Bibliometric Analysis of Chronic Traumatic Encephalopathy Research from 1999 to 2019

Abstract
:1. Introduction
2. Materials and Methods
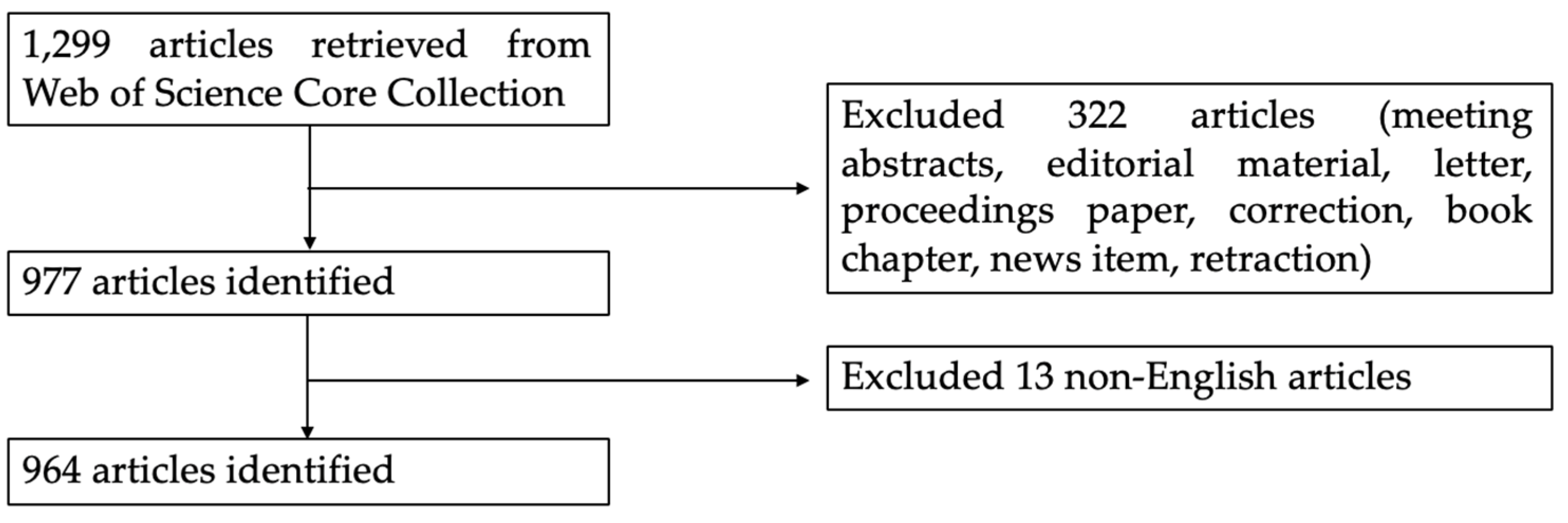
2.1. Data Collection
2.2. Data Analysis
3. Results
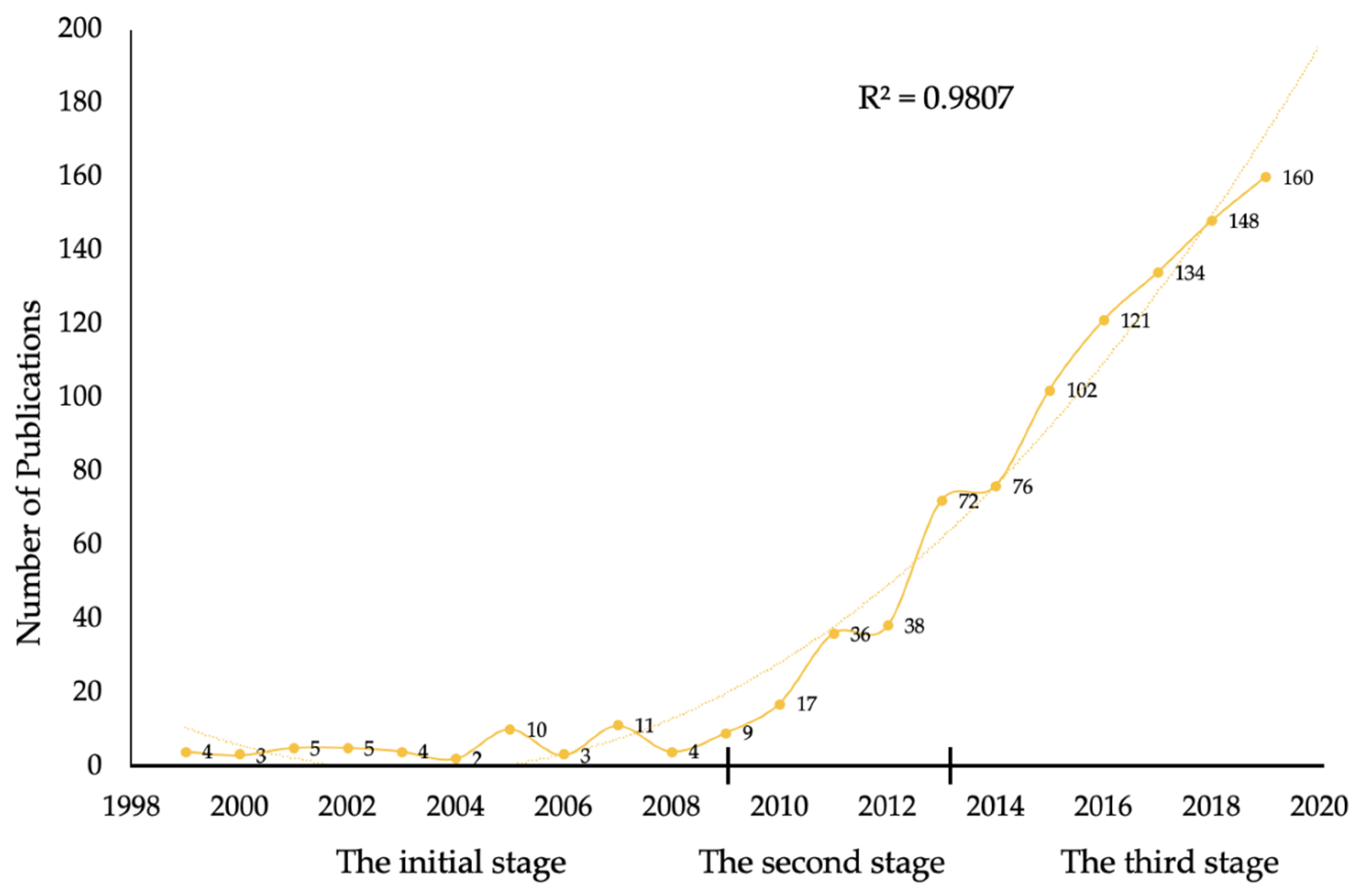
3.1. Publication Outputs and Development Trend
3.2. Analysis of Countries and Institutions
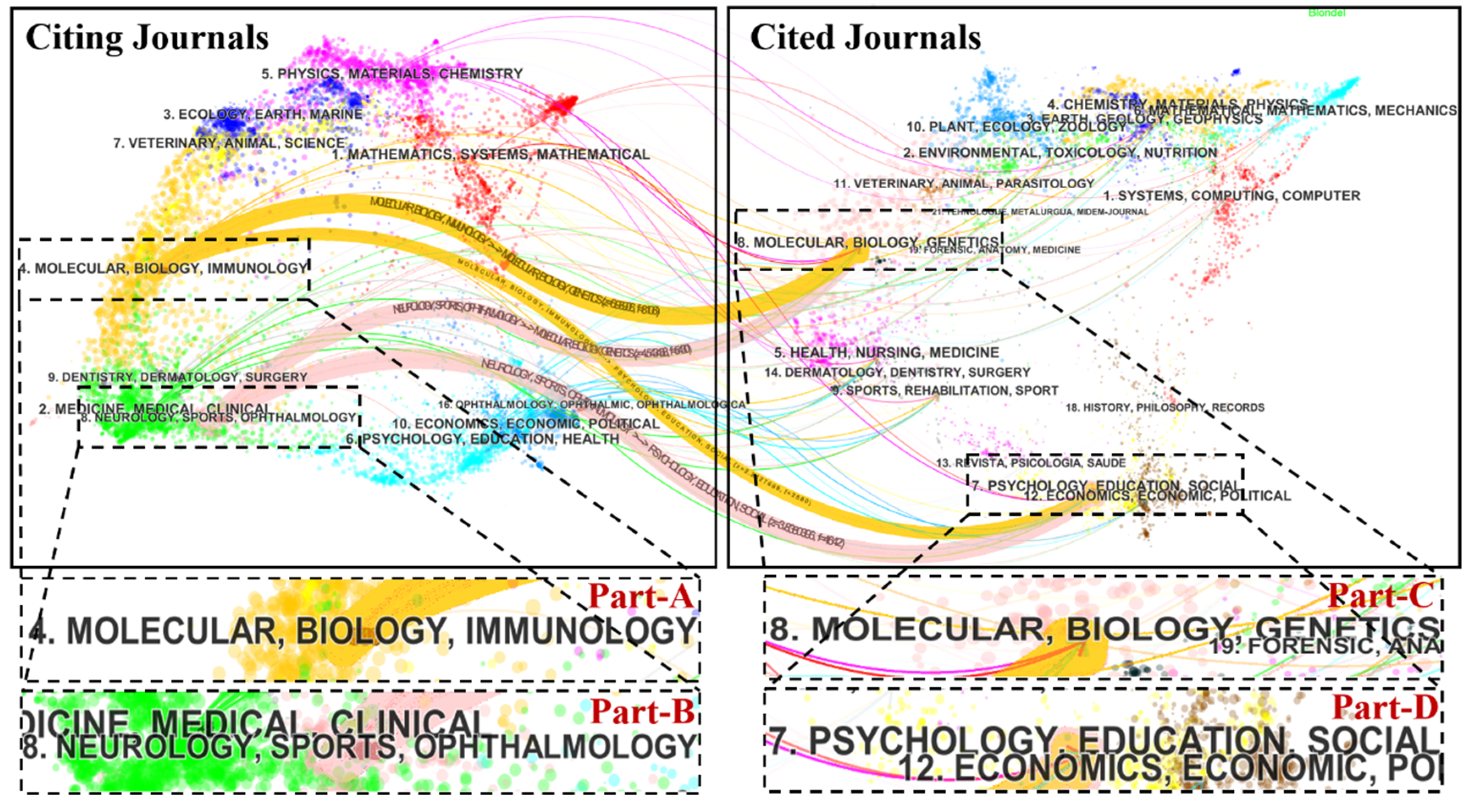
3.3. Journal Analysis
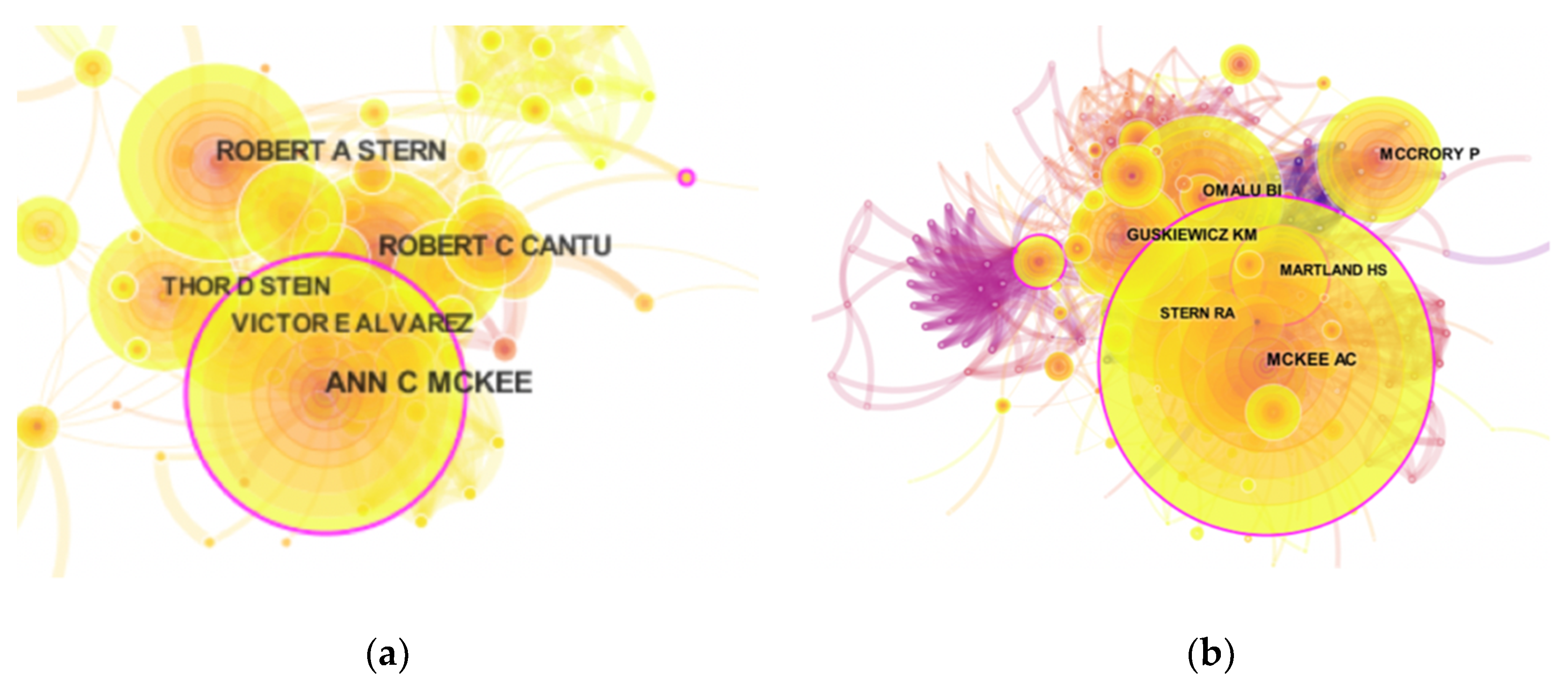
3.4. Analysis of Authors and Co-cited Authors
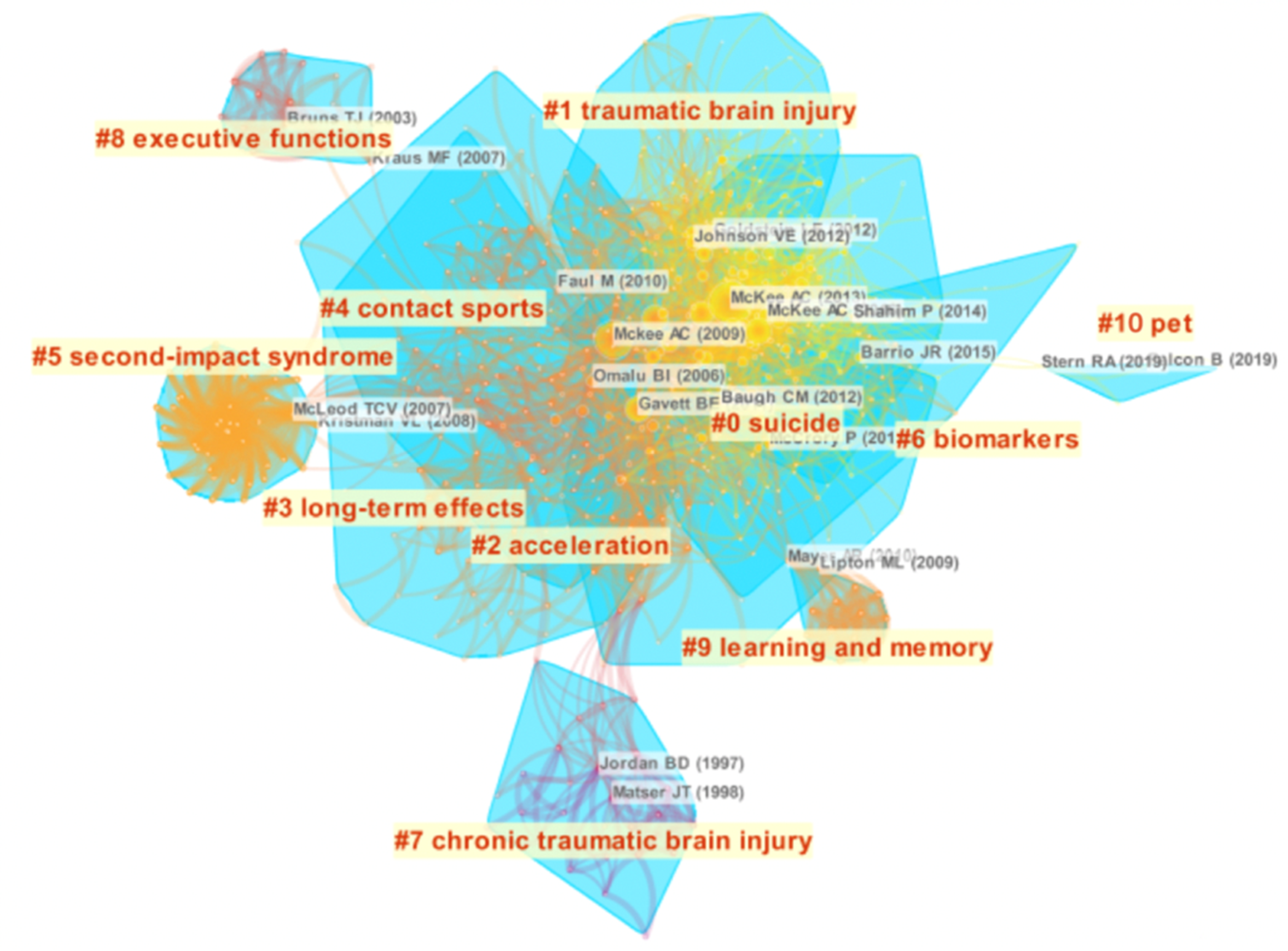
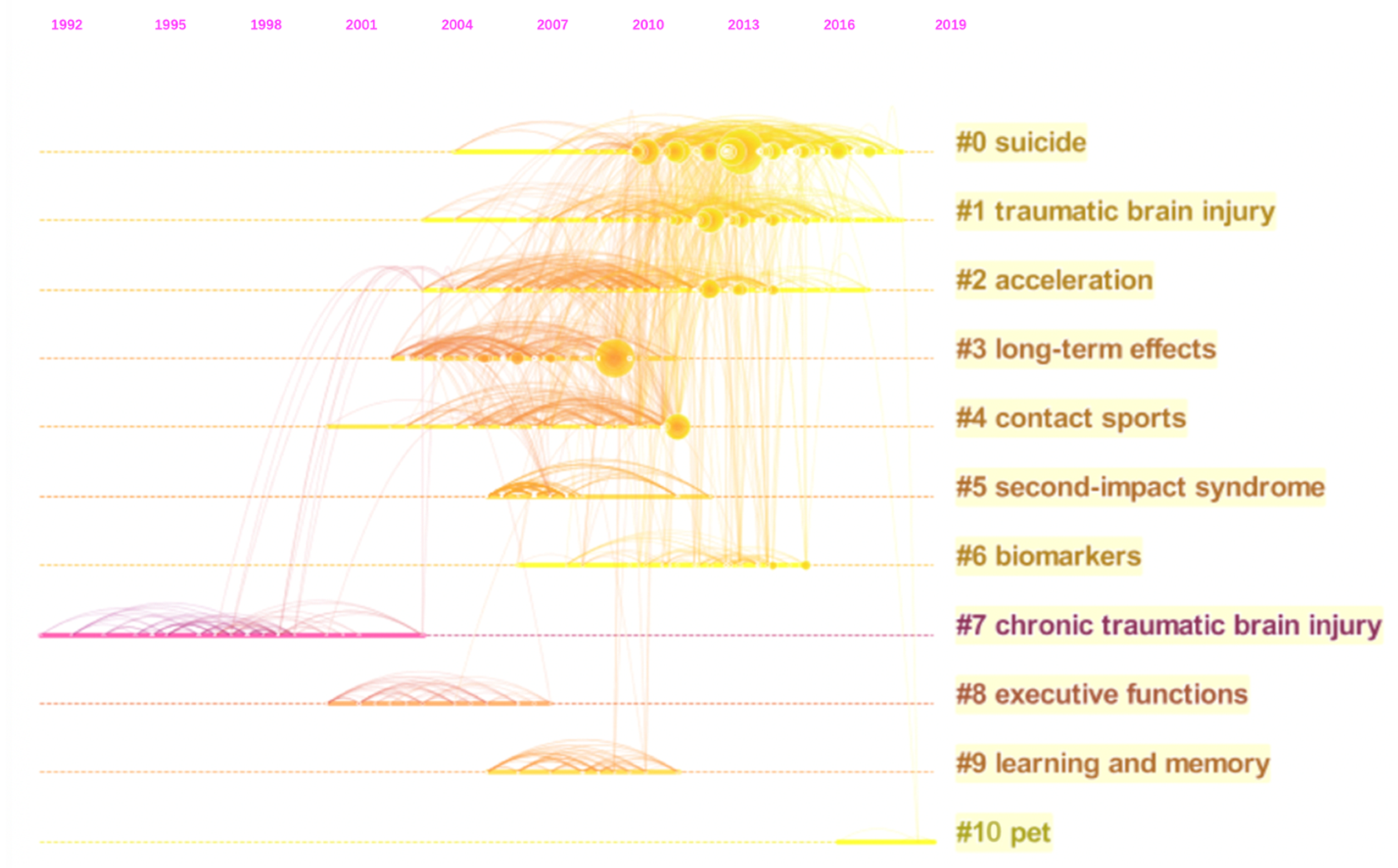
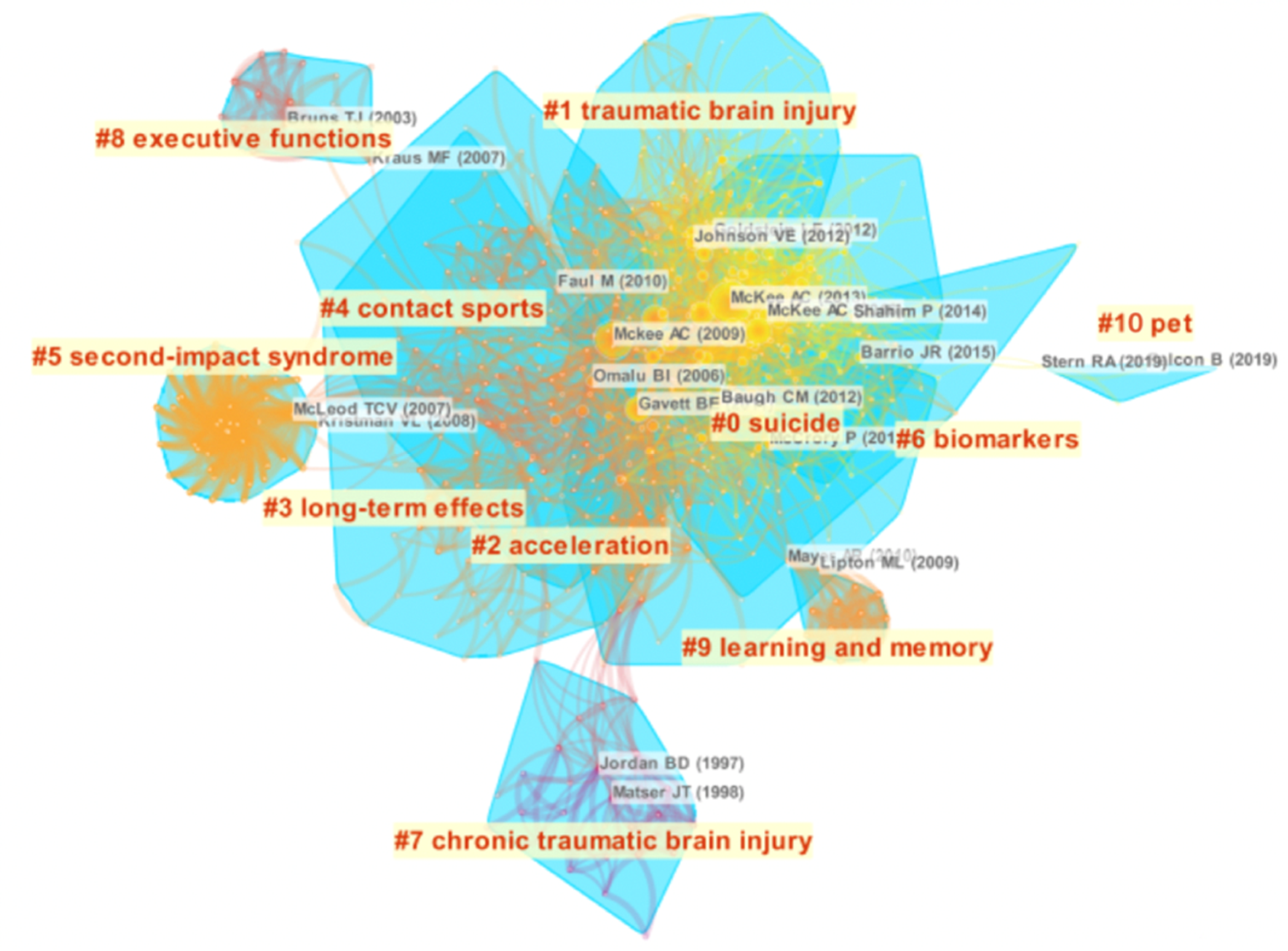
3.5. Analysis of Reference Co-Citation
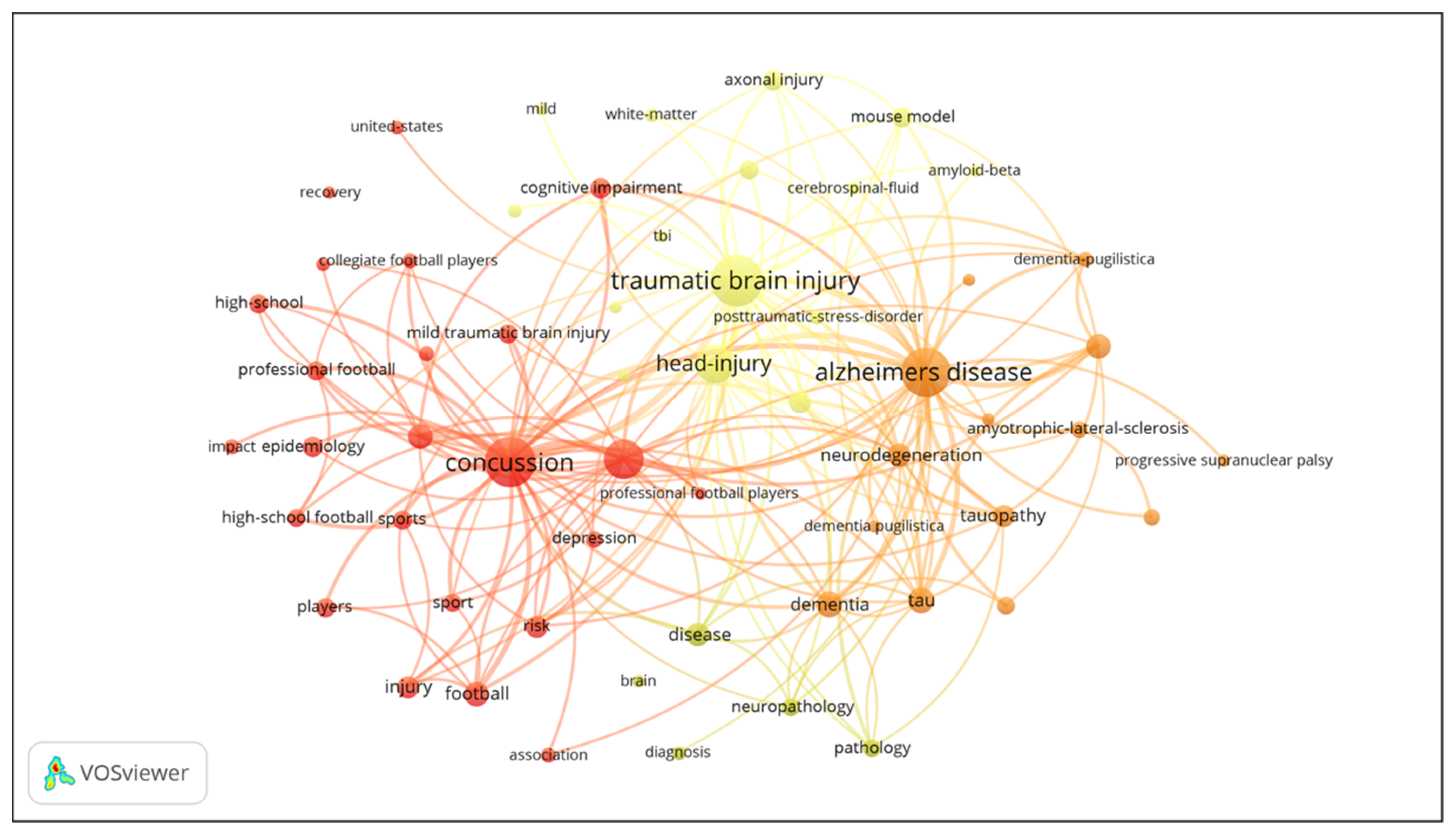
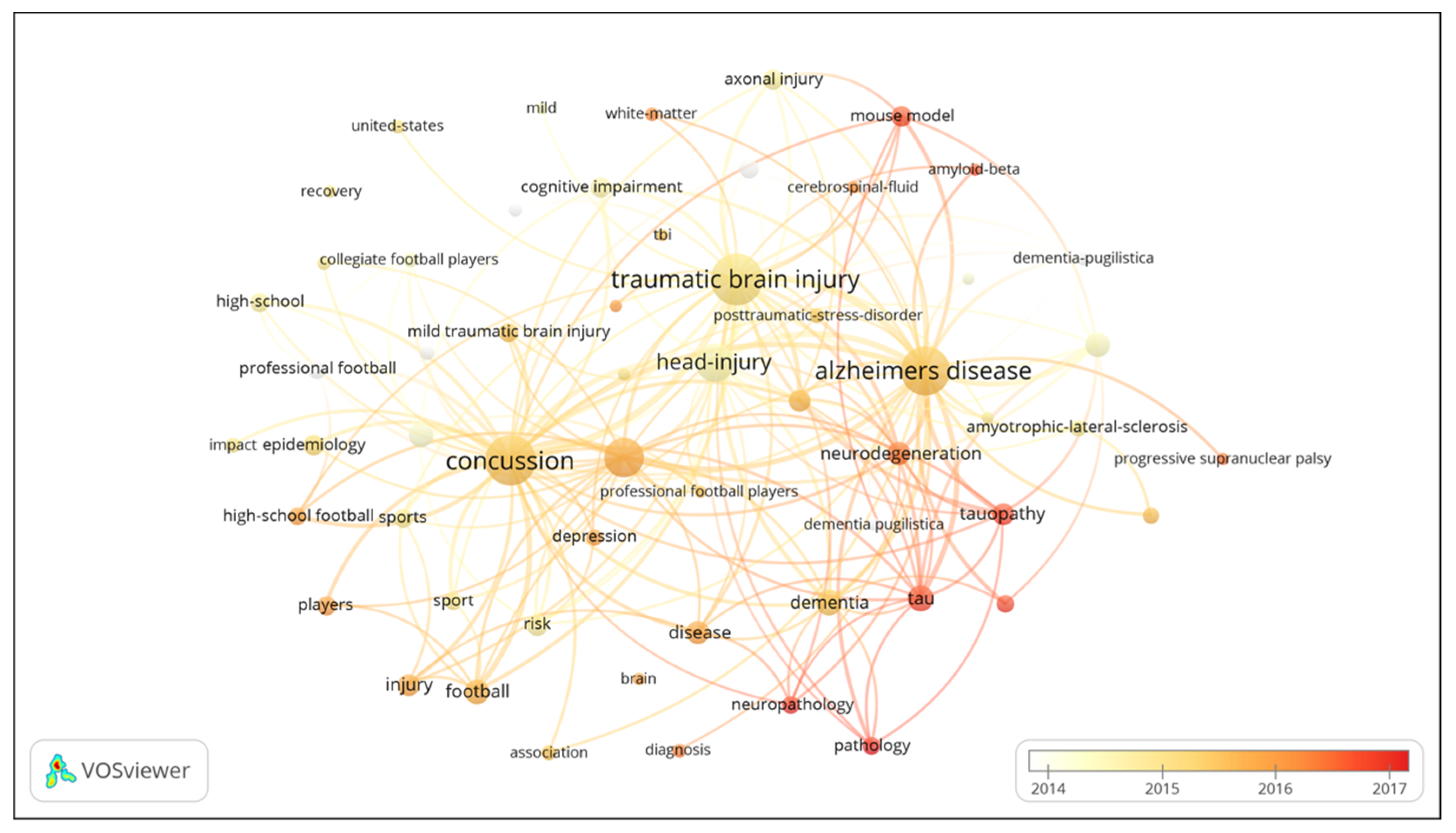
3.6. Analysis of Keywords
4. Discussion
4.1. Research Hotspots
4.2. Research Frontiers
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Costanza, A.; Weber, K.; Gandy, S.; Bouras, C.; Hof, P.R.; Giannakopoulos, P.; Canuto, A. Review: Contact sport-related chronic traumatic encephalopathy in the elderly: Clinical expression and structural substrates. Neuropathol. Appl. Neurobiol. 2011, 37, 570–584. [Google Scholar] [CrossRef] [PubMed]
- Daneshvar, D.H.; Baugh, C.M.; Nowinski, C.J.; McKee, A.C.; Stern, R.A.; Cantu, R.C. Helmets and mouth guards: The role of personal equipment in preventing sport-related concussions. Clin. Sports Med. 2011, 30, 145–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daneshvar, D.H.; Nowinski, C.J.; McKee, A.C.; Cantu, R.C. The epidemiology of sport-related concussion. Clin. Sports Med. 2011, 30, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavett, B.E.; Stern, R.A.; McKee, A.C. Chronic traumatic encephalopathy: A potential late effect of sport-related concussive and sub-concussive head trauma. Clin. Sports Med. 2011, 30, 179–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martland, H.S. Punch drunk. JAMA 1928, 91, 1103–1107. [Google Scholar] [CrossRef]
- Millspaugh, J.A. Dementia pugilistica. U. S. Nav. Med. Bull. 1937, 35, 297–303. [Google Scholar]
- Mez, J.; Daneshvar, D.H.; Kiernan, P.T.; Abdolmohammadi, B.; Alvarez, V.E.; Huber, B.R.; Alosco, M.L.; Solomon, T.M.; Nowinski, C.J.; McHale, L.; et al. Clinicopathological evaluation of chronic traumatic encephalopathy in players of American football. JAMA 2017, 318, 360–370. [Google Scholar] [CrossRef] [Green Version]
