Spatial and Temporal Impacts of Socioeconomic and Environmental Factors on Healthcare Resources: A County-Level Bayesian Local Spatiotemporal Regression Modeling Study of Hospital Beds in Southwest China

 and
and
Abstract
:1. Introduction
2. Materials and Methods
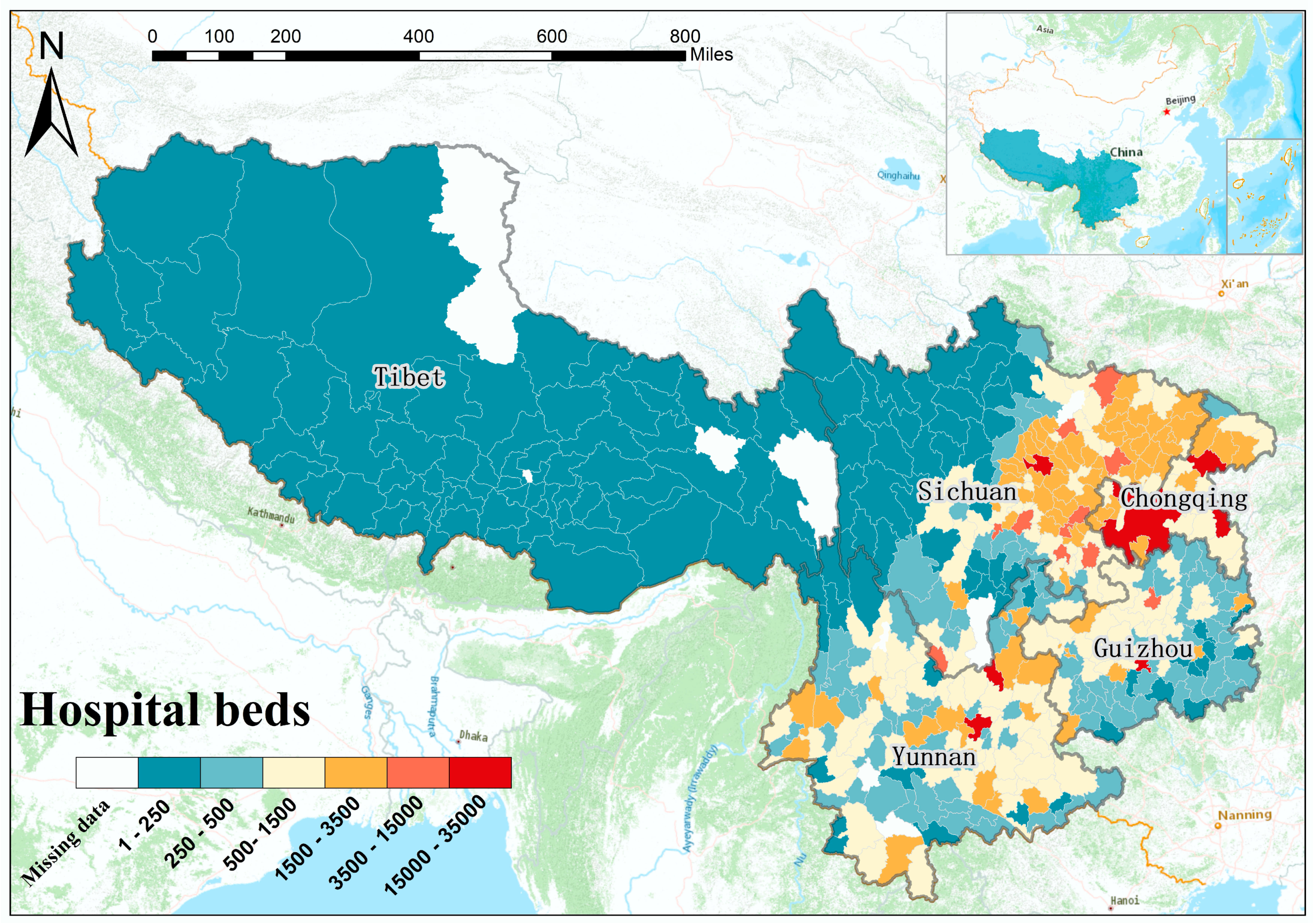
2.1. Study Area and Data
2.2. Covariates Screening Methods
2.3. Local Spatiotemporal Regression
2.3.1. Bayesian STVC Model
2.3.2. Models Implementation
2.3.3. Bayesian Inference and Model Evaluation
3. Results
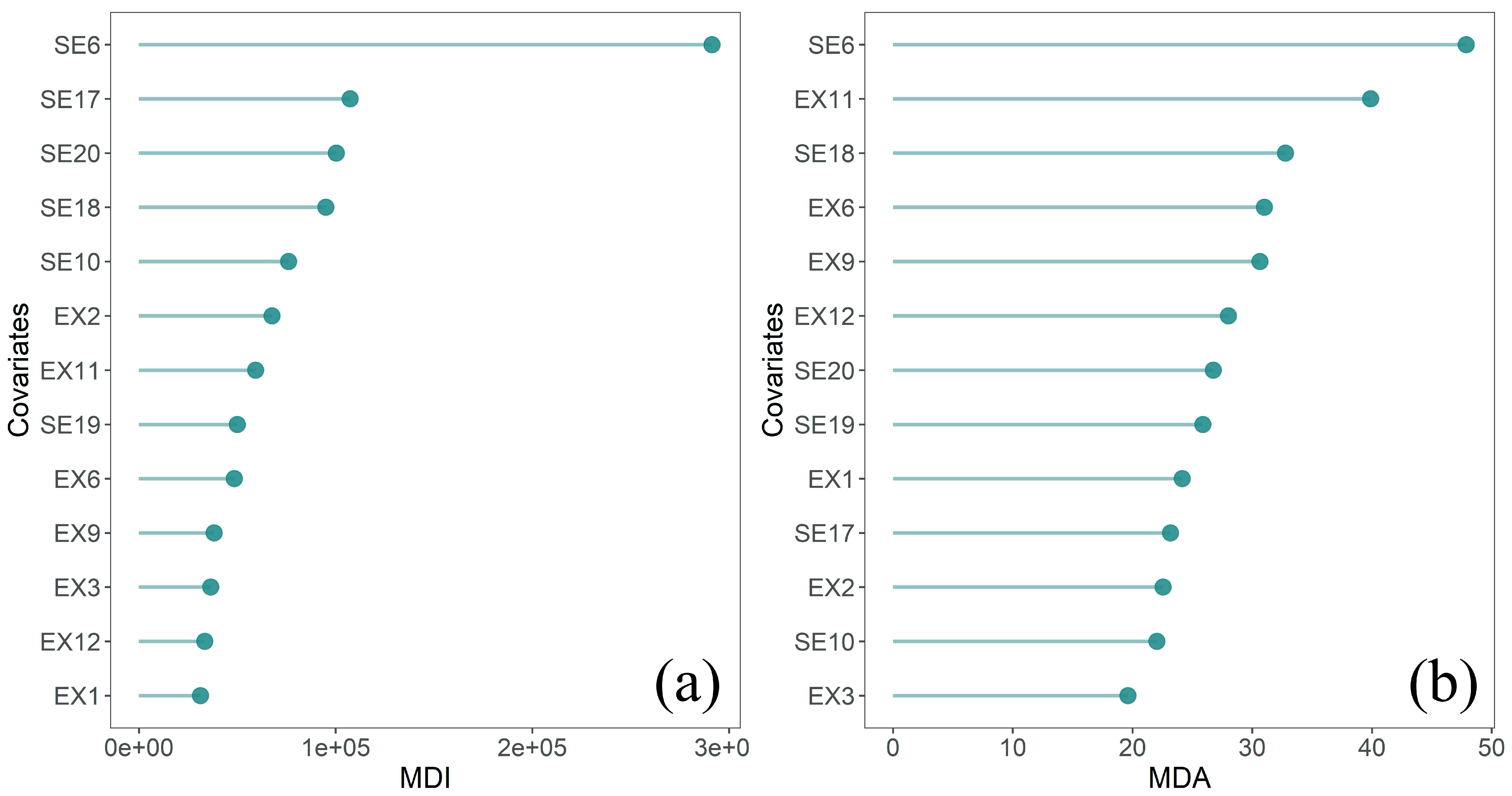
3.1. Covariates Selection
3.2. Model Evaluation and Comparison
3.3. Covariates’ Global Scale Impacts on Healthcare Resources
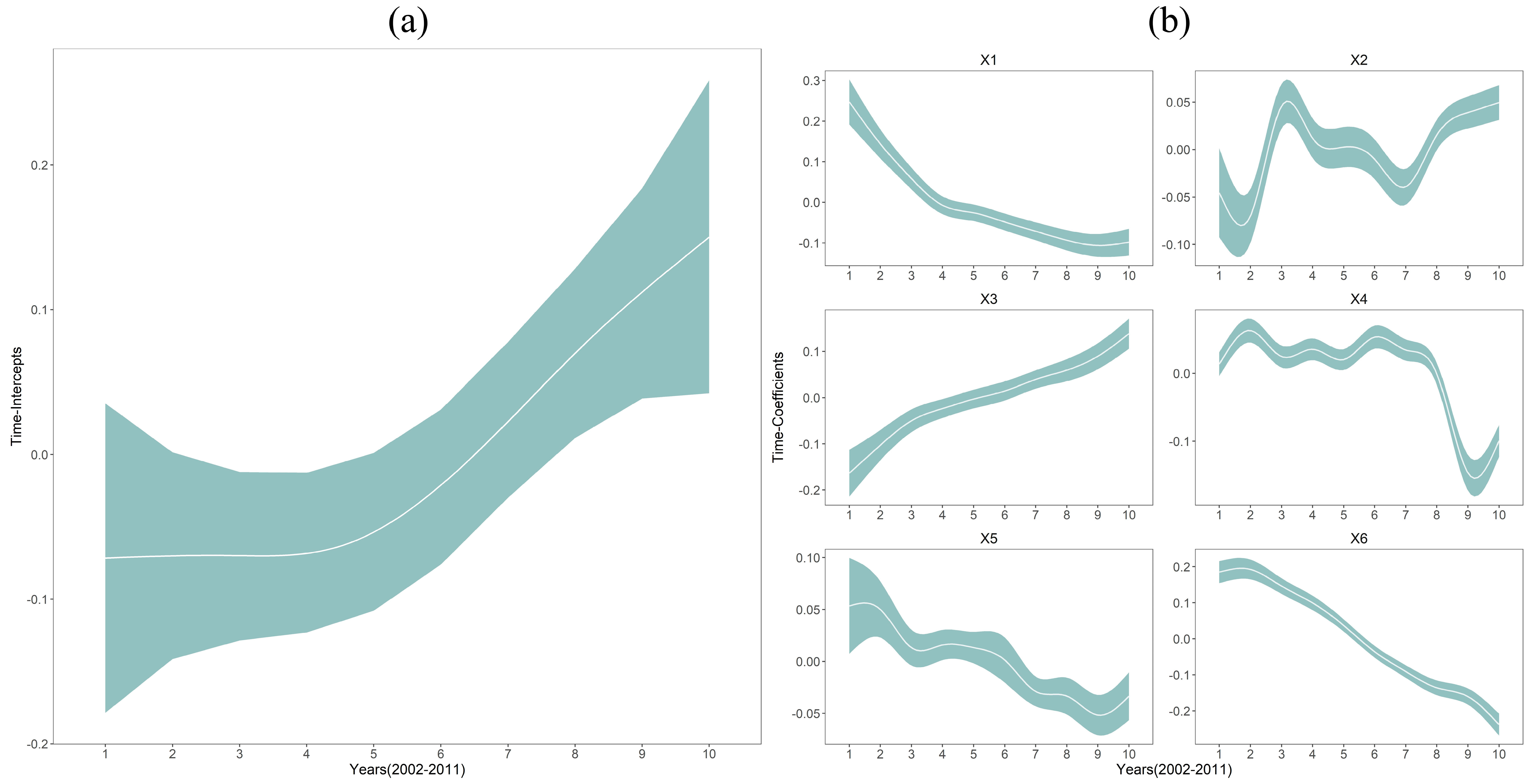
3.4. Covariates’ Temporal Heterogeneous Impacts on Healthcare Resources
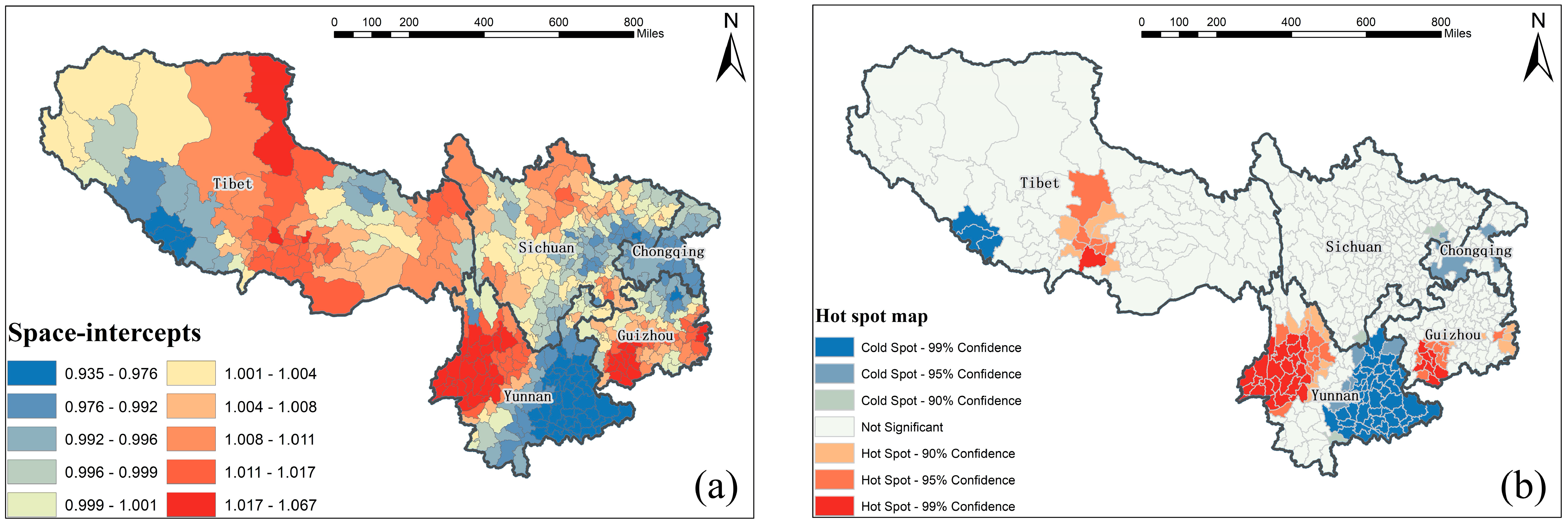
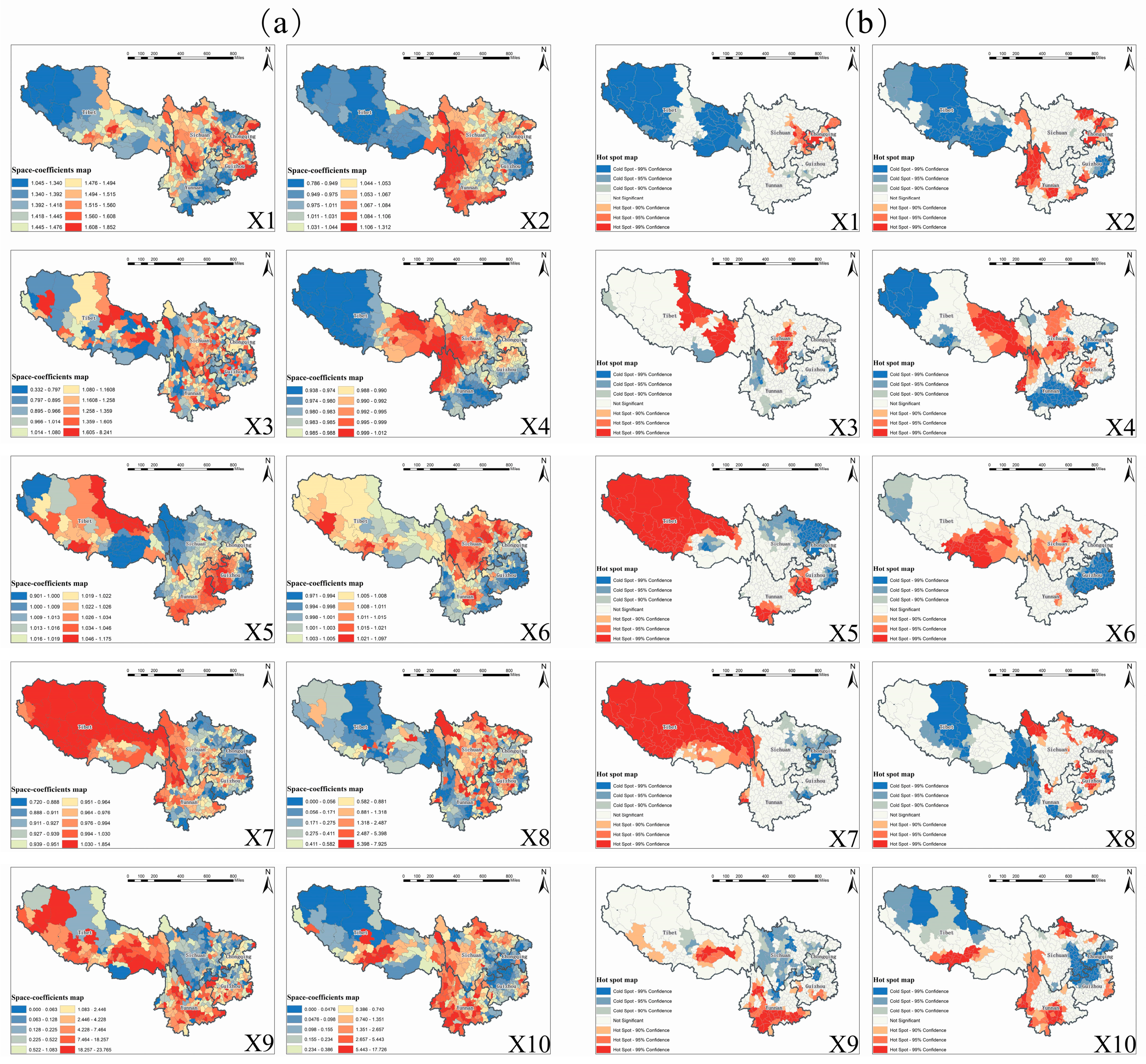
3.5. Covariates’ Spatial Heterogeneous Impacts on Healthcare Resources
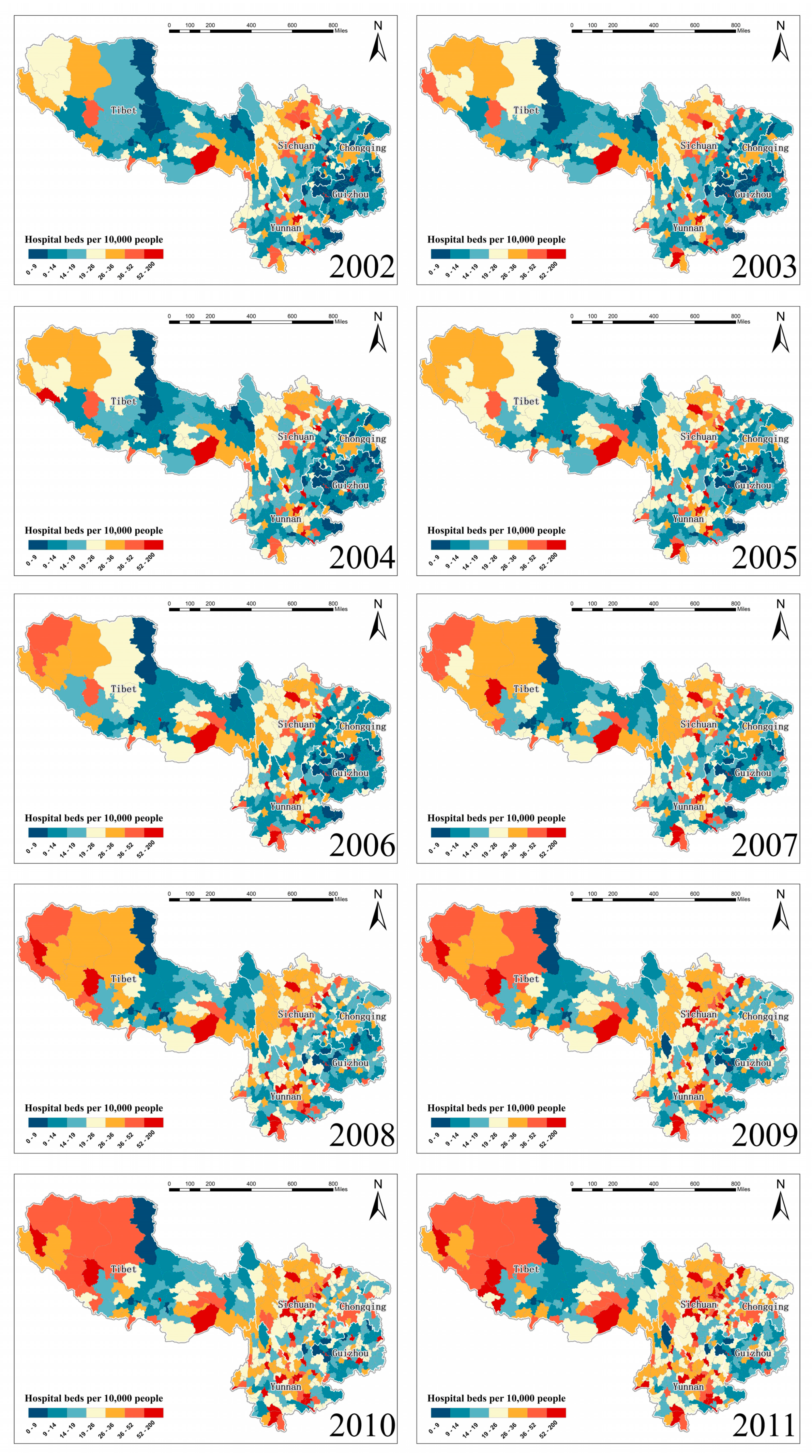
3.6. Estimated Spatiotemporal Maps of Healthcare Resources Equalities
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Minimum | Maximum | Mean | Std. Deviation | Skewness | Kurtosis |
|---|---|---|---|---|---|---|
| Y | 1.20 | 135.60 | 22.87 | 15.09 | 2.08 | 6.00 |
| SE1 | 0.00001 | 0.2513 | 0.0228 | 0.0267 | 2.33 | 9.33 |
| SE2 | 0.0002 | 684.30 | 14.69 | 36.40 | 7.85 | 90.56 |
| SE3 | 0.0001 | 1527.90 | 33.40 | 82.65 | 9.88 | 141.10 |
| SE4 | 4.99 | 6,329,247 | 32,533 | 194,713 | 19.74 | 486.90 |
