Organizational Support in Healthcare Redesign Education: A Mixed-Methods Exploratory Study of Expert Coach and Executive Sponsor Experiences

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
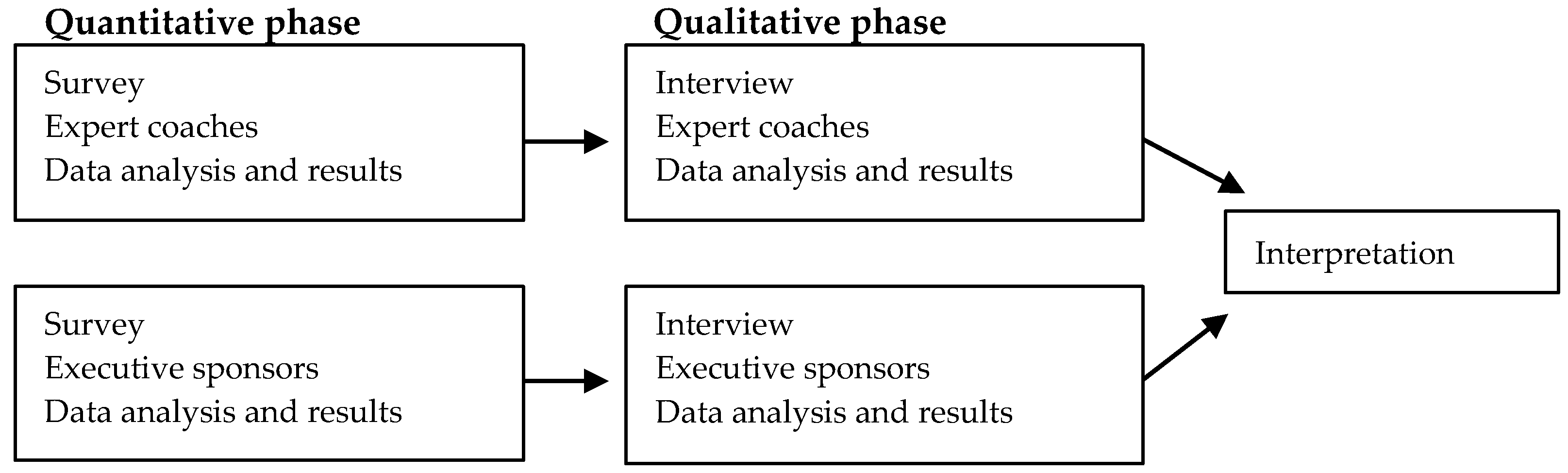
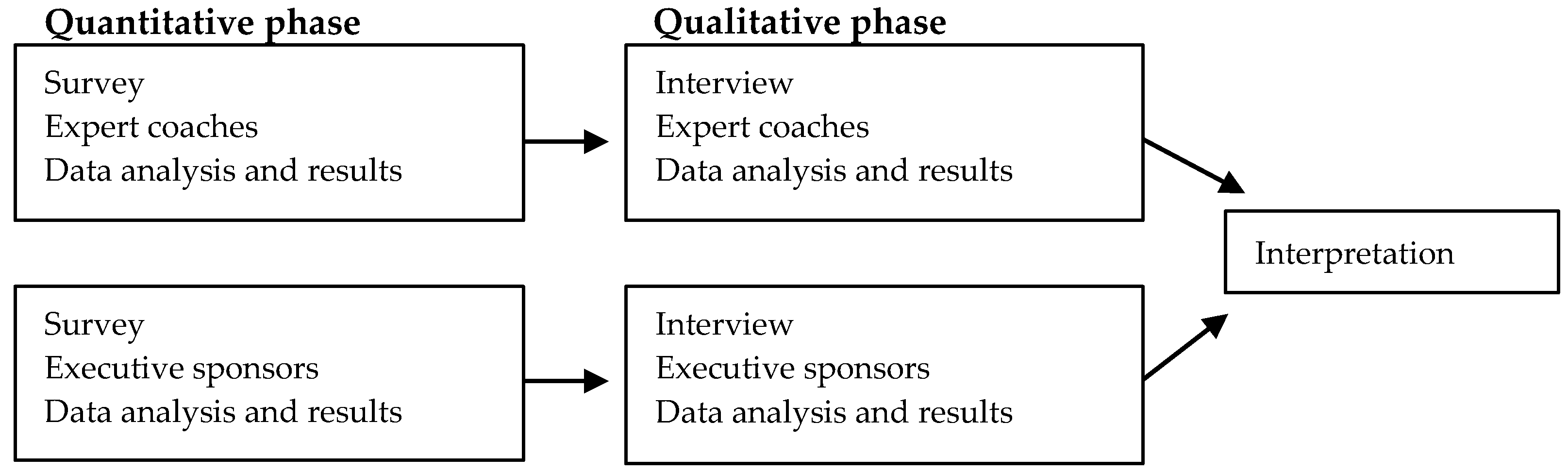
2.2. Study Design
2.3. Participants
2.4. Study Protocol
2.4.1. Surveys
2.4.2. Interviews
2.5. Analyses
3. Results
3.1. Quantitative Data—Expert Coach Online Survey
3.1.1. Overall Experience
- My ability as a coach has been enhanced by other development opportunities I’ve undertaken not necessarily as a result of the Redesign program. As expert coaches we are not ‘taught’ how to coach, and I know the standard and style of ‘coaching/mentoring’ differs greatly between one coach and another. There is also no oversight from the program as to the efficacy of coaching.
- In a rural LHD (Local Health District) face-to-face contact is more limited and this is affecting the type of support given.
- It would be great to have a toolbox to use for mentoring and coaching teams.
3.1.2. Organizational Support
- Sponsorship is a significant issue and ensuring teams have enough time to get outcomes is a constant battle. Aside from detailing up-front the time commitment from sponsors, and making the sponsorship capability development ‘more mandatory’…
- Redesign was well recognized by my Director; however, when the Director left the organization executive sponsorship was lost as the new Director supported [other]… initiatives.
- We have consistently told teams and their managers of the time commitment required and the need for backfill, but it is never forthcoming.
- Some sponsors are better prepared than others. Usually the sponsor gets better with repeat sponsor roles with a care focus. Ensuring team participants are released is still a struggle, as our sponsors are after faster, better, cheaper and don’t realize the effort required to make change stick.
3.2. Qualitative Data—Expert Coach Interviews
3.2.1. Theme 1: Structured Systems Facilitated Successful Outcomes
3.2.2. Theme 2: Focused Interaction Built Capacity
3.2.3. Theme 3: Coaching Required Managing Competing Priorities
3.2.4. Theme 4: Team Dynamics Influenced the Coaching Experiences
3.3. Quantitative Data—Executive Sponsor Online Survey
3.3.1. Overall Experience
3.3.2. Organizational Support
- It is probably the most worthwhile and useful program I’ve been involved in producing great change and sustainable change using great methodology and structure.
- Reduction in funding of departmental staff meant that the original program plans could not be fully implemented.
- The time commitment and requirements were intense.
- The challenge is back-fill. We freed up our staff which created a significant additional cost to the organization.
- Dysfunctional executive team… which undermined and did not support the service, therefore did not support the project team.
