High-Flow Oxygen through Nasal Cannula vs. Non-Invasive Ventilation in Hypercapnic Respiratory Failure: A Randomized Clinical Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Study Design
2.2. HFNC and NIV Application
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dysart, K.; Miller, T.L.; Wolfson, M.R.; Shaffer, T.H. Research in highflow therapy: Mechanisms of action. Respir. Med. 2009, 103, 1400–1405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kallstrom, T.J. American Association for Respiratory Care (AARC) AARC Clinical Practice Guideline: Oxygen therapy for adults in the acute care facility—2002 Revision & update. Respir. Care 2002, 47, 717–720. [Google Scholar] [PubMed]
- Bazuaye, E.A.; Stone, T.N.; Corris, P.A.; Gibson, G.J. Variability of inspired oxygen concentration with nasal cannulas. Thorax 1992, 47, 609–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, A.G.; Johnson, A.; Sandstedt, S. Rebreathing during oxygen treatment with face mask: The effect of oxygen flow rates on ventilation. Acta Anaesthesiol. Scand. 1991, 35, 289–292. [Google Scholar] [CrossRef]
- Spoletini, G.; Alotaibi, M.; Blasi, F.; Hill, N.S. Heated Humidified High-Flow Nasal Oxygen in Adults Mechanisms of Action and Clinical Implications. CHEST 2015, 148, 253–261. [Google Scholar] [CrossRef]
- Manley, B.J.; Dold, S.K.; Davis, P.G.; Roehr, C.C. High-flow nasal cannulae for respiratory support of preterm infants: A review of the evidence. Neonatology 2012, 102, 300–308. [Google Scholar] [CrossRef] [Green Version]
- Frat, J.P.; Thille, A.W.; Mercat, A.; Girault, C.; Ragot, S.; Pharm, D.; Prat, G.; Boulain, T.; Morawiec, E.; Cottereau, A.; et al. High-Flow Oxygen through Nasal Cannula in Acute Hypoxemic Respiratory Failure. N. Engl. J. Med. 2015, 372, 2185–2196. [Google Scholar] [CrossRef] [Green Version]
- Frat, J.P.; Joly, F.; Thille, A.W. Noninvasive ventilation versus oxygen therapy in patients with acute respiratory failure. Curr. Opin. Anaesthesiol. 2019, 32, 150–155. [Google Scholar] [CrossRef]
- Rochwerg, B.; Brochard, L.; Elliott, M.W.; Hess, D.; Hill, N.S.; Nava, S.; Navalesi, P.; Antonelli, M.; Brozek, J.; Conti, G.; et al. Official ERS/ATS clinical practice guidelines: Noninvasive ventilation for acute respiratory failure. Eur. Respir. J. 2017, 50, 1602426. [Google Scholar] [CrossRef]