- Mckee, A.C.; Cantu, R.C.; Nowinski, C.J.; Hedley-Whyte, E.T.; Gavett, B.E.; Budson, A.E.; Santini, V.E.; Lee, H.S.; Kubilus, C.A.; Stern, R.A. Chronic traumatic encephalopathy in athletes: Progressive tauopathy after repetitive head injury. J. Neuropathol. Exp. Neurol. 2009, 68, 709–735. [Google Scholar] [CrossRef]
- Omalu, B.I.; Fitzsimmons, R.P.; Hammers, J.; Bailes, J. Chronic traumatic encephalopathy in a professional American wrestler. J. Forensic Nurs. 2010, 6, 130–136. [Google Scholar] [CrossRef]
- Omalu, B.; Bailes, J.; Hamilton, R.L.; Kamboh, M.I.; Hammers, J.; Case, M.; Fitzsimmons, R. Emerging histomorphologic phenotypes of chronic traumatic encephalopathy in American athletes. Neurosurgery 2011, 69, 173–183. [Google Scholar] [CrossRef]
- Lim, L.J.; Ho, R.C.; Ho, C.S. Dangers of mixed martial arts in the development of chronic traumatic encephalopathy. Int. J. Environ. Res. Public Health 2019, 16, 254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bieniek, K.F.; Blessing, M.M.; Heckman, M.G.; Diehl, N.N.; Serie, A.M.; Paolini2nd, M.A.; Boeve, B.F.; Savica, R.; Reichard, R.R.; Dickson, D.W. Association between contact sports participation and chronic traumatic encephalopathy: A retrospective cohort study. Brain Pathol. 2020, 30, 63–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omalu, B.; Hammers, J.L.; Bailes, J.; Hamilton, R.L.; Kamboh, M.I.; Webster, G.; Fitzsimmons, R.P. Chronic traumatic encephalopathy in an Iraqi war veteran with posttraumatic stress disorder who committed suicide. Neurosurg. Focus 2011, 31, E3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, L.E.; Fisher, A.M.; Tagge, C.A.; Zhang, X.L.; Velisek, L.; Sullivan, J.A.; Upreti, C.; Kracht, J.M.; Ericsson, M.; Wojnarowicz, M.W.; et al. Chronic traumatic encephalopathy in blast-exposed military veterans and a blast neurotrauma mouse model. Sci. Transl. Med. 2012, 4, 134–160. [Google Scholar]
- Gardner, R.C.; Yaffe, K. Epidemiology of mild traumatic brain injury and neurodegenerative disease. Mol. Cell Neurosci. 2015, 66, 75–80. [Google Scholar] [CrossRef] [Green Version]
- Mckee, A.C.; Stern, R.A.; Nowinski, C.J.; Stein, T.D.; Alvarez, V.E.; Daneshvar, D.H.; Lee, H.S.; Wojtowicz, S.M.; Hall, G.; Baugh, C.M.; et al. The spectrum of disease in chronic traumatic encephalopathy. Brain 2013, 136, 43–64. [Google Scholar] [CrossRef]
