The Effectiveness of Individual or Group Physiotherapy in the Management of Sub-Acromial Impingement: A Randomised Controlled Trial and Health Economic Analysis

 and
and
Abstract
:1. Background
2. Methods
2.1. Study Design
2.2. Population
2.3. Intervention
2.4. Comparator
2.5. Steroid Injection
2.6. Outcome Measures
2.7. Study Withdrawals
2.8. Randomisation, Allocation Concealment and Blinding
2.9. Sample Size Calculation
2.10. Statistical Analysis
2.11. Health Economic Analysis
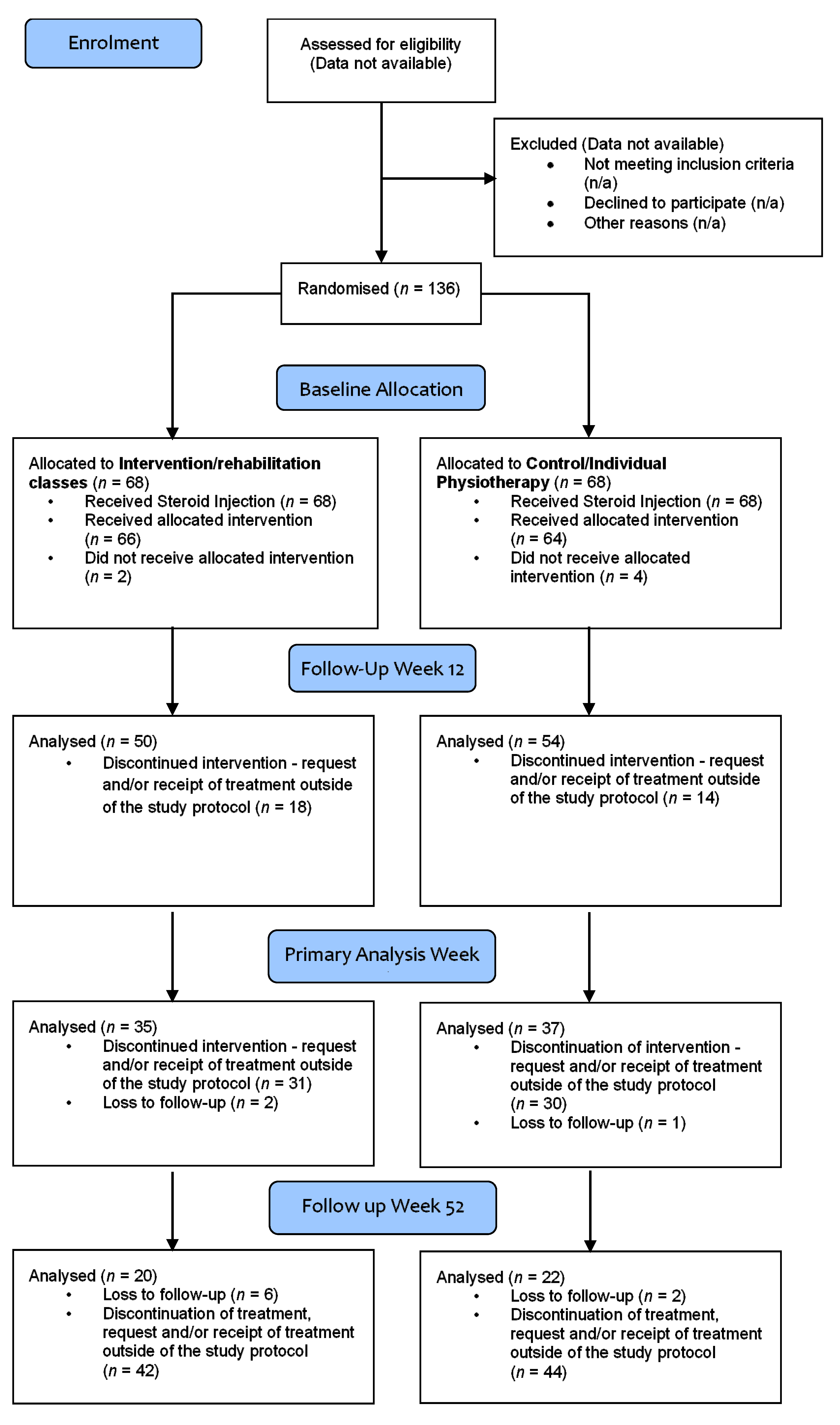
3. Results
3.1. Baseline Characteristics
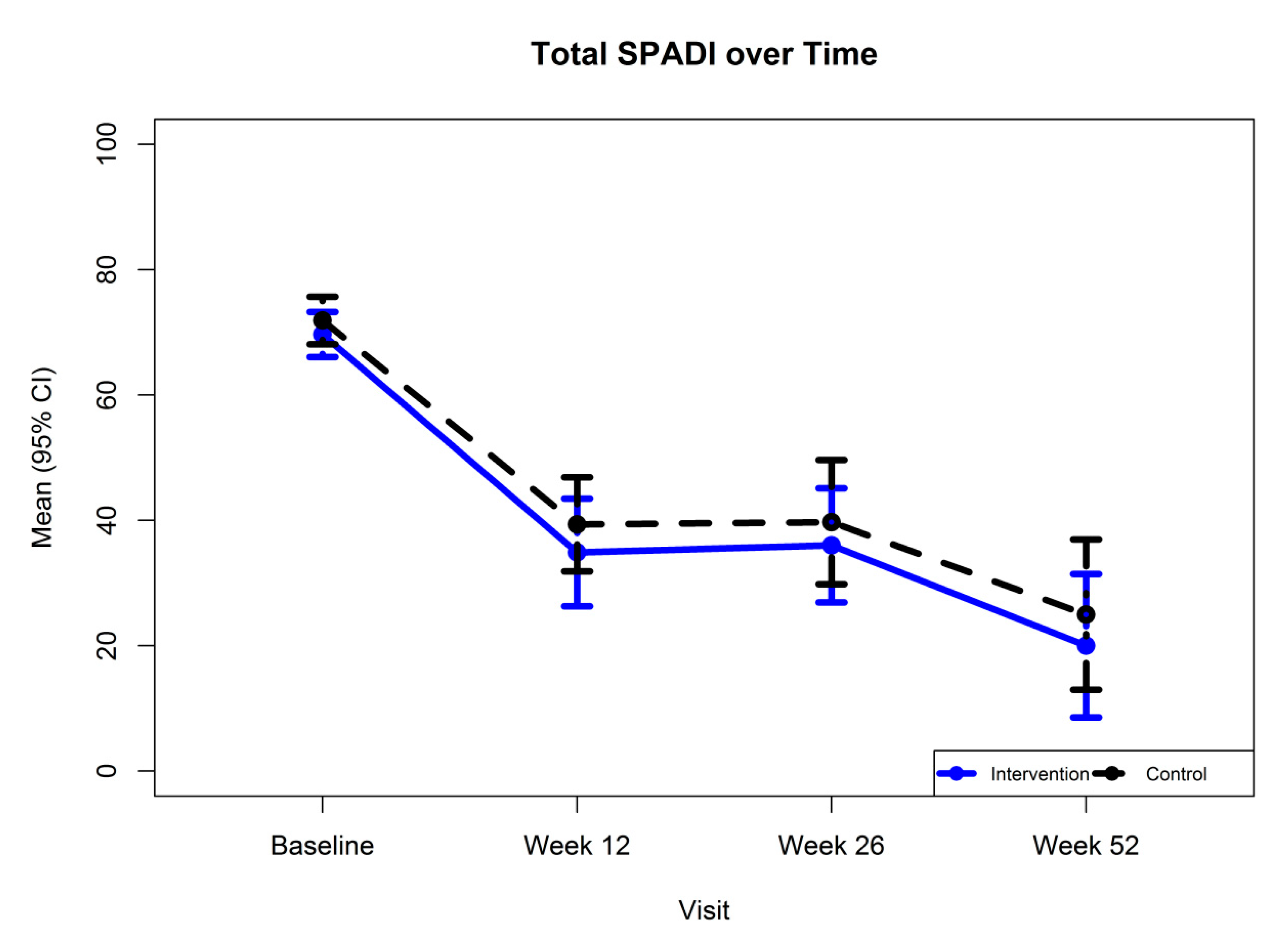
3.2. Primary Outcome Measure
3.3. Secondary Outcome Measures
3.4. Physiotherapy
3.5. Health Economic Analysis
4. Discussion
4.1. Summary
4.2. Strengths and Limitations
4.3. Comparison with Existing Literature
4.4. Implications for Research and/or Practice
4.5. How This Fits in to Clinical Practice
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Luime, J.J.; Koes, B.W.; Hendriksen, I.J.M.; Burdorf, A.; Verhagen, A.P.; Miedema, H.S.; Verhaar, J.A.N. Prevalence and incidence of shoulder pain in the general population: A systematic review. Scand. J. Rheumatol. 2004, 33, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Croft, P.; Pope, D.; Silman, A. The Clinical Course of Shoulder Pain: Prospective Cohort Study in Primary Care. BMJ 1996, 313, 601. [Google Scholar] [CrossRef] [PubMed]
- Virta, L.; Joranger, P.; Brox, J.I.; Eriksson, R. Costs of shoulder pain and resource use in primary health care: A cost-of-illness study in Sweden. BMC Musculoskelet. Disord. 2012, 13, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Largacha, M.; Parsons, I.M.; Campbell, B.; Titelman, R.M.; Smith, K.L.; Matsen, F., 3rd. Deficits in shoulder function and general health associated with sixteen common shoulder diagnoses: A study of 2674 patients. J. Shoulder Elbow Surg. 2006, 15, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Umer, M.; Qadir, I.; Azam, M. Subacromial impingement syndrome. Orthop. Rev. 2012, 4, e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdulla, S.Y.; Southerst, D.; Cotte, P.; Shearer, H.M.; Sutton, D.; Randhawa, K.; Varatharajan, S.; Wong, J.J.; Yu, H.; Marchand, A.; et al. Is exercise effective for the management of subacromial impingement syndrome and other soft tissue injuries of the shoulder? A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Man. Ther. 2015, 20, 646–656. [Google Scholar] [CrossRef]
