Assessing the Impact of Lean Healthcare on Inpatient Care: A Systematic Review

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
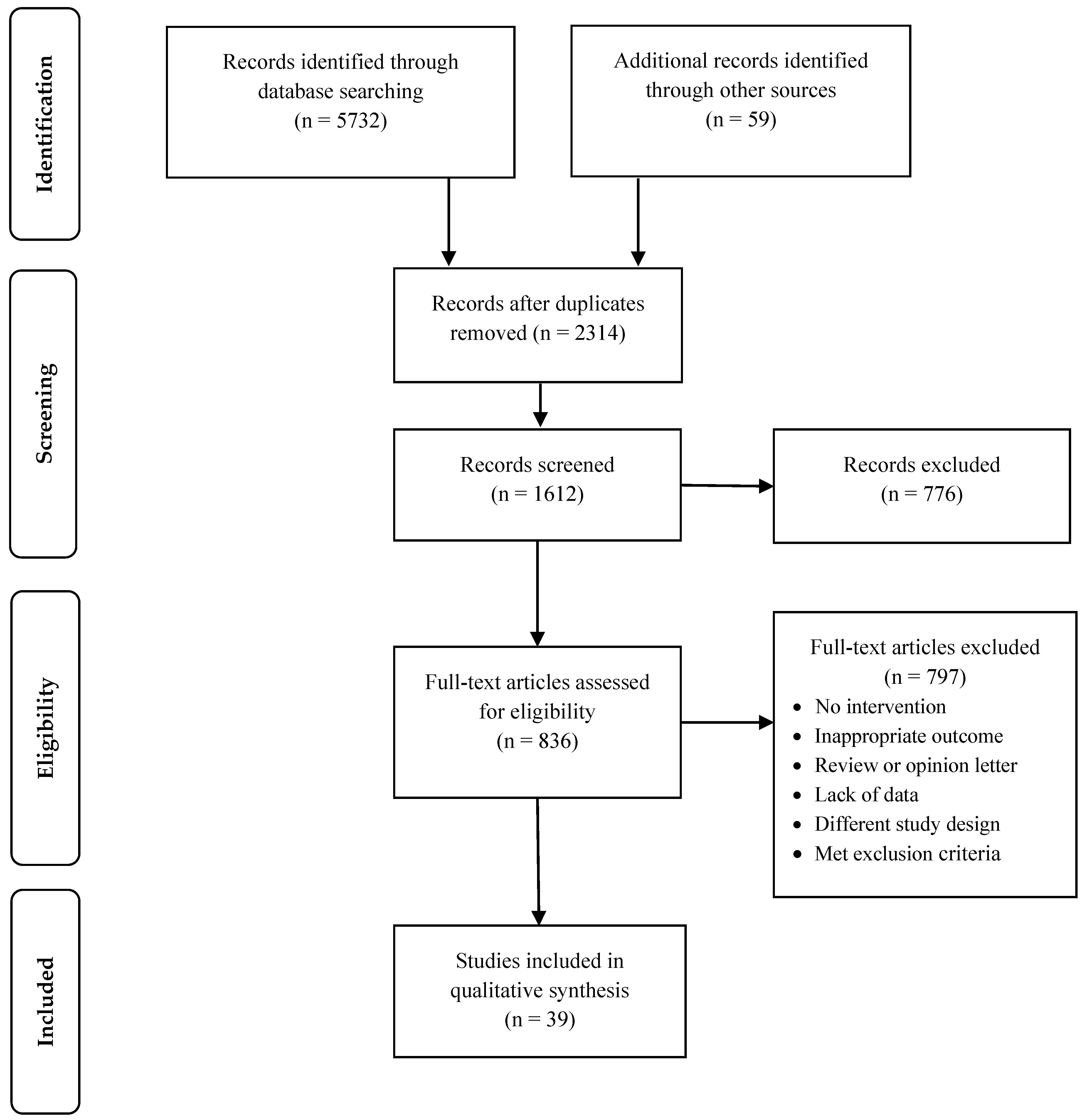
2. Methods
2.1. Data Source and Search Strategy
2.2. Study Selection
2.3. Data Extraction, Analysis and Synthesis
2.4. Risk of Bias
3. Results
4. Discussion
4.1. Length of Stay
4.2. On-Time Starts, Turnover Time, and Turnaround Time
4.3. Boarding Time, Early Discharge, and Readmission
4.4. Patient and Staff Satisfaction
4.5. Perioperative Process
4.6. Lean Healthcare
4.7. Risk of Bias
5. Limitations
6. Conclusions
7. Future Research
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lingaratnam, S.; Murray, D.; Carle, A.; Kirsa, S.W.; Paterson, R.; Rischin, D. Developing a Performance Data Suite to Facilitate Lean Improvement in a Chemotherapy Day Unit. J. Oncol. Pract. 2013, 9, e115–e121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fong, A.J.; Smith, M.; Langerman, A. Efficiency improvement in the operating room. J. Surg. Res. 2016, 204, 371–383. [Google Scholar] [CrossRef] [PubMed]
- Beck, M.J.; Okerblom, D.; Kumar, A.; Bandyopadhyay, S.; Scalzi, L.V. Lean intervention improves patient discharge times, improves emergency department throughput and reduces congestion. Hosp. Pract. 2016, 44, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, M.; Suárez, M.; Asenjo, M.; Bragulat, E. Improvement of emergency department patient flow using lean thinking. Int. J. Qual. Health Care 2018, 30, 250–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicosia, F.M.; Park, L.G.; Gray, C.P.; Yakir, M.J.; Hung, D.Y. Nurses’ Perspectives on Lean Redesigns to Patient Flow and Inpatient Discharge Process Efficiency. Glob. Qual. Nurs. Res. 2018, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- NEJM Catalyst (New England Journal of Medicine) What Is Patient Flow? Available online: https://catalyst.nejm.org/what-is-patient-flow/ (accessed on 20 December 2018).
- Tlapa, D.; Zepeda-Lugo, C.A.; Tortorella, G.L.; Baez-Lopez, Y.A.; Limon-Romero, J.; Alvarado-Iniesta, A.; Rodriguez-Borbon, M.I. Effects of Lean Healthcare on Patient Flow: A Systematic Review. Value Health 2020, 23, 260–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castaldi, M.; Sugano, D.; Kreps, K.; Cassidy, A.; Kaban, J. Lean philosophy and the public hospital. Perioper. Care Oper. Room Manag. 2016, 3, 25–28. [Google Scholar] [CrossRef]
- Dickson, E.W.; Anguelov, Z.; Vetterick, D.; Eller, A.; Singh, S. Use of Lean in the Emergency Department: A Case Series of 4 Hospitals. Ann. Emerg. Med. 2009, 54, 504–510. [Google Scholar] [CrossRef]
- Rutman, L.; Stone, K.; Reid, J.; Woodward, G.A.T.; Migita, R. Improving patient flow using lean methodology: An emergency medicine experience. Curr. Treat. Options Pediatr. 2015, 1, 359–371. [Google Scholar] [CrossRef] [Green Version]
- The Centers for Medicare and Medicaid Services (CMS) Medicare Hospital Compare Overview. Available online: https://www.medicare.gov/hospitalcompare/About/What-Is-HOS.html (accessed on 20 March 2019).
