Objective Analysis of Movement in Subjects with ADHD. Multidisciplinary Control Tool for Students in the Classroom

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.2.1. Sample Recruitment
2.2.2. Study Techniques Workshops
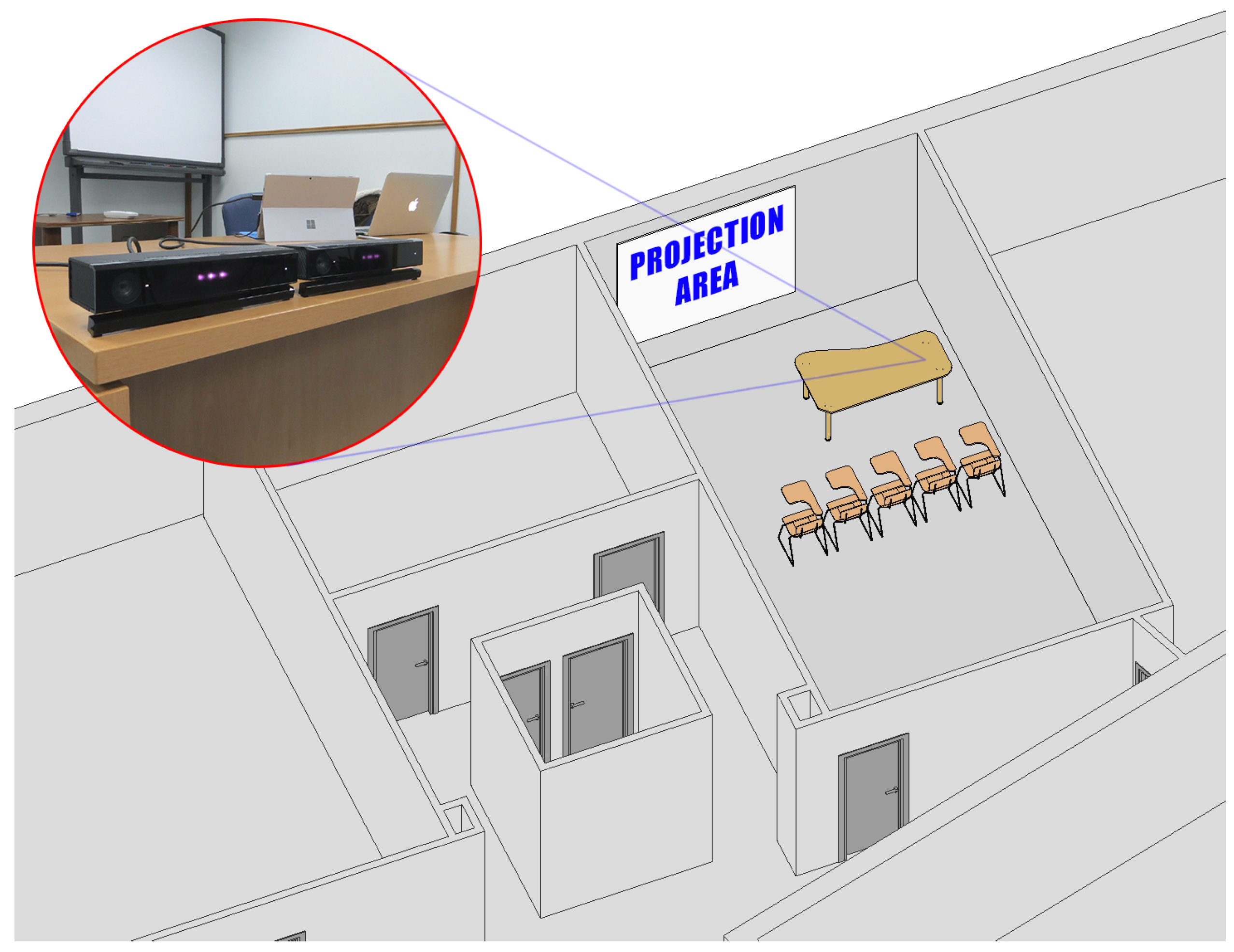
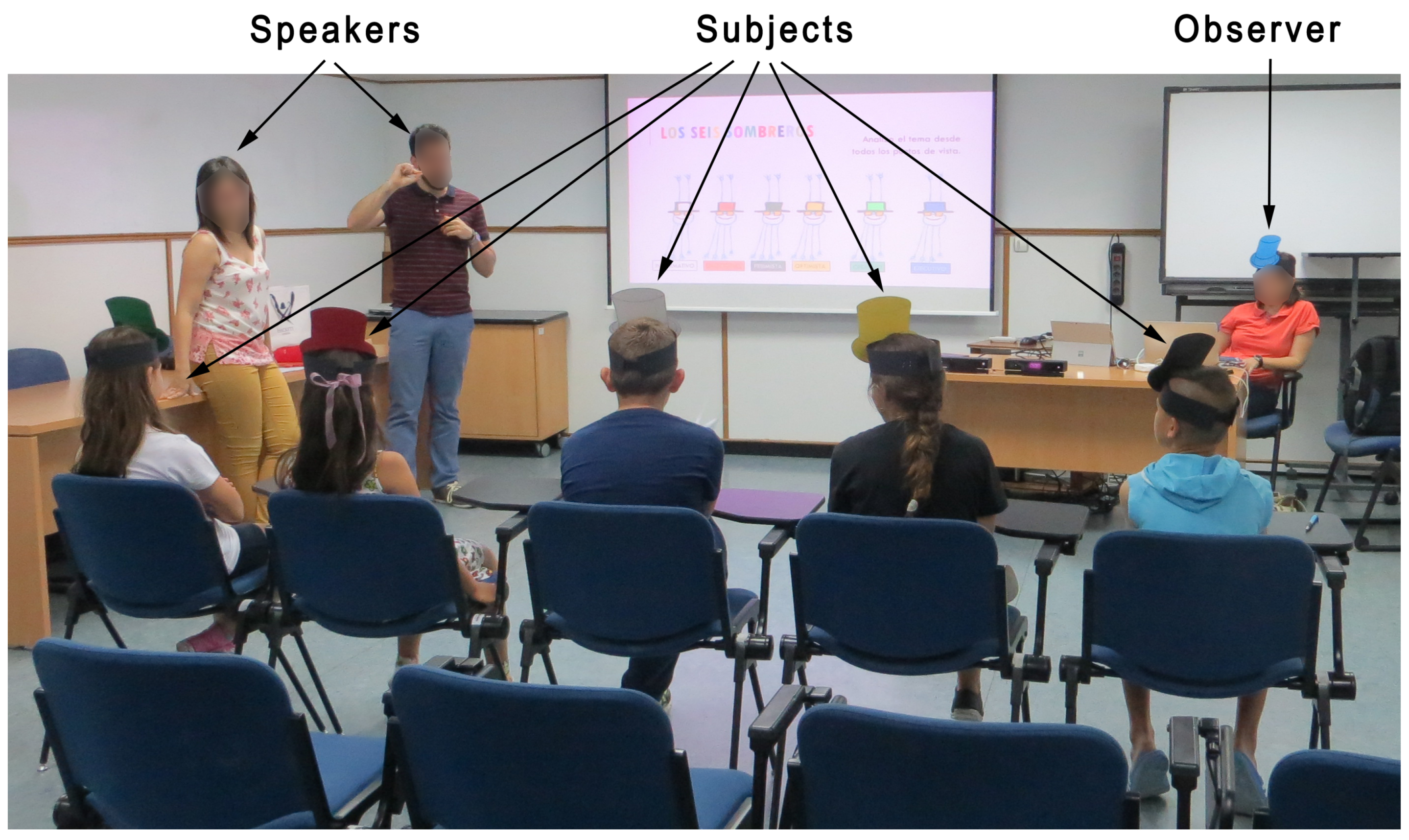
2.2.3. Classroom Layout
