Comparative Evaluation of Dental Implant Failure among Healthy and Well-Controlled Diabetic Patients—A 3-Year Retrospective Study


 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
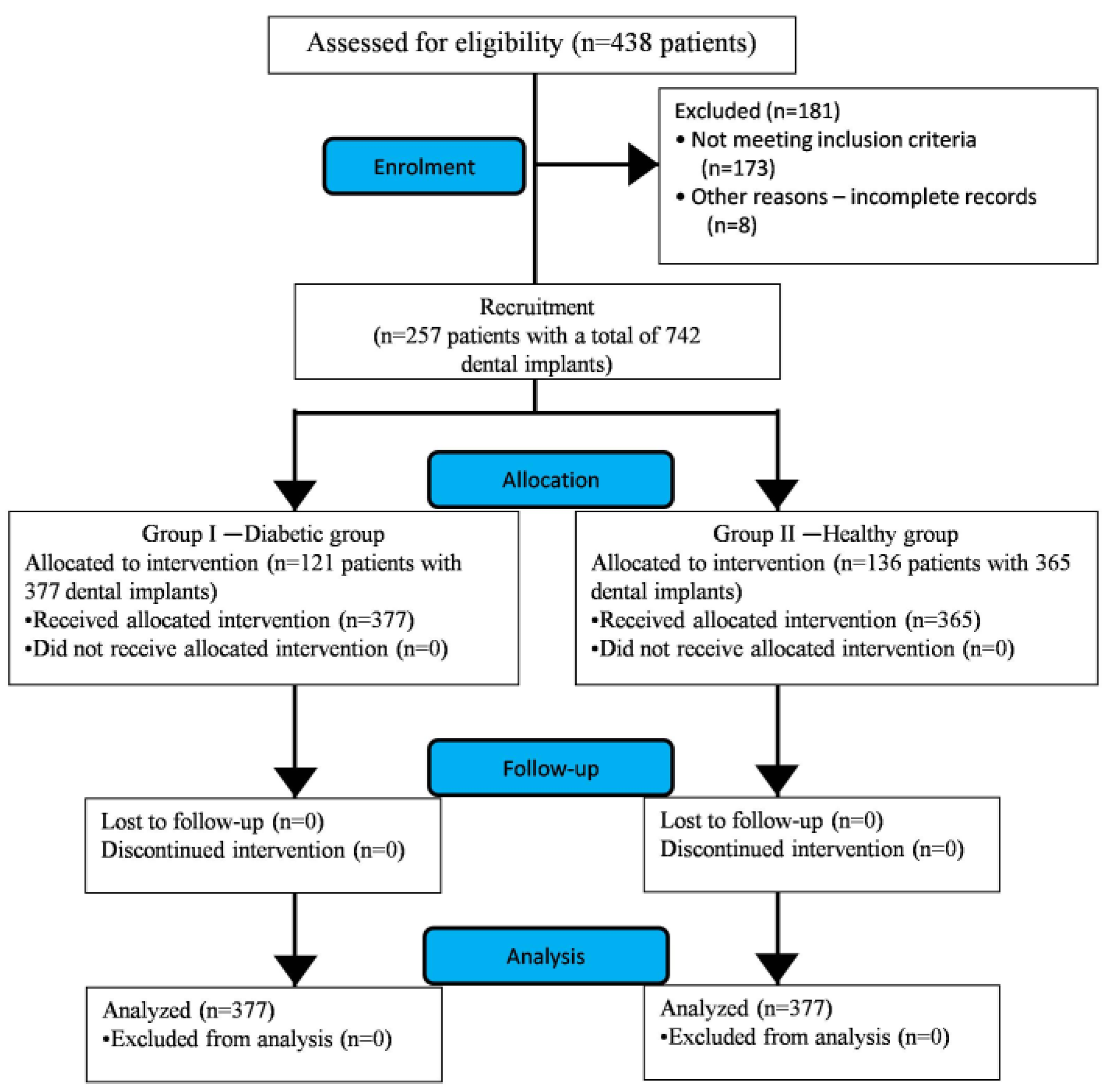
2.1. Description of the Study
2.2. Sample Description
2.3. Study Protocol
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistical Analysis Related to Sample
3.2. Inferential Statistical Analysis Related to Implant Failure
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017; Available online: https://www.idf.org/e-library/epidemiology-research/diabetes-atlas/134-idf-diabetes-atlas-8th-edition.html (accessed on 26 October 2019).