- Ieraci, S.; Digiusto, E.; Sonntag, P.; Dann, L.; Fox, D. Streaming by case complexity: Evaluation of a model for emergency department Fast Track. EMA Emerg. Med. Australas. 2008, 20, 241–249. [Google Scholar] [CrossRef]
- King, D.L.; Ben-Tovim, D.I.; Bassham, J. Redesigning emergency department patient flows: Application of Lean Thinking to health care. Emerg. Med. Australas. 2006, 18, 391–397. [Google Scholar] [CrossRef]
- Kelly, A.-M.; Bryant, M.; Cox, L.; Jolley, D. Improving emergency department efficiency by patient streaming to outcomes-based teams. Aust. Health Rev. 2007, 31, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murrell, K.L.; Offerman, S.R.; Kauffman, M.B. Applying Lean: Implementation of a Rapid Triage and Treatment System. West. J. Emerg. Med. 2011, 12, 184–191. [Google Scholar] [PubMed]
- Vermeulen, M.J.; Stukel, T.A.; Guttmann, A.; Rowe, B.H.; Zwarenstein, M.; Golden, B.; Nigam, A.; Anderson, G.; Bell, R.S.; Schull, M.J. Evaluation of an emergency department lean process improvement program to reduce length of stay. Ann. Emerg. Med. 2014, 64, 427–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trzeciak, S.; Mercincavage, M.; Angelini, C.; Cogliano, W.; Damuth, E.; Roberts, B.W.; Zanotti, S.; Mazzarelli, A.J. Lean Six Sigma to Reduce Intensive Care Unit Length of Stay and Costs in Prolonged Mechanical Ventilation. J. Healthc. Qual. 2018, 40, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Brunsman, A.C. Using lean methodology to optimize time to antibiotic administration in patients with sepsis. Am. J. Health Pharm. 2018, 75, S13–S23. [Google Scholar] [CrossRef]
- Artenstein, A.W.; Rathlev, N.K.; Neal, D.; Townsend, V.; Vemula, M.; Goldlust, S.; Schmidt, J.; Visintainer, P.; Albert, M.; Alli, G.; et al. Decreasing Emergency Department Walkout Rate and Boarding Hours by Improving Inpatient Length of Stay. West. J. Emerg. Med. 2017, 18, 982–992. [Google Scholar] [CrossRef] [Green Version]
- Molla, M.; Warren, D.S.; Stewart, S.L.; Stocking, J.; Johl, H.; Sinigayan, V. A Lean Six Sigma Quality Improvement Project Improves Timeliness of Discharge from the Hospital. Jt. Comm. J. Qual. Patient Saf. 2018, 44, 401–412. [Google Scholar] [CrossRef]
- Collar, R.M.; Shuman, A.G.; Feiner, S.; McGonegal, A.K.; Heidel, N.; Duck, M.; McLean, S.A.; Billi, J.E.; Healy, D.W.; Bradford, C.R. Lean management in academic surgery. J. Am. Coll. Surg. 2012, 214, 928–936. [Google Scholar] [CrossRef]
- Cima, R.R.; Brown, M.J.; Hebl, J.R.; Moore, R.; Rogers, J.C.; Kollengode, A.; Amstutz, G.J.; Weisbrod, C.A.; Narr, B.J.; Deschamps, C. Use of Lean and Six Sigma Methodology to Improve Operating Room Efficiency in a High-Volume Tertiary-Care Academic Medical Center. J. Am. Coll. Surg. 2011, 213, 83–92. [Google Scholar] [CrossRef]
- Singh, S.; Remya, T.; Shijo, T.M.; Nair, D.; Nair, P. Lean six sigma application in reducing nonproductive time in operation theaters. J. Natl. Accredit. Board Hosp. Healthc. Provid. 2014, 1, 1–7. [Google Scholar] [CrossRef]
- Tagge, E.P.; Thirumoorthi, A.S.; Lenart, J.; Garberoglio, C.; Mitchell, K.W. Improving operating room efficiency in academic children’s hospital using Lean Six Sigma methodology. J. Pediatr. Surg. 2017, 52, 1040–1044. [Google Scholar] [CrossRef] [PubMed]
- Jimmerson, C.; Weber, D.; Sobek, D. Reducing waste and errors: Piloting lean principles at Intermountain Healthcare. J. Qual. Patient Saf. 2005, 31, 249–257. [Google Scholar] [CrossRef]
- Hassanain, M.; Zamakhshary, M.; Farhat, G.; Al-Badr, A. Use of Lean methodology to improve operating room efficiency in hospitals across the Kingdom of Saudi Arabia. Int. J. Health Plan. Manag. 2016, 32, 133–146. [Google Scholar] [CrossRef]
- Bender, J.S.; Nicolescu, T.O.; Hollingsworth, S.B.; Murer, K.; Wallace, K.R.; Ertl, W.J. Improving operating room efficiency via an interprofessional approach. Am. J. Surg. 2015, 209, 447–450. [Google Scholar] [CrossRef]
- Toledo, A.; Carroll, T.; Arnold, E.; Tulu, Z.; Caffey, T.; Kearns, L.; Gerber, D. Reducing liver transplant length of stay: A lean six sigma approach. Prog. Transpl. 2013, 23, 350–364. [Google Scholar] [CrossRef]
- Sirvent, J.M.; Gil, M.; Alvarez, T.; Martin, S.; Vila, N.; Colomer, M.; March, E.; Loma-Osorio, P.; Metje, T. Lean techniques to improve flow of critically ill patients in a health region with its epicenter in the intensive care unit of a reference hospital. Med. Intensiva (Engl. Ed.) 2016, 40, 266–272. [Google Scholar] [CrossRef]
- Medicare Payment Advisory Commission A Data Book: Health Care Spending and the Medicare Program. Available online: http://www.medpac.gov/docs/default-source/data-book/jun19_databook_entirereport_sec.pdf?sfvrsn=0 (accessed on 15 April 2020).
- Ceschia, S.; Schaerf, A. Dynamic patient admission scheduling with operating room constraints, flexible horizons, and patient delays. J. Sched. 2016, 19, 377–389. [Google Scholar] [CrossRef]
- Demeester, P.; Souffriau, W.; De Causmaecker, P.; Vanden Berghe, G. A hybrid tabu search algorithm for automatically assigning patients to beds. Artif. Intell. Med. 2010, 48, 61–70. [Google Scholar] [CrossRef]
- Guido, R.; Solina, V.; Mirabelli, G.; Conforti, D. Offline Patient Admission, Room and Surgery Scheduling Problems. In New Trends in Emerging Complex Real Life Problems; Daniele, P., Scrimali, L., Eds.; Springer International Publishing: Taormina, Italy, 2018; pp. 275–283. [Google Scholar]
- Shortell, S.; Bennett, C.; Gayle, B. Assessing the Impact of Continuous Quality Improvement on Clinical Practice: What It Will Take to Accelerate Progress. Milbank Q. 1998, 76, 593–624. [Google Scholar] [CrossRef] [Green Version]
- Crema, M.; Verbano, C. How to combine lean and safety management in health care processes: A case from Spain. Saf. Sci. 2015, 79, 63–71. [Google Scholar] [CrossRef]
- Luce, B.R. The Value Challenge: Examining the Transformative Strategies to Measure or Evaluate the Value of Health Care Interventions. Value Health 2018, 21, 373–374. [Google Scholar] [CrossRef] [Green Version]
- Chan, H.; Lo, S.; Lee, L.; Lo, W.; Yu, W.; Wu, Y.; Ho, S.; Yeung, R.; Chan, J. Lean techniques for the improvement of patients’ flow in emergency department. World J. Emerg. Med. 2014, 5, 24–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, R.I. Lean Methodology in Health Care. Chest 2018, 154, 1448–1454. [Google Scholar] [CrossRef] [PubMed]
- Bercaw, R. Taking Improvement from the Assembly Line to Healthcare: The Application of Lean within the Healthcare Industry, 1st ed.; CRC Press: Boca Raton, FL, USA, 2011. [Google Scholar]
- Zidel, T.G. Lean Guide to Transforming Healthcare: How to Implement Lean Principles in Hospitals, Medical Offices, Clinics, and Other Healthcare Organizations, 1st ed.; Quality Press: Milwaukee, WI, USA, 2006. [Google Scholar]
- Westwood, N.; James-Moore, M.; Cooke, M. Going Lean in the NHS. Available online: https://www.england.nhs.uk/improvement-hub/wp-content/uploads/sites/44/2017/11/Going-Lean-in-the-NHS.pdf (accessed on 20 January 2020).
