Heatwave-Related Mortality Risk and the Risk-Based Definition of Heat Wave in South Korea: A Nationwide Time-Series Study for 2011–2017

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
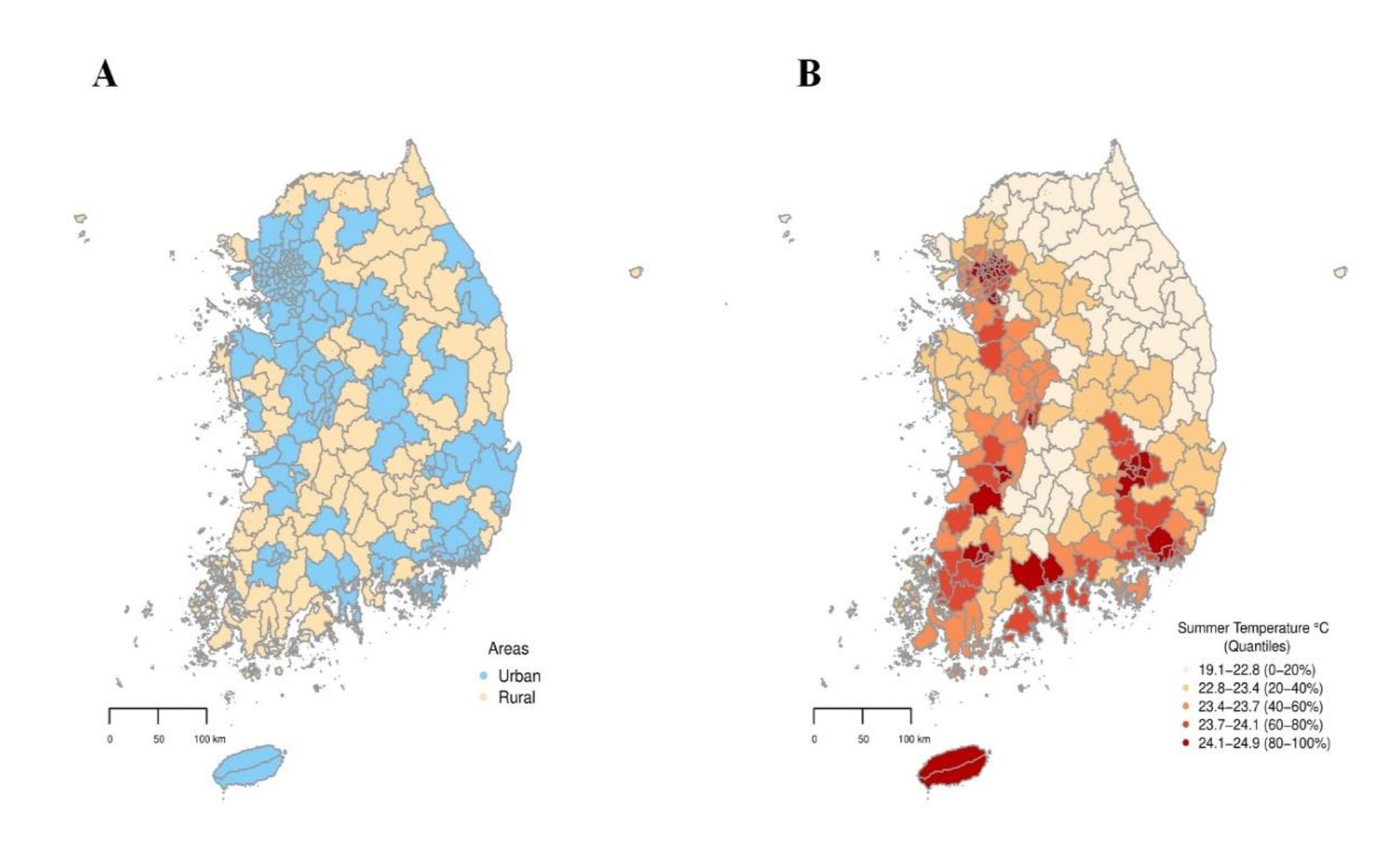
2.1. Study Area
2.2. Data Collection
2.3. Definition of Heatwave
2.4. Urban–Rural Classification
2.5. Statistical Analysis
2.5.1. Two-Stage Time-Series Analyses
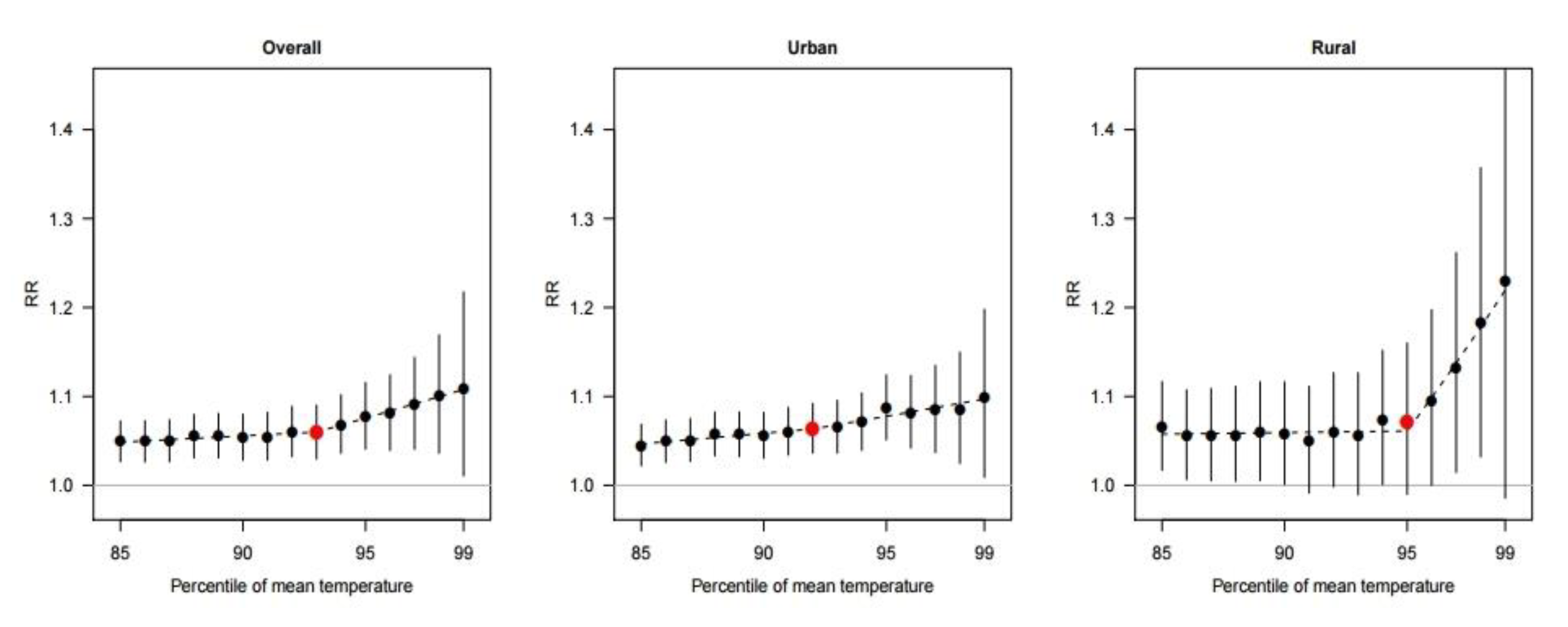
2.5.2. Identifying the Threshold Point of Heatwave
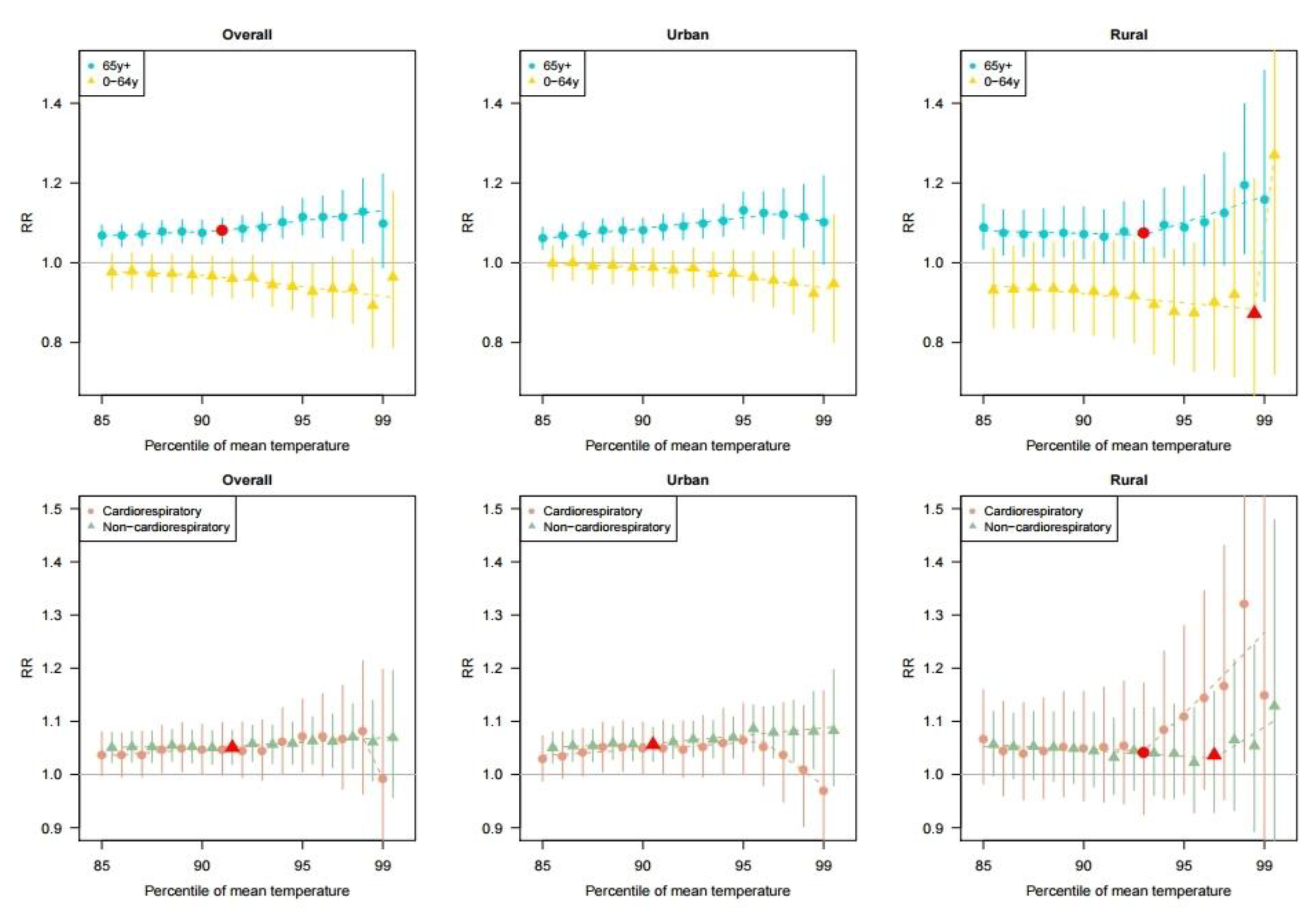
2.5.3. Subgroup Analysis
2.5.4. Sensitivity Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Anderson, G.B.; Bell, M.L. Heat waves in the United States: Mortality risk during heat waves and effect modification by heat wave characteristics in 43 US communities. Environ. Health Perspect. 2011, 119, 210–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baccini, M.; Kosatsky, T.; Analitis, A.; Anderson, H.R.; D’Ovidio, M.; Menne, B.; Michelozzi, P.; Biggeri, A.; Group, P.C. Impact of heat on mortality in 15 European cities: Attributable deaths under different weather scenarios. J. Epidemiol. Comm. Health 2011, 65, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Basu, R. High ambient temperature and mortality: A review of epidemiologic studies from 2001 to 2008. Environ. Health 2009, 8, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Y.; Barnett, A.G.; Tong, S. High temperatures-related elderly mortality varied greatly from year to year: Important information for heat-warning systems. Sci. Rep. 2012, 2, 830. [Google Scholar] [CrossRef] [Green Version]
- Hajat, S.; Kosatky, T. Heat-related mortality: A review and exploration of heterogeneity. J. Epidemiol. Comm. Health 2010, 64, 753–760. [Google Scholar] [CrossRef]
- Son, J.-Y.; Lee, J.-T.; Anderson, G.B.; Bell, M.L. The impact of heat waves on mortality in seven major cities in Korea. Environ. Health Perspect. 2012, 120, 566–571. [Google Scholar] [CrossRef] [Green Version]
- Tong, S.; Ren, C.; Becker, N. Excess deaths during the 2004 heatwave in Brisbane, Australia. Int. J. Biometeorol. 2010, 54, 393–400. [Google Scholar] [CrossRef]
