Correlation and Reliability Analyses among the Upper Cervical Rotation-Flexion Test, Upper Cervical Flexion-Extension Test, and Upper Cervical Flexion Angle Measurement Using Radiography

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Examiners
2.3. Measurement Systems
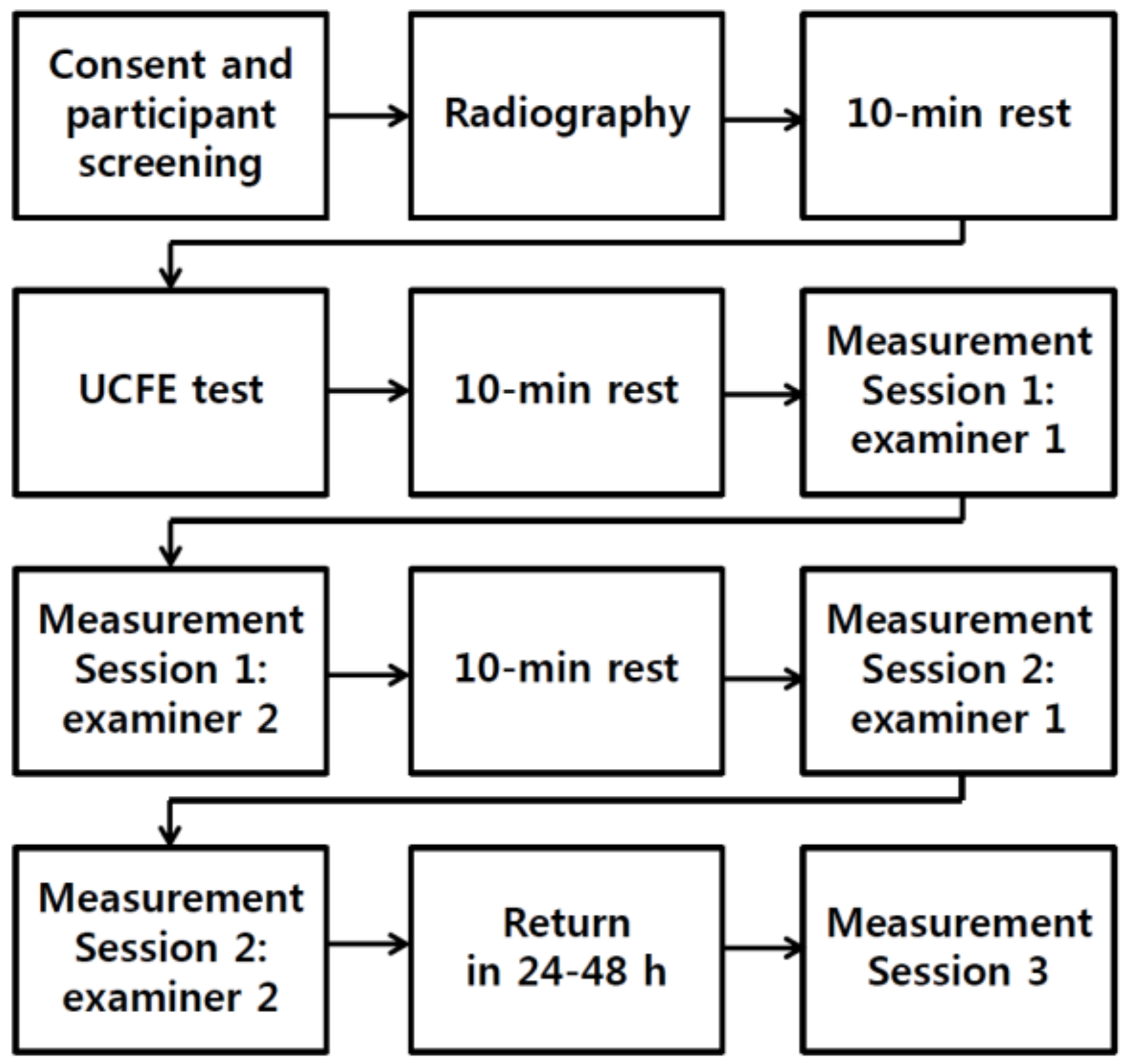
2.4. Procedure
2.5. Measurement of Upper Cervical Flexion Angle Using Radiography
2.6. UCFE Test
2.7. UCRF Test
2.8. Statistical Analysis
3. Results
3.1. Validity
3.2. Intra-Rater Reliability of the UCRF Test
3.3. Inter-Rater Reliability of the UCRF Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Stovner, L.; Hagen, K.; Jensen, R.; Katsarava, Z.; Lipton, R.B.; Scher, A.; Steiner, T.; Zwart, J.A. The global burden of headache: A documentation of headache prevalence and disability worldwide. Cephalalgia 2007, 27, 193–210. [Google Scholar] [CrossRef] [PubMed]
- Stovner, L.J.; Andree, C. Prevalence of headache in Europe: A review for the Eurolight project. J. Headache Pain 2010, 11, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stovner, L.J.; Hagen, K. Prevalence, burden, and cost of headache disorders. Curr. Opin. Neurol. 2006, 19, 281–285. [Google Scholar] [CrossRef]
- Amiri, M.; Jull, G.; Bullock-Saxton, J. Measuring range of active cervical rotation in a position of full head flexion using the 3D Fastrak measurement system: An intra-tester reliability study. Man. Ther. 2003, 8, 176–179. [Google Scholar] [CrossRef]
- Biondi, D.M. Cervicogenic headache: A review of diagnostic and treatment strategies. J. Am. Osteopath. Assoc. 2005, 105, 16–22S. [Google Scholar]
- Sjaastad, O.; Fredriksen, T.; Pfaffenrath, V. Cervicogenic headache: Diagnostic criteria. Headache J. Head Face Pain 1998, 38, 442–445. [Google Scholar] [CrossRef]
- Zito, G.; Jull, G.; Story, I. Clinical tests of musculoskeletal dysfunction in the diagnosis of cervicogenic headache. Man. Ther. 2006, 11, 118–129. [Google Scholar] [CrossRef]
- Sjaastad, O.; Bovim, G. Cervicogenic headache. The differentiation from common migraine. An overview. Funct. Neurol. 1991, 6, 93–100. [Google Scholar]
- Edwards, J.Z.; Greene, K.A.; Davis, R.S.; Kovacik, M.W.; Noe, D.A.; Askew, M.J. Measuring flexion in knee arthroplasty patients. J. Arthroplast. 2004, 19, 369–372. [Google Scholar] [CrossRef]
- Anderson, L.D.; D’alonzo, R.T. Fractures of the odontoid process of the axis. JBJS 1974, 56, 1663–1674. [Google Scholar] [CrossRef]
- Effendi, B.; Roy, D.; Cornish, B.; Dussault, R.; Laurin, C. Fractures of the ring of the axis. A classification based on the analysis of 131 cases. Bone Jt. J. 1981, 63, 319–327. [Google Scholar] [CrossRef]
- Levine, A.M.; Edwards, C. The management of traumatic spondylolisthesis of the axis. J. Bone Jt. Surg. Am. Vol. 1985, 67, 217–226. [Google Scholar] [CrossRef]