- Montesarchio, V.; Grimaldi, A.M.; Fox, B.A.; Rea, A.; Marincola, F.M.; Ascierto, P.A. Lean oncology: A new model for oncologists. J. Transl. Med. 2012, 10, 1–3. [Google Scholar] [CrossRef] [Green Version]
- De Souza, L. Trends and approaches in lean healthcare. Lead. Health Serv. 2009, 22, 121–139. [Google Scholar] [CrossRef]
- Costa, L.B.M.; Godinho Filho, M. Lean healthcare: Review, classification and analysis of literature. Prod. Plan. Control 2016, 27, 823–836. [Google Scholar] [CrossRef]
- Institute of Medicine. The Healthcare Imperative: Lowering Costs and Improving Outcomes; Yong, P., Saunders, R., Olsen, L., Workshop, S., Eds.; The National Academies Press: Washington, DC, USA, 2010; ISBN 9780309144339. [Google Scholar]
- Shortell, S.; Blodgett, J.; Rundall, T.; Kralovec, P. Use of Lean and Related Transformational Performance Improvement Systems in Hospitals in the United States: Results from a National Survey. Jt. Comm. J. Qual. Patient Saf. 2018, 44, 574–582. [Google Scholar] [CrossRef]
- Hseng-Long, Y.; Chin-Sen, L.; Chao-Ton, S.; Pa-Chun, W. Applying lean six sigma to improve healthcare: An empirical study. Afr. J. Bus. Manag. 2011, 5, 12356–12370. [Google Scholar] [CrossRef]
- Gayed, B.; Black, S.; Daggy, J.; Munshi, I.A. Redesigning a Joint Replacement Program using Lean Six Sigma in a Veterans Affairs Hospital. JAMA Surg. 2013, 148, 1050–1056. [Google Scholar] [CrossRef] [Green Version]
- Cromwell, S.; Chiasson, D.A.; Cassidy, D.; Somers, G.R. Improving Autopsy Report Turnaround Times by Implementing Lean Management Principles. Pediatr. Dev. Pathol. 2018, 21, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duska, L.R.; Mueller, J.; Lothamer, H.; Pelkofski, E.B.; Novicoff, W.M. Lean methodology improves efficiency in outpatient academic Gynecologic Oncology clinics. Gynecol. Oncol. 2015, 138, 707–711. [Google Scholar] [CrossRef] [PubMed]
- Damle, A.; Andrew, N.; Kaur, S.; Orquiola, A.; Alavi, K.; Steele, S.R.; Maykel, J. Elimination of waste: Creation of a successful Lean colonoscopy program at an academic medical center. Surg. Endosc. Other Interv. Tech. 2016, 30, 3071–3076. [Google Scholar] [CrossRef] [PubMed]
- Weaver, A.; Greeno, C.G.; Goughler, D.H.; Yarzebinski, K.; Zimmerman, T.; Anderson, C. The impact of system level factors on treatment timeliness: Utilizing the toyota production system to implement direct intake scheduling in a semi-rural community mental health clinic. J. Behav. Health Serv. Res. 2013, 40, 294–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Vliet, E.; Sermeus, W.; van Gaalen, C.M.; Sol, J.; Vissers, J. Efficacy and efficiency of a lean cataract pathway: A comparative study. Qual. Saf. Health Care 2010, 19, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Vest, J.R.; Gamm, L.D. A critical review of the research literature on Six Sigma, Lean and StuderGroup’s Hardwiring Excellence in the United States: The need to demonstrate and communicate the effectiveness of transformation strategies in healthcare. Implement Sci. 2009, 4, 35. [Google Scholar] [CrossRef] [Green Version]
- Curatolo, N.; Lamouri, S.; Huet, J.C.; Rieutord, A. A critical analysis of Lean approach structuring in hospitals. Bus. Process Manag. J. 2013, 20, 433–454. [Google Scholar] [CrossRef]
- Holden, R.J. Lean thinking in emergency departments: A critical review. Ann. Emerg. Med. 2011, 57, 265–278. [Google Scholar] [CrossRef]
- Nicolay, C.R.; Purkayastha, S.; Greenhalgh, A.; Benn, J.; Chaturvedi, S.; Phillips, N.; Darzi, A. Systematic review of the application of quality improvement methodologies from the manufacturing industry to surgical healthcare. Br. J. Surg. 2012, 99, 324–335. [Google Scholar] [CrossRef]
- Mason, S.E.E.; Nicolay, C.R.R.; Darzi, A. The use of Lean and Six Sigma methodologies in surgery: A systematic review. Surgeon 2015, 13, 91–100. [Google Scholar] [CrossRef]
- Amaratunga, T.; Dobranowski, J. Systematic Review of the Application of Lean and Six Sigma Quality Improvement Methodologies in Radiology. J. Am. Coll. Radiol. 2016, 13, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Dellifraine, J.L.; Langabeer, J.R.; Nembhard, I.M. Assessing the evidence of six sigma and lean in the health care industry. Qual. Manag. Health Care 2010, 19, 211–225. [Google Scholar] [CrossRef] [PubMed]
- Hussey, P.S.; De Vries, H.; Romley, J.; Wang, M.C.; Chen, S.S.; Shekelle, P.G.; McGlynn, E.A. A systematic review of health care efficiency measures: Health care efficiency. Health Serv. Res. 2009, 44, 784–805. [Google Scholar] [CrossRef] [PubMed]
- Mazzocato, P.; Savage, C.; Brommels, M.; Aronsson, H.; Thor, J. Lean thinking in healthcare: A realist review of the literature. Qual. Saf. Health Care 2010, 19, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Andersen, H.; Røvik, K.A.; Ingebrigtsen, T. Lean thinking in hospitals: Is there a cure for the absence of evidence? A systematic review of reviews. BMJ Open 2014, 4, 3505. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, E.; Ortiz, N. Lean Healthcare: Una revisión bibliográfica y futuras líneas de investigación. Sci. Tech. 2015, 20, 358–365. [Google Scholar] [CrossRef] [Green Version]
- D’Andreamatteo, A.; Ianni, L.; Lega, F.; Sargiacomo, M. Lean in healthcare: A comprehensive review. Health Policy (N. Y.) 2015, 119, 1197–1209. [Google Scholar] [CrossRef]
- Rotter, T.; Plishka, C.; Lawal, A.; Harrison, L.; Sari, N.; Goodridge, D.; Flynn, R.; Chan, J.; Fiander, M.; Poksinska, B.; et al. What Is Lean Management in Health Care? Development of an Operational Definition for a Cochrane Systematic Review. Eval. Health Prof. 2018, 42, 366–390. [Google Scholar] [CrossRef]
- Ali, M.; Wang, W.; Chaudhry, N.; Geng, Y. Hospital waste management in developing countries: A mini review. Waste Manag. Res. 2017, 35, 581–592. [Google Scholar] [CrossRef]
- Crema, M.; Verbano, C. Lean Management to support Choosing Wisely in healthcare: The first evidence from a systematic literature review. Int. J. Qual. Health Care 2017, 29, 889–895. [Google Scholar] [CrossRef]
- Tasdemir, C.; Gazo, R. A systematic literature review for better understanding of lean driven sustainability. Sustainability 2018, 10, 2544. [Google Scholar] [CrossRef] [Green Version]
- Maijala, R.; Eloranta, S.; Reunanen, T.; Ikonen, T.S. Successful Implementation of Lean as a Managerial Principle in Health Care: A Conceptual Analysis From Systematic Literature Review. Int. J. Technol. Assess. Health Care 2018, 34, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Terra, J.D.R.; Berssaneti, F.T. Application of lean healthcare in hospital services: A review of the literature (2007 to 2017). Production 2018, 28, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Habidin, N.F.; Shazali, N.A.; Ali, N.; Khaidir, N.A.; Jamaludin, N.H. Exploring lean healthcare practice and supply chain innovation for Malaysian healthcare industry. Int. J. Bus. Excell. 2014, 7, 394. [Google Scholar] [CrossRef]
- Shazali, N.A.N.; Habidin, N.N.F.; Ali, N.; Khaidir, N.A.; Jamaludin, N.H.; Jamaludin, H. Lean Healthcare Practice and Healthcare Performance in Malaysian Healthcare Industry. Int. J. Sci. Res. Publ. 2013, 3, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Jain, V.; Ajmera, P. Modelling of the factors affecting lean implementation in healthcare using structural equation modelling. Int. J. Syst. Assur. Eng. Manag. 2019, 10, 563–575. [Google Scholar] [CrossRef]
- Johnson, D.M.; Russell, R.S. SEM of service quality to predict overall patient satisfaction in medical clinics: A case study. Qual. Manag. J. 2015, 22, 18–36. [Google Scholar] [CrossRef]
- Habidin, N.F.; Che Omar, C.M.Z.; Ibrahim, N. Confirmatory Factor Analysis of Lean Healthcare Practices in Malaysian Healthcare Industry. J. Cotempor. Issues Thought 2012, 2, 17–29. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D.; et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Effective Practice and Organisation of Care (EPOC) EPOC Taxonomy. Available online: https://epoc.cochrane.org/epoc-taxonomy (accessed on 5 February 2020).