2.2.4. Computer Application ADHD Movements
2.3. Analysis of Data
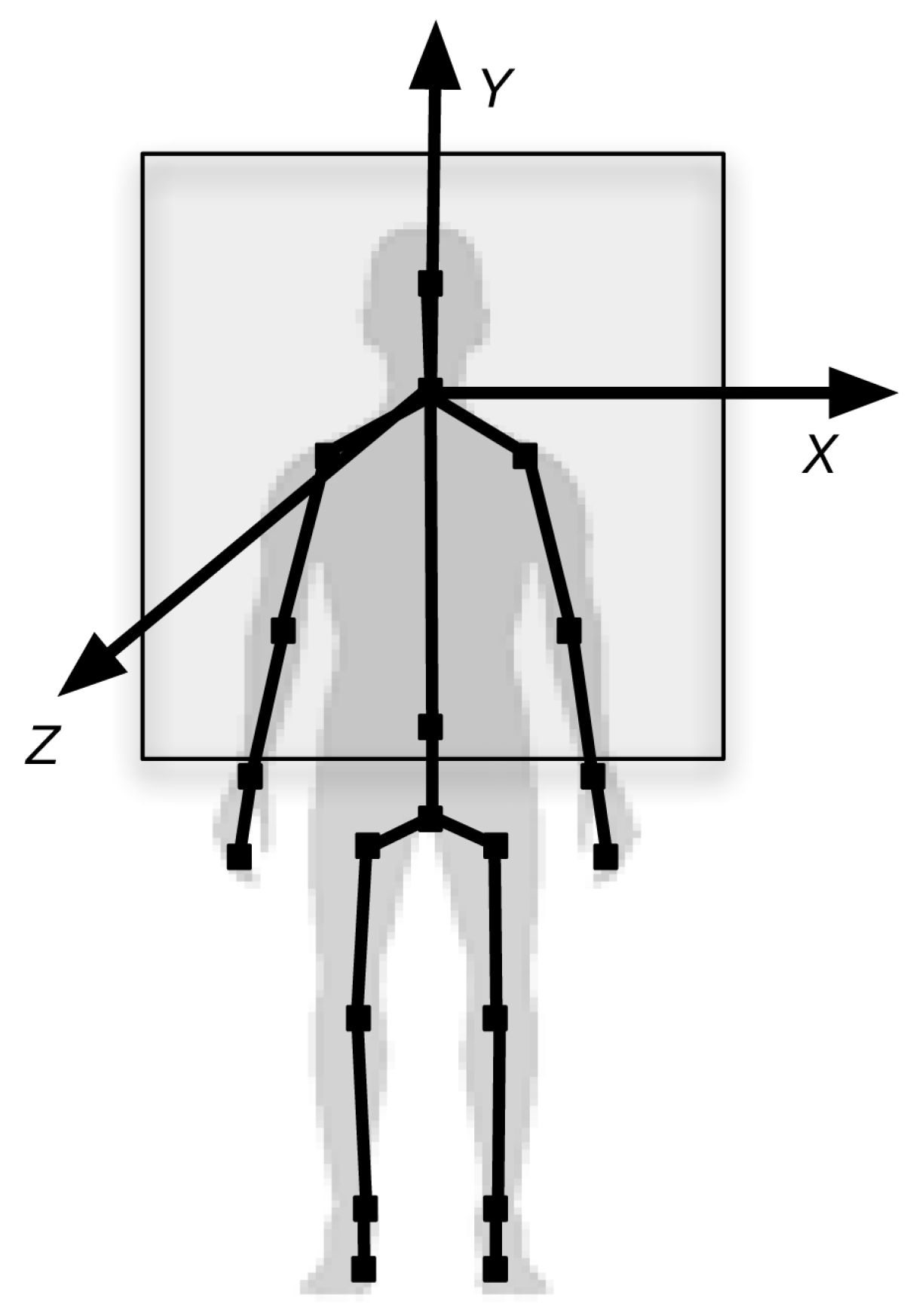
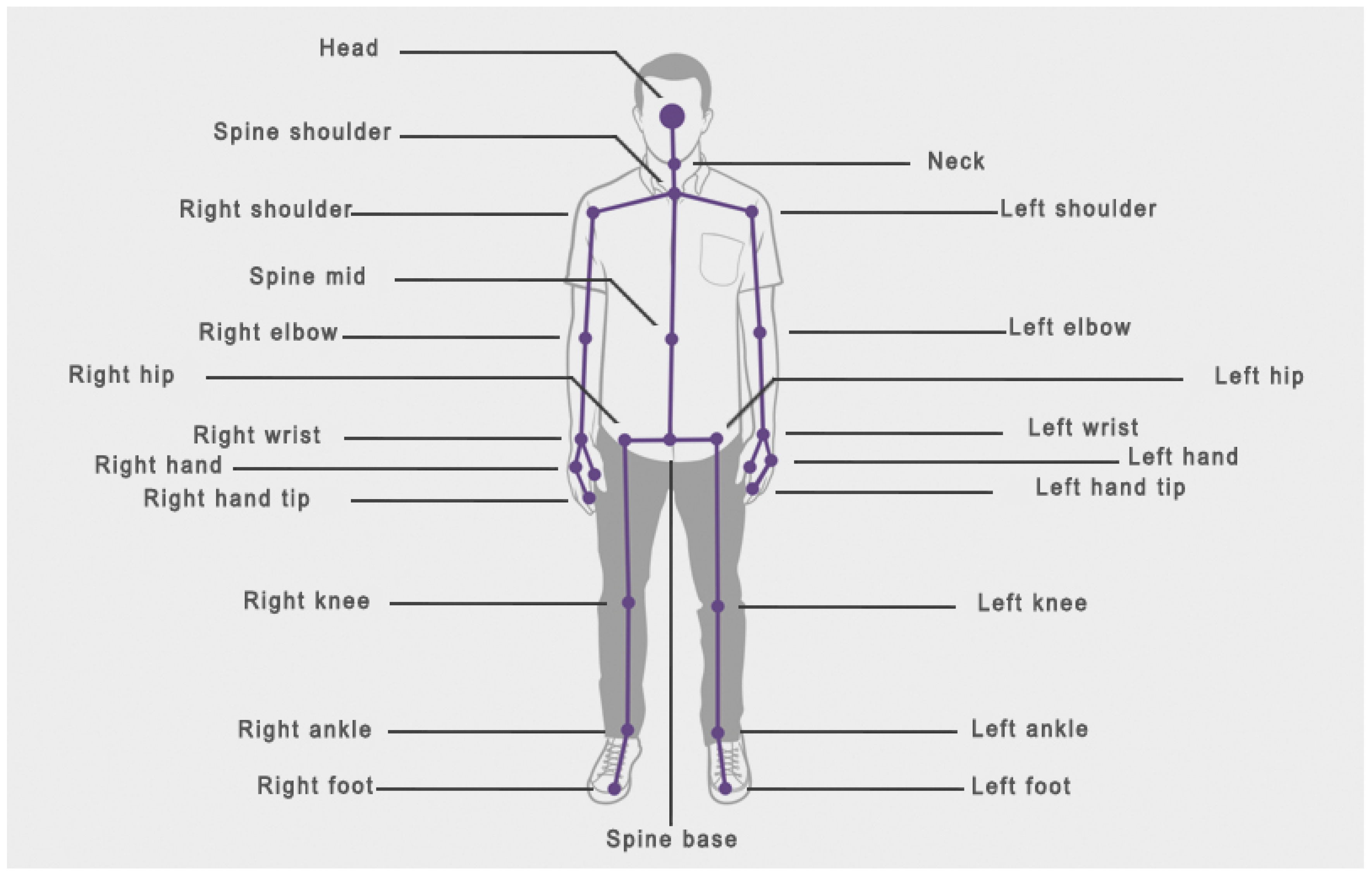
2.3.1. Data Registered by the Kinect Device
2.3.2. Data Registered by Observers
2.3.3. Statistical Analysis
3. Results
3.1. Average Differences in Movement for Every