Pain Acceptance and Pain-Related Disability Predict Healthcare Utilization and Medication Intake in Patients with Non-Specific Chronic Spinal Pain

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
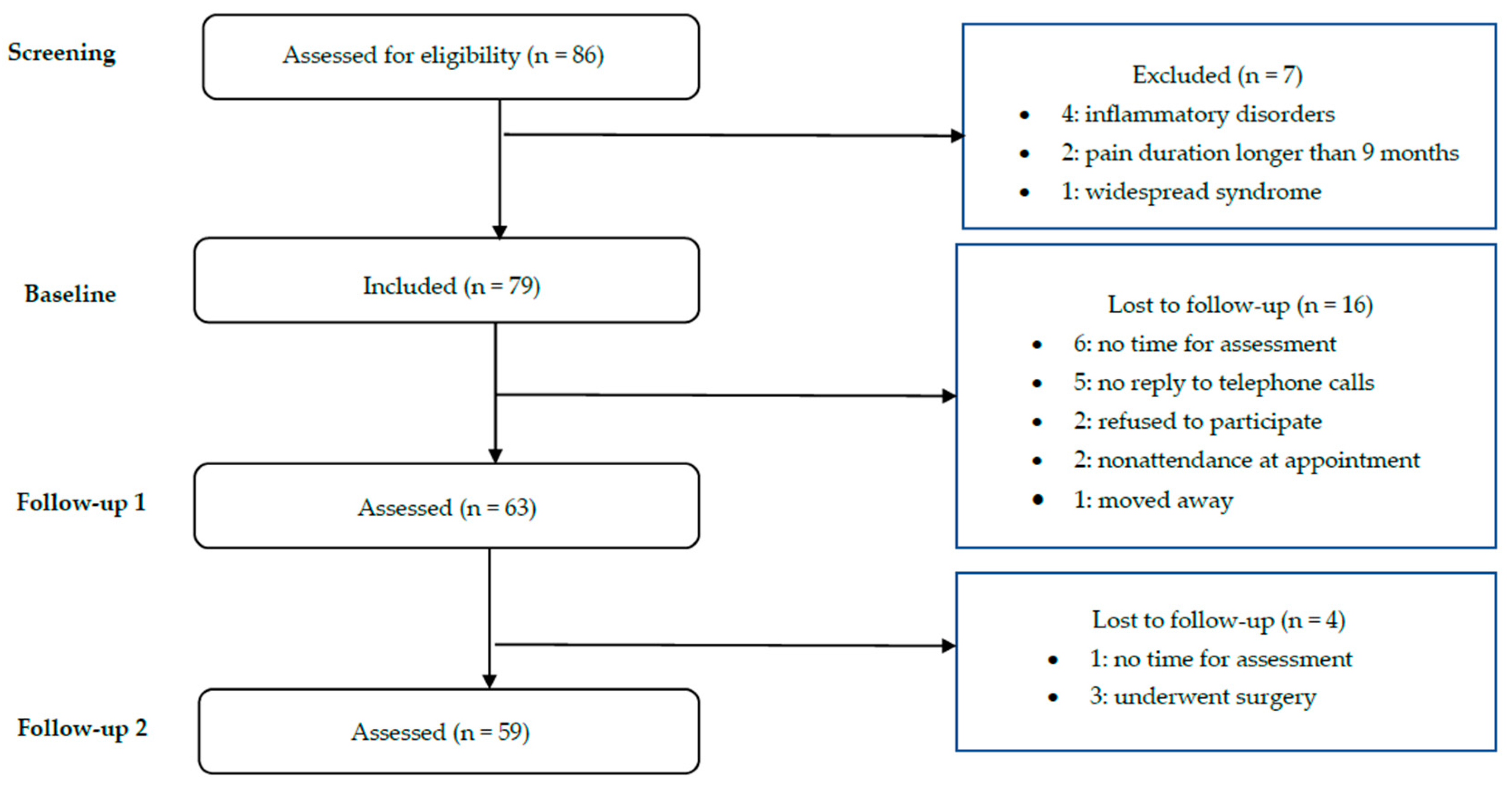
2.1. Procedure
2.2. Participants
2.3. Variables and Instruments
2.3.1. Demographic and Clinical Pain-Related Variables
2.3.2. Pain intensity
2.3.3. Anxiety and Depression Scale
2.3.4. Pain Catastrophizing
2.3.5. Pain Anxiety
2.3.6. Pain Acceptance
2.3.7. Impairment and Functioning
2.3.8. Healthcare Utilization
2.3.9. Medication Intake
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Global Burden of Disease 2013 Collaborators. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 301 Acute and Chronic Diseases and Injuries in 188 Countries, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2013, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finneruph, N.B.; First, M.B.; et al. Chronic Pain as a Symptom or a Disease: The IASP Classification of Chronic Pain for the International Classification of Diseases: (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maher, C.G.; Underwood, M.; Buchbinder, R. Non-Specific Low Back Pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef] [Green Version]
- Kim, L.H.; Vail, D.; Azad, T.D.; Bentley, J.P.; Zhang, Y.; Ho, A.L.; Fatemi, P.; Feng, A.; Varshneya, K.; Desai, M.; et al. Expenditures and Health Care Utilization among Adults with Newly Diagnosed Low Back and Lower Extremity Pain. JAMA 2019, 2, e193676. [Google Scholar] [CrossRef] [Green Version]
- The Pain Proposal 2010. Available online: http://www.efic.org/index.asp?sub=B57HFCF6J4043I. (accessed on 22 December 2019).