- Magliano, D.J.; Islam, R.M.; Barr, E.L.M.; Gregg, E.W.; Pavkov, M.E.; Harding, J.L.; Tabesh, M.; Koye, D.N.; Shaw, J.E. Trends in incidence of total or type 2 diabetes: Systematic review. BMJ 2019, 366. [Google Scholar] [CrossRef] [Green Version]
- Nazir, M.A.; AlGhamdi, L.; AlKadi, M.; AlBeajan, N.; AlRashoudi, L.; AlHussan, M. The burden of diabetes, its oral complications and their prevention and management. Open Access Maced. J. Med. Sci. 2018, 6, 1545–1553. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Classification and diagnosis of diabetes—Position statement. Diabetes Care 2015, 38, S8–S16. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Classification and diagnosis of diabetes: Standards of medical care in diabetes—2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [Green Version]
- Rhee, S.Y.; Kim, Y.S. The role of advanced glycation end products in diabetic vascular complications. Diabetes Metab. J. 2018, 42, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Saini, R.; Saini, S.; Sugandha, R. Periodontal disease: The sixth complication of diabetes. J Family Community Med. 2011, 18, 31. [Google Scholar] [CrossRef] [PubMed]
- Mauri-Obradors, E.; Estrugo-Devesa, A.; Jané-Salas, E.; Viñas, M.; López-López, J. Oral manifestations of diabetes mellitus. A systematic review. Med. Oral Patol. Oral Cir. Bucal 2017, 22, e586–e594. [Google Scholar] [CrossRef] [PubMed]
- Izuora, K.E.; Ezeanolue, E.E.; Neubauer, M.F.; Gewelber, C.L.; Allenback, G.L.; Umpierrez, G.E. Dental loss among ambulatory patients with Diabetes. J. Clin. Transl. Endocrinol. 2016, 4, 28–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maia, F.B.; De Sousa, E.T.; Sampaio, F.C.; Freitas, C.H.; Forte, F.D. Tooth loss in middle-aged adults with diabetes and hypertension: Social determinants, health perceptions, oral impact on daily performance (OIDP) and treatment need. Med. Oral Patol. Oral Cir. Bucal 2018, 23, e203–e210. [Google Scholar] [CrossRef]
- Rohani, B. Oral manifestations in patients with diabetes mellitus. World J. Diabetes 2019, 10, 485–489. [Google Scholar] [CrossRef]
- De Oliveira-Neto, O.B.; Santos, I.O.; Barbosa, F.T.; de Sousa-Rodrigues, C.F.; de Lima, F.J.C. Quality assessment of systematic reviews regarding dental implant placement on diabetic patients: An overview of systematic reviews. Med. Oral Patol. Oral Cir. Bucal. 2019, 24, e483–e490. [Google Scholar] [CrossRef]
- Katyayan, P.A.; Katyayan, M.; Shah, R.J. Rehabilitative considerations for dental implants in the diabetic patient. J. Indian Prosthodont. Soc. 2013, 13, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Naujokat, H.; Kunzendorf, B.; Wiltfang, J. Dental implants and diabetes mellitus-a systematic review. Int. J. Implant. Dent. 2016, 2, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howe, M.S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Diabetes and oral implant failure: A systematic review. J. Dent. Res. 2014, 93, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Moreno, G.; Aguilar-Salvatierra, A.; Rubio Roldan, J.; Guardia, J.; Gargallo, J.; Calvo-Guirado, J.L. Peri-implant evaluation in type 2 diabetes mellitus patients: A 3-year study. Clin. Oral Implants Res. 2014, 26, 1031–1035. [Google Scholar] [CrossRef]