Joint in the Experimental Group and the Control Group
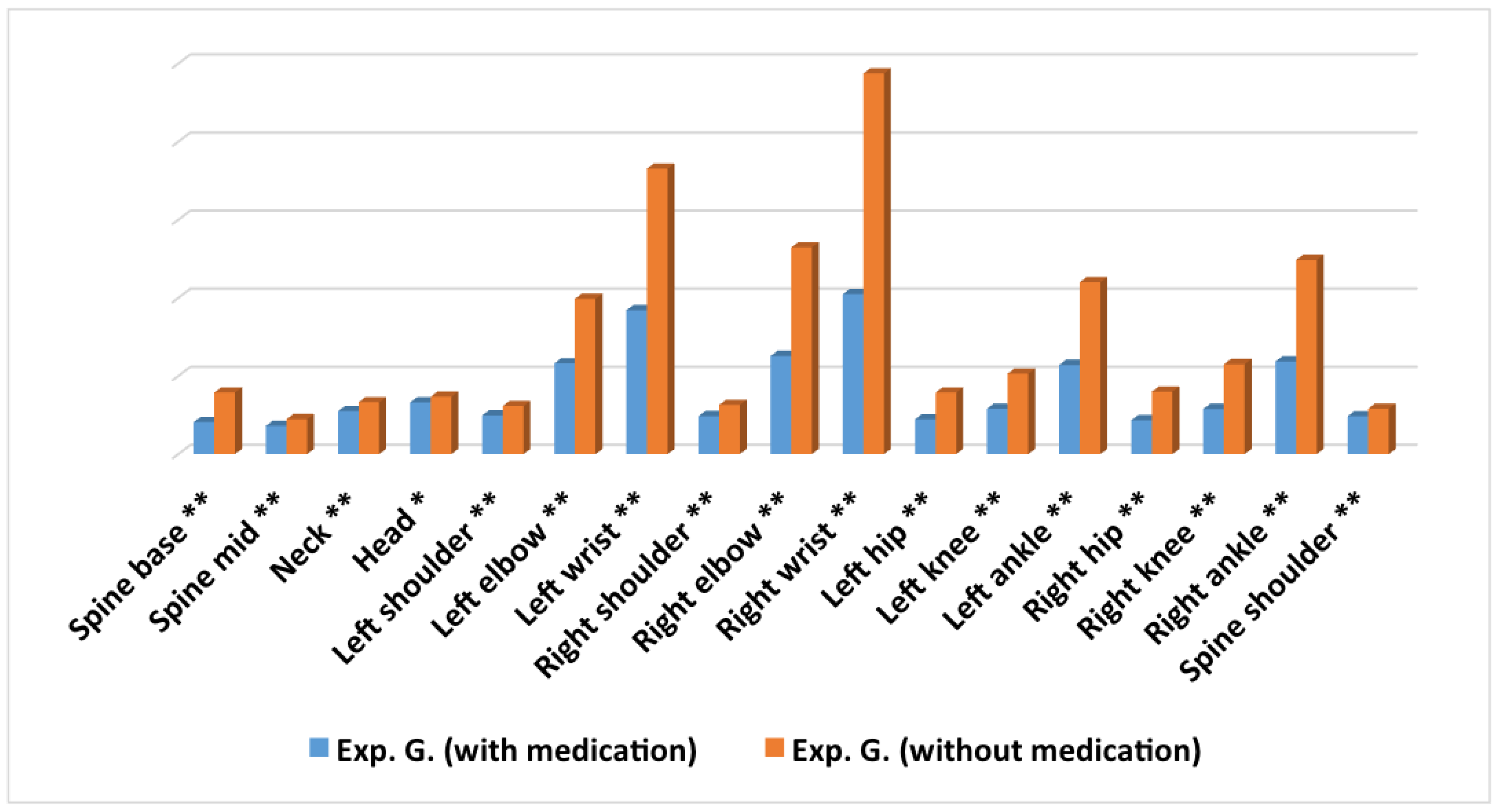
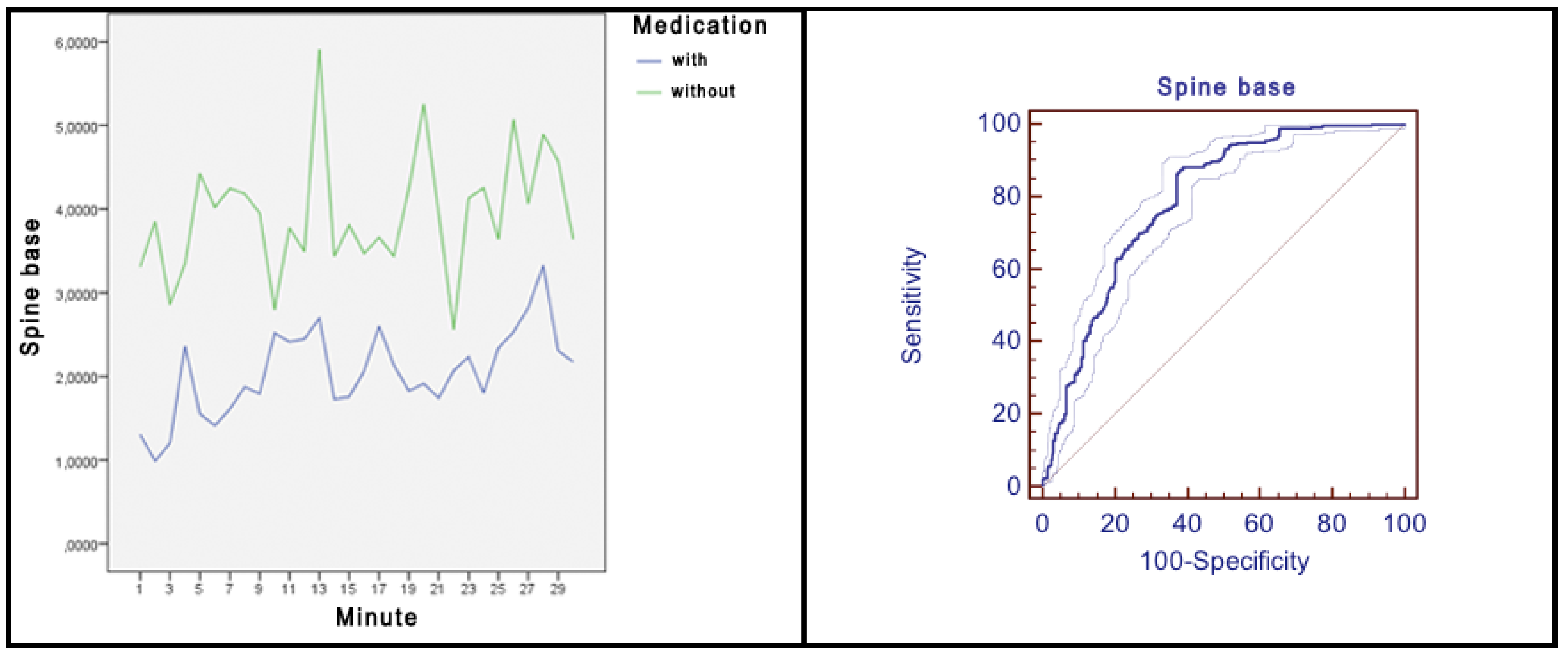
3.2. Average Differences in Movement for Every Joint within the Experimental Group with and without Medication Intake
3.3. Average Differences in Movement for Every Joint in the Experimental Group, According to Sex
3.4. Movement Difference Registered by Observers
4. Discussion
Limitations, Strengths, and Future Directions
5. Conclusions
- The software developed (ADHD Movements) for the Microsoft Kinect V.2 device is valid to capture the movement of 17 joints of up to 6 subjects in a teaching/learning situation.