- Magee, D.J. Orthopedic Physical Assessment-E-Book; Elsevier Health Sciences: St. Louis, MO, USA, 2014. [Google Scholar]
- Gajdosik, R.L.; Bohannon, R.W. Clinical measurement of range of motion: Review of goniometry emphasizing reliability and validity. Phys. Ther. 1987, 67, 1867–1872. [Google Scholar] [CrossRef] [PubMed]
- Jull, G. Management of cervical headache. Man. Ther. 1997, 2, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Dhimitri, K.; Brodeur, S.; Croteau, M.; Richard, S.; Seymour, C.J. Reliability of the cervical range of motion device in measuring upper cervical motion. J. Man. Manip. Ther. 1998, 6, 31–36. [Google Scholar] [CrossRef]
- Ernst, M.J.; Crawford, R.J.; Schelldorfer, S.; Rausch-Osthoff, A.-K.; Barbero, M.; Kool, J.; Bauer, C.M. Extension and flexion in the upper cervical spine in neck pain patients. Man. Ther. 2015, 20, 547–552. [Google Scholar] [CrossRef] [Green Version]
- Donatelli, R.A.; Wooden, M.J. Orthopaedic Physical Therapy-E-Book; Elsevier Health Sciences: St. Louis, MO, USA, 2009. [Google Scholar]
- Cook, G.; Burton, L.; Kiesel, K.; Bryant, M.; Torine, J. Movement: Functional Movement Systems: Screening, Assessment, and Corrective Strategies; On Target Publications Aptos: Santa Cruz, CA, USA, 2010; Volume 24. [Google Scholar]
- Lexell, J.E.; Downham, D.Y. How to assess the reliability of measurements in rehabilitation. Am. J. Phys. Med. Rehabil. 2005, 84, 719–723. [Google Scholar] [CrossRef]
- Chan, C.A. A review of the clinical significance of the occlusal plane: Its variation and effect on head posture. Int. Coll. Craniomandib. Orthop. (Iccmo) Anthol. 2007, 8, 1–63. [Google Scholar]
- Trevethan, R. Intraclass correlation coefficients: Clearing the air, extending some cautions, and making some requests. Health Serv. Outcomes Res. Methodol. 2017, 17, 127–143. [Google Scholar] [CrossRef]
- Ionan, A.C.; Polley, M.-Y.C.; McShane, L.M.; Dobbin, K.K. Comparison of confidence interval methods for an intra-class correlation coefficient (ICC). BMC Med Res. Methodol. 2014, 14, 121. [Google Scholar] [CrossRef] [Green Version]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231. [Google Scholar] [PubMed]
- Beckerman, H.; Roebroeck, M.; Lankhorst, G.; Becher, J.; Bezemer, P.D.; Verbeek, A. Smallest real difference, a link between reproducibility and responsiveness. Qual. Life Res. 2001, 10, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.-S.; Wang, C.-H.; Lin, J.-H.; Sheu, C.-F.; Hsieh, C.-L. The minimal detectable change of the simplified stroke rehabilitation assessment of movement measure. J. Rehabil. Med. 2008, 40, 615–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogduk, N.; Mercer, S. Biomechanics of the cervical spine. I: Normal kinematics. Clin. Biomech. 2000, 15, 633–648. [Google Scholar] [CrossRef]
