Correlation of Mortality Burdens of Cerebrovascular Disease and Diabetes Mellitus with Domestic Consumption of Soya and Palm Oils

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Selection Criteria
2.3. Calculations
2.3.1. Standardization of Data
2.3.2. Percentage Changes
- (1) The formula to calculate the percentage change of mortality burden of a disease or food-use consumption of oils between 2005 and 2010.
- (2) The formula to calculate the percentage change of mortality burden of a disease or food-use consumption of oils between 2010 and 2016.
2.4. Statistical Analysis
3. Results
3.1. Trends of Change in Mortality Burdens of CBVDs and DM Against Food-Use Consumption of Oils with Time
3.1.1. The Trend of Changes in the Mortality Burden and Food-Use Consumption of Oils in the 11 Countries by Time
3.1.2. The Trend of Changes in the Mortality Burden and Food-Use Consumption of Oils in the 11 Countries by Country Strata
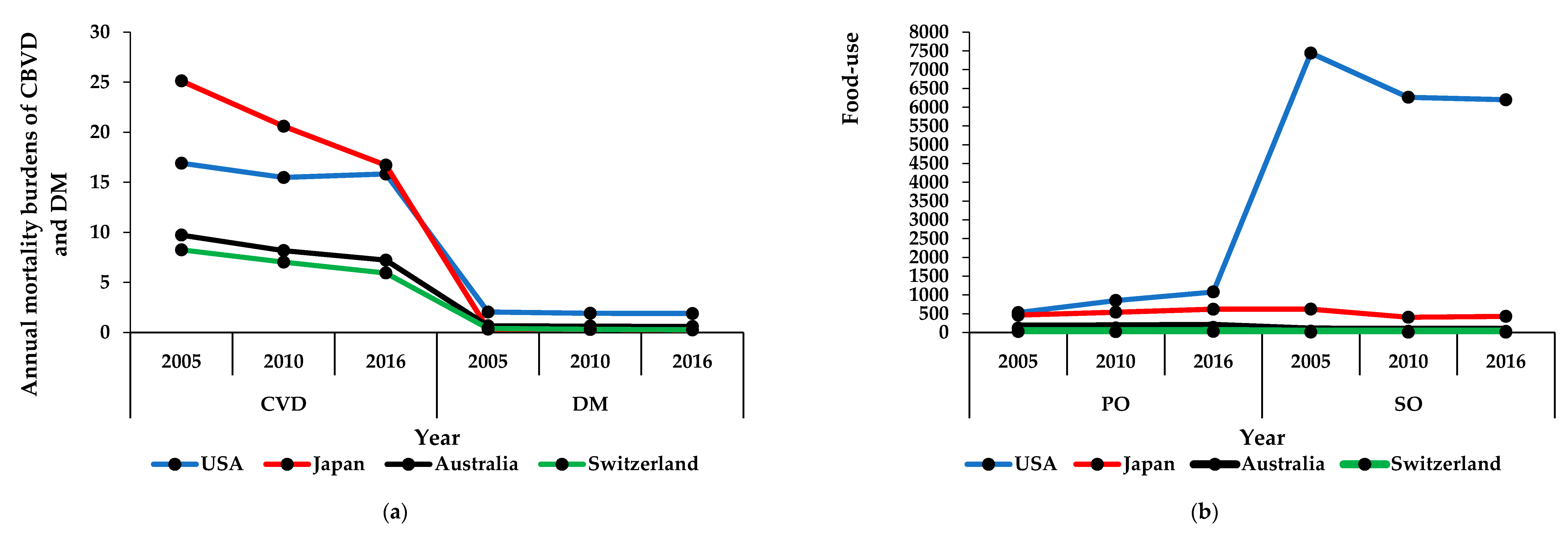
In High-Income Countries
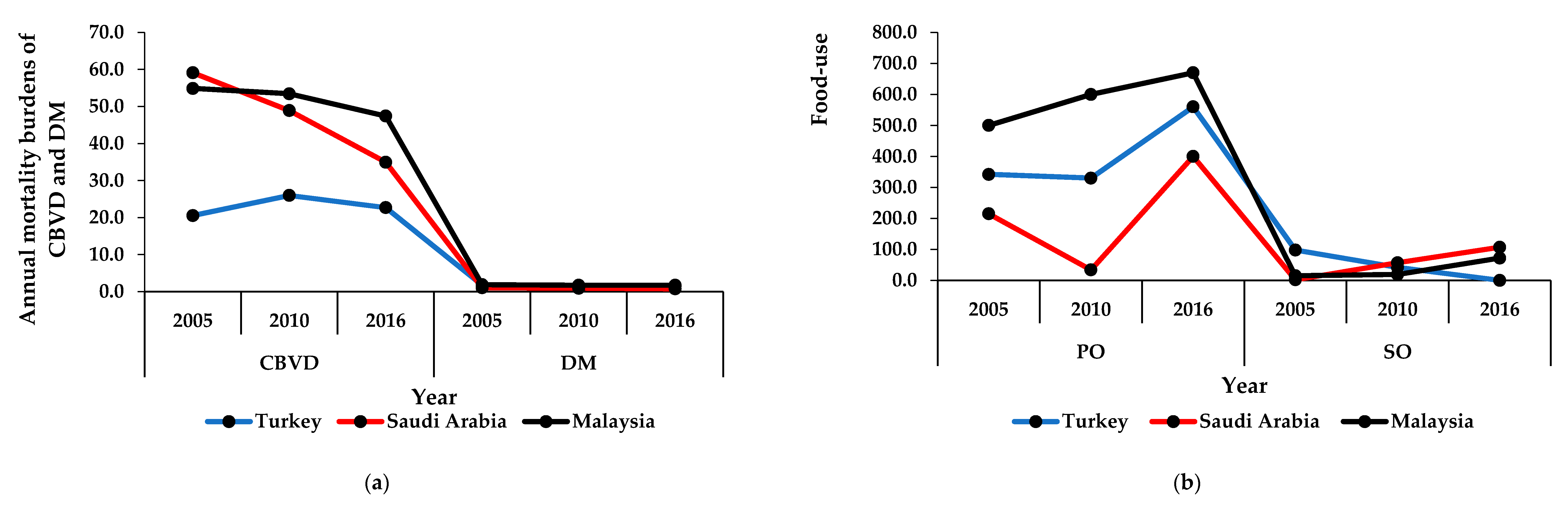
In High Middle-Income Countries
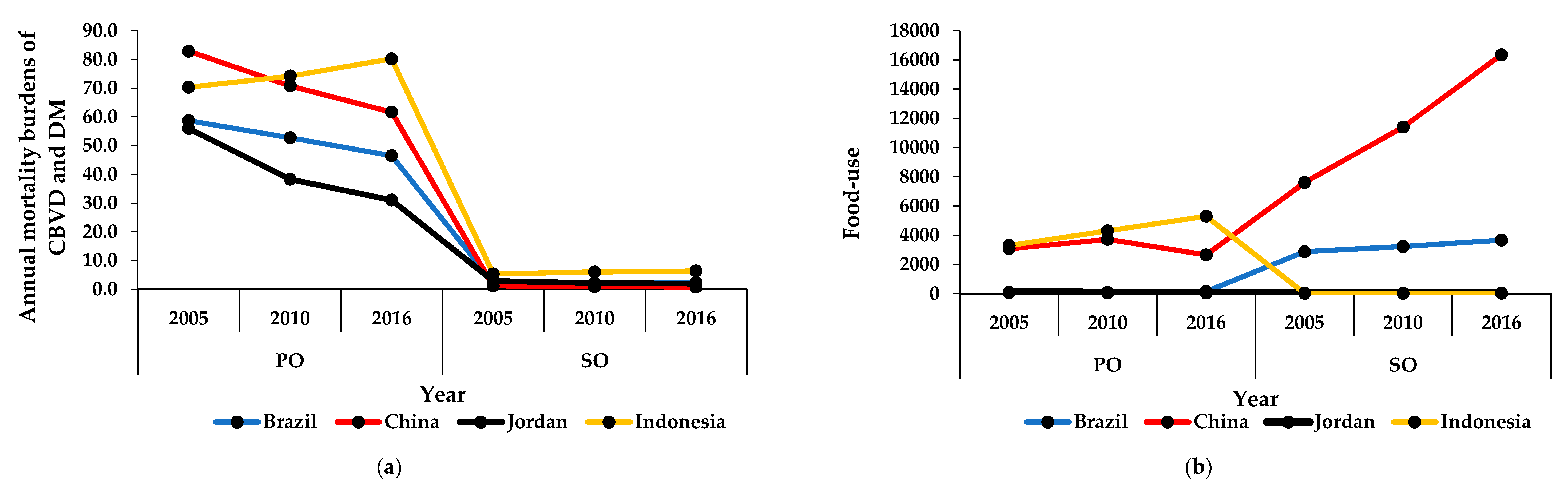
In Middle-Income Countries
3.2. Correlation of Mortality Burdens of Cerebrovascular Diseases or Consumption of Oils with Time
3.2.1. In High-Income Countries
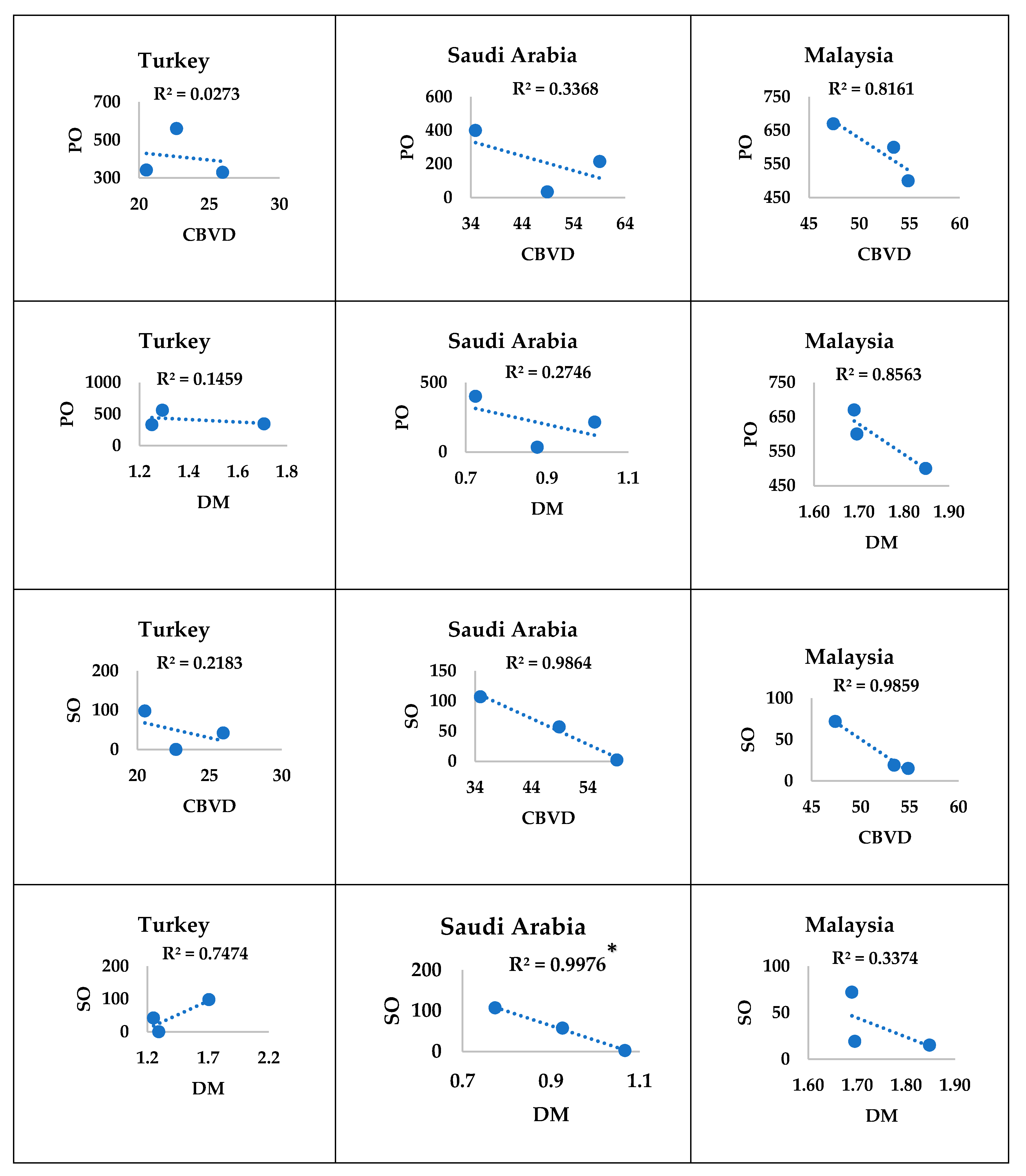
3.2.2. In High Middle-Income Countries
3.2.3. In Middle-Income Countries