- Students with ADHD present more movement and squirm more in their seat, than students without ADHD.
- Students with a firm diagnosis of ADHD without the prescribed medication present more movement and squirm more in their seat than ADHD students with the prescribed medication.
- ADHD students with and without taking their prescribed medication present a similar amount of movement in the head joint.
- Girls with ADHD present more movement than boys with ADHD.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM–5); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Alós, C.; Ruiz, C. Las otras verdades del TDAH. Aula Infant. 2013, 70, 1–52. [Google Scholar]
- Barkley, R. Avances en el diagnóstico y la subclasificación del trastorno por déficit de atención/hiperactividad: Qué puede pasar en el futuro respecto al DSM-V. Rev. Neurol. 2009, 48, 101–106. [Google Scholar] [CrossRef]
- Alberola, P. Los criterios de diagnóstico son vagos, ¿cómo se determina que un niño es más o menos movido? D. Inf. 2015, 5, 82–98. [Google Scholar]
- Artigas-Pallarés, J. Comorbilidad en el trastorno por déficit de atención/hiperactividad. Rev. Neurol. 2003, 36, 68–78. [Google Scholar] [CrossRef]
- Gawrilow, C.; Kühnhausen, J.; Schmid, J.; Stadler, G. Hyperactivity and Motoric Activity in ADHD: Characterization, Assessment, and Intervention. Front. Psychiatry 2014, 5, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohasi, K.; Vitaliano, G.; Polcari, A.; Teicher, M. Unraveling the nature of hyperactivity in children with attention-deficit/hyperactivity disorder. Arch. Gen. Psychiatry 2010, 67, 388–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teicher, M.; Polcari, A.; McGreenery, C. Utility of Objective Measures of Activity and Attention in the Assessment of Therapeutic Response to Stimulants in Children with Attention-Deficit/Hyperactivity Disorder. J. Child Adolesc. Psychopharmacol. 2008, 18, 265–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conrad, P. The discovery of hiperkinesis: Notes on the medicalization of deviant behavior. Soc. Probl. 1975, 23, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Fominaya, C. El TDAH no existe, y la medicación no es un tratamiento, sino un dopaje. ABC Padres e hijos, 20 October 2014. [Google Scholar]
- Schrag, P.; Divoky, D. The Myht of the Hiperactive Child and Othher Means of Child Control; Pantheon Books: New York, NY, USA, 1975. [Google Scholar]
- Timimi, S.; Moncrieff, J.; Jureidini, J.; Leo, J.; Cohen, D.; Whitfield, C.; Double, D.; Bindman, J.; Asen, E.; Bracken, P.; et al. A critique of the international consensus statement on ADHD. Clin. Child Fam. Psychol. Rev. 2004, 7, 59–63. [Google Scholar]
- De Vinuesa, F.G.; González, H.; Pérez, M. Volviendo a la Normalidad: La Invención del TDAH y del Trastorno Bipolar Infantil; Alianza Editorial: Madrid, Spain, 2014. [Google Scholar]
- García, L.; Cortese, S.; Anderson, D.; Martino, A.D.; Castellanos, F. Locomotor activity measures in the diagnosis of attention deficit hyperactivity disorder: Meta-analyses and new findings. J. Neurosci. Methods 2015, 252, 14–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, C.; Valentine, A.; Groom, M.; Walker, G.; Sayal, K.; Hollis, C. The clinical utility of the continuous performance test and objective measures of activity for diagnosing and monitoring ADHD in children: A systematic review. Eur. Child Adolesc. Psychiatry 2016, 25, 677–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaiswal, S.; Valstar, M.; Gillott, A.; Daley, D. Automatic detecion of ADHD and ASD from Expressive Behaviour in RGBD Data. arXiv 2016, arXiv:1612.02374. [Google Scholar]
- Li, F.; Zheng, Y.; Smith, S.; Shic, F.; Moore, C.; Zheng, X.; Qi, Y.; Liu, Z.; Leckman, J. A preliminary study of movement intensity during a Go/No-Go task and its association with ADHD outcomes and symptom severity. Child Adolesc. Psychiatry Ment. Health 2016, 10, 47. [Google Scholar] [CrossRef] [Green Version]
- O’mahony, N.; Florentino-Liano, B.; Carballo, J.; Baca-García, E.; Artés, A. Objective diagnosis of ADHD using IMUs. Med. Eng. Phys. 2014, 36, 922–926. [Google Scholar] [CrossRef]
- Wehmeier, P.; Schacht, A.; Wolff, C.; Otto, W.; Dittmann, L.; Banaschewski, T. Neuropsychological outcomes across the day in children with attention-deficit/hyperactivity disorder treated with atomoxetine: Results from a placebo-controlled study using a computer-based continuous performance test combined with an infra-red motion-tracking device. J. Child Adolesc. Psychopharmacol. 2011, 21, 433–444. [Google Scholar]