- Cochrane Effective Practice and Organisation of Care (EPOC). What Outcomes Should Be Reported in Cochrane Effective Practice and Organisation of Care (EPOC) Reviews? Available online: http://epoc.cochrane.org/resources/epoc-resources-review-authors (accessed on 15 November 2018).
- Sterne, J.; Higgins, J.; Elbers, R.; Reeves, B. The Development Group for ROBINS-I Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I): Detailed Guidance; Cochrane Bias Methods Group: Bristol, UK, 2016. [Google Scholar]
- Sterne, J.; Hernán, M.; Reeves, B.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.; Ansari, M.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Hernán, M.A.; McAleenan, A.; Reeves, B.C.; Higgins, J.P. Assessing risk of bias in a non-randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions; Cochrane: London, UK, 2019; pp. 205–228. [Google Scholar]
- De la Lama, J.; Fernandez, J.; Punzano, J.A.A.; Nicolas, M.; Nin, S.; Mengual, R.; Ramirez, J.A.A.; Raya, A.-L.L.; Ramos, G. Using Six Sigma tools to improve internal processes in a hospital center through three pilot projects. Int. J. Healthc. Manag. 2013, 6, 158–167. [Google Scholar] [CrossRef]
- Burkitt, K.H.; Mor, M.K.; Jain, R.; Kruszewski, M.S.; Mccray, E.E.; Moreland, M.E.; Muder, R.R.; Obrosky, D.; Mary, S.; Wilson, M.A.; et al. Toyota production system quality improvement initiative improves perioperative antibiotic therapy. Am. J. Manag. Care 2009, 15, 633–642. [Google Scholar] [PubMed]
- Yousri, T.A.A.; Khan, Z.; Chakrabarti, D.; Fernandes, R.; Wahab, K. Lean thinking: Can it improve the outcome of fracture neck of femur patients in a district general hospital? Injury 2011, 42, 1234–1237. [Google Scholar] [CrossRef]
- New, S.; Hadi, M.; Pickering, S.; Robertson, E.; Morgan, L.; Griffin, D.; Collins, G.; Rivero-Arias, O.; Catchpole, K.; McCulloch, P. Lean Participative Process Improvement: Outcomes and Obstacles in Trauma Orthopaedics. PLoS ONE 2016, 11, e0152360. [Google Scholar] [CrossRef]
- Beck, M.J.; Gosik, K. Redesigning an inpatient pediatric service using Lean to improve throughput efficiency. J. Hosp. Med. 2015, 10, 220–227. [Google Scholar] [CrossRef]
- Johnson, A.E.; Winner, L.; Simmons, T.; Eid, S.M.; Hody, R.; Sampedro, A.; Augustine, S.; Sylvester, C.; Parakh, K. Using Innovative Methodologies from Technology and Manufacturing Companies to Reduce Heart Failure Readmissions. Am. J. Med. Qual. 2016, 31, 272–278. [Google Scholar] [CrossRef]
- Vose, C.; Reichard, C.; Pool, S.; Snyder, M.; Burmeister, D. Using LEAN to improve a segment of emergency department flow. J. Nurs. Adm. 2014, 44, 558–563. [Google Scholar] [CrossRef]
- Sorensen, L.; Idemoto, L.; Streifel, J.; Williams, B.; Mecklenburg, R.; Blackmore, C. A multifaceted intervention to improve the quality of care for patients undergoing total joint arthroplasty. BMJ Open Qual. 2019, 8, e000664. [Google Scholar] [CrossRef] [Green Version]
- Moo-Young, J.A.; Sylvester, F.A.; Dancel, R.D.; Galin, S.; Troxler, H.; Bradford, K.K. Impact of a Quality Improvement Initiative to Optimize the Discharge Process of Pediatric Gastroenterology Patients at an Academic Children’s Hospital. Pediatr. Qual. Saf. 2019, 4, e213. [Google Scholar] [CrossRef] [PubMed]
- Farrokhi, F.R.; Gunther, M.; Williams, B.; Blackmore, C.C. Application of Lean Methodology for Improved Quality and Efficiency in Operating Room Instrument Availability. J. Healthc. Qual. 2015, 37, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Sayeed, Z.; Anoushiravani, A.; El-Othmani, M.; Barinaga, G.; Sayeed, Y.; Cagle, P.; Saleh, K.J. Implementation of a hip fracture care pathway using lean six sigma methodology in a level I trauma center. J. Am. Acad. Orthop. Surg. 2018, 26, 881–893. [Google Scholar] [CrossRef] [PubMed]
- Wannemuehler, T.J.; Elghouche, A.N.; Kokoska, M.S.; Deig, C.R.; Matt, B.H. Impact of Lean on surgical instrument reduction: Less is more. Laryngoscope 2015, 125, 2810–2815. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.; Lyons, C.; Whyte, R. Optimizing nursing time in a day care unit: Quality improvement using Lean Six Sigma methodology. Int. J. Qual. Health Care 2019, 31, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Niemeijer, G.; Trip, A.; Ahaus, K.; Does, R.; Wendt, K. Quality in trauma care: Improving the discharge procedure of patients by means of Lean Six Sigma. J. Trauma Inj. Infect. Crit. Care 2010, 69, 614–618. [Google Scholar] [CrossRef] [Green Version]
- Iannettoni, M.D.; Lynch, W.R.; Parekh, K.R.; McLaughlin, K.A. Kaizen method for esophagectomy patients: Improved quality control, outcomes, and decreased costs. Ann. Thorac. Surg. 2011, 91, 1011–1018. [Google Scholar] [CrossRef]
- Montella, E.; Di Cicco, M.V.; Ferraro, A.; Centobelli, P.; Raiola, E.; Triassi, M.; Improta, G. The application of Lean Six Sigma methodology to reduce the risk of healthcare–associated infections in surgery departments. J. Eval. Clin. Pract. 2017, 23, 530–539. [Google Scholar] [CrossRef]
- Fairbanks, C.B. Using six sigma and lean methodologies to improve or throughput. AORN J. 2007, 86, 73–82. [Google Scholar] [CrossRef]
- Niemeijer, G.C.; Flikweert, E.; Trip, A.; Does, R.; Ahaus, K.; Boot, A.; Wendt, K. The usefulness of lean six sigma to the development of a clinical pathway for hip fractures. J. Eval. Clin. Pract. 2013, 19, 909–914. [Google Scholar] [CrossRef]
- Cerfolio, R.J.; Ferrari-Light, D.; Ren-Fielding, C.; Fielding, G.; Perry, N.; Rabinovich, A.; Saraceni, M.; Fitzpatrick, M.; Jain, S.; Pachter, H.L. Improving Operating Room Turnover Time in a New York City Academic Hospital via Lean. Ann. Thorac. Surg. 2019, 107, 1011–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ankrum, A.L.; Neogi, S.; Morckel, M.A.; Wilhite, A.W.; Li, Z.; Schaffzin, J.K. Reduced isolation room turnover time using Lean methodology. Infect. Control Hosp. Epidemiol. 2019, 40, 1151–1156. [Google Scholar] [CrossRef] [PubMed]
- Peter, A.; Parvathaneni, A.; Wilson, C.; Tankalavage, T.; Cheriyath, P. Wheels on Time: A Six Sigma Approach to Reduce Delay in Operating Room Starting Time. Surg. Curr. Res. 2011, 1, 1–4. [Google Scholar] [CrossRef]
- Allen, T.T.; Tseng, S.-H.H.; Swanson, K.; McClay, M.A. Improving the Hospital Discharge Process with Six Sigma Methods. Qual. Eng. 2009, 22, 13–20. [Google Scholar] [CrossRef]
- El-Eid, G.R.; Kaddoum, R.; Tamim, H.; Hitti, E.A. Improving hospital discharge time. Medicine (U. S.) 2015, 94, e633. [Google Scholar] [CrossRef] [PubMed]
- Vijay, S.A. Reducing and optimizing the cycle time of patients discharge process in a hospital using six sigma dmaic approach. Int. J. Qual. Res. 2014, 8, 169–182. [Google Scholar]
- Deldar, R.; Soleimani, T.; Harmon, C.; Stevens, L.H.; Sood, R.; Tholpady, S.S.; Chu, M.W. Improving first case start times using Lean in an academic medical center. Am. J. Surg. 2017, 213, 991–995. [Google Scholar] [CrossRef]
- Adams, R.; Warner, P.; Hubbard, B.; Goulding, T. Decreasing Turnaround Time between General Surgery Cases: A Six Sigma Initiative. J. Nurs. Adm. 2004, 34, 140–148. [Google Scholar] [CrossRef] [Green Version]
- Joubert, B.; Bam, W. Review and classification of Lean project aims in hospitals. In Proceedings of the 2019 IEEE International Conference on Engineering, Technology and Innovation, ICE/ITMC, Valbonne Sophia-Antipolis, France, 17–19 June 2019. [Google Scholar]
- Franklin, J.; Franklin, T. Improving Preoperative Throughput. J. PeriAnesthesia Nurs. 2017, 32, 38–44. [Google Scholar] [CrossRef]
- Dexter, E.U.; Dexter, F.; Masursky, D.; Garver, M.P.; Nussmeier, N.A. Both Bias and Lack of Knowledge Influence Organizational Focus on First Case of the Day Starts. Anesth. Analg. 2009, 108, 1257–1261. [Google Scholar] [CrossRef]
- Foglia, R.; Ruiz, J.; Burkhalter, L. An Evolutionary Change in First Case on Time Starts Using Perioperative Process Improvement, Communication and Enhanced Data Integrity. Glob. J. Perioper. Med. 2017, 1, 013–016. [Google Scholar] [CrossRef] [Green Version]
- NHS Plan, Do, Study, Act (PDSA) Cycles and the Model for Improvement. Available online: https://improvement.nhs.uk/documents/2142/plan-do-study-act.pdf (accessed on 20 April 2020).