- Xu, Z.; Hu, W.; Su, H.; Turner, L.R.; Ye, X.; Wang, J.; Tong, S. Extreme temperatures and paediatric emergency department admissions. J Epidemiol. Comm. Health 2014, 68, 304–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, C.B. Climate Change 2014—Impacts, Adaptation and Vulnerability: Regional Aspects; Cambridge University Press: Cambridge, UK, 2014. [Google Scholar]
- Gasparrini, A.; Guo, Y.; Sera, F.; Vicedo-Cabrera, A.M.; Huber, V.; Tong, S.; Coelho, M.; Saldiva, P.H.N.; Lavigne, E.; Correa, P.M.; et al. Projections of temperature-related excess mortality under climate change scenarios. Lancet Planet. Health 2017, 1, e360–e367. [Google Scholar] [CrossRef]
- Meehl, G.A.; Tebaldi, C. More intense, more frequent, and longer lasting heat waves in the 21st century. Science 2004, 305, 994–997. [Google Scholar] [CrossRef] [Green Version]
- Gabriel, K.M.; Endlicher, W.R. Urban and rural mortality rates during heat waves in Berlin and Brandenburg, Germany. Environ. Pollut. 2011, 159, 2044–2050. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Zheng, Y.; Tang, X.; Guo, C.; Li, L.; Song, G.; Zhen, X.; Yuan, D.; Kalkstein, A.J.; Li, F. The urban heat island and its impact on heat waves and human health in Shanghai. Int. J. Biometeorol. 2010, 54, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Zhou, L.; Chen, X.; Ma, Z.; Liu, Y.; Huang, L.; Bi, J.; Kinney, P.L. Urbanization level and vulnerability to heat-related mortality in Jiangsu Province, China. Environ. Health Perspect. 2016, 124, 1863–1869. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.; Guo, Y.; Hochrainer-Stigler, S.; Liu, W.; See, L.; Yang, X.; Zhong, J.; Fei, F.; Chen, F.; Zhang, Y. Evidence for urban–rural disparity in temperature–mortality relationships in Zhejiang Province, China. Environ. Health Perspect. 2019, 127, 037001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashizume, M.; Wagatsuma, Y.; Hayashi, T.; Saha, S.K.; Streatfield, K.; Yunus, M. The effect of temperature on mortality in rural Bangladesh—A population-based time-series study. Int. J. Epidemiol. 2009, 38, 1689–1697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, J.E.; Blangiardo, M.; Fecht, D.; Elliott, P.; Ezzati, M. Vulnerability to the mortality effects of warm temperature in the districts of England and Wales. Nat. Clim. Change 2014, 4, 269–273. [Google Scholar] [CrossRef]