- Neumann, D.A. Kinesiology of the Musculoskeletal System-E-Book: Foundations for Rehabilitation; Elsevier Health Sciences: St. Louis, MO, USA, 2013. [Google Scholar]
- Hall, T.M.; Briffa, K.; Hopper, D.; Robinson, K. Comparative analysis and diagnostic accuracy of the cervical flexion–rotation test. J. Headache Pain 2010, 11, 391–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Mayoralas, D.M.; Fernández-de-las-Penas, C.; Palacios-Cena, D.; Cantarero-Villanueva, I.; Fernández-Lao, C.; Pareja, J.A. Restricted neck mobility in children with chronic tension type headache: A blinded, controlled study. J. Headache Pain 2010, 11, 399–404. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean ± SD | Pearson’s Correlation (r Value) | |||
|---|---|---|---|---|
| UCRF Test | UCFE Test | X-Ray | ||
| UCRF test | 8.84 ± 2.30 | 1 | 0.77 * | 0.80 * |
| UCFE test | 10.32 ± 3.64 | 0.77 * | 1 | 0.81 * |
| X-ray | 7.60 ± 2.71 | 0.80 * | 0.81 * | 1 |
| UCRF Test | SEM (°) | MDC (°) | ICC (95% CI) | ||
|---|---|---|---|---|---|
| 1st Session | 2nd Session | ||||
| Rater A | 9.10 ± 3.07 | 8.90 ± 2.25 | 0.70 | 1.95 | 0.93 **(0.85, 0.97) |
| Rater B | 8.82 ± 2.39 | 8.86 ± 2.33 | 0.54 | 1.50 | 0.94 **(0.87, 0.97) |
| Rater C | 8.86 ± 2.61 | 8.70 ± 2.64 | 0.58 | 1.61 | 0.95 **(0.90, 0.98) |
| 1st Session | 2nd Session | |||||
|---|---|---|---|---|---|---|
| ICC (95% CI) | SEM (°) | MDC (°) | ICC (95% CI) | SEM (°) | MDC (°) | |
| UCRF test | 0.90 ** (0.82, 0.95) | 0.80 | 2.24 | 0.95 ** (0.91, 0.98) | 0.48 | 1.35 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Do, K.; Choi, J.; Kim, J.; Yim, J. Correlation and Reliability Analyses among the Upper Cervical Rotation-Flexion Test, Upper Cervical Flexion-Extension Test, and Upper Cervical Flexion Angle Measurement Using Radiography. Int. J. Environ. Res. Public Health 2020, 17, 5262. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145262
Do K, Choi J, Kim J, Yim J. Correlation and Reliability Analyses among the Upper Cervical Rotation-Flexion Test, Upper Cervical Flexion-Extension Test, and Upper Cervical Flexion Angle Measurement Using Radiography. International Journal of Environmental Research and Public Health. 2020; 17(14):5262. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145262
Chicago/Turabian StyleDo, KwangSun, JaeSung Choi, JaeEun Kim, and JongEun Yim. 2020. "Correlation and Reliability Analyses among the Upper Cervical Rotation-Flexion Test, Upper Cervical Flexion-Extension Test, and Upper Cervical Flexion Angle Measurement Using Radiography" International Journal of Environmental Research and Public Health 17, no. 14: 5262. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17145262