- Ghiraldini, B.; Conte, A.; Casarin, R.C.; Casati, M.Z.; Pimentel, S.P.; Cirano, F.R.; Ribeiro, F.V. Influence of glycemic control on peri-implant bone healing: 12-month outcomes of local release of bone-related factors and implant stabilization in type 2 diabetics. Clin. Implant Dent. Relat. Res. 2016, 18, 801–809. [Google Scholar] [CrossRef]
- World Health Organization. Use of Glycated Haemoglobin (HbA1c) in the Diagnosis of Diabetes Mellitus: Abbreviated Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar] [PubMed]
- Khader, Y.S.; Dauod, A.S.; El-Qaderi, S.S.; Alkafajei, A.; Batayha, W.Q. Periodontal status of diabetics compared with non-diabetics: A meta-analysis. J. Diabetes Complications 2006, 20, 59–68. [Google Scholar] [CrossRef]
- Javed, F.; Romanos, G.E. Impact of diabetes mellitus and glycemic control on the osseointegration of dental implants: A systematic literature review. J. Periodontol. 2009, 80, 1719–1730. [Google Scholar] [CrossRef]
- Mellado-Valero, A.; Ferrer-García, J.C.; Herrera-Ballester, A.; Labaig-Rueda, C. Effects of diabetes on the osseointegration of dental implants. Med. Oral Patol. Oral Cir. Bucal 2007, 12, E38–E43. [Google Scholar]
- Olson, J.; Shernoff, A.; Tarlow, J.; Colwell, J.A.; Scheetz, J.P.; Bingham, S.F. Dental osseous implant assessments in a type 2 diabetic population: A prospective study. Int. J. Oral Maxillofac. Implants 2000, 15, 811–818. [Google Scholar]
- Balshi, T.; Wolfinger, G. Dental implants in the diabetic patient: A retrospective study. Implant Dent. 1999, 4, 355–359. [Google Scholar] [CrossRef] [Green Version]
- Farzad, P.; Andersson, L.; Nyberg, J. Dental implant treatment in diabetic patients. Implant Dent. 2002, 11, 262–267. [Google Scholar] [CrossRef]
- Tawil, G.; Younan, R.; Azar, P.; Sleilati, G. Conventional and advanced implant treatment in the type II diabetic patient: Surgical protocol and long-term clinical results. Int. J. Oral Maxillofac. Implants 2008, 23, 744–752. [Google Scholar]
- Oates, T.W.; Huynh-Ba, G.; Vargas, A.; Alexander, P.; Feine, J. A critical review of diabetes, glycemic control, and dental implant therapy. Clin. Oral Implants Res. 2013, 24, 117–127. [Google Scholar] [CrossRef] [Green Version]
- Oates, T.W.; Jr Galloway, P.; Alexander, P.; Vargas Green, A.; Huynh-Ba, G.; Feine, J.; McMahan, C.A. The effects of elevated hemoglobinA(1c) in patients with type 2 diabetes mellitus on dental implants: Survival and stability at one year. J. Am. Dent. Assoc. 2014, 145, 1218–1226. [Google Scholar] [CrossRef] [Green Version]
- Marchand, F.; Raskin, A.; Dionnes-Hornes, A.; Barry, T.; Dubois, N.; Valéro, R.; Vialettes, B. Dental implants and diabetes: Conditions for success. Diab. Metab. 2012, 38, 14–19. [Google Scholar] [CrossRef]
- Schwartz, A.V.; Sellmeyer, D.E.; Ensrud, K.E.; Cauley, J.A.; Tabor, H.K.; Schreiner, P.J.; Jamal, S.A.; Black, D.M.; Cummings, S.R. Older women with diabetes have an increased risk of fracture: A prospective study. J. Clin. Endocrinol. Metab. 2001, 86, 32–38. [Google Scholar] [CrossRef]