- Anderson, B.G.; Bell, M.L. Weather-related mortality: How heat, cold, and heat waves affect mortality in the United States. Epidemiology 2009, 20, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.; Choi, H.M.; Kim, D.; Honda, Y.; Guo, Y.-L.L.; Kim, H. Temporal changes in mortality attributed to heat extremes for 57 cities in Northeast Asia. Sci. Total Environ. 2018, 616, 703–709. [Google Scholar] [CrossRef]
- Robinson, P.J. On the definition of a heat wave. J. App. Meteorol. 2001, 40, 762–775. [Google Scholar] [CrossRef]
- Tong, S.; Wang, X.Y.; FitzGerald, G.; McRae, D.; Neville, G.; Tippett, V.; Aitken, P.; Verrall, K. Development of health risk-based metrics for defining a heatwave: A time series study in Brisbane, Australia. BMC Pub. Health 2014, 14, 435. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Gasparrini, A.; Armstrong, B.G.; Tawatsupa, B.; Tobias, A.; Lavigne, E.; Coelho, M.; Pan, X.; Kim, H.; Hashizume, M. Heat wave and mortality: A multicountry, multicommunity study. Environ. Health Perspect. 2017, 125, 087006. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Interior and Safety. Local Autonomy Acts; Ministry of Interior and Safety Korea: Seoul, Korea, 2017. [Google Scholar]
- Guo, Y.; Gasparrini, A.; Li, S.; Sera, F.; Vicedo-Cabrera, A.M.; Coelho, M.; Saldiva, P.H.N.; Lavigne, E.; Tawatsupa, B.; Punnasiri, K.; et al. Quantifying excess deaths related to heatwaves under climate change scenarios: A multicountry time series modelling study. PLoS Med. 2018, 15, e1002629. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Choi, H.M.; Lee, J.Y.; Kim, D.H.; Honda, Y.; Kim, H. Temporal changes in mortality impacts of heat wave and cold spell in Korea and Japan. Environ. Int. 2018, 116, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Ha, J.-S.; Park, J. High temperature, heat index, and mortality in 6 major cities in South Korea. Arch. Environ. Occup. Health 2006, 61, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.; FitzGerald, G.; Wang, X.-Y.; Aitken, P.; Tippett, V.; Chen, D.; Wang, X.; Guo, Y. Exploration of the health risk-based definition for heatwave: A multi-city study. Environ. Res. 2015, 142, 696–702. [Google Scholar] [CrossRef]