- Ding, I.; Chang, C. An eigenspace-based method with a user adaptation scheme for human gesture recognition by using Kinect 3D data. Appl. Math. Model. 2015, 39, 5769–5777. [Google Scholar] [CrossRef]
- Conzelmann, A.; Pusch, A.; Hahn, N.; Overfeld, J.; Nehfischer, M.; Wieser, M.; Warnke, A.; Renner, T.; Taurines, R.; Romanos, M.; et al. Movement and activity assessed with the Kinect in sitting children, and the influence of hyperactivity. J. Cyberther. Rehabil. 2012, 17, 1–2. [Google Scholar]
- Xu, X.; McGorry, R. The validity of the first and second generation Microsoft KinectTM for identifying joint center locations during static postures. Appl. Ergon. 2015, 49, 47–54. [Google Scholar] [CrossRef]
- Cohen, J. A coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1988. [Google Scholar]
- Akobeng, A. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr. 2007, 96, 644–647. [Google Scholar] [CrossRef]
- Alabbassi, H.; Gradinaru, A.; Moldoveanu, F.; Moldoveanu, A. Human Motion Tracking & Evaluation using Kinect V2 Sensor. In Proceedings of the 5th IEEE International Conference on E-Health and Bioengineering, Lasi, Romania, 19–21 November 2015; pp. 1–4. [Google Scholar]
- Jana, A. Kinect for Windows SDK: Programming Guide; Packt Publishing: Birmingham, UK, 2012. [Google Scholar]
- Boutsika, E. Kinect in Education: A Proposal for Children with Autism. Procedia Comput. Sci. 2014, 27, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Clark, R.; Pua, Y.; Bryant, A.; Hunt, M. Validity of the Microsoft Kinect for providing lateral trunk lean feedback during gait retraining. Gait Posture 2013, 38, 1064–1066. [Google Scholar] [CrossRef] [PubMed]
- OMS. CIE-10. Décima Revisión de la Clasificación Internacional de las Enfermedades. Trastornos Mentales y del Comportamiento; Descripción Clínicas y Pautas para el Diagnóstico, Méditor ed.m Madrid; Organizacion Mondial de la Salud: Madrid, Spain, 1992. [Google Scholar]
- Dutta, T. Evaluation of the Kinect sensor for 3-D kinematic measurement in the workplace. Appl. Ergon. 2011, 43, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Frati, V.; Prattichizzo, D. Using kinect for hand tracking and rendering in wearable haptics. In Proceedings of the IEEE World Haptics Conference, Istanbul, Turkey, 22–24 June 2011; pp. 317–321. [Google Scholar]
- Izadi, S.; Kim, D.; Hilliges, O.; Molyneaux, D.; Newcombe, R.; Kohli, P.; Shotton, J.; Hodges, S.; Freeman, D.; Davison, A.; et al. KinectFusion: Real-Time 3D Reconstruction and Interaction Using a Moving Depth; Association for Computing Machinery: New York, NY, USA, 2011; pp. 559–568. [Google Scholar]
- Noonan, P.; Cootes, T.; Hallett, W.; Hinz, R. The design and initial calibration of an optical tracking system using the microsoft kinect. In Proceedings of the IEEE Nuclear Science Symposium and Medical Imaging Conference, Valencia, Spain, 23–29 October 2011; pp. 3614–3617. [Google Scholar]
- Seer, S.; Brändle, N.; Ratti, C. Kinects and human kinetics: A new approach for studying pedestrian behavior. Trans. Res. Part C Emerg. Technol. 2014, 48, 212–228. [Google Scholar] [CrossRef]
- Diest, M.V.; Stegenga, J.; Wörtche, H.; Postema, K.; Verkerke, G.J.; Lamoth, C. Suitability of Kinect for measuring whole body movement patterns during exergaming. J. Biomech. 2014, 47, 2925–2932. [Google Scholar] [CrossRef] [PubMed]
- Weber, I.; Koch, J.; Meskemper, J.; Friedl, K.; Heinrich, K.; Hartmann, K. Is the MS Kinect suitable for motion analysis? Biomed. Eng. 2012, 57. [Google Scholar] [CrossRef] [Green Version]
- Teicher, M.; Ito, Y.; Glod, C.; Barber, N. Objective Measurement of Hyperactivity and Attentional Problems in ADHD. J. Am. Acad. Child Adolesc. Psychiatry 1996, 35, 334–342. [Google Scholar] [CrossRef]
- Parsons, T.; Bowerly, T.; Buckwalter, J.; Rizzo, A.A. A controlled clinical comparison of attention performance in children with ADHD in a virtual reality classroom compared to standard neuropsychological methods. Child Neuropsychol. J. Norm. Abnorm. Dev. Child. Adolesc. 2007, 13, 363–381. [Google Scholar] [CrossRef]
- Crescenzo, F.D.; Armando, M.; Mazzone, L.; Ciliberto, M.; Sciannamea, M.; Figueroa, C.; Janiri, L.; Quested, D.; Vicari, S. The use of actigraphy in the monitoring of methylphenidate versus placebo in ADHD: A meta-analysis. ADHD Atten. Deficit Hyperact. Disord. 2014, 6, 49–58. [Google Scholar] [CrossRef]