3.4. Qualitative Data—Executive Sponsor Interviews
3.4.1. Theme 1: Executive Sponsorship Was an Essential Role
3.4.2. Theme 2: Organizational Evolution Required Commitment from the Entire Team
3.4.3. Theme 3: Sponsors Became Emotionally Invested in the Projects and Teams
3.4.4. Theme 4: Sponsors Developed an Understanding of Topics
4. Discussion
4.1. Professional Development
4.2. Organizational Support and Investment
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Institute of Medicine. Measuring the Impact of Interprofessional Education on Collaborative Practice and Patient Outcomes; The National Academies Press: Washington, DC, USA, 2015; p. 182. [Google Scholar] [CrossRef]
- Shrank, W.H.; Rogstad, T.L.; Parekh, N. Waste in the US Health Care System: Estimated Costs and Potential for Savings. JAMA 2019. [Google Scholar] [CrossRef]
- Scott, I.A.; Duckett, S.J. In search of professional consensus in defining and reducing low-value care. Med. J. Aust. 2015, 203, 179–181. [Google Scholar] [CrossRef]
- Co, J.P. Educating for quality: Quality improvement as an activity of daily learning to improve educational and patient outcomes. Acad. Pediatr. 2014, 14, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Starr, S.R.; Kautz, J.M.; Sorita, A.; Thompson, K.M.; Reed, D.A.; Porter, B.L.; Mapes, D.L.; Roberts, C.C.; Kuo, D.; Bora, P.R.; et al. Quality Improvement Education for Health Professionals: A Systematic Review. Am. J. Med. Qual. 2015, 31, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, G.; Headrick, L.; Madigosky, W.; Ogrinc, G. Designing education to improve care. Jt. Comm. J. Qual. Patient Saf. 2012, 38, 5–14. [Google Scholar] [CrossRef]
- Bartlett, C.S.; Huerta, S.A. Creating change: An experiemental quality improvement and patient safety curriculum for medical students. MedEdPORTAL 2018, 14, 10660. [Google Scholar] [CrossRef]
- Earnest, M.; Brandt, B. Aligning practice redesign and interprofessional education to advance triple aim outcomes. J. Interprof. Care 2014, 28, 497–500. [Google Scholar] [CrossRef] [Green Version]
- Flynn, R.; Rotter, T.; Hartfield, D.; Newton, A.S.; Scott, S.D. A realist evaluation to identify contexts and mechanisms that enabled and hindered implementation and had an effect on sustainability of a lean intervention in pediatric healthcare. BMC Health Serv. Res. 2019, 19. [Google Scholar] [CrossRef]
- Konduri, N.; Rauscher, M.; Wang, S.C.J.; Malpica-Llanos, T. Individual capacity-building approaches in a global pharmaceutical systems strengthening program: A selected review. J. Pharm. Policy Pract. 2017, 10. [Google Scholar] [CrossRef] [Green Version]
- Melder, A.; Burns, P.; Mcloughlin, I.; Teede, H. Examining ‘institutional entrepreneurship’ in healthcare redesign and improvement through comparative case study research: A study protocol. BMJ Open 2018, 8, e020807. [Google Scholar] [CrossRef] [Green Version]
- Mintzberg, H. Structure in Fives: Designing Effective Organizations; Prentice-Hall, Inc.: Englewood Cliffs, NJ, USA, 1993; p. 312. [Google Scholar]
- Ham, C.; Kipping, R.; McLeod, H. Redesigning work processes in health care: Lessons from the National Health Service. Milbank Q. 2003, 81, 415–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, A.-C.; Fritzén, L.; Gäre, B.A. Pedagogical approaches in quality improvement coaching in healthcare: A Swedish case study of how improvement coaches approach learning in a contemporary healthcare system. Nord. J. Stud. Educ. Policy 2015, 2015, 30178. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.M.; Cohen, D.J.; Lin, A.; Augustine, J.; Handel, D.A.; Howell, E.; Kim, H.; Pines, J.M.; Schuur, J.D.; McConnell, K.J.; et al. Hospital Strategies for Reducing Emergency Department Crowding: A Mixed-Methods Study. Ann. Emerg. Med. 2018, 71, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Jeffs, L. Achieving the Quadruple Aim in Healthcare: The Essential Role of Authentic, Complex and Resilient Nurse Leaders. Nurs. Leadersh. (Toronto, Ont.) 2018, 31, 8–19. [Google Scholar] [CrossRef]
- Darker, C.D.; Nicolson, G.H.; Carroll, A.; Barry, J.M. The barriers and facilitators to the implementation of National Clinical Programmes in Ireland: Using the MRC framework for process evaluations 11 Medical and Health Sciences 1117 Public Health and Health Services. BMC Health Serv. Res. 2018, 18. [Google Scholar] [CrossRef]
- Kloppenborg, T.J.; Tesch, D.; Manolis, C. Project Success and Executive Sponsor Behaviors: Empirical Life Cycle Stage Investigations. Proj. Manag. J. 2014, 45, 9–20. [Google Scholar] [CrossRef]
- Gordon, M.; Darbyshire, D.; Baker, P. Non-technical skills training to enhance patient safety: A systematic review. Med. Educ. 2012, 46, 1042–1054. [Google Scholar] [CrossRef]
- Institute for Healthcare Improvement, IHI Triple Aim Initiative. Available online: http://www.ihi.org/Engage/Initiatives/TripleAim/Pages/default.aspx (accessed on 25 May 2020).