| SE5 | 5.67 | 10,310,602 | 89,787 | 302,255 | 18.75 | 464.19 |
| SE6 | 0.75 | 201,423 | 5514 | 8153 | 8.35 | 131.73 |
| SE7 | 4.00 | 122,519,466 | 502,703 | 4,014,174.76 | 20.24 | 501.36 |
| SE8 | 0.51 | 4558 | 42 | 166 | 16.96 | 363.20 |
| SE9 | 1.57 | 101,037,587 | 506,231 | 2,773,609 | 21.03 | 585.25 |
| SE10 | 0.77 | 256,720 | 5208 | 8618.07 | 8.33 | 172.10 |
| SE11 | 0.0002 | 140.52 | 12.77 | 15.47 | 2.36 | 9.04 |
| SE12 | 0.0002 | 179.10 | 19.27 | 20.76 | 2.24 | 9.23 |
| SE13 | 5.26 | 77,489,300 | 521,682 | 2,315,996 | 19.46 | 480.79 |
| SE14 | 4.53 | 442,463,903 | 362,658 | 7,002,860 | 55.50 | 3454.81 |
| SE15 | 3.13 | 4,366,522,055 | 2,906,142 | 74,407,402 | 49.34 | 2715.86 |
| SE16 | 2.75 | 2,940,718,935 | 3,408,027 | 60,985,621 | 41.88 | 1872.98 |
| SE17 | 4.72 | 617,811 | 9492 | 12,017 | 29.03 | 1426.97 |
| SE18 | 0.0001 | 653.65 | 15.64 | 34.12 | 7.95 | 98.80 |
| SE19 | 0.31 | 32,916 | 1027 | 1472 | 5.18 | 61.29 |
| SE20 | 122 | 728,600 | 4328 | 14,171 | 31.57 | 1502.91 |
| EX1 | 0.0844 | 0.87 | 0.68 | 0.16 | −1.93 | 2.85 |
| EX2 | 0.0001 | 38.03 | 1.67 | 3.11 | 4.72 | 31.53 |
| EX3 | 2093 | 21,169 | 10,234 | 2904 | 0.05 | 0.25 |
| EX4 | −46.83 | 224.05 | 130.81 | 61.98 | −1.11 | −0.10 |
| EX5 | 572.19 | 977.84 | 840.22 | 108.95 | −0.83 | −0.40 |
| EX6 | 0.76 | 2.72 | 1.53 | 0.31 | 0.86 | 1.03 |
| EX7 | 2.45 | 20.40 | 12.45 | 4.20 | −0.86 | −0.54 |
| EX8 | 71.77 | 296.55 | 147.03 | 51.68 | 0.57 | −0.64 |