- Karel, Y.H.J.M.; Scholten-Peeters, G.; Thoomes-de Graaf, M.; Duijn, E.; van Broekhoven, J.B.; Koes, B.W.; Verhagen, A.P. Physiotherapy for patients with shoulder pain in primary care: A descriptive study of diagnostic- and therapeutic management. Physiotherapy 2017, 103, 369–378. [Google Scholar] [CrossRef]
- Buchbinder, R.; Green, S.; Youd, J.M. Corticosteroid injections for shoulder pain. Cochrane Database Syst. Rev. 2003, 1, CD004016. [Google Scholar]
- Page, M.J.; Green, S.; McBain, B.; Surace, S.J.; Deitch, J.; Lyttle, N.; Mrocki, M.A.; Buchbinder, R. Manual therapy and exercise for rotator cuff disease. Cochrane Database Syst. Rev. 2016, 6, CD012224. [Google Scholar] [CrossRef]
- Diercks, R.; Bron, C.; Dorrestijn, O.; Meskers, C.; Naber, R.; de Ruiter, T.; Willems, J.; Winters, J.; van der Woude, H.J.; Dutch Orthopaedic Association. Guideline for diagnosis and treatment of subacromial pain syndrome. A multidisciplinary review by the Dutch Orthopaedic Association. Acta Orthop. 2014, 85, 314–322. [Google Scholar] [CrossRef] [Green Version]
- O’Keeffe, M.; Hayes, A.; McCreesh, K.; Purtill, H.; O’Sullivan, K. Are group-based and individual physiotherapy exercise programmes equally effective for musculoskeletal conditions? A systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 126–132. [Google Scholar] [CrossRef]
- Jowett, S.; Crawshaw, D.; Helliwell, P.; Hensor, E.M.A.; Hay, E.M.; Conaghan, P.G. Cost effectiveness of exercise therapy after corticosteroid injection for moderate to severe shoulder pain due to subacromial impingement syndrome: A trial based analysis. Rheumatology (Oxford) 2013, 52, 1485–1491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groenier, K.H.; Winters, J.C.; van Schuur, W.H.; De Winter, A.F.; Meyboom-De Jong, B. A simple classification system was recommended for patients with restricted shoulder or neck range of motion. J. Clin. Epidemiol. 