- Van Dam, P.J.; Griffin, P.; Reeves, N.S.; Prior, S.J.; Paton, B.; Verma, R.; Giles, A.; Kirkwood, L.; Peterson, G.M. Learning in Practice: Collaboration Is the Way to Improve Health System Outcomes. Healthcare 2019, 7, 90. [Google Scholar] [CrossRef] [Green Version]
- Silver, S.A.; Harel, Z.; McQuillan, R.; Weizman, A.V.; Thomas, A.; Chertow, G.M.; Nesrallah, G.; Bell, C.M.; Chan, C.T. How to Begin a Quality Improvement Project. Clin. J. Am. Soc. Nephrol. 2016, 11, 893–900. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.R. A General Inductive Approach for Analyzing Qualitative Evaluation Data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Brandrud, A.S.; Nyen, B.; Hjortdahl, P.; Sandvik, L.; Helljesen Haldorsen, G.S.; Bergli, M.; Nelson, E.C.; Bretthauer, M. Domains associated with successful quality improvement in healthcare—A nationwide case study. BMC Health Serv. Res. 2017, 17, 648. [Google Scholar] [CrossRef] [Green Version]
- Godfrey, M.M.; Andersson-Gare, B.; Nelson, E.C.; Nilsson, M.; Ahlstrom, G. Coaching interprofessional health care improvement teams: The coachee, the coach and the leader perspectives. J. Nurs. Manag. 2014, 22, 452–464. [Google Scholar] [CrossRef]
- Haugen, H.A.; Woodside, J. Beyond Implementation: A Prescription for Lasting EMR Adoption; Magnusson Skor Publishing: Denver, CO, USA, 2010. [Google Scholar]
- Kotecha, J.; Han, H.; Green, M.; Russell, G.; Martin, M.I.; Birtwhistle, R. The role of the practice facilitators in Ontario primary healthcare quality improvement. BMC Fam. Pract. 2015, 16, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stober, D.R.G.; Grant, A.M. Evidence Based Coaching Handbook: Putting Best Practices to Work for Your Clients; Stober, D.R.G., Grant, A.M., Eds.; Wiley: London, UK, 2006; p. 416. [Google Scholar]
- Harvey, G.; Lynch, E. Enabling Continuous Quality Improvement in Practice: The Role and Contribution of Facilitation. Front. Public Health 2017, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, T.; Fowler-Davis, S.; Nancarrow, S.; Ariss, S.M.B.; Enderby, P. Leadership in interprofessional health and social care teams: A literature review. Leadersh. Health Serv. 2018, 31, 452–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, L.; Galla, C. Building a culture of safety through team training and engagement. BMJ Qual. Saf. 2013, 22, 425–434. [Google Scholar] [CrossRef]
- Waring, J.J.; Bishop, S. Lean healthcare: Rhetoric, ritual and resistance. Soc. Sci. Med. 2010, 71, 1332–1340. [Google Scholar] [CrossRef]
- Bate, P.M.; Mendel, P.; Robert, G. Organizing for Quality: The Improvement Journeys of Leading Hospitals in Europe and the United States; Nuffield Trust: London, UK, 2008. [Google Scholar]
- James, V.; Rosenhead, R.; Taylor, P. Strategies for Project Sponsorship; Berrett-Koehler Publishers: San Francisco, CA, USA, 2013. [Google Scholar]
- Chandler, D.E.; Hall, P. Improving Executive Sponsorship of Projects: A Holistic Approach; Business Expert Press: New York, NY, USA, 2017. [Google Scholar]
- Hulscher, M.E.; Schouten, L.M.; Grol, R.P.; Buchan, H. Determinants of success of quality improvement collaboratives: What does the literature show? BMJ Qual. Saf. 2013, 22, 19–31. [Google Scholar] [CrossRef]
- Fischer, F.; Lange, K.; Klose, K.; Greiner, W.; Kraemer, A. Barriers and Strategies in Guideline Implementation—A Scoping Review. Healthcare (Basel) 2016, 4, 36. [Google Scholar] [CrossRef] [Green Version]
- Chandler, D.E.; Thomas, J.L. Does Executive Sponsorship Matter for Realizing Project Management Value? Proj. Manag. J. 2015, 46, 46–61. [Google Scholar] [CrossRef]
- Mery, G.; Dobrow, M.J.; Baker, G.R.; Im, J.; Brown, A. Evaluating investment in quality improvement capacity building: A systematic review. BMJ Open 2017, 7, e012431. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Group 1 | Group 2 |
|---|---|
| Expert Coaches | Executive Sponsors |
| (n = 28) | (n = 189) |