| EX9 | 0.000006 | 0.000283 | 0.000068 | 0.000022 | 3.51 | 28.03 |
| EX10 | 294.57 | 5154.40 | 1997.05 | 1476.69 | 0.87 | −0.57 |
| EX11 | 0.22 | 16.51 | 6.07 | 3.44 | 0.51 | −0.26 |
| EX12 | 0.0000 | 0.000388 | 0.000064 | 0.000031 | 2.84 | 24.56 |
| Socioeconomic | VIF | Selection | Environment | VIF | Selection |
|---|---|---|---|---|---|
| SE1 | 6.67 | N | EX1 | 1.68 | Y |
| SE2 | 6.19 | N | EX2 | 1.30 | Y |
| SE3 | 7.68 | N | EX3 | 3.00 | Y |
| SE4 | 39.34 | N | EX4 | 39.06 | N |
| SE5 | 24.53 | N | EX5 | 56.51 | N |
| SE6 | 2.50 | Y | EX6 | 2.95 | Y |
| SE7 | 8.97 | N | EX7 | 47.18 | N |
| SE8 | 20.72 | N | EX8 | 7.69 | N |
| SE9 | 39.99 | N | EX9 | 1.24 | Y |
| SE10 | 1.55 | Y | EX10 | 78.75 | N |
| SE11 | 17.04 | N | EX11 | 2.50 | Y |
| SE12 | 11.16 | N | EX12 | 1.20 | Y |
| SE13 | 50.85 | N | |||
| SE14 | 18.11 | N | |||
| SE15 | 61.97 | N | |||
| SE16 | 25.15 | N | |||
| SE17 | 1.37 | Y | |||
| SE18 | 4.63 | Y | |||
| SE19 | 1.36 | Y | |||
| SE20 | 1.17 | Y |
References
- Grad, F.P. The Preamble of the Constitution of the World Health Organization. (Public Health Classics). Bull. World Health Organ. 2002, 80. [Google Scholar] [CrossRef]
- Podger, A.; Secretary; Hagan, P. Reforming the Australianhealth care system:the role of government. Occasional Papers: New Series Number. Aust. Gov. Dep. Health Ageing 1999, 1, 36. [Google Scholar]
- Penchalaiah, B.; Sobha, P. Socio-Economic Inequality and its Effect on Healthcare Delivery in India: Inequality and Healthcare. Paripex Indian J. Res. 2012, 3, 275–277. [Google Scholar] [CrossRef]