- Al Jabbari, Y.; Nagy, W.W.; Iacopino, A.M. Implant dentistry for geriatric patients: A review of the literature. Quintessence Int. 2003, 34, 281–285. [Google Scholar]
- Dubey, R.K.; Gupta, D.K.; Singh, A.K. Dental implant survival in diabetic patients; review and recommendations. Natl. J. Maxillofac. Surg. 2013, 4, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Alsaadi, G.; Quirynem, M.; Komarek, A.; Van Steenberghe, D. Impact of local and systemic factors on the incidence of late oral implant loss. Clin. Oral Implants Res. 2008, 19, 670–676. [Google Scholar] [PubMed]
- Fiorellini, J.P.; Chen, P.K.; Nevins, M.; Nevins, M.L. A retrospective study of dental implants in diabetic patients. Int. J. Periodontics Restorative Dent. 2000, 20, 366–373. [Google Scholar] [PubMed]
- Moy, P.K.; Medina, D.; Shetty, V.; Aghaloo, T.L. Dental implant failure rates and associated risk factors. Int. J. Oral Maxillofac. Implants. 2005, 20, 569–577. [Google Scholar] [PubMed]
- Alzarea, B.K.; Sghaireen, M.G.; Taher, I.; Mohager, M. Prevalence of oral candidiasis in diabetic patients at Northern of Kingdom of Saudi Arabia. J. Biol. Res. (Thessalon) 2015, 10, 10–14. [Google Scholar] [CrossRef] [Green Version]
- Al-Zarea, B.; Sghaireen, M.G. Efficacy of myrrh mouth rinse vs. chlorhexidine mouth rinse in maintaining the soft tissue health around dental implants: A comparative study. Int. Med. J. 2020, 27, p92–p94. [Google Scholar]
- Daubert, D.M.; Weinstein, B.F.; Bordin, S.; Leroux, B.G.; Flemming, T.F. Prevalence and predictive factors for peri-implant disease and implant failure: A crosssectional analysis. J. Periodontol. 2015, 86, 337–347. [Google Scholar] [CrossRef]
- Morris, H.F.; Ochi, S.; Winkler, S. Implant survival in patients with type 2 diabetes: Placement to 36 months. Ann. Periodontol. 2000, 5, 157–165. [Google Scholar] [CrossRef]
- Michaeli, E.; Weinberg, I.; Nahlieli, O. Dental implants in the diabeticpatient: Systemic and rehabilitative considerations. Quintessence Int. 2009, 40, 639–645. [Google Scholar]
- Ting, M.; Palermo, M.; Donatelli, D.P.; Gaughan, J.P.; Suzuki, J.B.; Jefferies, S.R. A meta-analysis on the effect of implant characteristics on the survival of the wide-diameter implant. Int. J. Implant Dent. 2015, 1, 28. [Google Scholar] [CrossRef] [Green Version]
- Monje, A.; Catena, A.; Borgnakke, W.S. Association between diabetes mellitus/hyperglycaemia and peri-implant diseases: Systematic review and meta-analysis. J. Clin. Periodontol. 2017, 44, 636–648. [Google Scholar] [CrossRef]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implants 1986, 1, 11–25. [Google Scholar]
- Annibali, S.; Pranno, N.; Cristalli, M.P.; La Monaca, G.; Polimeni, A. Survival analysis of implant in patients with diabetes mellitus: A systematic review. Implant Dent. 2016, 25, 663–674. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
Common Inclusion Criteria:
| Common Exclusion Criteria: (A) Systemic
|
Inclusion Criteria for Diabetic Group I
| Exclusion Criteria for Diabetic Group I
|