- Bissell, A.D.; Ziadni, M.S.; Sturgeon, A.J. Perceived Injustice in Chronic Pain: An Examination Through the Lens of Predictive Processing. Pain Manag. 2018, 8, 129–138. [Google Scholar] [CrossRef]
- Scott, W.; Trost, Z.; Bernier, E.; Sullivan, M.J. Anger Differentially Mediates the Relationship between Perceived Injustice and Chronic Pain Outcomes. Pain 2013, 154, 1691–1698. [Google Scholar] [CrossRef]
- Sullivan, M.J.; Scott, W.; Trost, Z. Perceived Injustice. Clin. J. Pain 2012, 28, 484–488. [Google Scholar] [CrossRef] [Green Version]
- Carriere, J.S.; Sturgeon, J.A.; Yakobov, E.; Kao, M.C.; Mackey, S.C.; Darnall, B.D. The Impact of Perceived Injustice on Pain-related Outcomes: A Combined Model Examining the Mediating Roles of Pain Acceptance and Anger in a Chronic Pain Sample. Clin. J. Pain 2018, 34, 739–747. [Google Scholar] [CrossRef]
- Sullivan, M.J.; Yakobov, E.; Scott, W.; Tait, R. Perceived Injustice and Adverse Recovery Outcomes. Psychol. Inj. Law 2014, 7, 325–334. [Google Scholar] [CrossRef] [Green Version]
- Dueñas, M.; Ojeda, B.; Salazar-Couso, A.; Mico, J.A.; Failde, I. A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 2016, 9, 457–467. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, M.; Machado, G.; Latimer, J.; Maher, C.; Ferreira, P.H.; Smeets, R.J. Factors Defining Care-Seeking in Low Back Pain–A Meta-Analysis of Population Based Surveys. Eur. J. Pain 2010, 14, 747.e1. [Google Scholar] [CrossRef] [PubMed]
- Tiira, A.; Paananen, M.; Taimela, S.; Zitting, P.; Järvelin, M.; Karppinen, J.I. Determinants of Adolescent Health Care Use for Low Back Pain. Eur. J. Pain 2012, 16, 1467–1476. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, O.; Strauch, K.; Held, H.; Redaelli, M.; Chenot, J.-F.; Leonhardt, C.; Keller, S.; Baum, E.; Pfingsten, M.; Hildebrandt, J.; et al. Low Back Pain Patient Subgroups in Primary Care. Clin. J. Pain 2014, 30, 1023–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayner, L.; Hotopf, M.; Petkova, H.; Matcham, F.; Simpson, A.; McCracken, L.M. Depression in Patients with Chronic Pain Attending a Specialised Pain Treatment Center: Prevalence and Impact on Health Care Costs. Pain 2016, 157, 1472–1479. [Google Scholar] [CrossRef] [Green Version]
- Eriksen, J.; Sjøgren, P.; Ekholm, O.; Rasmussen, N.K. Health Care Utilisation among Individuals Reporting Long-Term Pain: An Epidemiological Study Based on Danish National Health Surveys. Eur. J. Pain 2004, 8, 517–523. [Google Scholar] [CrossRef]
- Failde, I. El Dolor Crónico, Algo Más Que Un Problema De Quien Lo Padece. Rev.Soc. Esp. Dolor 2014, 21, 1–2. [Google Scholar] [CrossRef]
- Jöud, A.; Björk, J.; Gerdle, B.; Grimby-Ekman, A.; Larsson, B. The Association between Pain Characteristics, Pain Catastrophizing and Health Care Use – Baseline Results from the SWEPAIN Cohort. Scand. J. Pain 2017, 16, 122–128. [Google Scholar] [CrossRef]
- Keeley, P.; Creed, F.; Tomenson, B.; Todd, C.; Borglin, G.; Dickens, C. Psychosocial Predictors of Health-Related Quality of Life and Health Service Utilisation in People with Chronic Low Back Pain. Pain 2008, 135, 142–150. [Google Scholar] [CrossRef]
- McCracken, L.M.; Eccleston, C. A Prospective Study of Acceptance of Pain and Patient Functioning with Chronic Pain. Pain 2005, 118, 164–169. [Google Scholar] [CrossRef]
