Exploring WHO Communication during the COVID 19 Pandemic through the WHO Website Based on W3C Guidelines: Accessible for All?


Abstract
:1. Introduction
2. Theoretical Framework
2.1. The World Health Organization and COVID-19
2.2. Relevance of Communication and Web Accessibility in Official Organisations
3. Materials and Methods
3.1. Case Study
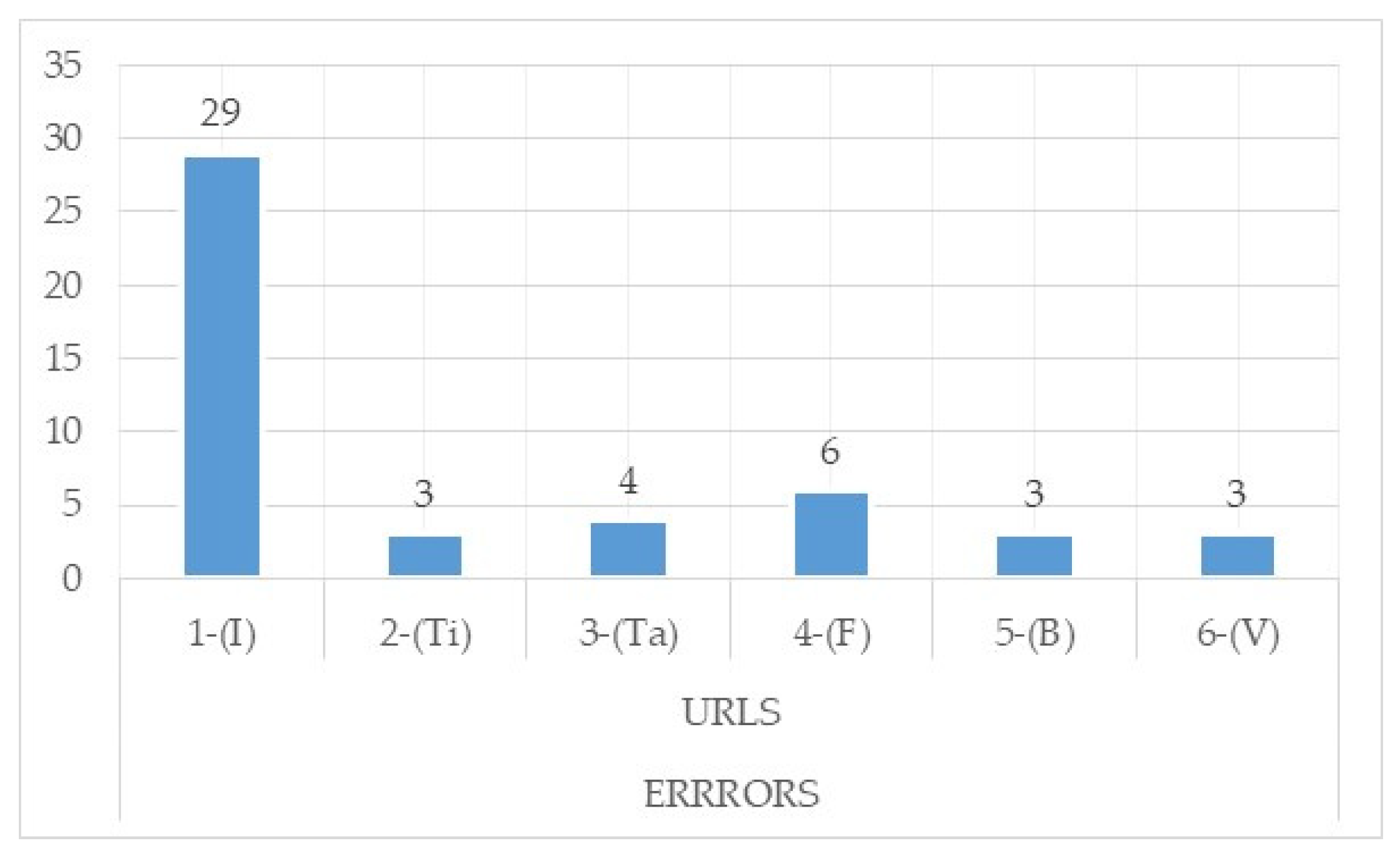
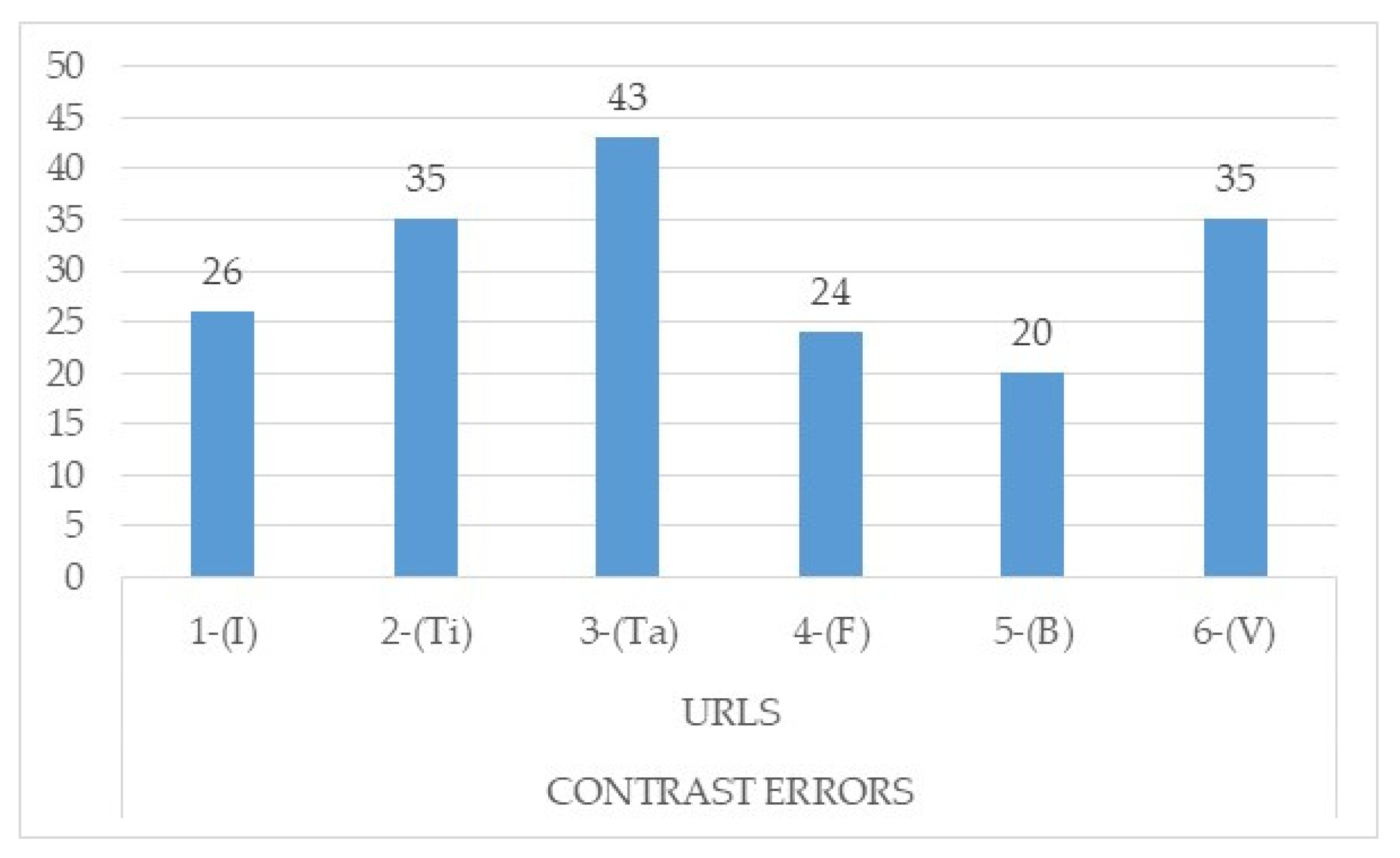
- Home page: the main page of the website.
- Standard page: a second-level reference page of the website that describes the structure of the website.
- Page with tables: a page that shows content laid out using tables.
- Page with forms: registration forms, application forms, information forms, etc.
