The Role of the Unitary Prevention Delegates in the Participative Management of Occupational Risk Prevention and Its Impact on Occupational Accidents in the Spanish Working Environment


Abstract
:1. Introduction
2. Materials and Methods
2.1. Source and Sample
2.2. Independent Variable (Presence or Absence of Prevention Delegates)
2.3. Dependent Variables
2.4. Model Adjustment Covariates
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
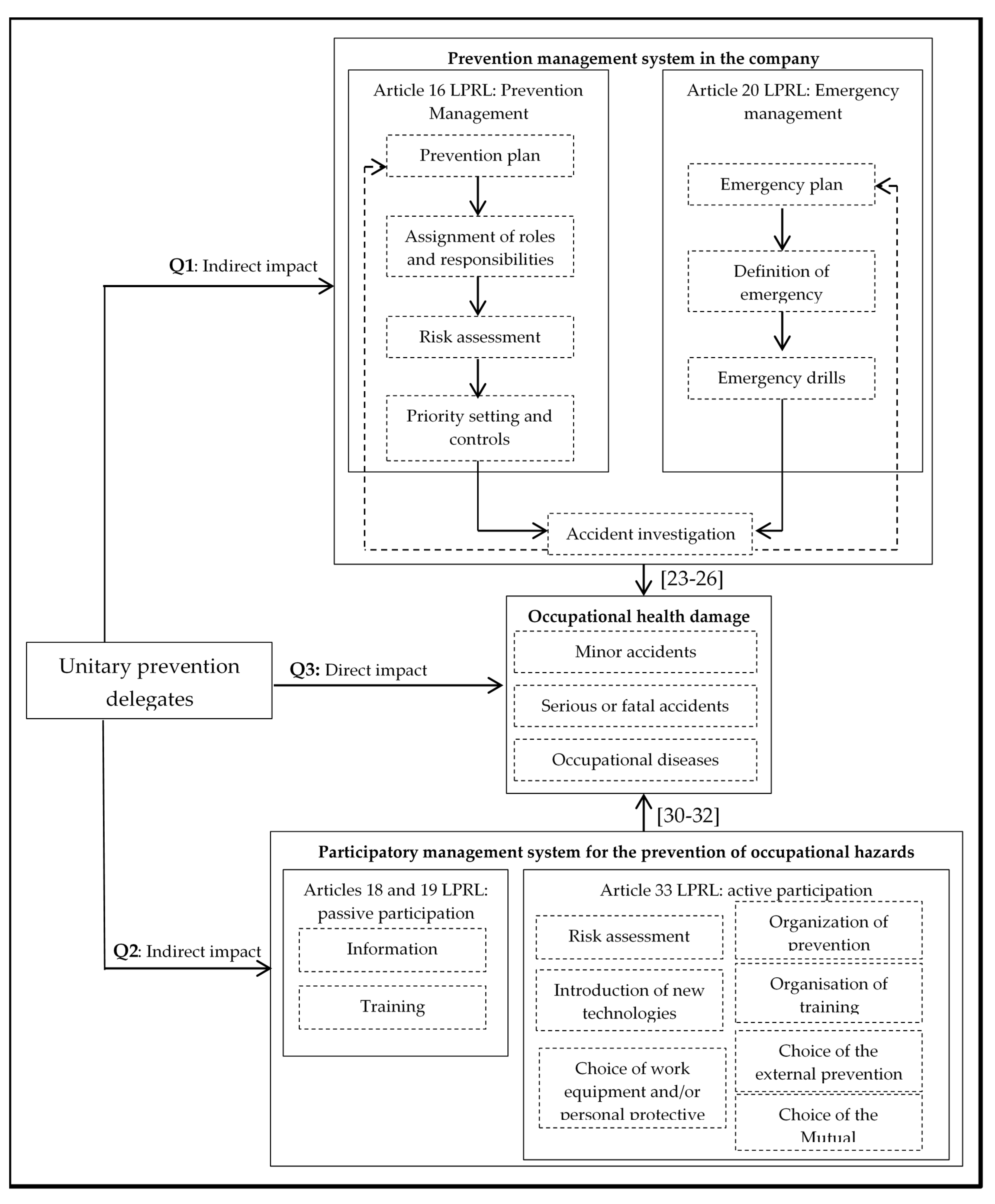
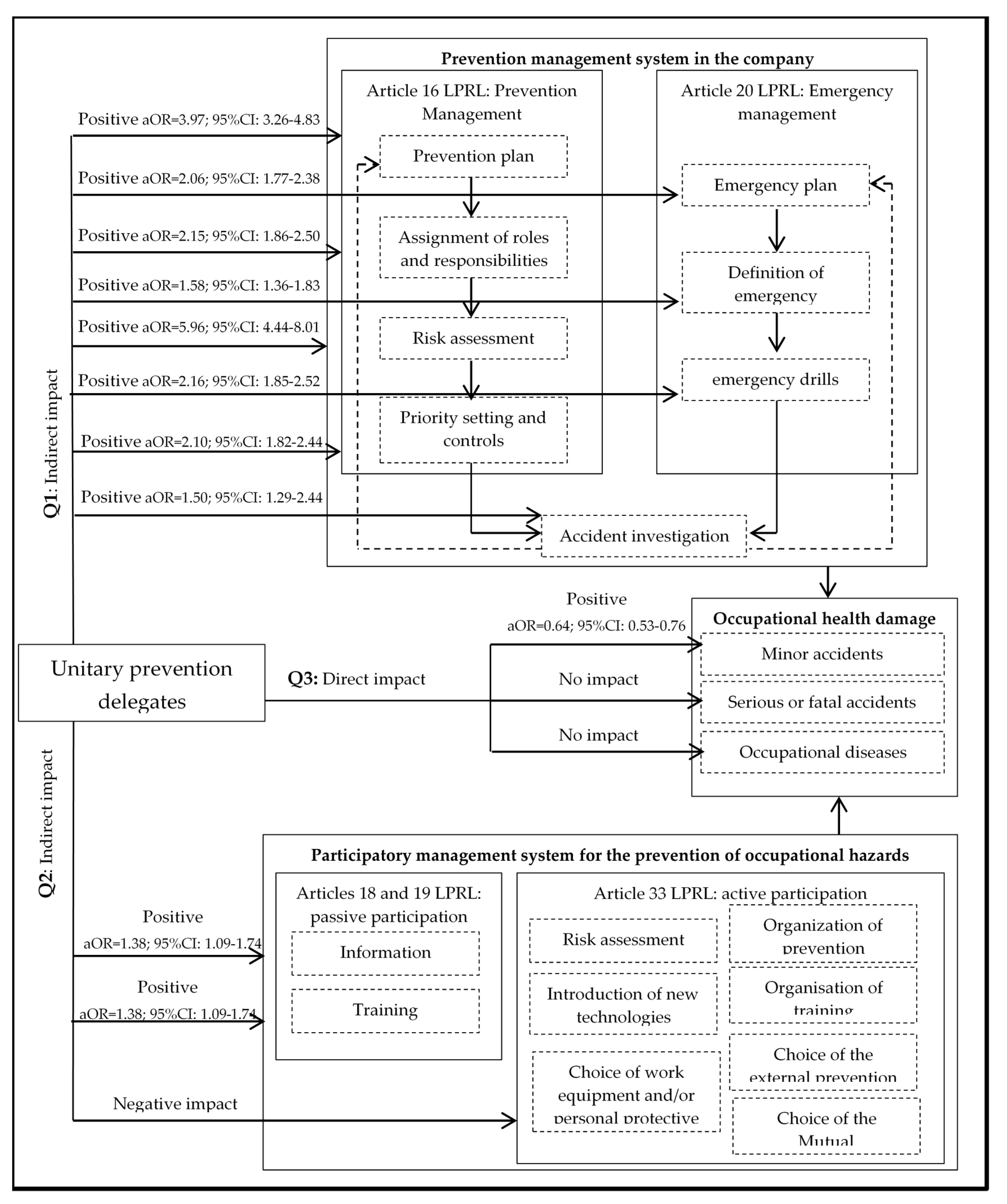
3.1. Impact on Preventive Management
3.2. Impact on the Activation of Participatory Management
3.3. Impact on Occupational Health Damage
3.4. Simplification and Summary of the Participatory Management Model
4. Discussion
Limitations
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Indicator | Category | No. (%) |
|---|---|---|
| Independent variable | ||
| There are unitary prevention delegates in the workplace | ||
| With prevention delegate | 1446 (28.1) | |
| No prevention delegate | 3645 (70.8) | |
| Dependent variables | ||
| Prevention management | ||
| Risks evaluation | ||
| Yes, it has been done | 3344 (78.1) | |
| No it has been carried | 937 (21.9) | |
| Prevention plan | ||
| Yes, it has been done | 3286 (68.6) | |
| No it has been carried | 1501 (31.4) | |
| Assignment of roles and responsibilities | ||
| Yes, it has been done | 1781 (39.3) | |
| No it has been carried | 2747 (60.7) | |
| Preventive planning | ||
| Yes, it has been done | 2907 (61.5) | |
| No it has been carried | 1823 (38.5) | |
| Priority setting and controls | ||
| Yes, it has been done | 2234 (48.7) | |
| No it has been carried | 2358 (51.3) | |
| Emergency plan | ||
| Yes, it has been done | 1607 (35.6) | |
| No it has been carried | 2907 (64.4) | |
| Definition of emergency measures | ||
| Yes, it has been done | 2627 (56.3) | |
| No it has been carried | 2037 (43.7) | |
| Emergency drills | ||
| Yes, it has been done | 1361 (29.7) | |
| No it has been carried | 3223 (70.3) | |
| Accident investigation | ||
| Yes, it has been done | 1774 (39) | |
| No it has been carried | 2.779 (61) | |
| Participation of the workers | ||
| Passive participation | ||
| Information | ||
| Yes | 2836 (85.5) | |
| No | 481 (14.5) | |
| Training | ||
| Yes | 3111 (61.3) | |
| No | 1966 (38.7) | |
| Active participation | ||
| Risks evaluation | ||
| Yes | 2517 (58) | |
| No | 1607 (42) | |
| Introduction of new technologies | ||
| Yes | 1532 (40.1) | |
| No | 2292 (59.9) | |
| Choice of work equipment and/or personal protective equipment | ||
| Yes | 1834 (42.2) | |