- Diaz-Orueta, U.; Iriarte, Y.; Climent, G.; Banterla, F. AULA: An ecological virtual reality test with distractors for evaluating attention in children and adolescents. Virtual Real. Sci. Vis. J. 2012, 5, 1–20. [Google Scholar]
- Hughes, C.; Pickering, J.; Baker, K.; Bolanos, G.; Silver, C. Differentiating ADHD from oral language difficulties in children: Role of movements and effects of stimulant medication. BMC Psychiatry 2014, 14, 370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mühlberger, A.; Jekel, K.; Probst, T.; Schecklmann, M.; Conzelmann, A.; Andreatta, M.; Rizzo, A.; Pauli, P.; Romanos, M. The Influence of Methylphenidate on Hyperactivity and Attention Deficits in Children with ADHD. J. Atten. Disord. 2016, 1, 277–289. [Google Scholar]
- Fernández, F.; González, C.; Sempere, M.; Navarro, I. Assessment of the techology to measure movements in the detection of students with attention deficit hyperactivity disorder. In Proceedings of the 9th International Technology, Education and Development Conference (INTED2015), Madrid, Spain, 2–3 March 2015. [Google Scholar]
- Chhabildas, N.; Pennington, B.; Willcutt, E. A comparison of the neuropsychological profiles of the DSM-IV subtypes of ADHD. J. Abnorm. Child Psychol. 2001, 29, 529–540. [Google Scholar] [CrossRef] [PubMed]
- Geurts, H.; Verté, S.; Oosterlaan, J.; Roeyers, H.; Sergeant, J. ADHD subtypes: Do they differ in their executive functioning profile? Arch. Clin. Neuropsychol. 2005, 20, 457–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merikangas, K.; He, J.; Burstein, M.; Swendsen, J.; Avenevoli, S.; Case, B.; Georgiades, K.; Heaton, L.; Swanson, S.; Olfson, M. Service utilization for lifetime mental disorders in U.S. adolescents: Results of the National Comorbidity Survey-Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 32–45. [Google Scholar] [CrossRef] [Green Version]
- Galna, B.; Barry, G.; Jackson, D.; Mhiripiri, D.; Olivier, P.; Rochester, L. Accuracy of the Microsoft Kinect sensor for measuring movement in people with Parkinson’s disease. Gait Posture 2014, 39, 1062–1068. [Google Scholar] [CrossRef] [Green Version]
- Clark, R.; Pua, Y.; Fortin, K.; Ritchie, C.; Webster, K.; Denehy, L.; Bryant, A. Validity of the Microsoft Kinect for assessment of postural control. Gait Posture 2012, 36, 372–377. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Kinect Joint | Levene Test | Experimental Group | Control Group | Statistical Significance and Magnitude Differences | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F | p | M | DE | M | DE | t | g.l. | p | d | |
| Spine base | 45.42 | <0.001 | 2.92 | 2.41 | 2.53 | 1.82 | 4.73 | 2512.24 | <0.001 | 0.18 |
| Spine mid | 74.18 | <0.001 | 2.14 | 1.76 | 1.62 | 1.05 | 9.59 | 2665.48 | <0.001 | 0.34 |
| Neck | 64.04 | <0.001 | 3.01 | 2.36 | 2.26 | 1.60 | 9.70 | 2612.67 | <0.001 | 0.36 |
| Head | 102.41 | <0.001 | 3.48 | 2.52 | 2.44 | 1.67 | 12.79 | 2628.94 | <0.001 | 0.46 |
| Left shoulder | 46.76 | <0.001 | 2.76 | 2.18 | 2.11 | 1.66 | 8.62 | 2496.40 | <0.001 | 0.32 |
| Left elbow | 46.53 | <0.001 | 7.72 | 6.06 | 6.54 | 4.79 | 5.50 | 2448.92 | <0.001 | 0.21 |
| Left wrist | 53.83 | <0.001 | 13.41 | 10.31 | 12.84 | 7.87 | 1.62 | 2497.42 | 0.105 | - |
| Right shoulder | 111.21 | <0.001 | 2.76 | 2.25 | 2.00 | 1.33 | 10.97 | 2665.93 | <0.001 | 0.39 |
| Right elbow | 15.46 | <0.001 | 9.50 | 7.85 | 7.92 | 7.00 | 5.38 | 2265.50 | <0.001 | 0.21 |
| Right wrist | 92.18 | <0.001 | 16.79 | 14.08 | 15.38 | 10.05 | 3.00 | 2571.63 | 0.003 | 0.11 |
| Left hip | 27.87 | <0.001 | 3.02 | 2.35 | 2.72 | 1.93 | 3.57 | 2393.97 | <0.001 | 0.14 |
| Left knee | 4.35 | 0.037 | 3.95 | 4.00 | 3.21 | 4.49 | 4.26 | 1890.72 | <0.001 | 0.18 |
| Left ankle | 10.13 | 0.001 | 8.16 | 7.72 | 8.23 | 8.70 | −0.205 | 1883.48 | 0.838 | - |
| Right hip | 25.15 | <0.001 | 3.02 | 2.34 | 2.72 | 1.97 | 3.47 | 2356.94 | 0.001 | 0.14 |
| Right knee | 24.75 | <0.001 | 4.23 | 4.79 | 3.14 | 3.47 | 6.76 | 2554.91 | <0.001 | 0.25 |
| Right ankle | 0.635 | 0.426 | 8.95 | 8.54 | 8.56 | 9.54 | 1.08 | 2666 | 0.279 | - |
| Spine shoulder | 73.26 | <0.001 | 2.65 | 2.21 | 1.97 | 1.40 | 9.61 | 2650.59 | <0.001 | 0.35 |
| Kinect Joint | Levene Test | Experimental Group (with Medication) | Control Group (with Medication) | Statistical Significance and Magnitude Differences | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F | p | M | DE | M | DE | t | g.l. | p | d | |
| Spine base | 32.30 | <0.001 | 2.05 | 1.83 | 3.94 | 2.60 | 16.92 | 1370.59 | <0.001 | 0.83 |
| Spine mid | 0.001 | 0.974 | 1.80 | 1.57 | 2.53 | 1.89 | 8.61 | 1676 | <0.001 | 0.42 |