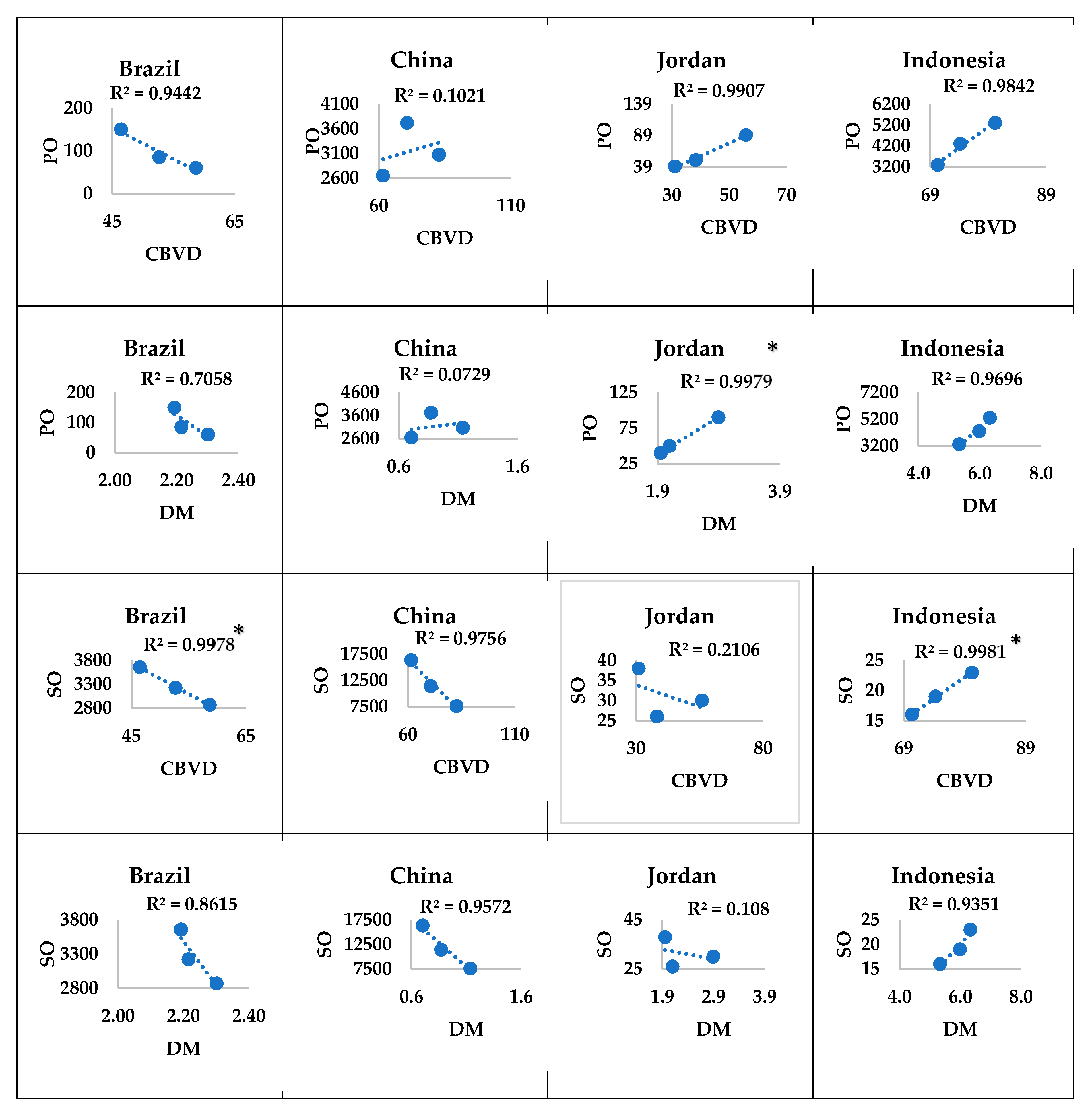
3.3. Correlation between Consumption of Oils and Mortality Burdens of Diseases
3.3.1. In High-Income Countries
3.3.2. In High Middle-Income Countries
3.3.3. In Middle-Income Countries
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gorelick, P.B. Cerebrovascular disease. Pathophysiology and diagnosis. Nurs. Clin. N. Am 1986, 21, 275–288. [Google Scholar]
- Hedges, D.; Farrer, T.J.; Bigler, E.D.; Hopkins, R.O. Cerebrovascular Disease and Cognition. In The Brain at Risk; Springer: Berlin/Heidelberg, Germany, 2019; pp. 85–99. [Google Scholar]
- Perneczky, R.; Tene, O.; Attems, J.; Giannakopoulos, P.; Ikram, M.A.; Federico, A.; Sarazin, M.; Middleton, L.T. Is the time ripe for new diagnostic criteria of cognitive impairment due to cerebrovascular disease? Consensus report of the International Congress on Vascular Dementia working group. BMC Med. 2016, 14, 162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, R.; Wilkins, E.; Nichols, M.; Kelly, P.; El-Sadi, F.; Wright, F.L.; Townsend, N. Epidemiology report: Trends in sex-specific cerebrovascular disease mortality in Europe based on WHO mortality data. Eur. Heart J. 2019, 40, 755–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, L.B. Epidemiology of Cerebrovascular Disease. In Vascular Medicine: A Companion to Braunwald’s Heart Disease E-Book; Elsevier: Amsterdam, The Netherlands, 2019; p. 361. [Google Scholar]