- Asl, I.M.; Abolhallaje, M.; Raadabadi, M.; Nazari, H.; Nazari, A.; Salimi, M.; Javani, A. Distribution of hospital beds in Tehran Province based on Gini coefficient and Lorenz curve from 2010 to 2012. Electron. Physician 2015, 7, 1653–1657. [Google Scholar] [PubMed] [Green Version]
- Han, J.H.; Sunderland, N.; Kendall, E.; Gudes, O.; Henniker, G. Professional practice and innovation: Chronic disease, geographic location and socioeconomic disadvantage as obstacles to equitable access to e-health. Health Inf. Manag. J. 2010, 39, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Sefiddashti, S.E.; Arab, M.; Ghazanfari, S.; Kazemi, Z.; Rezaei, S.; Karyani, A.K. Trends of geographic inequalities in the distribution of human resources in healthcare system: The case of Iran. Electron. Physician 2016, 8, 2607–2613. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wei, Y. A Spatial-Temporal Analysis of Health Care and Mortality Inequalities in China. Eurasian Geogr. Econ. 2010, 51, 767–787. [Google Scholar] [CrossRef] [Green Version]
- Song, X.; Wei, Y.; Deng, W.; Zhang, S.; Zhou, P.; Liu, Y.; Wan, J. Spatio-Temporal Distribution, Spillover Effects and Influences of China’s Two Levels of Public Healthcare Resources. Int. J. Environ. Res. Public Health 2019, 16, 582. [Google Scholar] [CrossRef] [Green Version]