- Burkart, K.; Schneider, A.; Breitner, S.; Khan, M.H.; Krämer, A.; Endlicher, W. The effect of atmospheric thermal conditions and urban thermal pollution on all-cause and cardiovascular mortality in Bangladesh. Environ. Pollut. 2011, 159, 2035–2043. [Google Scholar] [CrossRef] [Green Version]
- Rizwan, A.M.; Dennis, L.Y.; Chunho, L. A review on the generation, determination and mitigation of Urban Heat Island. J. Environ. Sci. 2008, 20, 120–128. [Google Scholar] [CrossRef]
- Hajat, S.; Kovats, R.S.; Lachowycz, K. Heat-related and cold-related deaths in England and Wales: Who is at risk? Occup. Environ. Med. 2007, 64, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Kovats, R.S.; Hajat, S. Heat stress and public health: A critical review. Annu. Rev. Public Health 2008, 29, 41–55. [Google Scholar] [CrossRef]
- Zeng, W.; Lao, X.; Rutherford, S.; Xu, Y.; Xu, X.; Lin, H.; Liu, T.; Luo, Y.; Xiao, J.; Hu, M. The effect of heat waves on mortality and effect modifiers in four communities of Guangdong Province, China. Sci. Total Environ. 2014, 482, 214–221. [Google Scholar] [CrossRef]
- Korean Statistical Information Service (KOSIS). Agriculture, Forestry and Fishery Survey; Korean Statistical Information Service (KOSIS): Seoul, Korea, 2018. [Google Scholar]
- Braunwald, E. Cardiovascular medicine at the turn of the millennium: Triumphs, concerns, and opportunities. N. Eng. J. Med. 1997, 337, 1360–1369. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Kinney, P.L.; Petkova, E.P.; Lavigne, E.; Zanobetti, A.; Schwartz, J.D.; Tobias, A.; Leone, M. Temporal variation in heat–mortality associations: A multicountry study. Environ. Health Perspect. 2015, 123, 1200–1207. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, B.; Sera, F.; Vicedo-Cabrera, A.M.; Abrutzky, R.; Åström, D.O.; Bell, M.L.; Chen, B.-Y.; de Sousa Zanotti Stagliorio Coelho, M.; Correa, P.M.; Dang, T.N. The role of humidity in associations of high temperature with mortality: A multicountry, multicity study. Environ. Health Perspect. 2019, 127, 097007. [Google Scholar] [CrossRef] [PubMed]