- Lee, M.K.; Choi, J.; Park, B.; Kim, B.; Lee, S.J.; Kim, S.H.; Yong, S.J.; Choi, E.H.; Lee, W.Y. High flow nasal cannulae oxygen therapy in acute-moderate hypercapnic respiratory failure. Clin. Respir. J. 2018, 12, 2046–2056. [Google Scholar] [CrossRef]
- Kim, E.S.; Lee, H.; Kim, S.J.; Park, J.; Lee, Y.J.; Park, J.S.; Yoon, H.I.; Lee, J.H.; Lee, C.T.; Cho, Y.J. Effectiveness ofhigh-flow nasal cannula oxygen therapy for acute respiratory failure with hypercapnia. J. Thorac. Dis. 2018, 10, 882–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bräunlich, J.; Köhler, M.; Wirtz, H. Nasal highflow improves ventilation in patients with COPD. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 1077–1085. [Google Scholar]
- Díaz-Lobato, S.; Folgado, M.A.; Chapa, A.; Alises, S.M. Efficacy of High-Flow Oxygen by Nasal Cannula with Active Humidification in a Patient with Acute Respiratory Failure of Neuromuscular Origin. Respir. Care 2013, 58, e164–e167. [Google Scholar] [CrossRef] [PubMed]
- Millar, J.; Lutton, S.; O’Connor, P. The use of high-flow nasal oxygen therapy in the management of hypercarbic respiratory failure. Ther. Adv. Respir. Dis. 2014, 8, 63–64. [Google Scholar] [CrossRef] [PubMed]
- Fraser, J.F.; Spooner, A.J.; Dunster, K.R.; Anstey, C.M.; Corley, A. Nasal high flow oxygen therapy in patients with COPD reduces respiratory rate and tissue carbon dioxide while increasing tidal and end-expiratory lung volumes: A randomised crossover trial. Thorax 2016, 71, 759–761. [Google Scholar] [CrossRef] [Green Version]
- Roca, O.; Riera, J.; Torres, F.; Masclans, J.R. High-flow oxygen therapy in acute respiratory failure. Respir. Care 2010, 55, 408–413. [Google Scholar]
- Wood, K.E.; Flaten, A.L.; Backes, W.J. Inspissated secretions: A lifethreatening complication of prolonged noninvasive ventilation. Respir. Care 2000, 45, 491–493. [Google Scholar]
- Richards, G.N.; Cistulli, P.A.; Ungar, R.G.; Berthon-Jones, M.; Sullivan, C.E. Mouth leak with nasal continuous positive airway pressure increases nasal airway resistance. Am. J. Respir. Crit. Care Med. 1996, 154, 182–186. [Google Scholar] [CrossRef]
- Sztrymf, B.; Messika, J.; Bertrand, F.; Hurel, D.; Leon, R.; Dreyfuss, D.; Ricard, J.D. Beneficial effects of humidified high flow nasal oxygen in critical care patients: A prospective pilot study. Intensive Care Med. 2011, 37, 1780–1786. [Google Scholar] [CrossRef]