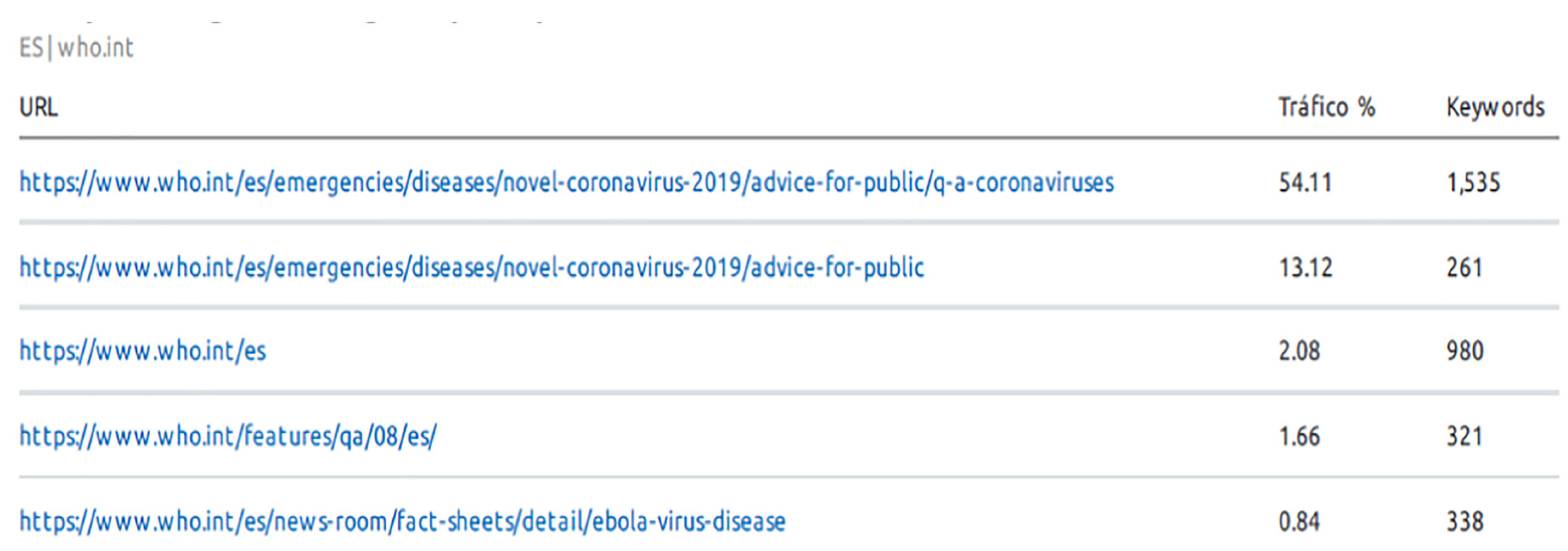
- Result of a search: the information necessary for the location of contents is extracted and checked by means of a keyword search; in this case of analysis, the word “COVID-19” is used as an example.
- Page containing video: to analyse compliance with the guidelines in the case of videos.
3.2. Other Tools Used to Complement the Manual Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| %B-WCAG 2.1 (Level A) | %B-WCAG 2.1 (Level AA) | ||