- McCracken, L.M.; Vowles, K.E. A Prospective Analysis of Acceptance of Pain and Values-Based Action in Patients with Chronic Pain. Heal. Psychol. 2008, 27, 215–220. [Google Scholar] [CrossRef]
- McCracken, L.M.; Vowles, K.E.; Gauntlett-Gilbert, J. A Prospective Investigation of Acceptance and Control-Oriented Coping with Chronic Pain. J. Behav. Med. 2007, 30, 339–349. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; E Vowles, K.; Zhao-O’Brien, J. Further Development of an Instrument to Assess Psychological Flexibility in People with Chronic Pain. J. Behav. Med. 2010, 33, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and Commitment Therapy: Model, Processes and Outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCracken, L.M.; Morley, S. The Psychological Flexibility Model: A Basis for Integration and Progress in Psychological Approaches to Chronic Pain Management. J. Pain 2014, 15, 221–234. [Google Scholar] [CrossRef] [Green Version]
- Esteve, R.; Bendayan, R.; López-Martínez, A.E.; Ramírez-Maestre, C. Resilience and Vulnerability Factors When Pain is Acute as Predictors of Disability: Findings from a Two-Year Longitudinal Study. Pain Med 2017, 18, 2116–2125. [Google Scholar] [CrossRef]
- Jensen, M.P.; A Turner, J.; Romano, J.M.; Fisher, L.D. Comparative Reliability and Validity of Chronic Pain Intensity Measures. Pain 1999, 83, 157–162. [Google Scholar] [CrossRef]
- Quintana, J.M.; Padierna, A.; Esteban, C.; Arostegui, I.; Bilbao, A.; Ruiz, I. Evaluation of the psychometric characteristics of the Spanish version of the Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 2003, 107, 216–221. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- García-Campayo, J.; Rodero, B.; Alda, M.; Sobradiel, N.; Montero, J.; Moreno, S. Validación De La Versión Española De La Escala De La Catastrofización Ante El Dolor (Pain Catastrophizing Scale) En La Fibromialgia. Med. Clín. 2008, 131, 487–492. [Google Scholar] [CrossRef]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- López-Martínez, A.E.; Esteve-Zarazaga, R.; Ramírez-Maestre, C. S517 The Spanish Version of the Pain Anxiety Symptoms Scale (Pass-20): Preliminary Data on its Reliability, Validity and Factorial Structure. Eur. J. Pain Suppl. 2011, 5, 265. [Google Scholar] [CrossRef]
- McCracken, L.M.; Zayfert, C.; Gross, R.T. The Pain Anxiety Symptoms Scale: Development and Validation of a Scale to Measure Fear of Pain. Pain 1992, 50, 67–73. [Google Scholar] [CrossRef]
- Bendayan, R.; Esteve, R.; Blanca, M.J. New Empirical Evidence of the Validity of the Chronic Pain Acceptance Questionnaire: The Differential Influence of Activity Engagement and Pain Willingness on Adjustment to Chronic Pain. Br. J. Heal. Psychol. 2011, 17, 314–326. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Vowles, K.E.; Eccleston, C. Acceptance of Chronic Pain: Component Analysis and a Revised Assessment Method. Pain 2004, 107, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Maestre, C.; Esteve, R. A New Version of the Impairment and Functioning Inventory for Patients with Chronic Pain (IFI-R). PM&R 2015, 7, 455–465. [Google Scholar] [CrossRef]