- Ravenscraft, S.A.; Shapiro, R.S.; Nahum, A.; Burke, W.C.; Adams, A.B.; Nakos, G.; Marini, J.J. Tracheal gas insufflation: Catheter effectiveness determined by expiratory flush volume. Am. J. Respir. Crit. Care Med. 1996, 153, 1817–1824. [Google Scholar] [CrossRef]
- Groves, N.; Tobin, A. High flow nasal oxygen generates positive airway pressure in adult volunteers. Aust. Crit. Care 2007, 20, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Corley, A.; Caruana, L.R.; Barnett, A.G.; Tronstad, O.; Fraser, J.F. Oxygen delivery through high-flow nasal cannulae increase end-expiratory lung volume and reduce respiratory rate in post-cardiac surgical patients. Br. J. Anaesth. 2011, 107, 998–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riera, J.; Pérez, P.; Cortés, J.; Roca, O.; Masclans, J.R.; Rello, J. Effect of high-flow nasal cannula and body position on end-expiratory lung volume: A cohort study using electrical impedance tomography. Respir. Care 2013, 58, 589–596. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Population | Patients | p Value | ||
|---|---|---|---|---|
| Intervention Group (n = 20) | Control Group (n = 20) | |||
| Age (years, SD) | 77.0 (11.0) | 76.0 (13.4) | 78.1 (8.1) | 0.544 |
| Gender (n, %) | 0.752 | |||
| Male | 19 (47.5) | 10 (50.0) | 9 (45.0) | |
| Female | 21 (52.5) | 10 (50.0) | 11 (55.0) | |
| BMI (kg/m2, SD) | 28.4 (8.6) | 25.9 (8.0) | 30.9 (8.5) | 0.060 |
| APACHE Score (SD) | 20.5 (7.6) | 21.6 (8.9) | 19.3 (6.1) | 0.305 |
| Mortality Risk (predicted) | 25.0 (15.0) | 32.5 (33.8) | 25.0 (15.0) | 0.531 |
| COPD (n, %) | 0.327 | |||
| No | 15 (37.5) | 6 (30.0) | 9 (45.0) | |
| Yes | 25 (62.5) | 14 (70.0) | 11 (55.0) | |
| CHF (n, %) | 0.749 | |||
| No | 23 (57.5) | 12 (60.0) | 11 (55.0) | |
| Yes | 17 (42.5) | 8 (40.0) | 9 (45.0) | |
| DM (n, %) | 1.000 | |||
| No | 22 (55.0) | 11 (55.0) | 11 (55.0) | |
| Yes | 18 (45.0) | 9 (45.0) | 9 (45.0) | |
| Total | Patients | p Value | ||
|---|---|---|---|---|
| Intervention Group | Control Group | |||
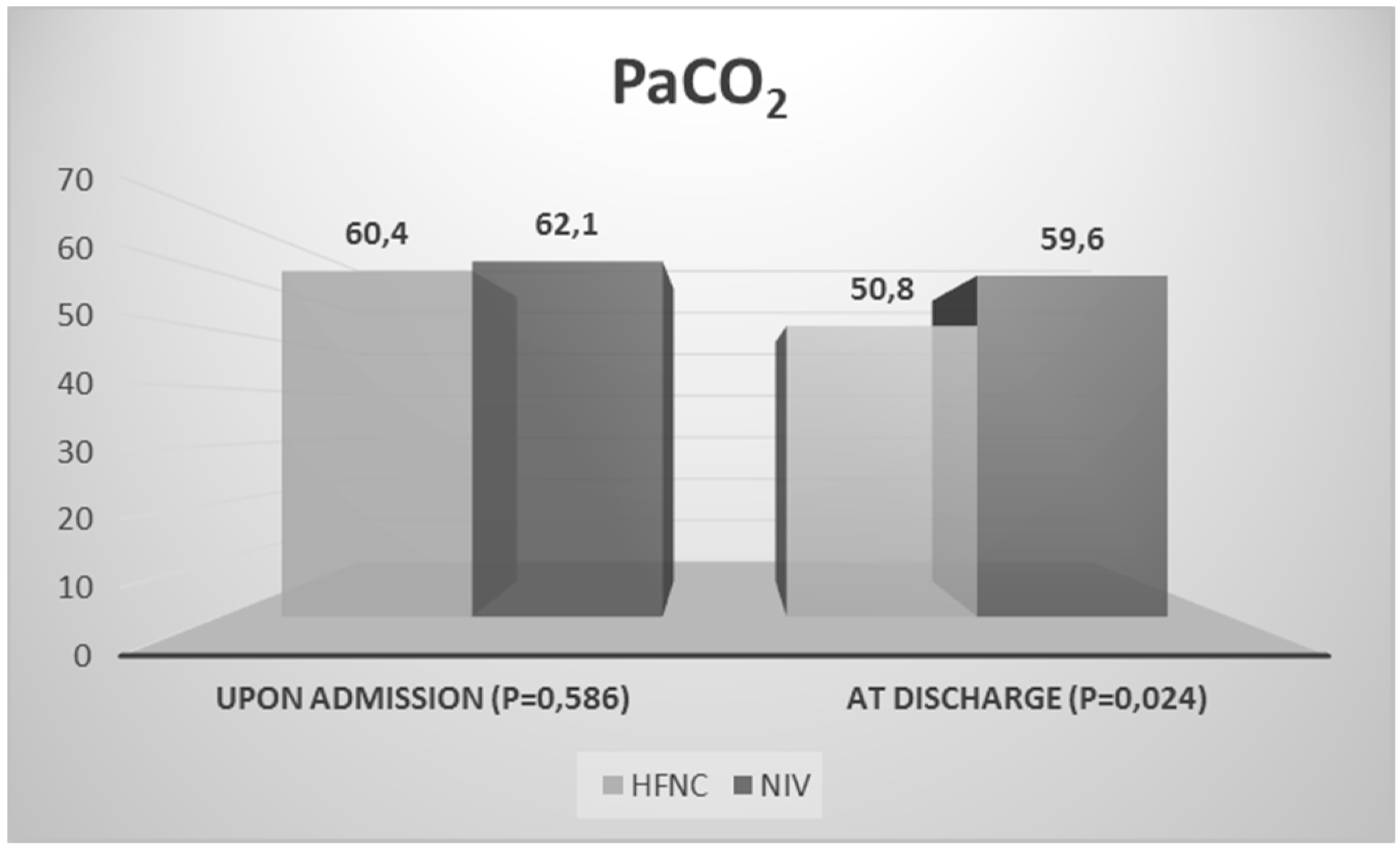
| PaCO2IN (mmHg) | 61.2 (10.0) | 60.4 (9.9) | 62.1 (10.3) | 0.586 |
| PaCO2 24 h (mmHg) | 54.2 (9.9) | 51.6 (9.6) | 56.8 (9.7) | 0.096 |
| pHIN | 7.4 (0.1) | 7.4 (0.1) | 7.4 (0.1) | 0.176 |
| pH24 h | 7.4 (0.1) | 7.4 (0.1) | 7.4 (0.1) | 0.208 |
| SaO2IN | 92.3 (4.9) | 92.4 (5.4) | 92.1 (4.6) | 0.851 |
| SaO2 24 h | 93.1 (3.0) | 93.3 (2.1) | 92.9 (3.8) | 0.644 |
| PaO2IN (mmHg) | 76.4 (28.9) | 65.2 (12.9) | 71.6 (19.8) | 0.192 |
| PaO2 24 h (mmHg) | 69.9 (9.7) | 67.9 (8.8) | 72.0 (10.4) | 0.180 |