| No | 2515 (57.8) | |
| Organisation of prevention | ||
| Yes | 1528 (40) | |
| No | 2293 (60) | |
| Organisation of training | ||
| Yes | 1731 (45.3) | |
| No | 2092 (54.7) | |
| Choice of third-party prevention service | ||
| Yes | 784 (20.5) | |
| No | 3039 (79.5) | |
| Choice of the Mutual | ||
| Yes | 316 (20.3) | |
| No | 1242 (79.7) | |
| Damage to health | ||
| Minor accidents. | 1064 (20.5) | |
| Serious or fatal accidents. | 69 (1.3) | |
| Occupational diseases | 70 (1.4) | |
| Adjustment Covariates | ||
| Size of the company | ||
| <10 | 3793 (74.7) | |
| 10–49 | 1052 (20.6) | |
| 50–249 | 205 (4.0) | |
| 250–499 | 22 (0.4) | |
| ≥500 | 16 (0.3) | |
| Activity sector | ||
| Agriculture | 203 (3.9) | |
| Industry | 818 (15.9) | |
| Construction | 739 (14.4) | |
| Services | 3387 (65.8) | |
| Working conditions (Above average) | ||
| Percentage according to own staff | ||
| Permanent employment | 3180 (61.8) | |
| Temporary | 1491 (29.0) | |
| Percentage according to external staff | ||
| Freelancers | 24 (0.5) | |
| ETT | 73 (1.4) | |
| Outsourced. | 162 (3.1) | |
| Percentage according to work day | ||
| Morning and afternoon | 3542 (68.8) | |
| Continues tomorrow | 1105 (21.5) | |
| Continuous afternoon | 429 (8.3) | |
| Continues at night | 97 (1.9) | |
| Morning and afternoon shifts | 350 (6.8) | |
| Shifts morning, afternoon and night | 156 (3.0) | |
| Percentage according to sex: | ||
| Men | 2549 (49.5) | |
| Women | 2151 (41.8) | |
| Percentage according to nationality | ||
| Nationals | 3405 (66.2) | |
| Foreign | 940 (18.3) | |
| Percentage according to age | ||
| between 16 and 19 years | 217 (4.2) | |
| between 20 and 24 | 1241 (24.1) | |
| between 25 and 54 | 3065 (59.6) | |
| between 55 and 65 | 1221 (23.7) | |
| over 65 years | 129 (2.5) |
References
- Law 31/1995 on the Prevention of Occupational Risks. Available online: https://www.boe.es/buscar/act.php?id=BOE-A-1995-24292 (accessed on 9 June 2020).
- Royal Decree 39/1997 of 17 January 1997, Approving the Prevention Services Regulations. Available online: https://www.boe.es/buscar/act.php?id=BOE-A-1997-1853 (accessed on 9 June 2020).
- Council Directive of 12 June 1989 on the Introduction of Measures to Encourage Improvements in the Safety and Health of Workers at Work. Available online: https://eur-lex.europa.eu/legal-content/ES/TXT/?uri=LEGISSUM%3Ac11113 (accessed on 9 June 2020).
- Benavides, F.; López-Ruiz, M.; Castejón, E. Tendencia secular de las lesiones por accidentes de trabajo en España, 1904–2005. Archivos de Prevención de Riesgos Laborales 2008, 11, 141–147. [Google Scholar]