- Tong, X.; Yang, Q.; Ritchey, M.D.; George, M.G.; Jackson, S.L.; Gillespie, C.; Merritt, R.K. The Burden of Cerebrovascular Disease in the United States. Prev. Chronic Dis. 2019, 16, E52. [Google Scholar] [CrossRef] [Green Version]
- Imura, H.; Maruyama, Y.; Amitani, R.; Maeda, M.; Shirakawa, M.; Nitta, T. Long-term impact of critical silent cerebrovascular disease in patients undergoing coronary artery bypass surgery: A propensity score and multivariate analyses. Perfusion 2019, 34, 147–153. [Google Scholar] [CrossRef]
- Portegies, M.L.; Koudstaal, P.J.; Ikram, M.A. Cerebrovascular disease. Handb. Clin. Neurol 2016, 138, 239–261. [Google Scholar] [CrossRef] [Green Version]
- Kaewput, W.; Thongprayoon, C.; Varothai, N.; Sirirungreung, A.; Rangsin, R.; Bathini, T.; Mao, M.A.; Cheungpasitporn, W. Prevalence and associated factors of hospitalization for dysglycemia among elderly type 2 diabetes patients: A nationwide study. World J. Diabetes 2019, 10, 212–223. [Google Scholar] [CrossRef]
- Shuja, M.; Mittal, S.; Zaman, M. Effective Prediction of Type II Diabetes Mellitus Using Data Mining Classifiers and SMOTE. In Advances in Computing and Intelligent Systems; Springer: Berlin/Heidelberg, Germany, 2020; pp. 195–211. [Google Scholar]