- Fletcher, D.; Edwards, D.; Tolchard, S.; Baker, R.; Berstock, J. Improving theatre turnaround time. BMJ Qual. Improv. Rep. 2017, 6, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overdyk, F.J.; Harvey, S.C.; Fishman, R.L.; Shippey, F. Successful strategies for improving operating room efficiency at academic institutions. Anesth. Analg. 1998, 86, 896–906. [Google Scholar] [CrossRef] [PubMed]
- Gottschalk, M.B.; Hinds, R.M.; Muppavarapu, R.C.; Brock, K.; Sapienza, A.; Paksima, N.; Capo, J.T.; Yang, S.S. Factors Affecting Hand Surgeon Operating Room Turnover Time. Hand 2016, 11, 489–494. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.M.; Padmanabhan, S.P.; Schallhorn, J.; Parikh, N.; Ramanathan, S. Improved utilization of operating room time for trainee cataract surgery in a public hospital setting. J. Cataract Refract. Surg. 2018, 44, 186–189. [Google Scholar] [CrossRef]
- The Joint Commission. The “patient flow standard” and the 4-hour recommendation. Jt. Comm. Perspect. 2013, 33, 1–4. [Google Scholar]
- Powell, E.S.; Khare, R.K.; Venkatesh, A.K.; Van Roo, B.D.; Adams, J.G.; Reinhardt, G. The relationship between inpatient discharge timing and emergency department boarding. J. Emerg. Med. 2012, 42, 186–196. [Google Scholar] [CrossRef]
- OECD. OECD Health at A Glance 2019; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Durvasula, R.; Kayihan, A.; Del Bene, S.; Granich, M.; Parker, G.; Anawalt, B.D.; Staiger, T. A Multidisciplinary Care Pathway Significantly Increases the Number of Early Morning Discharges in a Large Academic Medical Center. Qual. Manag. Health Care 2015, 24, 45–51. [Google Scholar] [CrossRef]
- National Guideline Centre Bed occupancy. Emergency and Acute Medical Care Contents; National Guideline Centre, Ed.; National Institute for Health and Care Excellence: London, UK, 2018; pp. 1–22. ISBN 9781473127418. [Google Scholar]
- Kociol, R.D.; Peterson, E.D.; Hammill, B.G.; Flynn, K.E.; Heidenreich, P.A.; Piña, I.L.; Lytle, B.L.; Albert, N.M.; Curtis, L.H.; Fonarow, G.C.; et al. National survey of hospital strategies to reduce heart failure readmissions findings from the get with the guidelines-heart failure registry. Circ. Hear. Fail. 2012, 5, 680–687. [Google Scholar] [CrossRef] [Green Version]
- Friebel, R.; Hauck, K.; Aylin, P.; Steventon, A. National trends in emergency readmission rates: A longitudinal analysis of administrative data for England between 2006 and 2016. BMJ Open 2018, 8, e020325. [Google Scholar] [CrossRef] [Green Version]
- National Health Service (NHS Digital) Emergency Readmissions within 30 Days of Discharge from Hospital. Available online: https://digital.nhs.uk/data-and-information/publications/clinical-indicators/ccg-outcomes-indicator-set/current/domain-3-helping-people-to-recover-from-episodes-of-ill-health-or-following-injury-ccg/3-2-emergency-readmissions-within-30-days-of-discharge-f (accessed on 24 April 2020).
- Haber, S.; Beil, H.; Adamache, W.; Amico, P.; Beadles, C.; Berzin, O.; Maggie Cole-Beebe, M.; Greenwald, L.; Kim, K.; Lauren Mittman, M.; et al. Evaluation of the Maryland All-Payer Mode; RTI International: Waltham, MA, USA; p. 2017.
- Department of Health A Simple Guide to Payment by Results. Available online: www.dh.gov.uk/pbr (accessed on 15 April 2020).
- Marley, K.A.; Collier, D.A.; Goldstein, S.M. The role of clinical and process quality in achieving patient satisfaction in hospitals. Decis. Sci. 2004, 35, 349–368. [Google Scholar] [CrossRef]
- Chiarini, A.; Cherrafi, A. Improving patient satisfaction using lean manufacturing tools. In Case studies from Italy. In Proceedings of the 20th Excellence in Services International Conference, Verona, Italy, 7–8 September 2017; pp. 177–182. [Google Scholar]
- Skeldon, S.C.; Simmons, A.; Hersey, K.; Finelli, A.; Jewett, M.A.; Zlotta, A.R.; Fleshner, N.E. Lean methodology improves efficiency in outpatient academic uro-oncology clinics. Urology 2014, 83, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Dansky, K.H.; Miles, J. Patient satisfaction with ambulatory healthcare services: Waiting time and filling time. Hosp. Health Serv. Adm. 1997, 42, 165–177. [Google Scholar] [PubMed]
- Mazzocato, P.; Holden, R.J.; Brommels, M.; Aronsson, H.; Bäckman, U.; Elg, M.; Thor, J. How does lean work in emergency care? A case study of a lean-inspired intervention at the Astrid Lindgren Children’s hospital, Stockholm, Sweden. BMC Health Serv. Res. 2012, 12, 13. [Google Scholar] [CrossRef] [Green Version]
- Shendell-Falik, N.; Feinson, M.; Mohr, B.J. Enhancing patient safety: Improving the patient handoff process through appreciative inquiry. J. Nurs. Adm. 2007, 37, 95–104. [Google Scholar] [CrossRef]
- Ayaad, O.; Haroun, A.; Yaseen, R.; Thiab, F.; Al-Rawashdeh, K.; Mohammad, I.; Aqtash, M.; Qadumi, S.; Altantawi, Y.; Nairat, A. Improving nurses’ hand-offprocess on oncology setting using lean management principles. Asian Pac. J. Cancer Prev. 2019, 20, 1563–1570. [Google Scholar] [CrossRef] [Green Version]
- Verbano, C.; Crema, M. Applying lean management to reduce radiology turnaround times for emergency department. Int. J. Health Plan. Manag. 2019, 34, e1711–e1722. [Google Scholar] [CrossRef]
- Ulhassan, W.; Sandahl, C.; Westerlund, H.; Henriksson, P.; Bennermo, M.; Schwarz, V.T.U.; Thor, J. Antecedents and characteristics of lean thinking implementation in a swedish hospital: A case study. Qual. Manag. Health Care 2013, 22, 48–61. [Google Scholar] [CrossRef]
- Simons, P.; Backes, H.; Bergs, J.; Emans, D.; Johannesma, M.; Jacobs, M.; Marneffe, W.; Vandijck, D. The effects of a lean transition on process times, patients and employees. Int. J. Health Care Qual. Assur. 2017, 30, 103–118. [Google Scholar] [CrossRef]
- Albanese, C.T.; Aaby, D.; Platchek, T. Advanced Lean In Healthcare; CreateSpace Independent Publishing Platform: Stanford, CA, USA, 2014; ISBN 1-4961-4189-X. [Google Scholar]
- Colosi, B. 2020 NSI National Health Care Retention & RN Staffing Report. Available online: www.nsinursingsolutions.com (accessed on 20 April 2020).