- Ameryoun, A.; Meskarpouramiri, M.; Dezfulinejad, M.L.; Khoddamivishteh, H.R.; Tofighi, S. The Assessment of Inequality on Geographical Distribution of Non-Cardiac Intensive Care Beds in Iran. Iran. J. Public Health 2011, 40, 25–33. [Google Scholar]
- Zhang, T.; Xu, Y.; Ren, J.; Sun, L.; Liu, C. Inequality in the distribution of health resources and health services in China: Hospitals versus primary care institutions. Int. J. Equity Health 2017, 16, 42. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wei, Y. Multidimensional Inequalities in Health Care Distribution in Provincial China: A Case Study of Henan Province. Tijdschr. Voor Econ. En Soc. Geogr. 2014, 105, 91–106. [Google Scholar] [CrossRef]
- Zhang, X.; Zhao, L.; Cui, Z.; Wang, Y. Study on Equity and Efficiency of Health Resources and Services Based on Key Indicators in China. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, J.; Shallcross, D. Geographic distribution of hospital beds throughout China: A county-level econometric analysis. Int. J. Equity Health 2016, 15, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, Y.; Liu, J.; Bian, Y.; Wang, Y. Equity analysis of hospital beds distribution in Mainland China. Chin. J. Health Stat. 2011, 14, 394–396. (In Chinese) [Google Scholar]
- Wang, S. Prediction and Influencing Factors of Hospital Bed Resource Allocation in China in 2020. Beijing University of Chinese Medicine China, 2011. Available online: http://cdmd.cnki.com.cn/article/cdmd-10026-1011117418.htm (accessed on 13 May 2020). (In Chinese).