- Ministry of Labour and Social Economy. Statistics on Accidents at Work. Available online: http://www.mitramiss.gob.es/estadisticas/eat/welcome.htm (accessed on 9 June 2020).
- Payá, R.; Beneyto, P.J. Participación sindical y salud laboral: Una relación positiva. Barataria Revista Castellano-Manchega De Ciencias Sociales 2018, 24, 61–81. [Google Scholar] [CrossRef]
- Benner, M. Before and Beyond the Global Economic Crisis; Edward Elgar: Cheltenham, UK, 2013. [Google Scholar]
- Barranco, O.; Molina, O. Sindicalismo y crisis económica: Amenazas, retos y oportunidades. Kultur 2014, 1, 171–194. [Google Scholar] [CrossRef] [Green Version]
- Beneyto, P.J.; Alós, R.; Jódar, P.; Vidal, S. La afiliación sindical en la crisis Estructura, evolución y trayectorias. Sociología del Trabajo 2016, 87, 25–44. [Google Scholar]
- Gago, A. Crisis, cambio en la UE y estrategias sindicales: El impacto de la condicionalidad en el repertorio estratégico de los sindicatos españoles durante la crisis de la eurozona. Revista Española de Ciencia Política 2016, 42, 45–68. [Google Scholar] [CrossRef] [Green Version]
- Lehndorff, S. Acting in different worlds. Challenges to transnatio-nal trade union cooperation in the Eurozone crisis. Transf. Eur. Rev. Labour. Res. 2015, 21, 157–170. [Google Scholar] [CrossRef]
- Alós, R.; Beneyto, P.J.; Jódar, P. Reforma laboral i desregulació del mercat de treball. Anuario IET de Trabajo y Relaciones Laborales 2017, 4, 73–86. [Google Scholar] [CrossRef] [Green Version]
- Cabrera-León, A.; Daponte, A.; Mateo, I.; Arroyo-Borrell, E.; Bartoll, X.; Bravo, M.J.; Bernal, M.; Renart, G.; Álvarez-Dardet, C.; Marí-Dell’Olmo, M.; et al. Indicadores contextuales para evaluar los determinantes sociales de la salud y la crisis económica española. Gac. Sanit. 2017, 31, 194–203. [Google Scholar] [CrossRef] [Green Version]
- Ferrando, J.; Palència, L.; Gotsens, M.; Puig-Barrachina, V.; Marí-Dell’olmo, M.; Rodríguez-Sanz, M.; Borrell, C. Trends in cancer mortality in Spain: The influence of the financial crisis. Gac. Sanit. 2019, 33, 229–234. [Google Scholar] [CrossRef]
- Porthé, V.; Vargas, I.; Ronda, E.; Malmusi, D.; Bosch, L.; Vázquez, M.L. Has the quality of health care for the immigrant population changed during the economic crisis in Catalonia (Spain)? Opinions of health professionals and immigrant users. Gac. Sanit. 2018, 32, 425–432. [Google Scholar] [CrossRef]
- Eurostat. Accidents at Work by Sex, Age and Severity (NACE Rev. 2 Activity A, C-N). Available online: https://data.europa.eu/euodp/es/data/dataset/rtRELcj5tHiQsy9thjh26g (accessed on 9 June 2020).