|---|---|---|---|
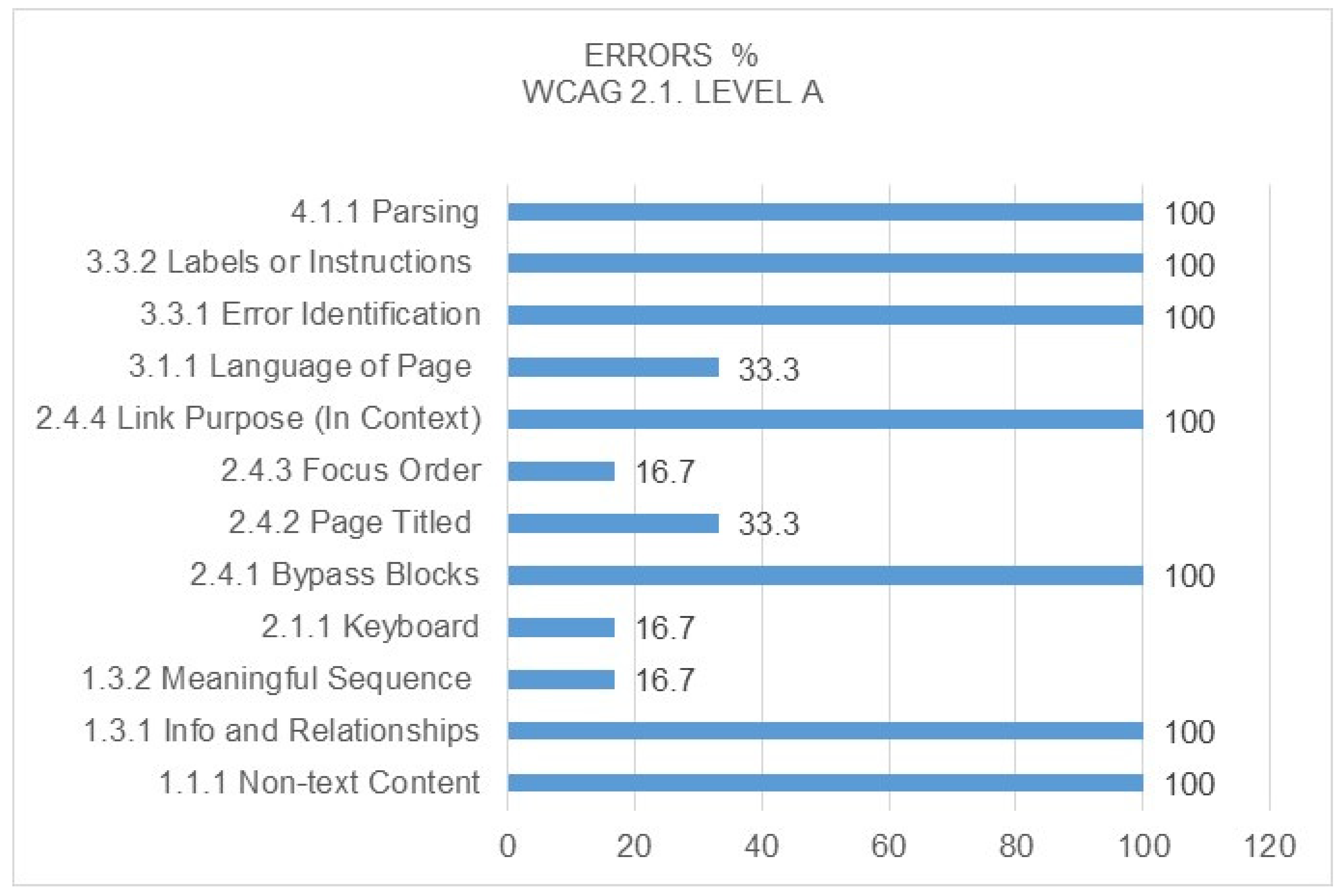
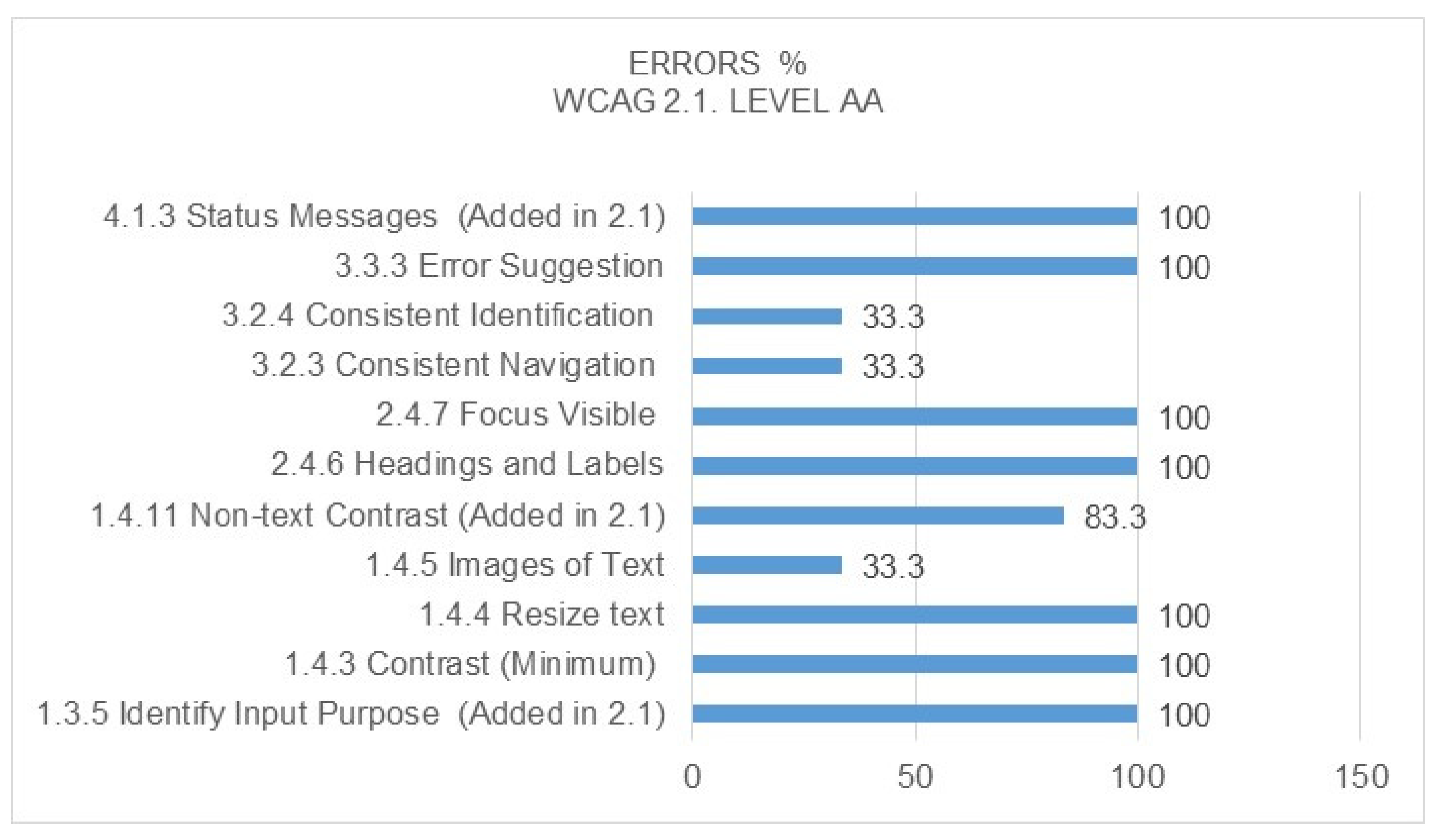
| 1 | Perceivable | 58.1 | 53.5 |
| 2 | Operable | 61.9 | 33.3 |
| 3 | Understandable | 64 | 61.5 |
| 4 | Robust | 50 | 0 |
| Weighted average | 58.5 | 37.1 |
References
- Datareportal. Digital 2020. Global Digital Overview. Available online: https://datareportal.com/reports/digital-2020-global-digital-overview (accessed on 25 March 2020).