- Viigimaa, M.; Sachinidis, A.; Toumpourleka, M.; Koutsampasopoulos, K.; Alliksoo, S.; Titma, T. Macrovascular complications of type 2 diabetes mellitus. Curr. Vasc. Pharmacol. 2020, 18, 110–116. [Google Scholar] [CrossRef]
- Peng, X.; Wang, X.; Fan, M.; Zhao, J.; Lin, L.; Liu, J. Plasma levels of von Willebrand factor in type 2 diabetes patients with and without cardiovascular diseases: A meta-analysis. Diabetes/Metab. Res. Rev. 2020, 36, e3193. [Google Scholar] [CrossRef]
- Hartley, A.; Marshall, D.C.; Salciccioli, J.D.; Sikkel, M.B.; Maruthappu, M.; Shalhoub, J. Trends in mortality from ischemic heart disease and cerebrovascular disease in Europe: 1980 to 2009. Circulation 2016, 133, 1916–1926. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.E.; Saposnik, G.; Biessels, G.J.; Doubal, F.N.; Fornage, M.; Gorelick, P.B.; Greenberg, S.M.; Higashida, R.T.; Kasner, S.E.; Seshadri, S. Prevention of stroke in patients with silent cerebrovascular disease: A scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2017, 48, e44–e71. [Google Scholar] [CrossRef] [PubMed]
- Paradise, M.B.; Shepherd, C.E.; Wen, W.; Sachdev, P.S. Neuroimaging and neuropathology indices of cerebrovascular disease burden: A systematic review. Neurology 2018, 91, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Santé, O.M.D.L. World Health Statistics 2018: Monitoring Health for the SDGs Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Bruins, M.J.; Van Dael, P.; Eggersdorfer, M. The role of nutrients in reducing the risk for noncommunicable diseases during aging. Nutrients 2019, 11, 85. [Google Scholar] [CrossRef] [PubMed]