- Falcon, B.; Zivanov, J.; Zhang, W.; Murzin, A.G.; Garringer, H.J.; Vidal, R.; Crowther, R.A.; Newell, K.L.; Ghetti, B.; Goedert, M.; et al. Novel tau filament fold in chronic traumatic encephalopathy encloses hydrophobic molecules. Nature 2019, 568, 420–423. [Google Scholar] [CrossRef]
- Yi, F.; Yang, P.; Sheng, H. Tracing the scientific outputs in the field of Ebola research based on publications in the Web of Science. BMC Res. Notes 2016, 9, 221. [Google Scholar] [CrossRef] [Green Version]
- Zhai, F.; Zhai, Y.; Cong, C.; Song, T.; Xiang, R.; Feng, T.; Liang, Z.; Zeng, Y.; Yang, J.; Yang, J.; et al. Research progress of coronavirus based on bibliometric analysis. Int. J. Environ. Res. Public Health 2020, 17, 3766. [Google Scholar] [CrossRef]
- Liu, H.; Hong, R.; Xiang, C.L.; Lv, C.; Li, H.H. Visualization and analysis of mapping knowledge domains for spontaneous combustion studies. Fuel 2020, 262, 116598. [Google Scholar] [CrossRef]
- Goerlandt, F.; Li, J.; Reniers, G. The landscape of risk communication research: A scientometric analysis. Int. J. Environ. Res. Public Health 2020, 17, 3255. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Hu, Z.; Liu, S.; Tseng, H. Emerging trends in regenerative medicine: A scientometric analysis in CiteSpace. Expert Opin. Biol. Ther. 2012, 12, 593–608. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Chen, Y.; Horowitz, M.; Hou, H.; Liu, Z.; Pellegrino, D. Towards an explanatory and computational theory of scientific discovery. J. Informetr. 2009, 3, 191–209. [Google Scholar] [CrossRef] [Green Version]
- Eck, N.J.V.; Waltman, L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics 2010, 84, 523–538. [Google Scholar]
- Trujillo, C.M.; Long, T.M. Document co-citation analysis to enhance transdisciplinary research. Sci. Adv. 2018, 4, e1701130. [Google Scholar] [CrossRef] [Green Version]
- Zou, Y.; Luo, Y.; Zhang, J.; Xia, N.; Tan, G.; Huang, C. Bibliometric analysis of oncolytic virus research, 2000 to 2018. Medicine (Baltimore) 2019, 98, e16817. [Google Scholar] [CrossRef]
- Ling, H.; Morris, H.R.; Neal, J.W.; Lees, A.J.; Hardy, J.; Holton, J.L.; Revesz, T.; Williams, D.D. Mixed pathologies including chronic traumatic encephalopathy account for dementia in retired association football (soccer) players. Acta Neuropathol. 2017, 133, 337–352. [Google Scholar] [CrossRef] [Green Version]