- Lewchuk, W.; Wolff, A.; King, A.; Polanyi, M. From job strain to employment strain: Health effects of precarious employment. Just Labour 2003, 3, 23–35. [Google Scholar] [CrossRef] [Green Version]
- García-Mainar, I.; Montuenga-Gómez, V. Causas de los accidentes de trabajo en España: Análisis longitudinal con datos de panel. Gac. Sanit. 2009, 23, 174–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benavides, F.; Benach, J.; Muntaner, C.; Delclós, J.; Catot, N.; Amable, M. Associations between temporary employment and occupational injury: What are the mechanisms? Occup. Env. Med. 2006, 63, 416–421. [Google Scholar] [CrossRef]
- Payá, R. Seguridad y salud laboral en el área mediterránea de relaciones laborales: Factores determinantes y análisis comparado. Aposta Revista de Ciencias Sociales 2020, 84, 25–44. [Google Scholar]
- Eurostat. Temporary Employees as Percentage of the Total Number of Employees, by Sex, Age and Citizenship (%). Available online: https://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=lfsa_etpgan&lang=en (accessed on 9 June 2020).
- Terrés, F.; Rodríguez, P.; Álvarez, E.; Castejón, E. Economic fluctuations affecting occupational safety. The Spanish case. Occup. Ergon. 2004, 4, 211–228. [Google Scholar]
- Arocena, P.; Núñez, I. An empirical analysis of the effectiveness of occupational health and safety management systems in SMEs. Int. Small Bus. J. 2010, 28, 398–419. [Google Scholar] [CrossRef]
- Fernández-Muñiz, B.; Montes-Peón, J.M.; Vázquez-Ordás, C.J. Relation between occupational safety management and firm performance. Saf. Sci. 2009, 47, 980–991. [Google Scholar] [CrossRef]
- Autenrieth, D.A.; Brazile, W.J.; Douphrate, D.I.; Román-Muñiz, I.N.; Reynolds, S.J. Comparing Occupational Health and Safety Management System Programming with Injury Rates in Poultry Production. J. Agromed. 2016, 21, 364–372. [Google Scholar] [CrossRef]
- Autenrieth, D.A.; Brazile, W.J.; Sandfort, D.R.; Douphrate, D.I.; Román-Muñiz, I.N.; Reynolds, S.J. The associations between occupational health and safety management system programming level and prior injury and illness rates in the U.S. dairy industry. Saf. Sci. 2016, 84, 108–116. [Google Scholar] [CrossRef]
- Boustras, G.; Guldenmund, F.W. The effects of the global financial crisis on Occupational Safety and Health (OSH): Effects on the workforce and organizational safety systems. Saf. Sci. 2018, 106, 244–245. [Google Scholar] [CrossRef]
- Anyfantis, I.; Boustras, G.; Karageorgiou, A. Maintaining occupational safety and health levels during the financial crisis—A conceptual model. Saf. Sci. 2018, 106, 246–254. [Google Scholar] [CrossRef]
- Sønderstrup-Andersen, H.H.K.; Bach, E. Managing preventive occupational health and safety activities in Danish enterprises during a period of financial crisis. Saf. Sci. 2018, 106, 291–301. [Google Scholar] [CrossRef] [Green Version]
- Payá Castiblanque, R. The Impact of the Direct Participation of Workers on the Rates of Absenteeism in the Spanish Labor Environment. Int. J. Env. Res. Public Health 2020, 17, 2477. [Google Scholar] [CrossRef] [Green Version]
- Feng, Y. Effect of safety investments on safety performance of building projects. Saf. Sci. 2013, 59, 28–45. [Google Scholar] [CrossRef]
- Robinson, A.M.; Smallman, C. Workplace injury and voice: A comparison of management and union perceptions. Work Employ. Soc. 2013, 27, 674–693. [Google Scholar] [CrossRef]
- Walters, D.; Wadsworth, E. Participation in safety and health in European workplaces: Framing the capture of representation. Eur. J. Industr. Relat. 2020, 26, 75–90. [Google Scholar] [CrossRef]
- Gracía, A.M.; López-Jacob, M.J.; Díaz-Gómez, J.R. La protección de la salud de los trabajadores en España: Una oportunidad para la participación, la negociación y el consenso en el marco de las relaciones laborales. Trab. Rev. Iberoam. Relac. Labor. 2013, 28, 39–53. [Google Scholar]
- Santos, A.; Gabaldon, D.; Grau, A.; Ingellis, A.; Muñoz, D. Country report—SPAIN: Worker Participation in the Management of Occupational Safety and Health—Qualitative Evidence from ESENER-2. Available online: https://osha.europa.eu/en/publications/country-report-spain-worker-participation-managementoccupational-safety-and-health/view (accessed on 1 April 2020).