2006, 59, 599–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heald, S.L.; Riddle, D.L.; Lamb, R.L. The shoulder pain and disability index: The construct validity and responsiveness of a region-specific disability measure. Phys. Ther. 1997, 77, 1079–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, J.S.; MacDermid, J.C.; Woodhouse, L.J. Measuring shoulder function: A systematic review of four questionnaires. Arthritis Rheum. 2009, 61, 623–632. [Google Scholar] [CrossRef]
- Williams, J.W., Jr.; Holleman, D.R., Jr.; Simel, D.L. Measuring shoulder function with the Shoulder Pain and Disability Index. J. Rheumatol. 1995, 22, 727–732. [Google Scholar]
- McHorney, C.A.; Ware, J.E.; Raczek, A.E. The MOS 36-item Short Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [Green Version]
- EuroQol Group. Euroqol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar]
- Abiodun, O.A. A validity study of the Hospital Anxiety and Depression Scale in general hospital units and a community sample in Nigeria. Br. J. Psychiatry 1994, 165, 669–672. [Google Scholar] [CrossRef]
- Carette, S.; Moffet, H.; Tardif, J.; Bessette, L.; Morin, F.; Frémont, P.; Bykerk, V.; Thorne, C.; Bell, M.; Bensen, W.; et al. Intraarticular corticosteroids, supervised physiotherapy, or a combination of the two in the treatment of adhesive capsulitis of the shoulder: A placebo-controlled trial. Arthritis Rheum. 2003, 48, 829–838. [Google Scholar] [CrossRef]
- Curtis, L. Unit Costs of Health and Social Care 2014; Personal Social Services Research Unit, University of Kent: Canterbury, UK, 2014. [Google Scholar]
- Department of Health. NHS Reference Costs 2013/2014; Department of Health: London, UK, 2014. [Google Scholar]
- Joint Formulary Committee. British National Formulary. Available online: http://www.medicinescomplete.com (accessed on 29 January 2015).
- Russell, S.; Jariwala, A.; Conlon, R.; Selfe, J.; Richards, J.; Walton, M. A blinded, randomized, controlled trial assessing conservative management strategies for frozen shoulder. J. Shoulder Elbow Surg. 2014, 23, 500–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asensio-García, M.D.R.; Bernabeú-Casas, R.C.; Palazón-Bru, A.; Tomás-Rodríguez, M.I.; Nouni-García, R. Effectiveness of a Group Physiotherapy Intervention in Nontraumatic, Inoperable Painful Shoulder: A Randomized Clinical Trial. Am. J. Phys. Med. Rehabil. 