- Little, P.; Somerville, J.; Williamson, I.; Warner, G.; Moore, M.; Wiles, R.; George, S.; Smith, A.; Peveler, R. Psychosocial, Lifestyle, and Health Status Variables in Predicting High Attendance among Adults. Br. J. Gen. Prac. 2001, 51, 987–994. [Google Scholar]
- Aban, I.B.; Cutter, G.R.; Mavinga, N. Inferences and Power Analysis Concerning Two Negative Binomial Distributions with an Application to MRI Lesion Counts Data. Comput. Stat. Data Anal. 2009, 53, 820–833. [Google Scholar] [CrossRef] [Green Version]
- Augustson, E.M. Issues of Acceptance in Chronic Pain Populations. Behav. Anal. Today 1999, 1, 14–17. [Google Scholar] [CrossRef]
- Eccleston, C.; Williams, A.C.; Rogers, W.S. Patients’ and Professionals’ Understandings of the Causes of Chronic Pain: Blame, Responsibility and Identity Protection. Soc. Sci. Med. 1997, 45, 699–709. [Google Scholar] [CrossRef]
- Thorne, F.M.; Morley, S. Prospective Judgments of Acceptable Outcomes for Pain, Interference and Activity: Patient-Determined Outcome Criteria. Pain 2009, 144, 262–269. [Google Scholar] [CrossRef]
- Kossakowska, K.; Szczepanik, M.; Woszczak, M. Factors of Subjective Assessment of the Effectiveness of Physiotherapy: A Study on Patients with Degenerative Disease of the Spine. Fam. Med. Prim. Care Rev. 2018, 20, 131–138. [Google Scholar] [CrossRef]
- Gardner, T.; Refshauge, K.; McAuley, J.H.; Goodall, S.; Hübscher, M.; Smith, L. Patient Led Goal Setting in Chronic Low Back Pain—What Goals are Important to the Patient and Are they Aligned to What We Measure? Patient Educ. Couns. 2015, 98, 1035–1038. [Google Scholar] [CrossRef] [PubMed]
- Jack, K.; McLean, S.M.; Moffett, J.K.; Gardiner, E. Barriers to Treatment Adherence in Physiotherapy Outpatient Clinics: A Systematic Review. Man. Ther. 2010, 15, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Peek, K.; Sanson-Fisher, R.; Mackenzie, L.; Carey, M. Interventions to Aid Patient Adherence to Physiotherapist Prescribed Self-Management Strategies: A Systematic Review. Physiotherapy 2016, 102, 127–135. [Google Scholar] [CrossRef]
- Pike, A.; Hearn, L.; Williams, A.C. Effectiveness of Psychological Interventions for Chronic Pain on Health Care Use and Work Absence: Systematic Review and Meta-Analysis. Pain 2016, 157, 777–785. [Google Scholar] [CrossRef]
- Gilpin, H.R.; Keyes, A.; Stahl, D.R.; Greig, R.; McCracken, L.M. Predictors of Treatment Outcome in Contextual Cognitive and Behavioral Therapies for Chronic Pain: A systematic review. J. Pain 2017, 18, 1153–1164. [Google Scholar] [CrossRef] [Green Version]
- Glenn, B.; Burns, J.W. Pain Self-Management in the Process and Outcome of Multidisciplinary Treatment of Chronic Pain: Evaluation of a Stage of Change Model. J. Behav. Med. 2003, 26, 417–433. [Google Scholar] [CrossRef]
- Jensen, M.P.; Nielson, W.R.; Kerns, R.D. Toward the Development of a Motivational Model of Pain Self-Management. J. Pain 2003, 4, 477–492. [Google Scholar] [CrossRef]
- Mun, C.J.; Otis, J.D.; Concato, J.; Reid, M.C.; Burg, M.M.; Czlapinski, R.; Kerns, R.D. Further Examination of the Pain Stages of Change Questionnaires Among Chronic Low Back Pain Patients. Clin. J. Pain 2019, 35, 744–752. [Google Scholar] [CrossRef]
- Qaseem, A.; Wilt, T.J.; McLean, R.M.; Forciea, M.A. Clinical Guidelines Committee of the American College of Physicians Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann. Intern. Med. 2017, 166, 514–530. [Google Scholar] [CrossRef] [Green Version]