- Mez, J.; Daneshvar, D.H.; Abdolmohammadi, B.; Chua, A.S.; Alosco, M.L.; Kiernan, P.T.; Evers, L.; Marshall, L.; Martin, B.M.; Palmisano, J.; et al. Duration of American football play and chronic traumatic encephalopathy. Ann. Neurol. 2020, 87, 116–131. [Google Scholar] [CrossRef] [Green Version]
- Cassidy, J.D.; Carroll, L.J.; Peloso, P.M.; Borg, J.; Holst, H.V.; Holm, L.; Kraus, J.; Coronado, V.G.; WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. Incidence, risk factors and prevention of mild traumatic brain injury: Results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J. Rehabil. Med. 2004, 43, 28–60. [Google Scholar] [CrossRef] [Green Version]
- Crisco, J.J.; Fiore, R.; Beckwith, J.G.; Chu, J.J.; Brolinson, P.G.; Duma, S.; McAllister, T.W.; Duhaime, A.C.; Greenwald, R.M. Frequency and location of head impact exposures in individual collegiate football players. J. Athl. Train. 2010, 45, 549–559. [Google Scholar] [CrossRef] [Green Version]
- Martin, R. Concussion and chronic traumatic encephalopathy: International rugby board’s response. Br. J. Sports Med. 2014, 48, 79–80. [Google Scholar]
- McCrory, P.; Meeuwisse, W.H.; Aubry, M.; Cantu, B.; Dvorák, J.; Echemendia, R.J.; Engebretsen, L.; Johnston, K.; Kutcher, J.S.; Raftery, M.; et al. Consensus statement on concussion in sport: The 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br. J. Sports Med. 2013, 47, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Aldag, M.; Armstrong, R.C.; Bandak, F.; Bellgowan, P.S.F.; Bentley, T.; Biggerstaff, S.; Caravelli, K.; Cmarik, J.; Crowder, A.; DeGraba, T.J.; et al. The biological basis of chronic traumatic encephalopathy following blast injury: A literature review. J. Neurotrauma. 2017, 34, 26–43. [Google Scholar] [CrossRef]
- McKee, A.C.; Robinson, M.E. Military-related traumatic brain injury and neurodegeneration. Alzheimers Dement. 2014, 10, 242–253. [Google Scholar] [CrossRef] [Green Version]
- Asken, B.M.; Sullan, M.J.; Snyder, A.R.; Houck, Z.M.; Bryant, V.E.; Hizel, L.P.; McLaren, M.E.; Dede, D.E.; Jaffee, M.S.; DeKosky, S.T.; et al. Factors influencing clinical correlates of Chronic Traumatic Encephalopathy (CTE): A review. Neuropsychol Rev. 2016, 26, 340–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montenigro, P.H.; Bernick, C.; Cantu, R.C. Clinical features of repetitive traumatic brain injury and chronic traumatic encephalopathy. Brain Pathol. 2015, 25, 304–317. [Google Scholar] [CrossRef]