- European Parliament’s European Science-Media Hub. ESMH selection: Sources of information about Coronavirus. 2020. Available online: https://sciencemediahub.eu/2020/03/23/esmh-selection-sources-of-information-about-corona-virus/ (accessed on 26 March 2020).
- Oyeyemi, S.O.; Gabarron, E.; Wynn, R. Ebola, Twitter, and misinformation: A dangerous combination? BMJ 2014, 349, g6178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkatraman, A.; Mukhija, D.; Kumar, N.; Nagpal, S.J.S. Zika Virus Misinformation on the Internet. Travel Med. Infect. Dis. 2016, 14, 421–422. [Google Scholar] [CrossRef] [PubMed]
- World Wide Web Consortium (W3C). Objetivos del W3C. Principios: Web para todo el mundo. Available online: https://www.w3c.es/Consorcio/mision (accessed on 25 March 2020).
- Castiel, L.D.; Sanz-Valero, J. El acceso a la información como determinante social de la salud. Nutrición Hospitalaria. Nutr. Hosp. 2010, 25, 26–30. [Google Scholar]
- Moonesinghe, R.; Bouye, K.; Penman-Aguilar, A. difference in health inequity between two population groups due to a social determinant of health. Int. J. Environ. Res. Public Health. 2014, 11, 13074–13083. [Google Scholar] [CrossRef] [Green Version]
- World Wide Web Consortium (W3C). Introducción a la Accesibilidad Web. ¿Qué es la Accesibilidad Web? Available online: https://www.w3c.es/Traducciones/es/WAI/intro/accessibility (accessed on 25 March 2020).
- European Centre for Disease Prevention and Control. Risk Assessment on COVID-19. ECDC Risk Assessment. 2020. Available online: https://www.ecdc.europa.eu/en/current-risk-assessment-novel-coronavirus-situation (accessed on 24 April 2020).
- Balsells, L.A.C.; González, J.C.G.; Balsells, M.A.C.; Chamorro, V.A.P. La accesibilidad de los portales web de las universidades públicas andaluzas. Rev. Española Doc. Científica 2017, 40, 169. [Google Scholar] [CrossRef]
- Da Silva, P.; Alturas, B. Web accessibility: Study of maturity level of Portuguese institutions of higher education. In Proceedings of the 2015 10th Iberian Conference on Information Systems and Technologies (CISTI); Institute of Electrical and Electronics Engineers (IEEE): Aveiro, Portugal, 2015; pp. 1–7. [Google Scholar]
- Ismailova, R.; Kimsanova, G. Universities of the Kyrgyz Republic on the Web: Accessibility and usability. Univers. Access Inf. Soc. 2016, 16, 1017–1025. [Google Scholar] [CrossRef]
- Wahbi, I.; Heider, A.; Alsmadi, I.; Mohammed, N. Evaluating Web Accessibility Metrics for Jordanian Universities. Int. J. Adv. Comput. Sci. Appl. 2016, 7, 113–122. [Google Scholar] [CrossRef] [Green Version]
- Lorca, P.; De Andrés, J.; Martinez-Prieto, A.B. The Relationship Between Web Content and Web Accessibility at Universities. Soc. Sci. Comput. Rev. 2017, 36, 311–330. [Google Scholar] [CrossRef]
- Angarita López, R.D.; Fernández Morales, F.H.; Niño Vega, J.A.; Duarte, J.E.; Gutiérrez Barrios, G.J. Accesibilidad de las revistas colombianas del área de humanidades bajo las pautas WCAG 2.1. Rev. Espacios 2020, 41, 6–18. Available online: http://revistaespacios.com/a20v41n04/20410418.html (accessed on 25 March 2020).