- Wideman, T.H.; Sullivan, M.J. Differential Predictors of the Long-Term Levels of Pain Intensity, Work Disability, Healthcare Use, and Medication Use in a Sample of Workers’ Compensation Claimants. Pain 2011, 152, 376–383. [Google Scholar] [CrossRef]
- Wideman, T.H.; Asmundson, G.G.J.; Smeets, R.J.E.M.; Zautra, A.J.; Simmonds, M.J.; Sullivan, M.J.L.; Haythornthwaite, J.A.; Edwards, R.R. Rethinking the Fear Avoidance Model: Toward a Multidimensional Framework of Pain-Related Disability. Pain 2013, 154, 2262–2265. [Google Scholar] [CrossRef] [PubMed]
- Fillingim, R.B. Sex, Gender, and Pain. In Principles of Gender-Specific Medicine: Gender in the Genomic Era; Legato, M.J., Ed.; Academic Press: San Diego, CA, USA, 2017; pp. 481–496. [Google Scholar]
- Samulowitz, A.; Gremyr, I.; Eriksson, E.; Hensing, G. “Brave Men” and “Emotional Women”: A Theory-Guided Literature Review on Gender Bias in Health Care and Gendered Norms towards Patients with Chronic Pain. Pain Res. Manag. 2018. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, A.; Wagner, T. Self-Reported Utilization of Health Care Services: Improving Measurement and Accuracy. Med. Care Res. Rev. 2006, 63, 217–235. [Google Scholar] [CrossRef]
- Clewley, D.; Rhon, D.; Flynn, T.; Koppenhaver, S.; Cook, C. Health Seeking Behavior as a Predictor of Healthcare Utilization in a Population of Patients with Spinal Pain. PLoS ONE 2018, 13, e0201348. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Mean (SD) | N (%) |
|---|---|---|
| Sex | ||
| Female | 50 (79.4) | |
| Male | 13 (20.6) | |
| Employment status | ||
| Full-Time employed | 29 (46) | |
| Homemaker | 21 (33.3) | |
| Other (student, retired, unemployed) | 13 (20.7) | |
| Pain intensity | 4.79 (2.16) | |
| Age | 49.57 (16.49) | |
| Depression | 11.54 (4.81) | |
| Pain catastrophizing | 15.40 (12.50) | |
| Pain anxiety | 57.29 (29.35) | |
| Pain acceptance | 72.54 (22.26) | |
| Disability | 2.71 (3.73) | |
| Healthcare utilization follow-up 1 | 1.76 (1.78) | |
| Healthcare utilization follow-up 2 | 0.85 (0.83) | |
| Medication intake follow-up 1 | 0.95 (0.91) | |
| Medication intake follow-up 2 | 1.20 (0.98) |
| Variable | Women | Men | t/χ2 | p | ||
|---|---|---|---|---|---|---|
| Mean/N | SD | Mean/N | SD | |||
| Employment status | Full-Time employed: 21 Homemaker: 21 Other (student, retired, unemployed): 8 | Full-Time employed: 8 Homemaker: 0 Other (student, retired, unemployed): 5 | 8.838 | 0.012 | ||
| Pain intensity | 5.05 | 1.89 | 3.81 | 2.85 | −1.487 | 0.158 |
| Age | 50.66 | 16.58 | 45.38 | 16.09 | −1.028 | 0.308 |
| Depression | 11.64 | 4.62 | 11.15 | 5.68 | −0.322 | 0.748 |
| Pain Catastrophizing | 14.74 | 12.06 | 17.92 | 14.29 | 0.816 | 0.418 |
| Pain anxiety | 58.14 | 29.70 | 54.00 | 28.91 | −0.450 | 0.654 |
| Pain acceptance | 72.34 | 20.34 | 73.31 | 29.50 | 0.139 | 0.890 |
| Disability | 2.78 | 3.55 | 2.46 | 4.50 | −0.272 | 0.786 |
| Healthcare utilization follow-up 1 | 1.80 | 1.81 | 1.62 | 1.71 | −0.332 | 0.741 |
| Healthcare utilization follow-up 2 | 0.84 | 0.81 | 0.88 | 0.89 | −0.354 | 0.725 |
| Medication intake follow-up 1 | 1.10 | 0.91 | 0.38 | 0.65 | −2.658 | 0.010 |