| HCO3- IN (mmol/L) | 36.4 (7.5) | 36.7 (5.2) | 36.2 (9.4) | 0.836 |
| HCO3- 24 h (mmol/L) | 36.2 (7.8) | 35.6 (7.2) | 36.8 (8.5) | 0.648 |
| Total | Patients | p Value | ||
|---|---|---|---|---|
| Intervention Group | Control Group | |||
| Length of hospitalization (days) | 11.5 (8.5) | 11.5 (7.8) | 11.0 (10.5) | 0.655 |
| Length of 24 h uninterrupted use of HFNC or NIV (days) | 2.0 (2.0) | 2.0 (1.0) | 2.0 (9.0) | 0.078 |
| Renal Failure | 0.197 | |||
| No | 24 (60.0) | 14 (70.0) | 10 (50.0) | |
| Yes | 16 (40.0) | 6 (30.0) | 10 (50.0) | |
| Hepatic Failure | 0.698 | |||
| No | 36 (90.0) | 18 (90.0) | 18 (90.0) | |
| Yes | 4 (10.0) | 2 (10.0) | 2 (10.0) | |
| Mortality Rate (number of deaths) | 0.669 | |||
| No | 34 (85.0) | 17 (85.0) | 17 (85.0) | |
| Yes | 6 (15.0) | 3 (15.0) | 3 (15.0) | |
| Question | Scale of Available Answers | Score |
|---|---|---|
| 0–5 (0 = least comfortable, 5 = most comfortable) | 3.9 |
| 0–5 (0 = least comfortable, 5 = most comfortable) | 3.3 |
| 31–37 °C | 34.5 °C |
| 0–5 (0 = least adequate, 5 = most adequate) | 4.3 |
| 0–5 (0 = worst, 5 = best) | 3 |
| 0–5 (0 = least dyspnea, 5 = most dyspnea) | 2.8 |
| 0–5 (0 = I would not prefer it at all, 5 = I would prefer it absolutely) | 3.1 |
| 0–5 (0 = I would not replace it at all, 5 = I would replace it absolutely) | 3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papachatzakis, Y.; Nikolaidis, P.T.; Kontogiannis, S.; Trakada, G. High-Flow Oxygen through Nasal Cannula vs. Non-Invasive Ventilation in Hypercapnic Respiratory Failure: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2020, 17, 5994. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165994
Papachatzakis Y, Nikolaidis PT, Kontogiannis S, Trakada G. High-Flow Oxygen through Nasal Cannula vs. Non-Invasive Ventilation in Hypercapnic Respiratory Failure: A Randomized Clinical Trial. International Journal of Environmental Research and Public Health. 2020; 17(16):5994. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165994
Chicago/Turabian StylePapachatzakis, Yiannis, Pantelis Theodoros Nikolaidis, Sofoklis Kontogiannis, and Georgia Trakada. 2020. "High-Flow Oxygen through Nasal Cannula vs. Non-Invasive Ventilation in Hypercapnic Respiratory Failure: A Randomized Clinical Trial" International Journal of Environmental Research and Public Health 17, no. 16: 5994. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165994