- Hajat, S.; Gasparrini, A. The excess winter deaths measure: Why its use is misleading for public health understanding of cold-related health impacts. Epidemiology 2016, 27, 486. [Google Scholar] [CrossRef] [Green Version]
- Buckley, J.P.; Samet, J.M.; Richardson, D.B. Commentary: Does air pollution confound studies of temperature? Epidemiology 2014, 25, 242–245. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Mean (Range) | |||
|---|---|---|---|
| Total (229 Districts) | Urban (147 Districts) | Rural (82 Districts) | |
| Mean temperature (°C) | 23.3 (19.1, 24.9) | 23.7 (19.1, 24.9) | 22.7 (20.0, 24.3) |
| Population (2011–2016) | 223793.6 (10392.8, 1151632.8) | 318843.4 (41727.5, 1151632.8) | 53399.4 (10392.8, 212373.7) |
| Deaths | |||
| Total | 2579.2 (148, 10929) | 3359.9 (344, 10929) | 1179.6 (148, 2561) |
| Aged 65 y+ | 1867.2 (107, 7493) | 2379.6 (250, 7493) | 948.6 (107, 2013) |
| Aged 0–64 y | 711.6 (41, 3436) | 979.9 (94, 3436) | 230.7 (41, 745) |
| Cardiorespiratory | 758.4 (31, 3432) | 970.1 (91, 3432) | 378.9 (31, 813) |
| Non-cardiorespiratory | 1820.8 (117, 7497) | 2389.8 (253, 7497) | 800.7 (117, 1748) |
| Deaths per 100,000 persons | |||
| Total | 1625.2 (612.9, 3370.1) | 1213.6 (612.9, 2458.0) | 2363.0 (1177.5, 3370.1) |
| Aged 65 y+ | 1251.2 (433.9, 2871.0) | 878.9 (433.9, 2043.3) | 1918.6 (837.9, 2871.0) |
| Aged 0–64 y | 373.7 (176.9, 537.2) | 334.5 (176.9, 517.7) | 443.9 (278.9, 537.2) |
| Cardiorespiratory | 504.1 (171.4, 1273.3) | 361.7 (171.4, 834.0) | 759.3 (298.3, 1273.3) |
| Non-cardiorespiratory | 1121.1 (435.8, 2413.1) | 851.9 (435.8, 1687.6) | 1603.7 (817.5, 2413.1) |
| Total (229 Districts) | Urban (147 Districts) | Rural (82 Districts) | |
|---|---|---|---|
| Threshold point (% of temperature) | 93% | 92% | 95% |
| Maximum heat-RR (95% CI) | 1.11 (1.01, 1.22) | 1.10 (1.01, 1.20) | 1.23 (0.99, 1.53) |
| Cut-off point with the maximum RR (%) | 99% | 99% | 99% |