- Troesch, B.; Biesalski, H.K.; Bos, R.; Buskens, E.; Calder, P.C.; Saris, W.H.; Spieldenner, J.; Verkade, H.J.; Weber, P.; Eggersdorfer, M. Increased intake of foods with high nutrient density can help to break the intergenerational cycle of malnutrition and obesity. Nutrients 2015, 7, 6016–6037. [Google Scholar] [CrossRef] [Green Version]
- Ismail, S.R.; Maarof, S.K.; Siedar Ali, S.; Ali, A. Systematic review of palm oil consumption and the risk of cardiovascular disease. PLoS ONE 2018, 13, e0193533. [Google Scholar] [CrossRef]
- Chen, B.K.; Seligman, B.; Farquhar, J.W.; Goldhaber-Fiebert, J.D. Multi-Country analysis of palm oil consumption and cardiovascular disease mortality for countries at different stages of economic development: 1980–1997. Glob. Health 2011, 7, 45. [Google Scholar] [CrossRef] [Green Version]
- Ismail, M.; Alsalahi, A.; Imam, M.U.; Ooi, D.J.; Khaza’ai, H.; Aljaberi, M.A.; Shamsudin, M.N.; Idrus, Z. Safety and Neuroprotective Efficacy of Palm Oil and Tocotrienol-Rich Fraction from Palm Oil: A Systematic Review. Nutrients 2020, 12, 521. [Google Scholar] [CrossRef] [Green Version]