2018, 97, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Booth, J.; Moseley, G.L.; Schiltenwolf, M.; Cashin, A.; Davies, M.; Hübscher, M. Exercise for chronic musculoskeletal pain: A biopsychosocial approach. Musculoskelet. Care 2017, 15, 413–421. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Variable | Intervention | Control |
|---|---|---|
| Number of patients (n) | 68 | 68 |
| Mean Age (SD) | 54.5 (10.9) | 58.1 (11.1) |
| Gender (n, %) | ||
| Female | 44 (64.7) | 39 (57.4) |
| Male | 24 (35.3) | 29 (42.6) |
| Ethnic origin (n, %) | ||
| Caucasian | 68 (100) | 66 (97) |
| Black | 0 | 2 (2.9) |
| Paid employment (n, %) | ||
| No | 34 (50) | 41 (60.3) |
| Yes | 34 (50) | 27 (39.7) |
| Off work due to shoulder pain (n, %) | 12 (35.3) | 6 (22.2) |
| Lost working days (median, IQR) | 14.5 (4–50) | 42.5 (24–80) |
| Right hand dominance (n, %) | 57 (83.8) | 56 (82.4) |
| Painful shoulder (n, %) | ||
| Right | 48 (70.6) | 42 (61.8) |
| Left | 20 (29.4) | 26 (38.2) |
| Duration of episode (weeks, median, IQR) | 30 (21–55) | 33.5 (20–80) |
| Onset of shoulder pain (n, %) | ||
| Injury | 20 (29.4) | 16 (23.5) |
| Previous episodes of shoulder pain (n, %) | ||
| Yes | 17 (25) | 18 (26.5) |
| Number of episodes | 3 (1–5) | 2.5 (1–5) |
| Time since last episode | 12 (7–48) | 24 (7–60) |
| Previous shoulder injection | ||
| Yes (n, %) | 16 (23.5) | 22 (32.3) |
| No of injections (median, range) | 1 (1–3) | 1 (1–3) |
| Improved with injection (n, %) | 13 (81.2) | 13 (59.1) |
| Duration of improvement (weeks, mean, range) | 8 (3–24) | 19 (8–50) |
| Time since last injection (months, mean, range) | 10 (7–15.5) | 15.5 (7–36) |
| Previous physiotherapy for shoulder | ||
| Yes (n, %) | 21 (30.9) | 21 (30.9) |
| Improved with physiotherapy (n, %) | 13 (61.9) | 7 (33.3) |
| Time since physiotherapy (months, mean, range) | 9 (5–48) | 15 (9–24) |
| SPADI Score | Intervention | Control | ||
|---|---|---|---|---|
| n | Mean (SD) | n | Mean (SD) | |
| SPADI–Pain | ||||
| Baseline | 68 | 74.6 (14.2) | 68 | 76.4 (14.7) |
| Week 12 | 50 | 42.6 (32.4) | 54 | 44.7 (29.9) |
| Week 26 | 35 | 43.4 (28.9) | 37 | 44.4 (31.2) |