| Neck | <0.001 | 0.996 | 2.75 | 2.18 | 3.32 | 2.51 | 4.93 | 1676 | <0.001 | 0.24 |
| Head | 4.63 | 0.031 | 3.31 | 2.45 | 3.68 | 2.59 | 3.02 | 1609.82 | 0.002 | 0.15 |
| Left shoulder | 0.381 | 0.537 | 2.48 | 2.04 | 3.08 | 2.29 | 5.69 | 1676 | <0.001 | 0.28 |
| Left elbow | 26.33 | <0.001 | 5.81 | 5.23 | 9.94 | 6.20 | 14.61 | 1526.61 | <0.001 | 0.72 |
| Left wrist | 15.68 | <0.001 | 9.21 | 8.60 | 18.28 | 9.99 | 19.75 | 1543.72 | <0.001 | 0.97 |
| Right shoulder | 0.490 | 0.484 | 2.43 | 2.04 | 3.15 | 2.41 | 6.60 | 1676 | <0.001 | 0.32 |
| Right elbow | 186.14 | <0.001 | 6.28 | 4.87 | 13.23 | 8.91 | 19.39 | 1163.32 | <0.001 | 0.95 |
| Right wrist | 147.05 | <0.001 | 10.24 | 9.40 | 24.37 | 14.77 | 22.94 | 1281.24 | <0.001 | 1.12 |
| Left hip | 13.56 | <0.001 | 2.22 | 1.96 | 3.94 | 2.43 | 15.70 | 1492.09 | <0.001 | 0.77 |
| Left knee | 102.38 | <0.001 | 2.91 | 2.91 | 5.15 | 4.71 | 11.50 | 1256.51 | <0.001 | 0.56 |
| Left ankle | 276.86 | <0.001 | 5.71 | 4.61 | 11.01 | 9.44 | 14.25 | 1090.70 | <0.001 | 0.70 |
| Right hip | 11.56 | 0.001 | 2.17 | 1.94 | 4.00 | 2.39 | 16.95 | 1494.15 | <0.001 | 0.83 |
| Right knee | 212.30 | <0.001 | 2.90 | 2.80 | 5.76 | 6.00 | 12.13 | 1064.31 | <0.001 | 0.60 |
| Right ankle | 266.49 | <0.001 | 5.93 | 5.37 | 12.43 | 10.07 | 16.12 | 1146.82 | <0.001 | 0.79 |
| Spine shoulder | 0.074 | 0.786 | 2.42 | 1.99 | 2.91 | 2.41 | 4.49 | 1676 | <0.001 | 0.22 |
| Kinect Joint | Boys | Girls | Statistical Significance and Magnitude Differences | ||||
|---|---|---|---|---|---|---|---|
| M | DE | M | DE | F | p | d | |
| Spine base | 2.95 | 2.45 | 2.86 | 2.32 | 2.15 | 0.643 | - |
| Spine mid | 2.03 | 1.67 | 2.41 | 1.94 | 62.34 | <0.001 | 0.22 |
| Neck | 2.77 | 2.15 | 3.62 | 2.72 | 152.60 | <0.001 | 0.37 |
| Head | 3.38 | 2.42 | 3.74 | 2.73 | 127.52 | <0.001 | 0.14 |
| Left shoulder | 2.56 | 2.02 | 3.26 | 2.47 | 1.14 | 0.286 | - |
| Left elbow | 7.44 | 6.03 | 8.43 | 6.06 | 27.58 | <0.001 | 0.16 |
| Left wrist | 13.13 | 10.66 | 14.11 | 9.36 | 13.38 | <0.001 | 0.10 |
| Right shoulder | 2.57 | 2.08 | 3.24 | 2.57 | 129.93 | <0.001 | 0.30 |
| Right elbow | 9.89 | 8.40 | 8.53 | 6.15 | 2.26 | 0.132 | - |
| Right wrist | 17.59 | 15.29 | 14.79 | 10.19 | 3.45 | 0.063 | - |
| Left hip | 3.00 | 2.31 | 3.06 | 2.46 | 4.37 | 0.081 | - |
| Left knee | 3.61 | 3.67 | 4.80 | 4.64 | 41.07 | <0.001 | 0.30 |
| Left ankle | 7.45 | 7.69 | 9.95 | 7.52 | 26.14 | <0.001 | 0.33 |
| Right hip | 2.99 | 2.28 | 3.09 | 2.49 | 4.29 | 0.075 | - |
| Right knee | 3.86 | 4.54 | 5.14 | 5.25 | 5.50 | 0.019 | 0.30 |
| Right ankle | 8.12 | 7.98 | 11.02 | 9.50 | 14.16 | <0.001 | 0.34 |
| Spine shoulder | 2.43 | 2.05 | 3.18 | 2.48 | 143.90 | <0.001 | 0.34 |
| Movement | Levene Test | Experimental Group | Control Group | Statistical Significance and Magnitude Differences | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F | p | M | DE | M | DE | t | g.l. | p | d | |
| Squirm | 0.82 | 0.367 | 8.50 | 4.71 | 5.27 | 4.65 | 2.77 | 63 | 0.007 | 0.69 |
| Leave sit | 0.25 | 0.614 | 1.35 | 3.59 | 1.12 | 3.38 | 0.268 | 62 | 0.790 | - |
| Movement | Levene Test | Experimental Group (without Medication) | Control Group (without Medication) | Statistical Significance and Magnitude Differences | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F | p | M | DE | M | DE | t | g.l. | p | d | |
| Squirm | 0.79 | 0.324 | 8.92 | 4.88 | 16.52 | 12.54 | 3.34 | 24 | 0.003 | 0.80 |
| Leave sit | 0.24 | 0.608 | 1.64 | 3.95 | 5.24 | 12.97 | −1.62 | 24 | 0.118 | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sempere-Tortosa, M.; Fernández-Carrasco, F.; Mora-Lizán, F.; Rizo-Maestre, C. Objective Analysis of Movement in Subjects with ADHD. Multidisciplinary Control Tool for Students in the Classroom. Int. J. Environ. Res. Public Health 2020, 17, 5620. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155620
Sempere-Tortosa M, Fernández-Carrasco F, Mora-Lizán F, Rizo-Maestre C. Objective Analysis of Movement in Subjects with ADHD. Multidisciplinary Control Tool for Students in the Classroom. International Journal of Environmental Research and Public Health. 2020; 17(15):5620. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155620
Chicago/Turabian StyleSempere-Tortosa, Mireia, Francisco Fernández-Carrasco, Francisco Mora-Lizán, and Carlos Rizo-Maestre. 2020. "Objective Analysis of Movement in Subjects with ADHD. Multidisciplinary Control Tool for Students in the Classroom" International Journal of Environmental Research and Public Health 17, no. 15: 5620. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155620