- Hayes, L.J.; O’Brien-Pallas, L.; Duffield, C.; Shamian, J.; Buchan, J.; Hughes, F.; Spence Laschinger, H.K.; North, N.; Stone, P.W. Nurse turnover: A literature review. Int. J. Nurs. Stud. 2006, 43, 237–263. [Google Scholar] [CrossRef]
- Ayalon, O.; Liu, S.; Flics, S.; Cahill, J.; Juliano, K.; Cornell, C.N. A Multimodal Clinical Pathway Can Reduce Length of Stay After Total Knee Arthroplasty. HSS J. 2011, 7, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohn, L.T.; Corrigan, J.; Donaldson, M.S. To Err is Human: Building A Safer Health System; Kohn, L., Corrigan, J., Donaldson, M., Eds.; National Academy Press: Washington, DC, USA, 2000; ISBN 978-0-309-26174-6. [Google Scholar]
- Van Citters, A.D.; Fahlman, C.; Goldmann, D.A.; Lieberman, J.R.; Koenig, K.M.; DiGioia, A.M.; O’Donnell, B.; Martin, J.; Federico, F.A.; Bankowitz, R.A.; et al. Developing a pathway for high-value, patient-centered total joint arthroplasty. Clin. Orthop. Relat. Res. 2014, 472, 1619–1635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koenig, K.M.; Bozic, K.J. Orthopaedic Healthcare Worldwide: The Role of Standardization in Improving Outcomes. Clin. Orthop. Relat. Res. 2015, 473, 3360–3363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, R.J.; Wilson, A.E.; Quezado, Z. Using Lean Six Sigma Methodology to Improve Quality of the Anesthesia Supply Chain in a Pediatric Hospital. Anesth. Analg. 2017, 124, 922–924. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.J.; Ding, J.; Guzzo, T.J. Improving Operating Room Efficiency. Curr. Urol. Rep. 2019, 20, 28. [Google Scholar] [CrossRef] [PubMed]
- Lunardini, D.; Arington, R.; Canacari, E.G.; Gamboa, K.; Wagner, K.; McGuire, K.J. Lean principles to optimize instrument utilization for spine surgery in an academic medical center: An opportunity to standardize, cut costs, and build a culture of improvement. Spine 2014, 39, 1714–1717. [Google Scholar] [CrossRef] [PubMed]
- Keehan, S.P.; Cuckler, G.A.; Sisko, A.M.; Madison, A.J.; Smith, S.D.; Stone, D.A.; Poisal, J.A.; Wolfe, C.J.; Lizonitz, J.M. National health expenditure projections, 2014–2024: Spending growth faster than recent trends. Health Aff. 2015, 34, 1407–1417. [Google Scholar] [CrossRef] [Green Version]
- Crosby, L.; Lortie, E.; Rotenberg, B.; Sowerby, L. Surgical Instrument Optimization to Reduce Instrument Processing and Operating Room Setup Time. Otolaryngol. Head Neck Surg. (U. S.) 2019, 162, 215–219. [Google Scholar] [CrossRef]
- Muir, G. How to Get Better Value Healthcare, 2nd ed.; Offox Press Ltd.: Oxford, UK, 2011; ISBN 9781904202066. [Google Scholar]
- Peimbert-García, R.E.; Matis, T.; Beltran-Godoy, J.H.; Garay-Rondero, C.L.; Vicencio-Ortiz, J.C.; López-Soto, D. Assessing the state of lean and six sigma practices in healthcare in Mexico. Lead. Health Serv. 2019, 32, 644–662. [Google Scholar] [CrossRef]
- Laureani, A.; Brady, M.; Antony, J. Applications of Lean Six Sigma in an Irish hospital. Lead. Health Serv. 2013, 26, 322–337. [Google Scholar] [CrossRef] [Green Version]
- Halim, U.A.; Khan, M.A.; Ali, A.M. Strategies to Improve Start Time in the Operating Theatre: A Systematic Review. J. Med. Syst. 2018, 42, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; McFadden, K.L.; Gowen, C.R. An exploratory analysis for Lean and Six Sigma implementation in hospitals: Together is better? Health Care Manag. Rev. 2018, 43, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, M.; Jovicic, M.; Djapan, M.; Zivanovic-Macuzic, I. Lean thinking in healthcare: Review of implementation results. Int. J. Qual. Res. 2016, 10, 219–230. [Google Scholar] [CrossRef]
- Van Der Linden, M.C.; Van Ufford, H.M.E.; De Beaufort, R.A.Y.; Grauss, R.W.; Hofstee, H.M.A.; Hoogendoorn, J.M.; Meylaerts, S.A.G.; Rijsman, R.M.; De Rooij, T.P.W.; Smith, C.; et al. The impact of a multimodal intervention on emergency department crowding and patient flow. Int. J. Emerg. Med. 2019, 12, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, B.; Chang, Y.; Grabowski, B.; Brown, D. Using lean-based systems engineering to increase capacity in the emergency department. West. J. Emerg. Med. 2014, 15, 770–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutman, L.E.; Migita, R.; Woodward, G.A.; Klein, E.J. Creating a Leaner Pediatric Emergency Department How Rapid Design and Testing of a Front-End Model Led to Decreased Wait Time. Pediatr. Emerg. Care 2015, 31, 395–398. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.; Senna, P.; Monteiro, A.; Pinha, D. Study on Techniques and Tools Used in Lean Healthcare Implementation: A Literature Review. Braz. J. Oper. Prod. Manag. 2016, 13, 406–420. [Google Scholar] [CrossRef]
- Henrique, D.B.; Godinho Filho, M. A systematic literature review of empirical research in Lean and Six Sigma in healthcare. Total Qual. Manag. Bus. Excell. 2020, 31, 429–449. [Google Scholar] [CrossRef]
- Poksinska, B.B.; Fialkowska-Filipek, M.; Engström, J. Does Lean healthcare improve patient satisfaction? A mixed-method investigation into primary care. BMJ Qual. Saf. 2017, 26, 95–103. [Google Scholar] [CrossRef] [Green Version]
- Poksinska, B. The current state of lean implementation in health care: Literature review. Qual. Manag. Health Care 2010, 19, 319–329. [Google Scholar] [CrossRef] [Green Version]
- Umut, B.; Sarvari, P.A. Applying lean tools in the clinical laboratory to reduce turnaround time for blood test results. Int. J. Adv. Sci. Eng. Technol. 2016, 4, 164–169. [Google Scholar]
- Ahmed, E.S.; Ahmad, M.N.; Othman, S.H. Business process improvement methods in healthcare: A comparative study. Int. J. Health Care Qual. Assur. 2019, 32, 887–908. [Google Scholar] [CrossRef] [PubMed]
- Snee, R.D. Lean Six Sigma—Getting better all the time. Int. J. Lean Six Sigma 2010, 1, 9–29. [Google Scholar] [CrossRef]
- Chassin, M.R.; Loeb, J.M. High-Reliability Health Care: Getting There from Here. Milbank Q. 2013, 91, 459–490. [Google Scholar] [CrossRef]
- Fournier, P.L.; Jobin, M.H. Understanding before implementing: The context of Lean in public healthcare organizations. Public Money Manag. 2018, 38, 37–44. [Google Scholar] [CrossRef]
- Niemeijer, G.C.; Trip, A.; De Jong, L.J.; Wendt, K.W.; Does, R.J. Impact of 5 years of Lean Six Sigma in a University Medical Center. Qual. Manag. Health Care 2012, 21, 262–268. [Google Scholar] [CrossRef]
- White, M.; Wells, J.; Butterworth, T. Leadership, a key element of quality improvement in healthcare. Results from a literature review of “Lean Healthcare” and the Productive Ward. Int. J. Lead. Public Serv. 2013, 9, 90–108. [Google Scholar] [CrossRef]
- Poksinska, B.; Swartling, D.; Drotz, E. The daily work of Lean leaders-lessons from manufacturing and healthcare. Total Qual. Manag. Bus. Excell. 2013, 24, 886–898. [Google Scholar] [CrossRef] [Green Version]
- OECD Length of Hospital Stay (Indicator). Available online: https://data.oecd.org/healthcare/length-of-hospital-stay.htm#indicator-chart (accessed on 22 April 2020).