- Keogh-Brown, M.R.; Jensen, H.T.; Basu, S.; Aekplakorn, W.; Cuevas, S.; Dangour, A.D.; Gheewala, S.H.; Green, R.; Joy, E.J.; Rojroongwasinkul, N. Evidence on the magnitude of the economic, health and population effects of palm cooking oil consumption: An integrated modelling approach with Thailand as a case study. Popul. Health Metr. 2019, 17, 12. [Google Scholar] [CrossRef] [Green Version]
- Moundi, I. International Commodity and Consumption Information as Compiled by the United States Department of Agricultur. 2019. Available online: https://www.indexmundi.com/agriculture/?commodity=palm-oil&graph=domestic-consumption (accessed on 22 June 2020).
- Network, G.B.O.D.C. Global Burden of Disease Study 2016 (GBD 2016) Healthcare Access and Quality Index Based on Amenable Mortality 1990–2016; Institute for Health Metrics and Evaluation (IHME): Seattle, WA, USA, 2018. [Google Scholar]
- World Health Organization. Age-standardized Death Rates per 100,000 by Cause. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/78 (accessed on 22 June 2020).
- Drye, E.E.; Normand, S.-L.T.; Wang, Y.; Ross, J.S.; Schreiner, G.C.; Han, L.; Rapp, M.; Krumholz, H.M. Comparison of hospital risk-standardized mortality rates calculated by using in-hospital and 30-day models: An observational study with implications for hospital profiling. Ann. Intern. Med. 2012, 156, 19–26. [Google Scholar] [CrossRef]
- Investopedia. Available online: https://www.investopedia.com/terms/p/percentage-change.asp (accessed on 22 June 2020).