- Wu, W.; Xu, J.; Shi, J.; Ren, H.; Wang, Y. Study on the Spatial-temporal Distribution and Influence of the Hospital-beds in Sichuan Province with GWR Method. Bull. Surv. Mapp. 2016, 4, 49–53. (In Chinese) [Google Scholar]
- Ye, Z.; Wu, Y.; Zhou, Z.; Fang, Y. Study on the Influencing Factors of Number of Beds in Health Institutions in Mainland China Based on GWR Model. Chin. J. Health Stat. 2018, 35, 530–534. (In Chinese) [Google Scholar]
- Lu, L.; Zeng, J. Inequalities in the geographic distribution of hospital beds and doctors in traditional Chinese medicine from 2004 to 2014. Int. J. Equity Health 2018, 17, 165. [Google Scholar] [CrossRef]
- Qin, X.; Hsieh, C. Economic growth and the geographic maldistribution of health care resources: Evidence from China, 1949–2010. China Econ. Rev. 2014, 31, 228–246. [Google Scholar] [CrossRef]
- Guo, Q.; Luo, K. Concentration of Healthcare Resources in China: The Spatial–Temporal Evolution and Its Spatial Drivers. Int. J. Environ. Res. Public Health 2019, 16, 4606. [Google Scholar] [CrossRef] [Green Version]
- Ceccherininelli, A.; Priebe, S. Economic factors and psychiatric hospital beds—An analysis of historical trends. Int. J. Soc. Econ. 2007, 34, 788–810. [Google Scholar] [CrossRef]
- Song, C.; Yang, X.; Shi, X.; Bo, Y.; Wang, J. Estimating missing values in China’s official socioeconomic statistics using progressive spatiotemporal Bayesian hierarchical modeling. Sci. Rep. 2018, 8, 10055. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Liu, Y.; Twum, P.; Li, S. National equity of health resource allocation in China: Data from 2009 to 2013. Int. J. Equity Health 2016, 15, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alam, A.; Ria, I.I. Equality of geographical distribution of public hospital beds in bangladesh: A spatio-temporal analysis. Manag. Health 2019, 22, 33–38. [Google Scholar]
- Yu, H.; Chen, J.; Wang, J.; Chiu, Y.; Qiu, H.; Wang, L. Identification of the Differential Effect of City-Level on the Gini Coefficient of Health Service Delivery in Online Health Community. Int. J. Environ. Res. Public Health 2019, 16, 2314. [Google Scholar] [CrossRef] [Green Version]
- Huang, B.; Wu, B.; Barry, M. Geographically and temporally weighted regression for modeling spatio-temporal variation in house prices. Int. J. Geogr. Inf. Sci. 2010, 24, 383–401. [Google Scholar] [CrossRef]
- Fotheringham, A.S.; Crespo, R.; Yao, J. Geographical and Temporal Weighted Regression (GTWR). Geogr. Anal. 2015, 47, 431–452. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Shi, X.; Bo, Y.; Wang, J.; Wang, Y.; Huang, D. Exploring spatiotemporal nonstationary effects of climate factors on hand, foot, and mouth disease using Bayesian Spatiotemporally Varying Coefficients (STVC) model in Sichuan, China. Sci. Total Environ. 2019, 648, 550–560. [Google Scholar] [CrossRef]
- Song, C.; Shi, X.; Wang, J. Spatiotemporally Varying Coefficients (STVC) model: A Bayesian local regression to detect spatial and temporal nonstationarity in variables relationships. Ann. Gis 2020, 1–15. [Google Scholar] [CrossRef]
- Bo, Y.; Song, C.; Wang, J.; Li, X. Using an autologistic regression model to identify spatial risk factors and spatial risk patterns of hand, foot and mouth disease (HFMD) in Mainland China. BMC Public Health 2014, 14, 358. [Google Scholar] [CrossRef] [Green Version]
- Liaw, A.; Wiener, M. Classification and Regression by randomForest. R News 2002, 2, 18–22. [Google Scholar]
- Vatcheva, K.P.; Lee, M.; Mccormick, J.B.; Rahbar, M.H. Multicollinearity in Regression Analyses Conducted in Epidemiologic Studies. Epidemiology 2016, 6, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, C.; He, Y.; Bo, Y.; Wang, J.; Ren, Z.; Guo, J.; Yang, H. Disease relative risk downscaling model to localize spatial epidemiologic indicators for mapping hand, foot, and mouth disease over China. Stoch. Environ. Res. Risk Assess. 2019, 33, 1815–1833. [Google Scholar] [CrossRef]
- Strobl, C.; Boulesteix, A.; Zeileis, A.; Hothorn, T. Bias in random forest variable importance measures: Illustrations, sources and a solution. BMC Bioinform. 2007, 8, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinezbello, D.A.; Lopezquilez, A.; Prieto, A.T. Spatio-Temporal Modeling of Zika and Dengue Infections within Colombia. Int. J. Environ. Res. Public Health 2018, 15, 1376. [Google Scholar] [CrossRef] [Green Version]
- Blangiardo, M.; Cameletti, M. Spatial and Spatio-Temporal Bayesian Models with R-INLA; John Wiley & Sons: Chichester, UK, 2015. [Google Scholar]
- Lindgren, F.; Rue, H. Bayesian Spatial Modelling with R-INLA. J. Stat. Softw. 2015, 63, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Besag, J. Spatial Interaction and the Statistical Analysis of Lattice Systems. J. R. Stat. Soc. Ser. B Methodol. 1974, 36, 192–225. [Google Scholar] [CrossRef]