| Week 52 | 20 | 25.4 (28.2) | 22 | 29.8 (29.7) |
| SPADI–Disability | ||||
| Baseline | 68 | 66.6 (16.4) | 68 | 69.1 (17.2) |
| Week 12 | 50 | 30.0 (29.5) | 54 | 36.0 (27.5) |
| Week 26 | 35 | 31.4 (26.3) | 37 | 36.8 (29.8) |
| Week 52 | 20 | 16.6 (23.7) | 22 | 21.9 (26.7) |
| SPADI–Total Score | ||||
| Baseline | 68 | 69.7 (14.9) | 68 | 71.9 (15.7) |
| Week 12 | 50 | 34.9 (30.2) | 54 | 39.4 (27.5) |
| Week 26 | 35 | 36.0 (26.5) | 37 | 39.7 (29.7) |
| Week 52 | 20 | 20.0 (24.5) | 22 | 25.0 (27.0) |
| SPADI | Mean (Standard Error) | Mean Difference (SE) | |
|---|---|---|---|
| Intervention | Control | ||
| Pain | −27.6 (4.7) | −30.3 (4.3) | 2.7 (6.3) |
| Disability | −33.6 (4.4) | −31.2 (3.9) | −2.4 (5.8) |
| Total Score | −31.3 (4.3) | −30.8 (3.8) | −0.43 (5.7) |
| Resource Item | Unit Cost | Details | Source |
|---|---|---|---|
| Practice GP visit | 35 | Per patient contact lasting 11.7 min. Excluding direct care staff costs & qualifications | Unit costs of Health and Social Care 2014 [21] |
| Accident & Emergency visit | 142 | Weighted average of type 01 emergency medicine, admitted and non-admitted. | NHS reference costs 2013–2014 [22] |
| Physiotherapy attendance | 42 | Non-Admitted, face to face follow-up attendance. | NHS reference costs 2013–2014 [22] |
| Rheumatology | 92 | Non-Admitted, face to face follow-up attendance. | NHS reference costs 2013–2014 [22] |
| Trauma & Orthopaedic outpatient attendance | 105 | Consultant led, non-admitted, follow-up face to face attendance | NHS reference costs 2013–2014 [22] |
| Outpatient Clinic attendance [unspecified] | 109 | weighted average of all outpatient attendances | NHS reference costs 2013–2014 [22] |
| Analgesics | various | - | British National Formulary 68 (January 2015) [23] |
| Service Use | 12 Weeks | 26 Weeks | 52 Weeks | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | Intervention | Control | |||||||
| n | Mean (sd) | n | Mean (sd) | n | Mean (sd) | n | Mean (sd) | n | Mean (sd) | n | Mean (sd) | |
| Practice GP visit | 50 | 4.2 (18.22) | 54 | 5.19 (19.71) | 35 | 18.00 (73.21) | 37 | 3.78 (11.02) | 20 | 7.00 (31.30) | 22 | 0 (0) |
| Accident & Emergency visit | 50 | 0 (0) | 54 | 0 (0) | 35 | 8.11 (48.00) | 37 | 0 (0) | 20 | 0 (0) | 22 | 0 (0) |