- Rainhorn, J. Le mouvementouvriercontre la peinture au plomb. Stratégiesyndicale, experience locale et transgression du discours dominant au débutdu XXe siècle. Politix 2010, 23, 7–26. [Google Scholar] [CrossRef]
- Vogel, L. La actualidad del modelo obrero italiano para la lucha a favor de la salud en el trabajo. Laboreal 2016, 12, 10–17. [Google Scholar] [CrossRef]
- Nichols, T.; Walters, D. Representation and consultation on health and safety in chemicals: An exploration of limits to the preferred model. Empl. Relat. 2006, 28, 230–254. [Google Scholar] [CrossRef]
- Coutrot, T. Le rôle des comités d´hygiène, de sécurité et des conditios de travail en France: Une analyse empirique. Travail et Emploi 2009, 17, 25–38. [Google Scholar] [CrossRef]
- Ollé-Espluga, L.; Vergara-Duarte, M.; Belvis, F.; Menéndez-Fuster, M.; Jódar, P.; Benach, J. What is the impact on occupational health and safety when workers knowthey have safety representatives? Saf. Sci. 2015, 74, 55–58. [Google Scholar] [CrossRef] [Green Version]
- Nichols, T.; Walters, D.; Tasiran, A.C. Trade unions, institutional mediation and industrial safety—Evidence from the UK. J. Ind. Relat. 2007, 49, 211–226. [Google Scholar] [CrossRef]
- Kazutaka, K. Roles of Participatory Action-oriented Programs in Promoting Safety and Health at Work. Saf. Health Work 2012, 3, 155–165. [Google Scholar] [CrossRef] [Green Version]
- Reilly, B.; Paci, P.; Holl, P. Unions, safety committees and workplace injuries. Br. J. Indust. Relat. 1995, 33, 275–288. [Google Scholar] [CrossRef]
- Walters, D.; Nichols, T. Worker Representation and Workplace Health and Safety; Palgrave Macmillan: Basingstoke, UK, 2007. [Google Scholar]
- Menéndez, M.; Benach, J.; Vogel, L. The Impact of Safety Representatives on Occupational Health. A European Perspective; The EPSARE Project; European Trade Union Institute (ETUI): Brussels, Belgium, 2009. [Google Scholar]
- Walters, D.; Wadsworth, E.J.K. Contexts and determinants of the management of occupational safety and health in European workplaces. Policy Pract. Health Saf. 2014, 12, 109–130. [Google Scholar] [CrossRef]
- Wadsworth, E.J.K.; Walters, D. The determinants of workplace health and safety practice in the UK. Policy Pract. Health Saf. 2014, 12, 3–22. [Google Scholar] [CrossRef]
- Peters, S.E.; Nielsen, K.M.; Nagler, E.M.; Revette, A.C.; Madden, J.; Sorensen, G. Ensuring Organization-Intervention Fit for a Participatory Organizational Intervention to Improve Food Service Workers’ Health and Wellbeing: Workplace Organizational Health Study. J. Occup. Environ. Med 2020, 62, 33–45. [Google Scholar] [CrossRef]
- Johnston, D.; Pagell, M.; Veltri, A.; Klassen, R. Values-in-action that support safe production. J. Saf. Res. 2020, 72, 75–91. [Google Scholar] [CrossRef]
- Yassi, A.; Lockhart, K.; Sykes, M.; Buck, B.; Stime, B.; Spiegel, J.M. Effectiveness of joint health and safety committees: A realist review. Am. J. Ind. Med. 2013, 56, 424–438. [Google Scholar] [CrossRef]
- Hasle, P.; Seim, R.; Refslund, B. From employee representation to problem-solving: Mainstreaming OHS management. Econ. Indust. Democr. 2019, 40, 662–681. [Google Scholar] [CrossRef] [Green Version]
- Yoshikawa, E.; Kogi, K. Outcomes for facilitators of workplace environment improvement applying a participatory approach. J. Occup. Health 2019, 61, 415–425. [Google Scholar] [CrossRef] [Green Version]
- Rutz, S.; Mathew, D.; Robben, P.; de Bont, A. Enhancing responsiveness and consistency: Comparing the collective use of discretion and discretionary room at inspectorates in England and the Netherlands. Regul. Gov. 2017, 11, 81–94. [Google Scholar] [CrossRef] [Green Version]
- Walters, D.; Quinlan, M. Voice and resistance: Coalminers’ struggles to represent their health and safety interests in Australia and New Zealand 1871–1925. Econ. Lab. Relat. Rev. 2019, 30, 513–531. [Google Scholar] [CrossRef]
- Frick, K. Resilience within a weaker work environment system: The position and influence of Swedish safety representatives. In Safety or Profit? International Studies in Governance, Change and the Work Environment; Nichols, T., Walters, D., Eds.; Baywood Publishing: New York, NY, USA, 2013; pp. 51–70. [Google Scholar]
- Walters, D.; Johnstone, R.; Quinlan, M.; Wadsworth, E.; Jane, K. Safeguarding workers: A study of health and safety representatives in the Queensland coal mining industry, 1990–2013. Relat. Ind. 2016, 71, 418–441. [Google Scholar] [CrossRef]
- Walters, D.; Quinlan, M.; Johnstone, R.; Wadsworth, E. Cooperation or resistance? Representing workers’ health and safety in a hazardous industry. Ind. Relat. J. 2016, 47, 379–395. [Google Scholar] [CrossRef]
- Payá, R.; Beneyto, P.J. Intervención sindical y salud laboral en la Unión Europea: Dimensiones, cobertura e impacto. Methaodos.Revista de Ciencias Sociales 2018, 6, 210–226. [Google Scholar] [CrossRef] [Green Version]
- García, A.M.; Benavides, F. Determinants of Workplace Occupational Safety and Health Practice in Spain. Policy Pract. Health Saf. 2014, 12, 67–87. [Google Scholar] [CrossRef]
- Crouch, C. Membership density and trade union power. Transf. Eur. Rev. Lab. Res. 2017, 23, 47–61. [Google Scholar] [CrossRef] [Green Version]
- Beneyto, P.J. Representación sindical en la Unión Europea y España: Estructura, cobertura y nuevos retos. Acciones e Investigaciones Sociales 2018, 38, 37–62. [Google Scholar] [CrossRef] [Green Version]
- INSHT. Encuesta Nacional de Gestión de la Seguridad y Salud en las Empresa (ENGE 2009). Instituto Nacional de Seguridad e Higiene en el Trabajo. Available online: http://istas.net/descargas/Informe_%20ENGE%202009.pdf (accessed on 11 June 2020).