- Blangiardo, M.; Cameletti, M.; Baio, G.; Rue, H. Spatial and spatio-temporal models with R-INLA. Spat. Spatio Temporal Epidemiol. 2013, 4, 33–49. [Google Scholar] [CrossRef] [Green Version]
- Ugarte, M.D.; Adin, A.; Goicoa, T.; Militino, A.F. On fitting spatio-temporal disease mapping models using approximate Bayesian inference. Stat. Methods Med. Res. 2014, 23, 507–530. [Google Scholar] [CrossRef]
- Rue, H.; Martino, S.; Chopin, N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. J. R. Stat. Soc. Ser. B Stat. Methodol. 2009, 71, 319–392. [Google Scholar] [CrossRef]
- Rue, H.; Riebler, A.; Sorbye, S.H.; Illian, J.B.; Simpson, D.; Lindgren, F. Bayesian Computing with INLA: A Review. Arxiv Methodol. 2016, 4, 395–421. [Google Scholar] [CrossRef] [Green Version]
- Schrodle, B.; Held, L. Spatio—Temporal disease mapping using INLA. Environmetrics 2011, 22, 725–734. [Google Scholar] [CrossRef]
- Lazic, S.E. Bayesian Regression Modeling with INLA X.; Wang, Y.R. Yue and J. J. Faraway 2018 Boca Raton CRC Press 312 pp., £66.99 ISBN 978-1-498-72725-9. J. R. Stat. Soc. Ser. A Stat. Soc. 2019, 182, 1115. [Google Scholar] [CrossRef]
- Song, C.; He, Y.; Bo, Y.; Wang, J.; Ren, Z.; Yang, H. Risk Assessment and Mapping of Hand, Foot, and Mouth Disease at the County Level in Mainland China Using Spatiotemporal Zero-Inflated Bayesian Hierarchical Models. Int. J. Environ. Res. Public Health 2018, 15, 1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiegelhalter, D.J.; Best, N.G.; Carlin, B.P.; Der Linde, A.V. Bayesian measures of model complexity and fit. J. R. Stat. Soc. Ser. B Stat. Methodol. 2002, 64, 583–639. [Google Scholar] [CrossRef] [Green Version]
- Held, L.; Schrödle, B.; Rue, H. Posterior and cross-validatory predictive checks: A comparison of MCMC and INLA. In Statistical Modelling and Regression Structures; Physica-Verlag HD: Heidelberg, Germany, 2009; pp. 91–110. [Google Scholar]
- Whitehead, M.M. Where Do We Stand? Research and Policy Issues Concerning Inequalities in Health and in Healthcare. Acta Oncol. 1999, 38, 41–50. [Google Scholar] [CrossRef] [Green Version]
- Hotchkiss, D.R.; Godha, D.; Do, M. Expansion in the private sector provision of institutional delivery services and horizontal equity: Evidence from Nepal and Bangladesh. Health Policy Plan. 2014, 29. [Google Scholar] [CrossRef] [Green Version]
- Saito, E.; Gilmour, S.; Yoneoka, D.; Gautam, G.S.; Rahman, M.; Shrestha, P.K.; Shibuya, K. Inequality and inequity in healthcare utilization in urban Nepal: A cross-sectional observational study. Health Policy Plan. 2016, 31, 817–824. [Google Scholar] [CrossRef] [Green Version]
- Ji, X.; Li, X.; He, Y.; Liu, X. A Simple Method to Improve Estimates of County-Level Economics in China Using Nighttime Light Data and GDP Growth Rate. Isprs Int. J. Geo Inf. 2019, 8, 419. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Yang, H.; Duan, Z.; Pan, J. Spatial accessibility of primary health care in China: A case study in Sichuan Province. Soc. Sci. Med. 2018, 209, 14–24. [Google Scholar] [CrossRef]
- Wang, X.; Pan, J. Assessing the disparity in spatial access to hospital care in ethnic minority region in Sichuan Province, China. BMC Health Serv. Res. 2016, 16, 399. [Google Scholar] [CrossRef] [Green Version]
- Pan, J.; Zhao, H.; Wang, X.; Shi, X. Assessing spatial access to public and private hospitals in Sichuan, China: The influence of the private sector on the healthcare geography in China. Soc. Sci. Med. 2016, 170, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Brunsdon, C.; Fotheringham, A.S.; Charlton, M. Geographically Weighted Regression: A Method for Exploring Spatial Nonstationarity. Geogr. Anal. 2010, 28, 281–298. [Google Scholar] [CrossRef]
- Tang, J. Trends and Patterns of Spatial Distribution in Allocation of Health Care Resources among China’s Counties, 2000–2016; China School of Public Health, Sichuan University: Chengdu, Chian, 2019; Available online: http://lib.scu.edu.cn/paper (accessed on 13 May 2020). (In Chinese)
- Yip, W.; Fu, H.; Chen, A.T.; Zhai, T.; Jian, W.; Xu, R.; Pan, J.; Hu, M.; Zhou, Z.; Chen, Q. 10 years of health-care reform in China: Progress and gaps in universal health coverage. Lancet 2019, 394, 1192–1204. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, T.; Fu, B. A measure of spatial stratified heterogeneity. Ecol. Indic. 2016, 67, 250–256. [Google Scholar] [CrossRef]
- Pan, J.; Liu, G.G. The determinants of Chinese provincial government health expenditures: Evidence from 2002–2006 data. Health Econ. 2012, 21, 757–777. [Google Scholar] [CrossRef]
- Moraga, P. Geospatial Health Data: Modeling and Visualization with R-INLA and Shiny; CRC Press: Boca Raton, FL, USA, 2019. [Google Scholar]