| Medication intake follow-up 2 | 1.35 | 0.97 | 0.81 | 0.91 | −1.783 | 0.080 |
| Predictors | Follow-Up 1 | Follow-Up 2 | ||||
|---|---|---|---|---|---|---|
| IRR | 95% CI | p | IRR | 95% CI | p | |
| Sex (female/male) | 0.949 | 0.498–1.807 | 0.874 | 1.045 | 0.596–1.832 | 0.877 |
| Employment status | ||||||
| Full-time employed | 0.757 | 0.381–1.502 | 0.425 | 0.861 | 0.476–1.558 | 0.622 |
| Homemaker | 0.673 | 0.323–1.401 | 0.290 | 0.805 | 0.424–1.529 | 0.507 |
| Other | 1 | ---- | ---- | 1 | ---- | ---- |
| Pain intensity | 1.154 | 1.020–1.304 | 0.023 | 1.019 | 0.909–1.143 | 0.744 |
| Age | 1.001 | 0.985–1.017 | 0.935 | 0.989 | 0.975–1.004 | 0.164 |
| Depression | 1.013 | 0.961–1.068 | 0.635 | 1.020 | 0.972–1.070 | 0.415 |
| Pain catastrophizing | 1.010 | 0.989–1.031 | 0.362 | 1.009 | 0.991–1.028 | 0.339 |
| Pain anxiety | 1.009 | 1.000–1.018 | 0.041 | 1.007 | 0.998–1.016 | 0.113 |
| Pain acceptance | 0.984 | 0.973–0.995 | 0.004 | 0.993 | 0.983–1.004 | 0.200 |
| Disability | 1.072 | 1.004–1.145 | 0.037 | 1.071 | 1.033–1.111 | 0.000 |
| Predictors | Follow-Up 1 | Follow-Up 2 | ||||
|---|---|---|---|---|---|---|
| IRR | 95% CI | p | IRR | 95% CI | p | |
| Sex (female/male) | 0.341 | 0.163–0.713 | 0.004 | 0.602 | 0.364–0.998 | 0.049 |
| Employment status | ||||||
| Full-time employed | 1.144 | 0.554–2.362 | 0.717 | 0.909 | 0.541–1.529 | 0.719 |
| Homemaker | 2.519 | 1.231–5.154 | 0.011 | 1.444 | 0.853–2.445 | 0.172 |
| Other | 1 | --- | --- | 1 | --- | --- |
| Pain intensity | 1.191 | 1.056–1.344 | 0.004 | 1.148 | 1.044–1.263 | 0.004 |
| Age | 1.017 | 1.001–1.034 | 0.041 | 1.011 | 0.997–1.025 | 0.121 |
| Depression | 1.061 | 1.014–1.111 | 0.011 | 1.053 | 1.013–1.094 | 0.008 |
| Pain catastrophizing | 1.024 | 1.005–1.043 | 0.014 | 1.006 | 0.990–1.022 | 0.440 |
| Pain anxiety | 1.016 | 1.007–1.024 | 0.000 | 1.008 | 1.001–1.016 | 0.031 |
| Pain acceptance | 0.979 | 0.969–0.990 | 0.000 | 0.988 | 0.980–0.997 | 0.011 |
| Disability | 1.036 | 0.972–1.104 | 0.277 | 1.014 | 0.957–1.075 | 0.637 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esteve, R.; López-Martínez, A.E.; Ruíz-Párraga, G.T.; Serrano-Ibáñez, E.R.; Ramírez-Maestre, C. Pain Acceptance and Pain-Related Disability Predict Healthcare Utilization and Medication Intake in Patients with Non-Specific Chronic Spinal Pain. Int. J. Environ. Res. Public Health 2020, 17, 5556. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155556
Esteve R, López-Martínez AE, Ruíz-Párraga GT, Serrano-Ibáñez ER, Ramírez-Maestre C. Pain Acceptance and Pain-Related Disability Predict Healthcare Utilization and Medication Intake in Patients with Non-Specific Chronic Spinal Pain. International Journal of Environmental Research and Public Health. 2020; 17(15):5556. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155556
Chicago/Turabian StyleEsteve, Rosa, Alicia Eva López-Martínez, Gema Teresa Ruíz-Párraga, Elena Rocío Serrano-Ibáñez, and Carmen Ramírez-Maestre. 2020. "Pain Acceptance and Pain-Related Disability Predict Healthcare Utilization and Medication Intake in Patients with Non-Specific Chronic Spinal Pain" International Journal of Environmental Research and Public Health 17, no. 15: 5556. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155556