- Montenigro, P.H.; Baugh, C.M.; Daneshvar, D.H.; Mez, J.; Budson, A.E.; Au, R.; Katz, D.I.; Cantu, R.C.; Stern, R.A. Clinical subtypes of chronic traumatic encephalopathy: Literature review and proposed research diagnostic criteria for traumatic encephalopathy syndrome. Alzheimers Res. Ther. 2014, 6, 68–84. [Google Scholar] [CrossRef]
- Victoroff, J. Traumatic encephalopathy: Review and provisional research diagnostic criteria. NeuroRehabilitation 2013, 32, 211–224. [Google Scholar] [CrossRef]
- Jordan, B.D. The clinical spectrum of sport-related traumatic brain injury. Nat. Rev. Neurol. 2013, 9, 222–230. [Google Scholar] [CrossRef]
- Saing, T.; Dick, M.; Nelson, P.T.; Kim, R.C.; Cribbs, D.H.; Head, E. Frontal cortex neuropathology in dementia pugilistica. J. Neurotrauma 2012, 29, 1054–1070. [Google Scholar] [CrossRef] [Green Version]
- Omalu, B.I.; Bailes, J.; Hammers, J.L.; Fitzsimmons, R.P. Chronic traumatic encephalopathy, suicides and parasuicides in professional American athletes: The role of the forensic pathologist. Am. J. Forensic Med. Pathol. 2010, 31, 130–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKee, A.C.; Gavett, B.E.; Stern, R.A.; Nowinski, C.J.; Cantu, R.C.; Kowall, N.W.; Perl, D.P.; Hedley-Whyte, E.T.; Price, B.; Sullivan, C.; et al. TDP-43 proteinopathy and motor neuron disease in chronic traumatic encephalopathy. J. Neuropathol. Exp. Neurol. 2010, 69, 918–929. [Google Scholar] [CrossRef] [PubMed]
- McKee, A.C.; Cairns, N.J.; Dickson, D.W.; Folkerth, R.D.; Keene, C.D.; Litvan, I.; Perl, D.P.; Stein, T.D.; Vonsattel, J.P.; Stewart, W.; et al. The first NINDS/NIBIB consensus meeting to define neuropathological criteria for the diagnosis of chronic traumatic encephalopathy. Acta Neuropathol. 2016, 131, 75–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Small, G.W.; Kepe, V.; Siddarth, P.; Ercoli, L.M.; Merrill, D.A.; Donoghue, N.; Bookheimer, S.Y.; Martinez, J.; Omalu, B.; Bailes, J.; et al. PET scanning of brain tau in retired national football league players: Preliminary findings. Am. J. Geriatr. Psychiatry 2013, 21, 138–144. [Google Scholar] [CrossRef]
