error Difference | Cohen’s d | M (SD) | ||
|---|---|---|---|---|---|---|---|---|
| Offenders | Non-Offenders | |||||||
| Age | 1.058 | 261 | 0.291 | 1.258 | 1.189 | 0.13 | 31.70 (8.6) | 30.45 (10.50) |
| Driving experience | 2.748 | 261 | 0.006 | 2.590 | 0.942 | 0.34 | 10.37 (7.28) | 7.78 (7.79) |
| Driving frequency | −2.785 | 261 | 0.006 | −0.209 | 0.075 | 0.34 | 1.47 (.67) | 1.26 (.53) |
| Attentional network tasks | −0.377 | 261 | 0.706 | −5.068 | 13.428 | 0.05 | 704.53 (97.87) | 709.60 (119.33) |
| Alerting | 1.395 | 261 | 0.164 | 5.313 | 3.809 | 0.17 | 40.57 (31.81) | 35.26 (29.84) |
| Orienting | −1.249 | 261 | 0.213 | −5.102 | 4.085 | 0.15 | 42.30 (33.04) | 47.40 (33.18) |
| Executive function | −0.640 | 261 | 0.523 | −3.091 | 4.828 | 0.08 | 85.53 (35.60) | 88.63 (42.55) |
| ADHD | 2.879 | 261 | 0.004 | 0.49204 | 0.17090 | 0.35 | 2.09 (1.42) | 1.60 (1.34) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zamani Sani, S.H.; Fathirezaie, Z.; Sadeghi-Bazargani, H.; Badicu, G.; Ebrahimi, S.; Grosz, R.W.; Sadeghi Bahmani, D.; Brand, S. Driving Accidents, Driving Violations, Symptoms of Attention-Deficit-Hyperactivity (ADHD) and Attentional Network Tasks. Int. J. Environ. Res. Public Health 2020, 17, 5238. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145238
Zamani Sani SH, Fathirezaie Z, Sadeghi-Bazargani H, Badicu G, Ebrahimi S, Grosz RW, Sadeghi Bahmani D, Brand S. Driving Accidents, Driving Violations, Symptoms of Attention-Deficit-Hyperactivity (ADHD) and Attentional Network Tasks. International Journal of Environmental Research and Public Health. 2020; 17(14):5238. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145238
Chicago/Turabian StyleZamani Sani, Seyed Hojjat, Zahra Fathirezaie, Homayoun Sadeghi-Bazargani, Georgian Badicu, Safyeh Ebrahimi, Robert Wilhelm Grosz, Dena Sadeghi Bahmani, and Serge Brand. 2020. "Driving Accidents, Driving Violations, Symptoms of Attention-Deficit-Hyperactivity (ADHD) and Attentional Network Tasks" International Journal of Environmental Research and Public Health 17, no. 14: 5238. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145238