- Abner, E.L.; Nelson, P.T.; Kryscio, R.J.; Schmitt, F.A.; Fardo, D.W.; Woltjer, R.L.; Cairns, N.J.; Yu, L.; Dodge, H.H.; Xiong, C.; et al. Diabetes is associated with cerebrovascular but not Alzheimer’s disease neuropathology. Alzheimer’s Dement. 2016, 12, 882–889. [Google Scholar] [CrossRef] [Green Version]
- Beaglehole, R.; Epping-Jordan, J.; Patel, V.; Chopra, M.; Ebrahim, S.; Kidd, M.; Haines, A. Improving the prevention and management of chronic disease in low-income and middle-income countries: A priority for primary health care. Lancet 2008, 372, 940–949. [Google Scholar] [CrossRef]
- Barthel, M.; Jennings, S.; Schreiber, W.; Sheane, R.; Royston, S.; Fry, J.; Khor, Y.; McGill, J. Study on the environmental impact of palm oil consumption and on existing sustainability standards. In Directorate-General for Environment; European Commission: Brussels, Belgium, 2018. [Google Scholar]
- Choi, J.Y.; Morris, J.C.; Hsu, C.Y. Aging and Cerebrovascular Disease. Neurol. Clin. 1998, 16, 687–711. [Google Scholar] [CrossRef]
- Goto, A.; Takao, T.; Yoshida, Y.; Kawazu, S.; Iwamoto, Y.; Terauchi, Y. Causes of death and estimated life expectancy among people with diabetes: A retrospective cohort study in a diabetes clinic. J. Diabetes Investig. 2020, 11, 52–54. [Google Scholar] [CrossRef] [Green Version]
- Satman, I.; Yilmaz, T.; Sengül, A.; Salman, S.; Salman, F.; Uygur, S.; Bastar, I.; Tütüncü, Y.; Sargin, M.; Dinççag, N. Population-based study of diabetes and risk characteristics in Turkey: Results of the turkish diabetes epidemiology study (TURDEP). Diabetes Care 2002, 25, 1551–1556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akinci, F.; Yildirim, A.; Gözü, H.; Sargın, H.; Orbay, E.; Sargın, M. Assessment of health-related quality of life (HRQoL) of patients with type 2 diabetes in Turkey. Diabetes Res. Clin. Pract. 2008, 79, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Sozmen, K.; Unal, B.; Capewell, S.; Critchley, J.; O’Flaherty, M. Estimating diabetes prevalence in Turkey in 2025 with and without possible interventions to reduce obesity and smoking prevalence, using a modelling approach. Int. J. Public Health 2015, 60, 13–21. [Google Scholar] [CrossRef]
- Choudhary, M.; Grover, K. Palm (Elaeis guineensis Jacq.) Oil. In Fruit Oils: Chemistry and Functionality; Springer: Berlin/Heidelberg, Germany, 2019; pp. 789–802. [Google Scholar]
- Noh, K.M. Primary health care reform in 1CARE for 1 Malaysia. Int. J. Public Health Res. Spec. Issue 2011 2011, 2011, 50–56. [Google Scholar]
- Alzaied, T.A.M.; Alshammari, A. An evaluation of primary healthcare centers (PHC) services: The views of users. Health Sci. J. 2016, 10, 1. [Google Scholar]
- Al Asmri, M.; Almalki, M.J.; Fitzgerald, G.; Clark, M. The public healthcare system and primary care services in Saudi Arabia: A system in transition. East. Mediterr. Health J. 2019, in press. [Google Scholar] [CrossRef]
- Kilic, B.; Kalaca, S.; Unal, B.; Phillimore, P.; Zaman, S. Health policy analysis for prevention and control of cardiovascular diseases and diabetes mellitus in Turkey. Int. J. Public Health 2015, 60, 47–53. [Google Scholar] [CrossRef]
- Ho, B.K.; Jasvindar, K.; Gurpreet, K.; Ambigga, D.; Suthahar, A.; Cheong, S.M.; Lim, K.H. Prevalence, awareness, treatment and control of diabetes mellitus among the elderly: The 2011 National Health and Morbidity Survey, Malaysia. Malays. Fam. Physician Off. J. Acad. Fam. Physicians Malays. 2014, 9, 12–19. [Google Scholar]