- Smid, L.M.; Kepe, V.; Vinters, H.V.; Bresjanac, M.; Toyokuni, T.; Satyamurthy, N.; Wong, K.P.; Huang, S.C.; Silverman, D.H.; Miller, K.; et al. Postmortem 3-D brain hemisphere cortical tau and amyloid-β pathology mapping and quantification as a validation method of neuropathology imaging. J. Alzheimers Dis. 2013, 36, 261–274. [Google Scholar] [CrossRef] [Green Version]
- Small, G.W.; Kepe, V.; Ercoli, L.M.; Siddarth, P.; Bookheimer, S.Y.; Miller, K.J.; Lavretsky, H.; Burggren, A.C.; Cole, G.M.; Vinters, H.V.; et al. PET of brain amyloid and tau in mild cognitive impairment. N. Engl. J. Med. 2006, 355, 2652–2663. [Google Scholar] [CrossRef] [Green Version]
- Kepe, V.; Bordelon, Y.; Boxer, A.; Huang, S.C.; Liu, J.; Thiede, F.C.; Mazziotta, J.C.; Mendez, M.F.; Donoghue, N.; Small, G.W.; et al. PET imaging of neuropathology in tauopathies: Progressive supranuclear palsy. J. Alzheimers Dis. 2013, 36, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Barrio, J.R.; Small, G.W.; Wong, K.P.; Huang, S.C.; Liu, J.; Merrill, D.A.; Giza, C.C.; Fitzsimmons, R.P.; Omalu, B.; Bailes, J.; et al. In vivo characterization of chronic traumatic encephalopathy using [F-18] FDDNP PET brain imaging. Proc. Natl. Acad. Sci. USA 2015, 112, E2039–E2047. [Google Scholar] [CrossRef] [Green Version]
- Omalu, B.; Small, G.W.; Bailes, J.; Ercoli, L.M.; Merrill, D.A.; Wong, K.P.; Huang, S.C.; Satyamurthy, N.; Hammers, J.L.; Lee, J.; et al. Postmortem autopsy-confirmation of antemortem [F-18] FDDNP-PET scans in a football player with chronic traumatic encephalopathy. Neurosurgery 2018, 82, 237–246. [Google Scholar] [CrossRef] [Green Version]
- Drechsel, D.N.; Hyman, A.A.; Cobb, M.H.; Kirschner, M.W. Modulation of the dynamic instability of tubulin assembly by the microtubule-associated protein tau. Mol. Biol. Cell 1992, 3, 1141–1154. [Google Scholar] [CrossRef] [Green Version]
- Spillantini, M.G.; Goedert, M. Tau protein pathology in neurodegenerative diseases. Trends Neurosci. 1998, 21, 428–433. [Google Scholar] [CrossRef]
- Zhang, W.; Tarutani, A.; Newell, K.L.; Murzin, A.G.; Matsubara, T.; Falcon, B.; Vidal, R.; Garringer, H.J.; Shi, Y.; Ikeuchi, T.; et al. Novel tau filament fold in corticobasal degeneration. Nature 2020, 580, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, A.; Falcon, B.; He, S.; Murzin, A.G.; Murshudov, G.; Garringer, H.J.; Crowther, R.A.; Ghetti, B.; Goedert, M.; Scheres, S. Cryo-EM structures of tau filaments from Alzheimer’s disease. Nature 2017, 547, 185–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kellogg, E.H.; Hejab, N.; Poepsel, S.; Downing, K.H.; DiMaio, F.; Nogales, E. Near-atomic model of microtubule-tau interactions. Science 2018, 360, 1242–1246. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rank | Country | Counts | Centrality | Institution | Counts | Centrality |