- Mcmillen, D.P. Geographically Weighted Regression: The Analysis of Spatially Varying Relationships. Am. J. Agric. Econ. 2004, 86, 554–556. [Google Scholar] [CrossRef]
- Gelfand, A.E.; Kim, H.; Sirmans, C.F.; Banerjee, S. Spatial Modeling with Spatially Varying Coefficient Processes. J. Am. Stat. Assoc. 2003, 98, 387–396. [Google Scholar] [CrossRef]
- Shi, X.; Kwan, M.P. Introduction: Geospatial health research and GIS. Ann. GIS 2015, 21, 93–95. [Google Scholar] [CrossRef]
- Wang, F. Why public health needs GIS: A methodological overview. Ann. GIS 2020, 26, 1–12. [Google Scholar] [CrossRef] [Green Version]






| Abbreviation | Variables | Units |
|---|---|---|
| SE1 | Population density | Person/km2 |
| SE2 | Employee population density | Person/km2 |
| SE3 | Local telephone users’ density | Person/km2 |
| SE4 | Local government budgetary expenditures per capita | Yuan |
| SE5 | Local general budget revenue per capita | Yuan |
| SE6 | Residents’ saving deposits per capita | Yuan |
| SE7 | Loan balance of financial institutions per capita | Yuan |
| SE8 | Above-scale total industrial density | Number/km2 |
| SE9 | Above-scale total industrial output value per capita | Yuan |
| SE10 | Total investment in fixed assets per capita | Yuan |
| SE11 | Junior high school student density | Person/km2 |
| SE12 | Primary school student density | Person/km2 |
| SE13 | Gross domestic product (GDP) | Million |
| SE14 | First industry output per capita | Yuan |
| SE15 | Second industry output per capita | Yuan |
| SE16 | Tertiary industry output per capita | Yuan |
| SE17 | GDP per capita | Yuan |
| SE18 | Urban worker population density | Person/km2 |
| SE19 | Average wage of employees in urban units | Yuan |
| SE20 | Total retail sales of consumer goods per capita | Yuan |
| EX1 | Normalized vegetation index (NDVI) | / |
| EX2 | Nighttime light index | / |
| EX3 | Precipitation | 0.1 mm |
| EX4 | Temperature | 0.1 centigrade |
| EX5 | Air pressure | 1 N/m2 |
| EX6 | Wind speed | m/s |
| EX7 | Vapor pressure | hPa |
| EX8 | Sunshine hours | hours |
| EX9 | River network density | km/km2 |
| EX10 | Elevation | Meter |
| EX11 | Slope | ° |
| EX12 | Road network density | km/km2 |
| Index | DIC | WAIC | PDIC | PWAIC | LS | R2 |
|---|---|---|---|---|---|---|
| Model 1 | 6028.53 | 6119.66 | 12.16 | 84.16 | 0.68 | 0.75 |
| Model 2 | 1928.71 | 1998.96 | 475.17 | 486.15 | 0.20 | 0.89 |
| Model 3 | 7917.86 | 7934.69 | 44.59 | 56.22 | 0.88 | 0.51 |
| Model 4 | 2036.76 | 2010.19 | 1144.72 | 931.87 | 0.22 | 0.86 |
| Model 5 | 1778.38 | 1749.55 | 1165.08 | 944.15 | 0.19 | 0.92 |
| Covariate | Name | Coefficient | SD | 2.5% CI | 97.5% CI |
|---|---|---|---|---|---|
| X1 | Residents’ saving deposits per capita | 0.2159 | 0.0115 | 0.1932 | 0.2385 |
| X2 | Total investment in fixed assets per capita | 0.0387 | 0.0088 | 0.0213 | 0.056 |
| X3 | GDP per capita | 0.0499 | 0.0081 | 0.0338 | 0.0659 |
| X4 | Urban worker population density | 0.0187 | 0.0099 | −0.0009 | 0.0382 |
| X5 | Total retail sales of consumer goods per capita | 0.0179 | 0.0113 | −0.0043 | 0.0401 |
| X6 | Nighttime light index | 0.0686 | 0.0132 | 0.0425 | 0.0946 |
| X7 | Wind speed | 0.0778 | 0.0074 | 0.0632 | 0.0923 |
| X8 | River network density | 0.0337 | 0.0088 | 0.0163 | 0.0509 |
| X9 | Slope | 0.0954 | 0.0082 | 0.0793 | 0.1115 |
| X10 | Road network density | 0.0235 | 0.0084 | 0.0069 | 0.0401 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, C.; Wang, Y.; Yang, X.; Yang, Y.; Tang, Z.; Wang, X.; Pan, J. Spatial and Temporal Impacts of Socioeconomic and Environmental Factors on Healthcare Resources: A County-Level Bayesian Local Spatiotemporal Regression Modeling Study of Hospital Beds in Southwest China. Int. J. Environ. Res. Public Health 2020, 17, 5890. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165890
Song C, Wang Y, Yang X, Yang Y, Tang Z, Wang X, Pan J. Spatial and Temporal Impacts of Socioeconomic and Environmental Factors on Healthcare Resources: A County-Level Bayesian Local Spatiotemporal Regression Modeling Study of Hospital Beds in Southwest China. International Journal of Environmental Research and Public Health. 2020; 17(16):5890. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165890
Chicago/Turabian StyleSong, Chao, Yaode Wang, Xiu Yang, Yili Yang, Zhangying Tang, Xiuli Wang, and Jay Pan. 2020. "Spatial and Temporal Impacts of Socioeconomic and Environmental Factors on Healthcare Resources: A County-Level Bayesian Local Spatiotemporal Regression Modeling Study of Hospital Beds in Southwest China" International Journal of Environmental Research and Public Health 17, no. 16: 5890. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165890