- Kattan, W.; Wan, T. Factors Influencing Variations in Hospitalization for Diabetes with Hypoglycemia. J. Clin. Med. 2018, 7, 367. [Google Scholar] [CrossRef] [Green Version]
- Boutron, I.; Page, M.J.; Higgins, J.P.; Altman, D.G.; Lundh, A.; Hróbjartsson, A. Chapter 7: Considering bias and conflicts of interest among the included studies. In Cochrane Handbook for Systematic Reviews of Interventions; Cochrane: London, UK, 2019; pp. 1–30. [Google Scholar]
- World Health Organization Quality of Care: A Process for Making Strategic Choices in Health Systems. Available online: https://www.who.int/management/quality/assurance/QualityCare_B.Def.pdf (accessed on 10 April 2019).


{kind=link}
| Author | LOS | TOT | TAT | On-Time Starts | Discharge Order Time | Boarding Time | Readmission | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| - | NC | + | - | NC | + | - | NC | + | - | NC | + | - | NC | + | - | NC | + | - | NC | + | |
| Iannettoni, 2011 | √ | ||||||||||||||||||||
| Hseng-Long, 2011 | √ | ||||||||||||||||||||
| Gayed, 2013 | √ | ||||||||||||||||||||
| Dela Lama, 2013 | √ | ||||||||||||||||||||
| Beck, 2016 | √ | √ | |||||||||||||||||||
| Castaldi, 2016 | √ | √ | |||||||||||||||||||
| Trzeciak, 2018 | √ | ||||||||||||||||||||
| Burkitt, 2009 | √ | ||||||||||||||||||||
| New, 2016 | √ | √ | |||||||||||||||||||
| Collar, 2012 | √ | √ | |||||||||||||||||||
| Artenstein, 2017 | √ | √ | √ | ||||||||||||||||||
| Hassanain, 2016 | √ | √ | |||||||||||||||||||
| Yousri, 2011 | √ | ||||||||||||||||||||
| Montella, 2017 | √ | ||||||||||||||||||||
| Cima, 2011 | √ | √ | |||||||||||||||||||
| Singh, 2014 | √ | ||||||||||||||||||||
| Bender, 2015 | √ | √ | |||||||||||||||||||
| Beck, 2015 | √ | √ | |||||||||||||||||||
| Tagge, 2017 | √ | √ | |||||||||||||||||||
| Toledo, 2013 | √ | √ | |||||||||||||||||||
| Fairbanks, 2007 | √ | √ | |||||||||||||||||||
| Molla, 2018 | √ | √ | √ | ||||||||||||||||||
| Niemeijer, 2010 | √ | √ | |||||||||||||||||||
| Sayeed, 2018 | √ | √ | |||||||||||||||||||
| Brunsman, 2018 | √ | ||||||||||||||||||||
| Johnson, 2016 | √ | √ | |||||||||||||||||||
| Sirvent, 2016 | √ | √ | √ | √ | |||||||||||||||||
| Vose, 2014 | √ | ||||||||||||||||||||
| Niemeijer, 2013 | √ | ||||||||||||||||||||
| Sorensen, 2019 | √ | √ | √ | ||||||||||||||||||
| Moo-Young, 2019 | √ | √ | √ | ||||||||||||||||||
| Cerfolio, 2019 | √ | ||||||||||||||||||||
| Ankrum, 2019 | √ | ||||||||||||||||||||
| Peter, 2011 | √ | ||||||||||||||||||||
| Allen, 2009 | √ | ||||||||||||||||||||
| El-Eid, 2015 | √ | √ | |||||||||||||||||||
| Vijay, 2014 | √ | ||||||||||||||||||||
| Deldar, 2017 | √ | ||||||||||||||||||||
| Adams, 2004 | √ | ||||||||||||||||||||
| Total | 16 | 7 | N | 6 | 2 | N | 5 | N | N | N | N | 7 | 8 | 1 | N | 4 | N | N | 2 | 7 | N |
| First Author, Year, Country | Setting, Study Design, (n), Time Frame | Main Intervention | Outcomes | Summary of Findings |
|---|---|---|---|---|
| Iannettoni, 2011, USA [99] | Cardiothoracic, Pre–Post, (n = 64), 60 mo. | Lean and Kaizen | Length of stay (Average) | Decreased from 14 days to 5 days |
| Hseng-Long, 2011, Taiwan [47] | Cardiology, Pre–Post, (n = 46), 15 mo. | Lean and Six Sigma | Length of stay (Average) | Decreased by 3 days |
| Gayed, 2013, USA [48] | Department of Surgery, Pre–Post, (n = 540), 35 mo. | Lean Six Sigma | Length of stay (Mean) | Decreased from 5.3 days to 3.4 days (p < 0.001) |
| De la Lama, 2013, Spain [85] | Rehabilitation ward, Pre–Post, (n = 75,490), 15 mo. | Six Sigma | Length of stay (Mean) | Decreased from 164.1 days to 58.2 days (p < 0.001) |
| Beck, 2016, USA [3] | Emergency department, Pre–Post, (n = 6906), 25 mo. | Lean | Discharge order entry time (Median) | Decreased from 1:43 pm to 11:28 am (p < 0.0001) |
| Discharge time (Median) | Decreased from 3:25 pm to 2:25 pm (p < 0.0001) | |||
| Discharge before noon (Percentage) | Increased from 14% to 26% (p < 0.0001) | |||
| Boarding time (Median) | Decreased from 176 min to 127 min (p < 0.0001) | |||
| Length of stay (Average) | Decreased from 3.8 days to 3.4 days | |||
| Castaldi, 2016, USA [8] | Operating room, Pre–Post, 32 mo. | Lean and RIE | OR turnover time (Average) | Decreased from 54 min to 41 min (p = 0.0001) |
| On-time Starts (Percentage) | Increased from 54% to 84% (p = 0.0001) | |||
| Trzeciak, 2018, USA [17] | Intensive care unit, Cohort study, (n = 269), 24 mo. | Lean Six Sigma | Length of stay (Median) | Decreased from 29 days to 22 days (p < 0.001) |
| Burkitt, 2009, USA [86] | Department of Surgery, Cohort study, (n = 1779), 48 mo. | TPS | Length of stay (Median) | Non-significant change (p = 0.90) |
| New, 2016, UK [88] | Orthopedic trauma theatre, Pre–Post, (n = 1041), 18 mo. | Lean | Length of stay (Mean) | Non-significant change (p = 0.396) |
| Readmission (Proportion) | Non-significant change (p = 0.30) | |||
| Collar, 2012, USA [21] | Operating room, Cohort study, (n = 199), 18 mo. | Lean | Turnover time (Mean) | Decreased from 38.4 min to 29 min (p < 0.001) |
| Turnaround time (Mean) | Decreased from 89.5 min to 69.3 min (p < 0.001) | |||
| Artenstein, 2017, USA [19] | Emergency Department, Pre–Post, 24 mo. | Lean Six Sigma and BPPI | Length of stay (Mean) | Decreased from 5.3 days to 5 days (p < 0.005) |
| Boarding time (Mean) | Decreased from 7.6 h to 5.5 h (p = 0.007) | |||
| Discharge before noon (Percentage) | Increased from 43% to 54.1% (p < 0.001) | |||
| Hassanain, 2016, Saudi Arabia [26] | Operating room, Cohort study, 28 mo. | Lean | On-time start (Percentage) | Increased from 14% to 34% (p < 0.001) |
| Room turnover time (Median) | Non-significant change | |||
| Yousri, 2011, UK [87] | Department of Surgery, Pre–Post, (n = 608), 24 mo. | Lean | Length of stay (Median) | Non-significant change (p = 0.178) |
| Montella, 2017, Italy [100] | Department of Surgery, Pre–Post, (n = 22,262), 48 mo. | Lean Six Sigma | Length of stay (Mean) | Decreased from 45 days to 36 days (p = 0.038) |
| Cima, 2011, USA [22] | Operating room, Pre–Post, (n = 8497), 18 mo. | Lean Six Sigma | On-time starts (Percentage) | TS increased from 50% to 80% (p < 0.05); GYN increased from 64% to 92% (p < 0.05); Gen/CRS increased from 60% to 92% (p < 0.05) |
| Turnover time (Average) | TS decreased from 40 min to 30 min (p < 0.05); GYN decreased from 35 min to 20 min (p < 0.05); Gen/CRS decreased from 34 min to 23 min (p < 0.05) | |||