| As experts in the field, they provide mentoring and coaching to students (project teams), stakeholders, and executive sponsors such that the knowledge recipients can apply the redesign body of knowledge to their project work. They build and use local networks to influence project outcomes. Expert coaches may also teach face-to-face parts of the program, provide formative feedback on project deliverables, and contribute to course reviews and enhancements. | These are persons with high levels of influence within their organizations who are accountable for the project, securing any required resources, and helping to remove organizational barriers [22]. They govern the project direction and decisions, keep the project aligned with strategic aims, manage executive stakeholder relationships through mechanisms, such as steering committees, and manage escalated project risks and issues. |
| Statements | Strongly Agree | Slightly Agree | Neutral | Slightly Disagree | Strongly Disagree |
|---|---|---|---|---|---|
| The program has helped improve my own capacity to mentor others | 8 (53%) | 4 (27%) | 2 (13%) | 1 (7%) | 0 (0%) |
| I felt supported as a coach and mentor by the program facilitators | 8 (53%) | 7 (47%) | 0 (0%) | 0 (0%) | 0 (0%) |
| I felt supported as a coach by my organization | 6 (40%) | 7 (47%) | 2 (13%) | 0 (0%) | 0 (0%) |
| I had adequate resources available to effectively mentor team members | 7 (47%) | 6 (40%) | 2 (13%) | 0 (0%) | 0 (0%) |
| I felt the projects were well suited to the redesign methodology | 7 (47%) | 8 (53%) | 0 (0%) | 0 (0%) | 0 (0%) |
| I felt that team members appreciated my mentorship | 13 (87%) | 2 (13%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Statements | Strongly Agree | Slightly Agree | Neutral | Slightly Disagree | Strongly Disagree |
|---|---|---|---|---|---|
| The project/s was well aligned with local health service priorities | 9 (60%) | 6 (40%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Sponsors were well prepared for their role * | 4 (29%) | 5 (36%) | 2 (14%) | 2 (14%) | 1 (7%) |
| I felt that team members were well selected | 4 (27%) | 6 (40%) | 4 (27%) | 1 (7%) | 0 (0%) |
| I was able to negotiate the resources my team/s required for their project/s | 3 (20%) | 9 (60%) | 1 (7%) | 2 (13%) | 0 (0%) |
| The team/s were provided with sufficient quarantined time to conduct their project/s | 3 (20%) | 4 (27%) | 4 (27%) | 4 (27%) | 0 (0%) |
| I was provided with enough time to mentor and guide project teams | 6 (40%) | 7 (47%) | 1 (7%) | 1 (7%) | 0 (0%) |
| My organization values the redesign program | 8 (53%) | 5 (33%) | 1 (7%) | 1 (7%) | 0 (0%) |
| My organization recognized my team/s achievements | 6 (40%) | 5 (33%) | 3 (20%) | 1 (7%) | 0 (0%) |
| Major Theme | Sub-Theme(s) | Quotes |
|---|---|---|
| Coaching success is dependent on the structure |
| “Setting the stage before each project is important” “My role is around making sure people have skills in project management and improvement methodologies” “Trying to articulate where I fit in is a challenge” |
| Focused interaction builds capacity |
| “Negotiating with managers on an ongoing basis can be challenging” “I’ve got my network outside of here which is really valuable” “It’s more than mentoring… it’s about getting your hand dirty, actually get in and do it with them” “People learn more from each other” |
| Coaching demands a shift in priorities |
| “A challenge as coaches is just keeping up” “Some sponsors want what they want…it affects the morale of the team” “Capacity waxes and wanes” |
| Team dynamics influence coaching experiences |
| “Different skill sets and different levels of knowledge…frustration comes out” “I feel really valuable” “I don’t like to tell people what to do…I like a hovering approach” |
| Statements | Yes Responses n (%) |
|---|---|
| I felt supported as a sponsor by program facilitators | 21 (58%) |
| I felt supported as a sponsor by my organization | 13 (36%) |