- Hall, A.; Forrest, A.; Sears, A.; Carlan, N. Making a Difference: Knowledge Activism and Worker Representation in Joint OHS Committees. Relat. Ind. 2006, 61, 408–436. [Google Scholar] [CrossRef] [Green Version]
- Tucker, E. Worker health and safety struggles: Democraticpossibilities and constraints. New Solut. J. Environ. Occup. Health Policy 1996, 6, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Ollé-Espluga, L.; Menéndez-Fuster, M.; Muntaner, C.; Benach, J.; Vergara-Duarte, M.; Vázquez, M.L. Safety representatives’ views on their interaction with workers in a context of unequal power relations: An exploratory qualitative study in Barcelona (Spain). Am. J. Ind. Med. 2014, 57, 338–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EU-OSHA. Third European Survey of Enterprises on New and Emerging Risks (ESENER 3). European Agency for Safety and Health at Work. Available online: https://visualisation.osha.europa.eu/esener#!/es/survey/detailpage-european-bar-chart/2019/drivers-and-barriers/es/E3Q262_5/activity-sector/14/11 (accessed on 21 June 2020).
- Hovden, J.; Lie, T.; Karlsen, J.E.; Alteren, B. The safety representativeunder pressure. A study of occupational health and safety managementin the Norwegian oil and gas industry. Saf. Sci. 2008, 46, 493–509. [Google Scholar] [CrossRef]
- Gunningham, N. Occupational health and safety, workerparticipation and the mining industry in a changing world of work. Econ. Ind. Democr. 2008, 29, 336–361. [Google Scholar] [CrossRef]
- Gumbrell-McKornincks, R.; Hyman, R. Trade Unions in Western Europe; Oxford University Press: Oxford, UK, 2013. [Google Scholar]
- Lippel, K.; Walters, D. Regulating health and safety and workers’ compensation in Canada for the mobile workforce: Now you see them, now you don’t. New Solut. J. Environ. Occup. Health Policy 2019, 29, 317–348. [Google Scholar] [CrossRef]
- Conghua, X.; Tang, L.; Walters, D. Who is dominant? Occupational health and safety management in Chinese shipping. J. Indust. Relat. 2017, 59, 65–84. [Google Scholar] [CrossRef] [Green Version]
- INSHT. La Gestión Preventiva de las Empresas en España. Year 2016. Instituto Nacional de Seguridad e Higiene en el Trabajo. Available online: https://www.insst.es/documents/94886/603437/La+gesti%C3%B3n+preventiva+en+las+empresas+en+Espa%C3%B1a.+A%C3%B1o+2016/183ab502-f657-489c-a575-689e884ccb84 (accessed on 22 June 2020).