| Total | Urban | Rural | ||
|---|---|---|---|---|
| (229 Districts) | (147 Districts) | (82 Districts) | ||
| Aged 65 y+ | Threshold point (% of temperature) | 91% | - 1 | 93% |
| Maximum heat-RR (95% CI) | 1.13 (1.05, 1.21) | 1.13 (1.08, 1.18) | 1.20 (1.02, 1.40) | |
| Cut-off point with the maximum RR (%) | 98% | 95% | 98% | |
| Aged 0–64 y | Threshold point (% of temperature) | - 1 | - 1 | 98% |
| Maximum heat-RR (95% CI) | 0.98 (0.93, 1.03) | 1.00 (0.96, 1.04) | 1.27 (0.72, 2.24) | |
| Cut-off point with the maximum RR (%) | 86% | 86% | 99% | |
| Cardiorespiratory | Threshold point (% of temperature) | - 1 | - 1 | 93% |
| Maximum heat-RR (95% CI) | 1.08 (0.96, 1.21) | 1.06 (1.00, 1.13) | 1.32 (1.02, 1.71) | |
| Cut-off point with the maximum RR (%) | 98% | 95% | 98% | |
| Non-cardiorespiratory | Threshold point (% of temperature) | 91% | 90% | 96% |
| Maximum heat-RR (95% CI) | 1.07 (1.01, 1.13) | 1.09 (1.04, 1.13) | 1.13 (0.86, 1.48) | |
| Cut-off point with the maximum RR (%) | 97% | 95% | 99% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, C.; Park, C.; Lee, W.; Pehlivan, N.; Choi, M.; Jang, J.; Kim, H. Heatwave-Related Mortality Risk and the Risk-Based Definition of Heat Wave in South Korea: A Nationwide Time-Series Study for 2011–2017. Int. J. Environ. Res. Public Health 2020, 17, 5720. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165720
Kang C, Park C, Lee W, Pehlivan N, Choi M, Jang J, Kim H. Heatwave-Related Mortality Risk and the Risk-Based Definition of Heat Wave in South Korea: A Nationwide Time-Series Study for 2011–2017. International Journal of Environmental Research and Public Health. 2020; 17(16):5720. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165720
Chicago/Turabian StyleKang, Cinoo, Chaerin Park, Whanhee Lee, Nazife Pehlivan, Munjeong Choi, Jeongju Jang, and Ho Kim. 2020. "Heatwave-Related Mortality Risk and the Risk-Based Definition of Heat Wave in South Korea: A Nationwide Time-Series Study for 2011–2017" International Journal of Environmental Research and Public Health 17, no. 16: 5720. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165720