| Physiotherapy attendance (non-study treatment) | 50 | 4.2 (29.70) | 54 | 0.78 (5.72) | 35 | 0 (0) | 37 | 0 (0) | 20 | 6.30 (28.17) | 22 | 0 (0) |
| Outpatient attendances | 50 | 4.2 (20.78) | 54 | 0 (0) | 35 | 21.8 (98.21) | 37 | 0 (0) | 20 | 9.2 (41.14) | 22 | 0 (0) |
| Mean health services costs | 50 | 12.60 (47.83) | 54 | 5.96 (20.32) | 35 | 47.91 (138.57) | 37 | 3.78 (11.02) | 20 | 31.70 (115.59) | 22 | 0 (0) |
| Mean difference (bootstrap 95% CI) * | 6.64 (−5.48, 21.25) | 44.13 (5.38, 96.59) | 31.70 (0, 85.75) | |||||||||
| Costs | Intervention | Control | Mean Difference (Bootstrap 95% CI) * | ||
|---|---|---|---|---|---|
| n | Mean (sd) | n | Mean (sd) | ||
| Total health service cost | 17 | 79.65 (206.84) | 17 | 2.06 (8.49) | 77.59 (−1.62, 178.09) |
| Physiotherapy treatment cost | 68 | 74.53 (33.64) | 68 | 188.59 (96.01) | −114.06 (−136.73, −89.38) |
| Overall cost | 17 | 173.53 (206.81) | 17 | 214.53 (83.45) 254.06 (8.49) | −41.00 (−129.20, 79.13) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryans, I.; Galway, R.; Harte, A.; Verghis, R.; Agus, A.; Heron, N.; McKane, R. The Effectiveness of Individual or Group Physiotherapy in the Management of Sub-Acromial Impingement: A Randomised Controlled Trial and Health Economic Analysis. Int. J. Environ. Res. Public Health 2020, 17, 5565. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155565
Ryans I, Galway R, Harte A, Verghis R, Agus A, Heron N, McKane R. The Effectiveness of Individual or Group Physiotherapy in the Management of Sub-Acromial Impingement: A Randomised Controlled Trial and Health Economic Analysis. International Journal of Environmental Research and Public Health. 2020; 17(15):5565. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155565
Chicago/Turabian StyleRyans, Ian, Rhona Galway, Annette Harte, Rejina Verghis, Ashley Agus, Neil Heron, and Roland McKane. 2020. "The Effectiveness of Individual or Group Physiotherapy in the Management of Sub-Acromial Impingement: A Randomised Controlled Trial and Health Economic Analysis" International Journal of Environmental Research and Public Health 17, no. 15: 5565. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155565