|---|---|---|---|---|---|---|
| 1 | United States | 732 | 0.82 | Boston University | 114 | 0.12 |
| 2 | Canada | 88 | 0.09 | VA Boston Healthcare System | 48 | 0.04 |
| 3 | England | 72 | 0.17 | Emerson Hospital | 40 | 0.10 |
| 4 | Australia | 69 | 0.06 | University of Toronto | 38 | 0.05 |
| 5 | Scotland | 28 | 0.01 | Harvard University | 37 | 0.06 |
| 6 | Japan | 23 | 0.02 | University of Pennsylvania | 35 | 0.11 |
| 7 | China | 21 | 0.06 | Uniformed Services University HLTH SCI | 33 | 0.02 |
| 8 | Germany | 20 | 0.01 | University of Pittsburgh | 33 | 0.09 |
| 9 | Ireland | 20 | 0.09 | Harvard Medical School | 29 | 0.04 |
| 10 | Sweden | 17 | 0.00 | Vanderbilt University | 27 | 0.03 |
| Others | 73 | Others | 1094 |
| Ranking | Journal | Country | Count | Percentage (%) | IF 2019 |
|---|---|---|---|---|---|
| 1 | Journal of Neurotrauma | United States | 64 | 6.639 | 3.793 |
| 2 | Frontiers in Neurology | Switzerland | 24 | 2.490 | 2.889 |
| 3 | Journal of Alzheimer’s Disease | The Netherlands | 22 | 2.282 | 3.909 |
| 4 | Journal of Neuropathology and Experimental Neurology | United States | 21 | 2.178 | 2.923 |
| 5 | Acta Neuropathologica | Germany | 20 | 2.075 | 14.251 |
| 6 | Brain Injury | England | 19 | 1.971 | 1.69 |
| 7 | British journal of Sports Medicine | England | 18 | 1.867 | 12.022 |
| 8 | Journal of Head Trauma Rehabilitation | United States | 15 | 1.556 | 2.814 |
| 9 | American Journal of Sports Medicine | United States | 13 | 1.349 | 5.81 |
| 10 | Acta Neuropathologica Communications | United Kingdom | 12 | 1.245 | 6.27 |
| Others | 736 | 76.349 |
| Rank | Author | Counts | Co-cited Author | Counts | Co-cited Reference | Count |
|---|---|---|---|---|---|---|
| 1 | McKee AC | 59 | McKee AC | 648 | McKee AC, 2013, Brain, V136, P43 | 394 |
| 2 | Stern RA | 42 | Omalu BI | 328 | McKee AC, 2009, J Neuropath Exp Neur, V68, P709 | 334 |
| 3 | Cantu RC | 37 | McCrory P | 269 | McKee AC, 2016, Acta Neuropathol, V131, P75 | 169 |
| 4 | Stein TD | 32 | Guskiewicz KM | 253 | Gavett BE, 2011, Clin Sport Med, V30, P179 | 161 |