- Bosquez-Barcenes, V.A.; De Bolívar, U.E.; Durango, R.D.P.; Fierro-Saltos, W.R.; Pacheco-Mendoza, S.R.; De Milagro, U.E. Analisis de accesibilidad web en las universitated ecuatorianas para attender las necesidades de estudiantes con discapacidad. Rev. Investig. Enlace Univ. 2019, 18, 129–144. [Google Scholar] [CrossRef] [Green Version]
- Loges, W.E. Canaries in the Coal Mine. Commun. Res. 1994, 21, 5–23. [Google Scholar] [CrossRef]
- Lyu, J.C. How young Chinese depend on the media during public health crises? A comparative perspective. Public Relat. Rev. 2012, 38, 799–806. [Google Scholar] [CrossRef]
- Clift, C. What’s the World Health Organization For? In Final Report from the Centre on Global Health Security Working Group on Health Governance; Chatham House: London, UK, 2014; Available online: https://www.chathamhouse.org/sites/default/files/field/field_document/20140521WHOHealthGovernanceClift.pdf (accessed on 25 March 2020).
- World Health Organization (WHO). Who We Are. Available online: https://www.who.int/es/about/who-we-are (accessed on 25 March 2020).
- World Health Organization (WHO). Countries. Available online: https://www.who.int/countries/en/ (accessed on 25 March 2020).
- World Health Organization (WHO). Ámbitos en los que Trabajamos. Available online: https://www.who.int/es/about/what-we-do (accessed on 25 March 2020).
- World Health Organization (WHO). What Is COVID-19? Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/q-a-coronaviruses (accessed on 25 March 2020).
- World Health Organization. Disability and Health: Key Facts. 2018. Available online: https://www.who.int/es/news-room/fact-sheets/detail/disability-and-health (accessed on 26 March 2020).
- Asociación Española de Comunicación Científica. Lista de Fuentes Fiables Sobre el Nuevo Coronavirus. AECC. 2020. Available online: https://www.aecomunicacioncientifica.org/lista-de-fuentes-fiables-sobre-el-nuevo-coronavirus/ (accessed on 10 April 2020).
- Din, H.N.; McDaniels-Davidson, C.; Nodora, J.; Madanat, H.; Almario, C. Profiles of a Health Information-Seeking Population and the Current Digital Divide: Cross-Sectional Analysis of the 2015–2016 California Health Interview Survey. J. Med. Internet Res. 2019, 21, e11931. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Priorities: Health for All. Available online: https://www.who.int/dg/priorities/health-for-all/en/ (accessed on 26 March 2020).
- Sorokowski, P.; Groyecka, A.; Kowal, M.; Sorokowska, A.; Bialek, M.; Lebuda, I.; Dobrowolska, M.; Zdybek, P.; Karwowski, M. Can information about pandemics increase negative attitudes toward foreign groups? A Case of COVID-19 outbreak. Sustainability 2020, 12, 4912. [Google Scholar] [CrossRef]
- Best, A.; Berland, A.; Greenhalgh, T.; Bourgeault, I.L.; Saul, J.E.; Barker, B. Networks as systems. J. Health Organ. Manag. 2018, 32, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, M. The Concepts and Principles of Equity and Health. Int. J. Health Serv. 1992, 22, 429–445. [Google Scholar] [CrossRef] [PubMed]
- Abeysinghe, S. Pandemics, Science and Policy. H1N1 and the World Health Organisation, Palgrave Macmillan, Series: Palgrave Studies in Science, Knowledge and Policy; Palgrave Macmillan: London, UK, 2015. [Google Scholar]
- Lamb-White, J. World Health Organisation. Int. J. Health Care Qual. Assur. 2007, 20, 20. [Google Scholar] [CrossRef]
- Comité Español de Representantes de Personas con Discapacidad. Derechos humanos y discapacidad. In Informe España 2018; Grupo Editorial Cinca: Madrid, Spain, 2019; Available online: https://www.cermi.es/sites/default/files/docs/colecciones/Informe%202018_ONU.pdf (accessed on 4 June 2020).
- McHale, N. An introduction to web accessibility, Web standards, and web standards makers. J. Web Libr. 2011, 5, 152–160. [Google Scholar] [CrossRef]
- Edworthy, J.; Hellier, E.; Newbold, L.; Titchener, K. Passing crisis and emergency risk communications: The effects of communication channel, information type, and repetition. Appl. Ergon. 2015, 48, 252–262. [Google Scholar] [CrossRef] [Green Version]
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keam, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus disease 2019 (COVID-19): A literature review. J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef]
- Basch, C.H.; Mohlman, J.; Hillyer, G.C.; Garcia, P. Public health communication in time of crisis: Readability of on-line COVID-19 information. Disaster Med. Public Health Prep. 2020, 1–3. [Google Scholar] [CrossRef]
- Brajnik, G. A comparative test of web accessibility evaluation methods. In The 10th International ACM SIGACCESS Conference; Association for Computing Machinery (ACM): Halifax, HX, Canada, 2008; pp. 113–120. [Google Scholar]
- Paddison, C.; Englefield, P. Applying heuristics to perform a rigorous accessibility inspection in a commercial context. ACM SIGCAPH Comput. Phys. Handicap. 2002, 126. [Google Scholar] [CrossRef]
- Abu Shawar, B. Evaluating Web Accessibility of Educational Websites. Int. J. Emerg. Technol. Learn. 2015, 10, 4–10. [Google Scholar] [CrossRef] [Green Version]
- World Wide Web Consortium (W3C). Website Accessibility Conformance Evaluation Methodology. WCAG-EM. 2014, p. 1. Available online: https://www.w3.org/TR/WCAG-EM/ (accessed on 10 April 2020).