| Singh, 2014, India [23] | Operating room, Pre–Post, (n = 231), 6 mo. | Lean Six Sigma | Turnaround time (Mean) | Decreased from 17.6 min to 10.4 min (p < 0.0002) |
| Bender, 2015, USA [27] | Operating room, Pre–Post, (n = 25,903), 36 mo. | Lean Six Sigma | On-time starts (Percentage) | Increased from 32% to 73% |
| Turnover time (Average) | Non-significant change | |||
| Beck, 2015, USA [89] | Inpatient pediatric service, Pre–Post, (n = 3509), 12 mo. | Lean Six Sigma | Time of patient discharge (Median) | Decreased from 15:48 min to 14:15 min (p < 0.0001) |
| Patients discharged by noon (Proportion) | Decreased from 27% to 14% (p < 0.0001) | |||
| Length of stay (Mean) | Non-significant change (p = 0.864) | |||
| Tagge, 2017, USA [24] | Operating room, Pre–Post, (n = 612), 6 mo. | Lean Six Sigma | Turnover time (Median) | Decreased from 41 min to 32 min (p < 0.0001) |
| Turnaround time (Median) | Decreased from 81.5 min to 71 min (p < 0.0001) | |||
| Toledo, 2013, USA [28] | Organ transplant center, Pre–Post, (n = 103), 48 mo. | Lean Six Sigma | Length of stay (Median) | Decreased from 11 days to 8 days (p < 0.05) |
| 30-day readmission (Rate) | Non-significant change (p = 0.63) | |||
| Fairbanks, 2007, USA [101] | Operation Room, Pre–Post, 12 mo. | Lean Six Sigma | On-time start (Percentage) | Increased from 12% to 89% |
| Turnaround time (Mean) | Decreased from 23.8 min to 17.9 min | |||
| Molla, 2018, USA [20] | Operating room, Pre–Post, (n = 1471), 28 mo. | Lean Six Sigma | Discharge orders released by 10:00 (Percentage) | Increased by 21.3% (p < 0.001) |
| Patients discharged by noon (Percentage) | Increased by 7.5% (p = 0.001) | |||
| 30-day readmission (Rate) | Non-significant change (p = 0.492) | |||
| Length of stay (Mean) | Non-significant change (p = 0.153) | |||
| Niemeijer, 2010, The Netherlands [98] | Trauma Care, Pre–Post, (n = 1693), 18 mo. | Lean Six Sigma | Length of stay (Average) | Decreased from 11.8 days to 8.5 days |
| Sayeed, 2018, USA [95] | Operating room, Pre–Post, (n = 505), 24 mo. | Lean Six Sigma | Length of stay (Average) | Decreased from 6 days to 5.2 days (p = 0.02) |
| 30-day readmissions (Rate) | Non-significant change (p = 0.13) | |||
| Brunsman, 2018, USA [18] | Inpatient pharmacy, Cohort study, (n = 102), 15 mo. | Lean | Length of stay (Median) | Decreased from 22.9 days to 13.2 days (p = 0.049) |
| Johnson, 2016, USA [90] | Emergency department, Pre–Post, (n = 1394), 24 mo. | Lean Six Sigma | Heart failure patient’s readmission (Average) | Decreased from 28.4% to 18.9% (p < 0.01) |
| Length of stay (Mean) | Non-significant change (p = 0.70) | |||
| Sirvent, 2016, Spain [29] | Intensive care unit, Pre–Post, (n = 1388), 12 mo. | Lean | ICU boarding time (Mean) | Decreased from 360.8 min to 276.7 min (p = 0.036) |
| Length of stay in ICU (Mean) | Non-significant change (p = 0.992) | |||
| Readmissions (Percentage) | Non-significant change (p = 0.966) | |||
| Vose, 2014, USA [91] | Emergency department, Pre–Post, 24 mo. | Lean | Boarding time (Average) | Decreased from 58.9 min to 43.6 min |
| Niemeijer, 2013, The Netherlands [102] | Department of Surgery, Pre–Post, (n = 332), 45 mo. | Lean Six Sigma | Length of stay (Average) | Decreased from 13.5 days to 9.3 days (p = 0.000) |
| Sorensen, 2019, USA [92] | Department of Surgery, Pre–Post, (n = 4253), 36 mo. | Lean | Length of stay (Mean) | Decreased from 3.2 days to 2.4 days (p < 0.001) |
| 30-day readmission (Percentage) | Decreased from 3.1% to 1.1% (p = 0.032) | |||
| Discharge to home (vs. rehabilitation facility or skilled nursing facility) (Percentage) | Increased from 72% to 91% (p < 0.001) for hip patients; Increased from 70% to 87% (p< 0.001) for knee patients | |||
| Moo-Young, 2019, USA [93] | Pediatric gastroenterology, Pre–Post, (n = 355), 12 mo. | Lean Six Sigma | 30-day readmission (Rate) | Non-significant change (p = 0.54) |
| Discharged before 1 pm (Percentage) | Non-significant change | |||
| Length of stay (Mean) | Decreased from 5.7 days to 4.7 days (p = 0.055) | |||
| Cerfolio, 2019, USA [103] | Operating room, Pre–Post, (n = 128), 6 mo. | Lean | OR turnover time (Median) | Decreased from 37 min to 14 min (p < 0.0001) |
| Ankrum, 2019, USA [104] | Isolation room, Pre–Post, (n = 38), 2 mo. | Lean | Room turnover time (Median) | Decreased from 130 min to 65 min (p < 0.0001) |
| Peter, 2011, USA [105] | Operating room, Pre–Post, 24 mo. | Lean Six Sigma | Cases starting on time (Percentage) | Increased from 13% to 80% |
| Allen, 2009, USA [106] | Hospital discharge process, Pre–Post, (n = 150), 6 mo. | Six Sigma | Discharge time (Average) | Decrease from 3.3 h to 2.8 h (p = 0.068) |
| El-Eid, 2015, Lebanon [107] | Emergency department, Pre–Post, (n = 17,054), 10 mo. | Six Sigma | Discharge time (Mean) | Decreased from 2.2 h to 1.7 h. (p < 0.001) |
| Length of stay (Mean) | Decreased from 3.4 days to 3.1 days (p < 0.001) | |||
| Vijay, 2014, India [108] | Department of Surgery, Pre–Post, (n = 120), 3 mo. | Six Sigma | Cycle time of patient discharge process (Average) | Decreased from 234 min to 143 min |
| Deldar, 2017, USA [109] | Operating room, Pre–Post, (n = 4492), 7 months | Lean | On-time starts (Percentage) | Increased from 57% to 69% (p < 0.01) |
| Adams, 2004, USA [110] | Operating room, Pre–Post, (n = 96), 8 mo. | Six Sigma | Turnaround time between cases in the OR (Mean) | Decreased from 22.8 min to 15.6 min |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zepeda-Lugo, C.; Tlapa, D.; Baez-Lopez, Y.; Limon-Romero, J.; Ontiveros, S.; Perez-Sanchez, A.; Tortorella, G. Assessing the Impact of Lean Healthcare on Inpatient Care: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 5609. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155609
Zepeda-Lugo C, Tlapa D, Baez-Lopez Y, Limon-Romero J, Ontiveros S, Perez-Sanchez A, Tortorella G. Assessing the Impact of Lean Healthcare on Inpatient Care: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(15):5609. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155609
Chicago/Turabian StyleZepeda-Lugo, Carlos, Diego Tlapa, Yolanda Baez-Lopez, Jorge Limon-Romero, Sinue Ontiveros, Armando Perez-Sanchez, and Guilherme Tortorella. 2020. "Assessing the Impact of Lean Healthcare on Inpatient Care: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 15: 5609. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155609