- Macinko, J.; Starfield, B.; Erinosho, T. The Impact of Primary Healthcare on Population Health in Low-and Middle-Income Countries. J. Ambul. Care Manag. 2009, 32, 150–171. [Google Scholar] [CrossRef] [PubMed]
- Schroders, J.; Wall, S.; Hakimi, M.; Dewi, F.S.T.; Weinehall, L.; Nichter, M.; Nilsson, M.; Kusnanto, H.; Rahajeng, E.; Ng, N. How is Indonesia coping with its epidemic of chronic noncommunicable diseases? A systematic review with meta-analysis. PLoS ONE 2017, 12, e0179186. [Google Scholar] [CrossRef] [PubMed]
- McNamara, D.J. Palm Oil and Health: A Case of Manipulated Perception and Misuse of Science. J. Am. Coll. Nutr. 2010, 29, 240S–244S. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| USA | Japan | Australia | Switzerland | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2005 | 2010 | 2016 | 2005 | 2010 | 2016 | 2005 | 2010 | 2016 | 2005 | 2010 | 2016 | |
| CBVD | 16.91 | 15.48 | 15.83 | 25.13 | 20.60 | 16.71 | 9.73 | 8.18 | 7.23 | 8.26 | 7.03 | 5.94 |
| DM | 2.05 | 1.91 | 1.90 | 0.34 | 0.30 | 0.25 | 0.67 | 0.64 | 0.60 | 0.41 | 0.32 | 0.27 |
| PO | 531.00 | 852.00 | 1080.00 | 464.00 | 539.00 | 620.00 | 117.00 | 120.00 | 135.00 | 25.00 | 22.00 | 29.00 |
| SO | 7441.00 | 6264.00 | 6198.00 | 621.00 | 407.00 | 430.00 | 34.00 | 31.00 | 29.00 | 10.00 | 9.00 | 8.00 |
| Turkey | Saudi Arabia | Malaysia | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 2005 | 2010 | 2016 | 2005 | 2010 | 2016 | 2005 | 2010 | 2016 | |
| CBVD | 20.52 | 25.96 | 22.67 | 59.11 | 48.89 | 34.94 | 54.86 | 53.43 | 47.42 |
| DM | 1.71 | 1.25 | 1.29 | 1.02 | 0.88 | 0.72 | 1.85 | 1.70 | 1.69 |
| PO | 342.00 | 330.00 | 560.00 | 215.00 | 34.00 | 400.00 | 500.00 | 600.00 | 670.00 |
| SO | 98.00 | 42.00 | 0.00 | 2.00 | 57.00 | 107.00 | 15.00 | 19.00 | 72.00 |
| Brazil | China | Jordan | Indonesia | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2005 | 2010 | 2016 | 2005 | 2010 | 2016 | 2005 | 2010 | 2016 | 2005 | 2010 | 2016 | |
| CBVD | 58.67 | 52.70 | 46.47 | 82.82 | 70.75 | 61.64 | 55.95 | 38.28 | 31.03 | 70.33 | 74.18 | 80.21 |
| DM | 2.30 | 2.22 | 2.19 | 1.14 | 0.87 | 0.71 | 2.89 | 2.10 | 1.95 | 5.33 | 5.98 | 6.33 |
| PO | 60.00 | 85.00 | 150.00 | 3074.00 | 3717.00 | 2650.00 | 90.00 | 50.00 | 40.00 | 3300.00 | 4300.00 | 5300.00 |
| SO | 2871.00 | 3225.00 | 3660.00 | 7607.00 | 11400.00 | 16350.00 | 30.00 | 26.00 | 38.00 | 16.00 | 19.00 | 23.00 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ismail, M.; Alsalahi, A.; Khaza’ai, H.; Imam, M.U.; Ooi, D.J.; Samsudin, M.N.; Idrus, Z.; Sokhini, M.H.M.; A. Aljaberi, M. Correlation of Mortality Burdens of Cerebrovascular Disease and Diabetes Mellitus with Domestic Consumption of Soya and Palm Oils. Int. J. Environ. Res. Public Health 2020, 17, 5410. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155410
Ismail M, Alsalahi A, Khaza’ai H, Imam MU, Ooi DJ, Samsudin MN, Idrus Z, Sokhini MHM, A. Aljaberi M. Correlation of Mortality Burdens of Cerebrovascular Disease and Diabetes Mellitus with Domestic Consumption of Soya and Palm Oils. International Journal of Environmental Research and Public Health. 2020; 17(15):5410. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155410
Chicago/Turabian StyleIsmail, Maznah, Abdulsamad Alsalahi, Huzwah Khaza’ai, Mustapha Umar Imam, Der Jiun Ooi, Mad Nasir Samsudin, Zulkifli Idrus, Muhammed Ha’iz Mohd Sokhini, and Musheer A. Aljaberi. 2020. "Correlation of Mortality Burdens of Cerebrovascular Disease and Diabetes Mellitus with Domestic Consumption of Soya and Palm Oils" International Journal of Environmental Research and Public Health 17, no. 15: 5410. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155410