| No Prevention Delegate No. (%) A | With Prevention Delegate No. (%) A | p-Value B | |
|---|---|---|---|
| Company size | 0.000 | ||
| <10 | 3053 (80.5) | 740 (19.5) | |
| 10–49 | 537 (51) | 515 (49) | |
| 50–249 | 50(24.4) | 155 (75.6) | |
| 250–499 | 3 (13.6) | 19 (86.4) | |
| = >500 | 0 (0) | 16 (100) | |
| Sector of activity | 0.000 | ||
| Agriculture | 154 (75.9) | 49 (24.1) | |
| Industry | 496 (61.4) | 312 (38.6) | |
| Construction | 500 (67.8) | 238 (32.2) | |
| Services | 2496 (74.7) | 847 (25.3) |
| Dimensions | Indicator | Category |
|---|---|---|
| Independent variable |
| 1 = With prevention delegate 2 = No prevention delegate |
| Dependent variables | ||
| Prevention management | It has been carried out in the workplace:
| 1 = Yes, it has been done 2 = No, it has been carried out or is planned |
| Participation of the workers | Passive participation:
| 1 = Yes 2 = No |
| Damage to health | Health damage produced in the last two years:
| 1 = Yes 2 = No |
| Adjustment Covariates | ||
| Company type |
| 1 ≤ 10 2 = 10–49 3 = 50–249 4 = 250–499 5 ≥ 500 |
| 1 = Agriculture 2 = Industry 3 = Construction 4 = Services | |
| Working conditions | Percentage according to own staff
| 1-Above average. 2-Below average |
| Indicator | No Prevention Delegate | With Prevention Delegate | cOR (95% CI) C | aOR (95% CI) D |
|---|---|---|---|---|
| N (%) A | N (%) B | |||
| Risks evaluation | 2213 (71.8) | 1131 (94.3) | 6.45 (4.99–8.32) E | 5.96 (4.44–8.01) E |
| Prevention plan | 2088 (60.8) | 1198 (88.5) | 4.96 (4.14–5.95) E | 3.97 (3.26–4.83) E |
| Assignment of roles and responsibilities | 1042 (32.2) | 739 (57.2) | 2.82 (2.47–3.22) E | 2.15 (1.86–2.50) E |
| Preventive planning | 1802 (53.4) | 1105 (81.5) | 3.84 (3.30–4.48) E | 3.01 (2.55–3.56) E |
| Priority setting and controls | 1365 (41.7) | 869 (65.9) | 2.71 (2.37–3.09) E | 2.10 (1.82–2.44) E |
| Emergency plan | 948 (29.5) | 659 (50.7) | 2.46 (2.16–2.81) E | 2.06 (1.77–2.38) E |
| Definition of emergency measures | 1704 (51.2) | 923 (69.1) | 2.13 (1.86–2.44) E | 1.58 (1.36–1.83) E |
| Emergency drills | 762 (23.4) | 599 (45.1) | 2.69 (2.36–3.09) E | 2.16 (1.85–2.52) E |
| Accident investigation | 1055 (32.6) | 719 (54.6) | 4.48 (2.17–2.82) E | 1.50 (1.29–1.74) E |
| Indicator | No Prevention Delegate | With Prevention Delegate | cOR (95% CI) C | aOR (95% CI) D |
|---|---|---|---|---|
| N (%) A | N (%) B | |||
| Passive participation | ||||
| Information | 1838 (84.1) | 998 (88.2) | 1.41 (1.14–1.74) F | 1.38 (1.09–1.74) F |
| Training | 1915 (52.7) | 1196 (82.9) | 4.35 (3.74–5.06) E | 3.51 (2.97–4.15) E |
| Active participation | ||||
| Risk assessment | 1611 (64.0) | 604 (46.3) | 0.48 (0.42–0.55) E | 0.47 (0.40–0.55) E |
| Introduction of new technologies | 1140 (45.3) | 392 (30.0) | 0.52 (0.45–0.60) E | 0.57 (0.49–0.67) E |
| Choice of work equipment and/or personal protective equipment | 1273 (50.6) | 561 (30.6) | 0.74 (0.64–0.84) E | 0.71 (0.61–0.82) E |
| Organisation of prevention | 1125 (44.7) | 403 (30.9) | 0.55 (0.48–0.64) E | 0.61 (0.52–0.71) E |
| Organisation of training | 1296 (51.5) | 435(33.3) | 0.47 (0.41–0.54) E | 0.49 (0.42–0.57) E |
| Choice of the external prevention service | 590 (23.4) | 194 (14.9) | 0.57 (0.48–0.68) E | 0.71 (0.58–0.86) F |
| Choice of the Mutual | 81 (32.2) | 235 (18.0) | 0.46 (0.39–0.54) E | 0.57 (0.48–0.69) E |
| Minor Work Accidents A | Serious or Fatal Accidents at Work A | Occupational Diseases A | ||||
|---|---|---|---|---|---|---|
| aOR (95% CI) B | p- Value | aOR (95% CI) B | p- Value | aOR (95% CI) B | p- Value | |
| There is a unitary prevention delegate | ||||||
| No | 1 C | 1 C | 1 C | |||
| Yes | 0.64 (0.53–0.76) | 0.000 | 0.92 (0.51–1.66) | 0.785 | 1.53 (0.84–2.76) | 0.163 |
| Socio-demographic adjustment variables | ||||||
| Company size | ||||||
| <10 | 1 C | 1 C | 1 C | |||
| 10–49 | 2.46 (2.03–2.97) | 0.000 | 5.27 (2.52–11.01) | 0.000 | 5.05 (2.59–9.87) | 0.000 |
| 50–249 | 4.08 (3.32–6.96) | 0.000 | 12.18 (4.71–31.47) | 0.000 | 8.56 (3.08–23.76) | 0.000 |
| 250–499 | 8.66 (5.43–30.84) | 0.001 | 115.6 (23.5–566.6) | 0.000 | 6.20 (0.66–58.0) | 0.110 |