- World Wide Web Consortium (W3C). Web Content Accessibility Guidelines (WCAG) Overview. Available online: https://www.w3.org/WAI/standards-guidelines/wcag/ (accessed on 10 April 2020).
- World Wide Web Consortium (W3C). Web Content Accessibility Guidelines 1.0. Available online: https://www.w3.org/TR/WAI-WEBCONTENT/ (accessed on 10 April 2020).
- World Wide Web Consortium (W3C). Web Content Accessibility Guidelines (WCAG) 2.0. Available online: http://www.w3.org/TR/2008/REC-WCAG20-20081211/#conformance-reqs (accessed on 10 April 2020).
- Revilla Muñoz, O.; Carreras Montoto, O. Accesibilidad Web. WCAG 2.1 de Forma Sencilla; Itákora Pres: Madrid, Spain, 2018; pp. 1–264. [Google Scholar]
- World Wide Web Consortium (W3C). Comprender las WCAG 2.0. Available online: http://www.sidar.org/traducciones/wcag20/es/comprender-wcag20/conformance.html (accessed on 15 April 2020).
- World Wide Web Consortium (W3C). How to Meet WCAG. Available online: https://www.w3.org/WAI/WCAG21/quickref/?showtechniques=134¤tsidebar=%23col_customize&versions=2.1 (accessed on 15 April 2020).
- Observatorio de Infoaccesibilidad de Discapnet. Accesibilidad Web en los Portales de Ayuntamientos de Capitales de Provincia. 2008. Available online: https://www.discapnet.es/sites/default/files/areas-tematicas/tecnologia/informedetalleayuntamientos2008.pdf (accessed on 15 April 2020).
- Jandoo, T. WHO guidance for digital health: What it means for researchers. Digit. Health 2020, 6, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Health People 2020. Available online: http://www.healthypeople.gov/2020/default (accessed on 27 June 2020).
- World Wide Web Consortium (W3C). Involving Users in Evaluating Web Accessibility. Available online: https://www.w3.org/WAI/test-evaluate/involving-users/ (accessed on 21 July 2020).









| Principle | Guideline WCAG 2.1 (Success Criteria) | Checkpoints | Level |
|---|---|---|---|
| 1–Perceivable | Guideline 1.1: Text Alternatives | 1.1.1 Non-text Content | A |
| Guideline 1.2: Time-based Media | 1.2.1 Prerecorded Audio-only and Video-only | A | |
| 1.2.2 Captions (Prerecorded) | A | ||
| 1.2.3 Audio Description or Media Alternative (Prerecorded) | A | ||
| Guideline 1.3: Adaptable | 1.3.1 Info and Relationships | A | |
| 1.3.2 Meaningful Sequence | A | ||
| 1.3.3 Sensory Characteristics | A | ||
| Guideline 1.4: Distinguishable | 1.4.1 Use of Color | A | |
| 1.4.2 Audio Control | A | ||
| 2–Operable | Guideline 2.1: Keyboard Accessible | 2.1.1 Keyboard | A |
| 2.1.2 No Keyboard Trap | A | ||
| 2.1.4 Character Key Shortcuts (Added in 2.1) | A | ||
| Guideline 2.2: Enough Time | 2.2.1 Timing Adjustable | A | |
| 2.2.2 Pause, Stop, Hide | A | ||
| Guideline 2.3: Seizures and Physical Reactions | 2.3.1 Three Flashes or Below Threshold | A | |
| Guideline 2.4: Navigable | 2.4.1 Bypass Blocks | A | |
| 2.4.2 Page Titled | A | ||
| 2.4.3 Focus Order | A | ||
| 2.4.4 Link Purpose (In Context) | A | ||
| Guideline 2.5: Input Modalities | 2.5.1 Pointer Gestures (Added in 2.1) | A | |
| 2.5.2 Pointer Cancellation (Added in 2.1) | A | ||
| 2.5.3 Label in Name (Added in 2.1) | A | ||
| 2.5.4 Motion Actuation (Added in 2.1) | A | ||
| 3–Understandable | Guideline 3.1: Readable | 3.1.1 Language of Page | A |
| Guideline 3.2: Predictable | 3.2.1 On Focus | A | |
| 3.2.2 On Input | A | ||
| Guideline 3.3: Input Assistance | 3.3.1 Error Identification | A | |
| 3.3.2 Labels or Instructions | A | ||
| 4–Robust | Guideline 4.1: Compatible | 4.1.1 Parsing | A |
| 4.1.2 Name, Role, Value | A |
| Principle | Guideline WCAG 2.1 (Success Criteria) | Checkpoints | Level |