| I had adequate resources available to effectively sponsor team members | 10 (28%) |
| I felt the projects were suitable for the program | 29 (81%) |
| I felt that projects generally aligned with organizational goals | 25 (69%) |
| I felt that team members appreciated my sponsorship | 25 (69%) |
| My work as a team sponsor was recognized | 10 (28%) |
| My expectations of sponsoring project teams were met | 15 (42%) |
| Statements | Strongly Agree | Slightly Agree | Neutral | Slightly Disagree | Strongly Disagree |
|---|---|---|---|---|---|
| The project/s was well aligned with local health service priorities | 29 (78%) | 6 (16%) | 2 (5%) | 0 (0%) | 0 (0%) |
| Redesign leads (expert coaches) mentored the project teams well | 29 (78%) | 6 (16%) | 2 (5%) | 0 (0%) | 0 (0%) |
| The right team members were well selected | 24 (65%) | 8 (22%) | 4 (11%) | 0 (0%) | 1 (3%) |
| I was able to negotiate the resources my team/s required for their project/s | 15 (41%) | 15 (41%) | 3 (8%) | 3 (8%) | 1 (3%) |
| The team/s were provided with sufficient quarantined time to conduct their project/s | 18 (49%) | 12 (32%) | 2 (5%) | 5 (13%) | 0 (0%) |
| I could find enough time to effectively sponsor project teams | 8 (22%) | 20 (54%) | 2 (5%) | 5 (13%) | 2 (5%) |
| My organization values the redesign program | 22 (59%) | 9 (24%) | 5 (13%) | 1 (3%) | 0 (0%) |
| My organization recognized my team/s’ achievements | 19 (51%) | 14 (38%) | 2 (5%) | 1 (3%) | 1 (3%) |
| Major Theme | Sub-Theme(s) | Quotes |
|---|---|---|
| Executive sponsorship is an essential role |
| “The role of a sponsor should be crystal clear” “The volume of work was daunting—Only negative” “It gives liberty to the project and …students enjoy having that additional contact where they probably wouldn’t have that in their current role” “You (sponsors) can never have enough training and support” |
| Organizational evolution requires commitment from the entire team |
| “Sponsors are for risk management” “Teams get a sponsor… It’s a positive way to make change” “We’re still reaping the benefits” |
| Sponsors become emotionally invested in projects and teams |
| “I had to be aware of the workload of the students and the stress that they were under” “It’s a massive amount of travel for students…up to 8 h just to get to an airport to attend face-to-face days” “Unless someone is monitoring it all the time…it loses a lot of its impact” “It’s frustrating and energy sapping…you’ve seen it all before” |
| Projects provide sponsors with opportunities to develop specific content knowledge |
| “It was very beneficial for me, to get a handle of the health and complex care needs of the community” “The beauty of what we did…what we can do with existing software” “It was very educational for me at the beginning…the whole integrated care space” |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Dam, P.J.; Griffin, P.; Peterson, G.M.; Reeves, N.S.; Kirkwood, L.; Prior, S.J. Organizational Support in Healthcare Redesign Education: A Mixed-Methods Exploratory Study of Expert Coach and Executive Sponsor Experiences. Int. J. Environ. Res. Public Health 2020, 17, 5308. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155308
Van Dam PJ, Griffin P, Peterson GM, Reeves NS, Kirkwood L, Prior SJ. Organizational Support in Healthcare Redesign Education: A Mixed-Methods Exploratory Study of Expert Coach and Executive Sponsor Experiences. International Journal of Environmental Research and Public Health. 2020; 17(15):5308. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155308
Chicago/Turabian StyleVan Dam, Pieter J., Phoebe Griffin, Gregory M. Peterson, Nicole S. Reeves, Lea Kirkwood, and Sarah J. Prior. 2020. "Organizational Support in Healthcare Redesign Education: A Mixed-Methods Exploratory Study of Expert Coach and Executive Sponsor Experiences" International Journal of Environmental Research and Public Health 17, no. 15: 5308. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155308