| 5 | Alvarez VE | 26 | Stern RA | 243 | Goldstein LE, 2012, Sci Transl Med, V4, P0 | 150 |
| 6 | Alosco ML | 23 | Martland HS | 211 | Stern RA, 2013, Neurology, V81, P1122 | 147 |
| 7 | Tripodis Y | 22 | Omalu B | 201 | McKee AC, 2010, J Neuropath Exp Neur, V69, P918 | 145 |
| 8 | Nowinski CJ | 19 | Jordan BD | 199 | Omalu B, 2011, Neurosurgery, V69, P173 | 142 |
| 9 | Daneshvar DH | 19 | Corsellis JA | 198 | Stern RA, 2011, PM & R, V3, P0 | 120 |
| 10 | Bauhg CM | 16 | Gavett BE | 195 | Baugh CM, 2012, Brain Imaging Behav, V6, P244 | 107 |
| Others | 1115 | Others | 5725 | Others | 4357 |
| Supportive Neuropathological Features of CTE | |
|---|---|
| 1 | Abnormal p-tau immunoreactive pretangles and NFTs preferentially affecting superficial layers (layers II–III), in contrast to layers III and V as in AD |
| 2 | In the hippocampus, pretangles, NFTs or extracellular tangles preferentially affecting CA2 and pretangles and prominent proximal dendritic swellings in CA4. These regional p-tau pathologies differ from the preferential involvement of CA1 and subiculum found in AD |
| 3 | Abnormal p-tau immunoreactive neuronal and astrocytic aggregates in subcortical nuclei, including the mammillary bodies and other hypothalamic nuclei, amygdala, nucleus accumbens, thalamus, midbrain tegmentum, and isodendritic core |
| 4 | p-Tau immunoreactive thorny astrocytes at the glial limitans most commonly found in the subpial and periventricular regions |
| 5 | p-Tau immunoreactive large grain-like and dot-like structures |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qi, B.; Jin, S.; Qian, H.; Zou, Y. Bibliometric Analysis of Chronic Traumatic Encephalopathy Research from 1999 to 2019. Int. J. Environ. Res. Public Health 2020, 17, 5411. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155411
Qi B, Jin S, Qian H, Zou Y. Bibliometric Analysis of Chronic Traumatic Encephalopathy Research from 1999 to 2019. International Journal of Environmental Research and Public Health. 2020; 17(15):5411. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155411
Chicago/Turabian StyleQi, Bote, Shuting Jin, Hongsheng Qian, and Yu Zou. 2020. "Bibliometric Analysis of Chronic Traumatic Encephalopathy Research from 1999 to 2019" International Journal of Environmental Research and Public Health 17, no. 15: 5411. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155411