|---|---|---|---|
| 1–Perceivable | Guideline 1.2: Time-based Media | 1.2.4 Captions (Live) | AA |
| 1.2.5 Audio Description (Prerecorded) | AA | ||
| Guideline 1.3: Adaptable | 1.3.4 Orientation (Added in 2.1) | AA | |
| 1.3.5 Identify Input Purpose (Added in 2.1) | AA | ||
| Guideline 1.4: Distinguishable | 1.4.3 Contrast (Minimum) | AA | |
| 1.4.4 Resize text | AA | ||
| 1.4.5 Images of Text | AA | ||
| 1.4.10 Reflow (Added in 2.1) | AA | ||
| 1.4.11 Non-text Contrast (Added in 2.1) | AA | ||
| 1.4.12 Text Spacing (Added in 2.1) | AA | ||
| 1.4.13 Content on Hover or Focus (Added in 2.1) | AA | ||
| 2–Operable | Guideline 2.4: Navigable | 2.4.5 Multiple Ways | AA |
| 2.4.6 Headings and Labels | AA | ||
| 2.4.7 Focus Visible | AA | ||
| 3–Understandable | Guideline 3.1: Readable | 3.1.2 Language of Parts | AA |
| Guideline 3.2: Predictable | 3.2.3 Consistent Navigation | AA | |
| 3.2.4 Consistent Identification | AA | ||
| Guideline 3.3: Input Assistance | 3.3.3 Error Suggestion | AA | |
| 3.3.4 Error Prevention (Legal, Financial, Data) | AA | ||
| 4–Robust | Guideline 4.1: Compatible | 4.1.3 Status Messages (Added in 2.1) | AA |
| 1.1.1 | 1.2.1; 1.2.2; 1.2.3; 1.4.2 | 1.3.1 | 1.3.2 | 1.3.3 | 1.4.1 | 2.1.1 | 2.1.2 | 2.1.4 | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P | A | B | M | A | B | M | A | B | M | A | B | M | A | B | M | A | B | M | A | B | M | A | B | M | A | B | M | TP | TB | TM | %B | |
| WHO | 6 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0,00 |
| Total | 6 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0,00 |
| Tools | Description | Checkpoints | URL |
|---|---|---|---|
| Mozilla Firefox, Microsoft Internet Explorer, Google Chrome en Android, Safari en iOS | Use zoom out (Control + +) to increase text size and zoom in (control + −) to decrease | 1.4.4 Resize text (AA) | https://www.w3.org/WAI/WCAG21/quickref/?versions=2.0#qr-visual-audio-contrast-scale |
| Google Mobile Friendly | Responsive Design | 1.4.10 Reflow (AA) | https://search.google.com/test/mobile-friendly |
| Accessibility insights | Color Contrast Analyser | 1.4.11 Non-text Contrast (AA) | https://accessibilityinsights.io/docs/en/web/overview |
| CSS Tool | It allows evaluating if the content is cut, overlapping or overflowing | 1.4.12 Text Spacing (AA) | https://www.usableyaccesible.com/archivos/CSS_WCAG21_1_4_12.css |
| PEAT | Detection of epilepsy | 2.3.1 Three Flashes or Below Threshold (A) | http://trace.wisc.edu/edu/peat |
| Validator (X) HTML de W3C | Validator Html | 4.1.1 Parsing (A) | http://validator.w3.org |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Díaz, E.; Iglesias-Sánchez, P.P.; Jambrino-Maldonado, C. Exploring WHO Communication during the COVID 19 Pandemic through the WHO Website Based on W3C Guidelines: Accessible for All? Int. J. Environ. Res. Public Health 2020, 17, 5663. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165663
Fernández-Díaz E, Iglesias-Sánchez PP, Jambrino-Maldonado C. Exploring WHO Communication during the COVID 19 Pandemic through the WHO Website Based on W3C Guidelines: Accessible for All? International Journal of Environmental Research and Public Health. 2020; 17(16):5663. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165663
Chicago/Turabian StyleFernández-Díaz, Elena, Patricia P. Iglesias-Sánchez, and Carmen Jambrino-Maldonado. 2020. "Exploring WHO Communication during the COVID 19 Pandemic through the WHO Website Based on W3C Guidelines: Accessible for All?" International Journal of Environmental Research and Public Health 17, no. 16: 5663. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165663