| => 500 | 3.85 (1.16–12.73) | 0.000 | 23.13 (2.96–180.4) | 0.000 | 26.6 (3.94–180.5) | 0.001 |
| Activity sector | ||||||
| Agriculture | 1 C | 1 C | 1 C | |||
| Industry | 0.98 (0.67–1.44) | 0.925 | 0.81 (0.25–2.62) | 0.728 | 1.12 (0.25–5.07) | 0.881 |
| Construction | 1.90 (1.30–2.78) | 0.001 | 1.04 (0.33–3.31) | 0.943 | 1.13 (0.24–5.26) | 0.877 |
| Services | 0.43 (0.30–0.62) | 0.000 | 0.36 (0.11–1.14) | 0.083 | 0.83 (0.20–5.26) | 0.807 |
| Percentage according to own staff D | ||||||
| Undefined | 1.08 (0.83–1.41) | 0.573 | 0.28 (0.10–0.74) | 0.011 | 0.65 (0.27–1.56) | 0.336 |
| Temporary | 1.35 (1.04–1.75) | 0.027 | 0.34 (0.13–0.94) | 0.037 | 0.53 (0.22–1.27) | 0.155 |
| Percentage according to external staff D | ||||||
| Freelancers | 5.76 (1.99–16.65) | 0.000 | 0.12 (0.01–5.32) | 0.274 | 0.75 (0.08–7.38) | 0.807 |
| ETT | 0.44 (0.22–0.88) | 0.021 | 0.57 (0.12–2.75) | 0.485 | 1.06 (0.40–2.78) | 0.914 |
| Subcontractor | 2.91 (1.91–4.45) | 0.001 | 3.07 (1.36–6.93 | 0.007 | 0.56 (0.22–1.44) | 0.474 |
| Percentage according to working day D | ||||||
| Morning and afternoon | 1.13 (0.82–1.55) | 0.459 | 0.79 (0.30–2.08) | 0.627 | 2.60 (1.06–6.38) | 0.038 |
| Continues tomorrow | 0.99 (0.73–1.34) | 0.952 | 1.00 (0.40–2.46) | 0.994 | 1.96 (0.92–4.18) | 0.080 |
| Continuous afternoon | 1.90 (1.38–2.62) | 0.000 | 1.16 (0.41–3.25) | 0.784 | 1.80 (0.75–4.33) | 0.190 |
| Continues at night | 0.77 (0.69–1.45) | 0.363 | 2.00 (0.61–6.63) | 0.255 | 0.73 (0.15–3.57) | 0.700 |
| Morning and afternoon shifts | 1.00 (0.69–1.45) | 0.997 | 2.23 (0.89–5.60) | 0.088 | 2.83 (1.21–6.67) | 0.017 |
| Shifts morning, afternoon and night | 5.26 (3.38–8.19) | 0.000 | 0.76 (0.24–2.38) | 0.632 | 6.01 (2.45–14.71) | 0.000 |
| Percentage according to sex D | ||||||
| Men | 1.29 (1.11–1.51) | 0.001 | 0.96 (0.56–1.63) | 0.874 | 0.48 (0.29–0.82) | 0.006 |
| Women | 0.83 (0.61–1.14) | 0.384 | 0.25 (0.08–0.81) | 0.021 | 0.29 (0.10–0.76) | 0.013 |
| Percentage according to nationality D | ||||||
| Nationals | 0.97 (0.74–1.26) | 0.804 | 1.51 (0.61–3.71) | 0.373 | 0.56 (0.22–1.44) | 0.228 |
| Foreign | 1.01 (0.78–1.32) | 0.931 | 0.97 (0.42–2.26) | 0.944 | 0.20 (0.07–0.61) | 0.004 |
| Percentage according to age D | ||||||
| Between 16 and 19 years | 1.19 (0.84–1.68) | 0.335 | 1.39 (0.55–3.50) | 0.482 | 2.66 (1.22–5.80) | 0.014 |
| Between 20 and 24 | 1.48 (1.20–1.82) | 0.000 | 1.47 (0.78–2.78) | 0.235 | 3.03 (1.66–5.51) | 0.000 |
| Between 25 and 54 | 1.47 (1.18–1.83) | 0.001 | 0.96 (0.49–1.91) | 0.916 | 2.37 (1.10–5.11) | 0.028 |
| Between 55 and 65 | 1.71 (1.40–2.09) | 0.000 | 1.93 (1.04–3.59) | 0.037 | 1.11 (0.58–2.15) | 0.746 |
| Over 65 years | 3.09 (1.98–4.80) | 0.000 | 0.86 (0.23–3.28) | 0.828 | 2.45 (0.72–8.30) | 0.150 |
| Chi squared | 1062,416 | 0.000 | 182,161 | 0.000 | 132,867 | 0.000 |
| Cox and Snell R2 | 0.194 | 0.036 | 0.027 | |||
| R2 Nagelkerke | 0.303 | 0.275 | 0.198 | |||
| Population | 5147 | 5147 | 5147 | |||
| Number of valid cases and percentage | 4812 (93.5%) | 4809 (93.4%) | 4809 (93.4%) | |||
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Payá Castiblanque, R. The Role of the Unitary Prevention Delegates in the Participative Management of Occupational Risk Prevention and Its Impact on Occupational Accidents in the Spanish Working Environment. Int. J. Environ. Res. Public Health 2020, 17, 5678. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165678
Payá Castiblanque R. The Role of the Unitary Prevention Delegates in the Participative Management of Occupational Risk Prevention and Its Impact on Occupational Accidents in the Spanish Working Environment. International Journal of Environmental Research and Public Health. 2020; 17(16):5678. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165678
Chicago/Turabian StylePayá Castiblanque, Raúl. 2020. "The Role of the Unitary Prevention Delegates in the Participative Management of Occupational Risk Prevention and Its Impact on Occupational Accidents in the Spanish Working Environment" International Journal of Environmental Research and Public Health 17, no. 16: 5678. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165678