Inclusion Criteria for Healthy Group II
| Exclusion Criteria for Healthy Group II
|
| Variable | Response | Study Group | Total | ||
|---|---|---|---|---|---|
| Study Group I—Diabetic | Study Group II—Healthy | ||||
| Sample Size | No. of patients | 121 | 136 | 257 | |
| Dental implants placed | 377 | 365 | 742 | ||
| Age (expressed as mean ± SD) | 62.41 ± 13.62 | 59.24 ± 29.36 | - | ||
| Gender | Males | 182 (48.27) | 178 (48.76) | 360 (48.51) | |
| Females | 195 (51.72) | 187 (51.23) | 382 (51.48) | ||
| Location in jaw | Maxilla | 175 (46.41) | 168 (46.02) | 343 (46.22) | |
| Mandible | 202 (53.58) | 197 (53.97) | 399 (53.77) | ||
| Variable | Study Groups | Total (742) | p Value | ||||
|---|---|---|---|---|---|---|---|
| Diabetic (n = 377) | Healthy (n = 365) | ||||||
| Implant failure rate | 37 (9.81) | 33 (9.04) | 70 (9.43) | 0.422 | |||
| Gender | Males | 18 (4.77) | 15 (4.10) | 33 (4.44) | 0.390 | ||
| Females | 19 (5.03) | 18 (4.93) | 37 (4.98) | 0.392 | |||
| Implant stability | Osseointegration | 17 (4.50) | 16 (4.38) | 33 (4.44) | 0.365 | ||
| Functional Loading | 20 (5.30) | 17 (4.65) | 37 (4.98) | 0.361 | |||
| Arch | Maxilla | 16 (4.24) | 14 (3.83) | 30 (4.04) | 0.921 | ||
| Mandible | 21 (5.57) | 19 (5.20) | 40 (5.39) | 0.402 | |||
| Location in the arch | Maxilla | Anterior | 7 (1.85) | 6 (1.64) | 13 (1.75) | 0.999 | |
| Posterior | 9 (2.38) | 8 (2.19) | 17 (2.29) | 0.983 | |||
| Mandible | Anterior | 9 (2.38) | 8 (2.19) | 17 (2.29) | 0.430 | ||
| Posterior | 12 (3.18) | 11 (3.01) | 23 (3.09) | 0.411 | |||
| Length of implant | <10 mm | 20 (5.30) | 17 (4.65) | 37 (4.98) | 0.918 | ||
| >10 mm | 17 (4.50) | 16 (4.38) | 33 (4.44) | 0.901 | |||
| Implant survival rate | 340 (90.18) | 332 (90.95) | 672 (90.56) | 0.410 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sghaireen, M.G.; Alduraywish, A.A.; Srivastava, K.C.; Shrivastava, D.; Patil, S.R.; Al Habib, S.; Hamza, M.; Ab Rahman, S.; Lynch, E.; Alam, M.K. Comparative Evaluation of Dental Implant Failure among Healthy and Well-Controlled Diabetic Patients—A 3-Year Retrospective Study. Int. J. Environ. Res. Public Health 2020, 17, 5253. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145253
Sghaireen MG, Alduraywish AA, Srivastava KC, Shrivastava D, Patil SR, Al Habib S, Hamza M, Ab Rahman S, Lynch E, Alam MK. Comparative Evaluation of Dental Implant Failure among Healthy and Well-Controlled Diabetic Patients—A 3-Year Retrospective Study. International Journal of Environmental Research and Public Health. 2020; 17(14):5253. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145253
Chicago/Turabian StyleSghaireen, Mohammed Ghazi, Abdulrahman A. Alduraywish, Kumar Chandan Srivastava, Deepti Shrivastava, Santosh R Patil, Selham Al Habib, May Hamza, Saifulizan Ab Rahman, Edward Lynch, and Mohammad Khursheed Alam. 2020. "Comparative Evaluation of Dental Implant Failure among Healthy and Well-Controlled Diabetic Patients—A 3-Year Retrospective Study" International Journal of Environmental Research and Public Health 17, no. 14: 5253. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145253