Medication-Related Osteonecrosis of Jaws (MRONJ) Prevention and Diagnosis: Italian Consensus Update 2020

 ,
,  , ,
, ,  ,
,  , ,
, ,  , , , , , , and add
Show full author list
, , , , , , and add
Show full author list
Abstract
:1. Introduction
2. The Six Issues
2.1. Clinical Diagnosis of MRONJ: Practices at Risk of Inappropriateness and Good Practices
2.1.1. Questionable Practices
2.1.2. Good Practices
2.2. Radiologic Diagnosis of MRONJ: Practices at Risk of Inappropriateness and Good Practices
2.2.1. Questionable Practices
2.2.2. Good Practices
2.3. Prevention of MRONJ: Practices at Risk of Inappropriateness and Good Practices
2.3.1. Questionable Practices
2.3.2. Good Practices
2.4. Dental Management: Practices at Risk of Inappropriateness and Good Practices
2.4.1. Questionable Practices
2.4.2. Good Practices
2.5. Drug Holiday or Temporary Suspension for Patients at Risk of MRONJ: Practices at Risk of Inappropriateness and Good Practices
- -
- BPs have a long half-life and are able to accumulate in the bone tissue, potentially influencing the post-extractive bone tissue repair. Furthermore, for some largely used BPs (above all zoledronic acid), a possible antiangiogenic effect was described in the literature, potentially reducing the soft tissue repair process. Consequently, a precautionary and temporary suspension of the drug administration has been claimed by most of authors as potentially useful, even if no definitive data have been published;
- -
- Denosumab (Xgeva®), a monoclonal human anti-RANKL inhibitor, is a drug with a short half-life and does not accumulate in the bone. A possible rebound effect on the bone turnover has been described after drug withdrawal, so that some authors advised against a (long) suspension.
- -
- BPs (e.g., alendronate, ibandronate) are synthetic analogues of pyrophosphates, which firmly bind to the hydroxyapatite and reduce bone metabolism/remodeling [6]. The half-life of BPs in circulation is short (ranging from 30 min to 2 h); however, once they have been incorporated into bone tissue, they can persist more than 10 years, depending on the skeletal turnover time [11,45]. Usually, BPs (i.e., alendronate) is administered orally (e.g., 150 mg/every 4 week); in a few patients BPs are administered intramuscularly (e.g., neridronate 2 mg/kg every 3 months) or intravenously (e.g., zoledronate 5 mg/every 12 months) [6,14,45].
- -
- Denosumab (Prolia®), a monoclonal human IgG2 antibody that highly binds the receptor activator of nuclear factor-kB ligand (RANK-L), blocks the osteoclast maturation, function and survival. Its half-life is 25–32 days and it does not amass in the bone with a peculiar regimen (1 dose s.c. of 60 mg every six months) [46,47,48]. The suspension of denosumab determines within the following 3–6 months the rebound of the fracture risk, especially in patients at high risk of fracture [47,49,50]. Of note, when a patient is treated with denosumab, after a previous BP administration, he/she must be classified with the ONJ risk profile for the BP user.
2.5.1. Questionable Practices
2.5.2. Good Practices
2.6. MRONJ Therapy: Practices at Risk of Inappropriateness and Good Practices
2.6.1. Questionable Practices
2.6.2. Good Practices
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Campisi, G.; Bedogni, A.; Bertoldo, F.; Bettini, G.; Biasotto, M.; Colella, G.; Consolo, U.; di Fede, O.; Favia, G.; Fusco, V.; et al. Proceedings of the Closed Round Table and Italian Consensus on the Medication-Related Osteonecrosis of Jaws (MRONJ) at the Symposium of Italian Society of Oral Pathology and Medicine (SIPMO) Ancona, 20 October 2018—Part I. Front. Physiol. 2019, 10. [Google Scholar] [CrossRef]
- Campisi, G.; Bedogni, A.; Bertoldo, F.; Bettini, G.; Biasotto, M.; Colella, G.; Consolo, U.; di Fede, O.; Favia, G.; Fusco, V.; et al. Proceedings of the Closed Round Table and Italian Consensus on the Medication-Related Osteonecrosis of Jaws (MRONJ) at the Symposium of Italian Society of Oral Pathology and Medicine (SIPMO) Ancona, 20 October 2018—Part II. Front. Physiol. 2019, 10. [Google Scholar] [CrossRef]
- Campisi, G.; Bedogni, A.; Bertoldo, F.; Bettini, G.; Biasotto, M.; Colella, G.; Consolo, U.; di Fede, O.; Favia, G.; Fusco, V.; et al. Proceedings of the Closed Round Table and Italian Consensus on the Medication-Related Osteonecrosis of Jaws (MRONJ) at the Symposium of Italian Society of Oral Pathology and Medicine (SIPMO) Ancona, 20 October 2018—Part III. Front. Physiol. 2019, 10. [Google Scholar] [CrossRef]
- Bedogni, A.; Campisi, G.; Fusco, V. Medication Related Osteonecrosis of the Jaw (MRONJ); Qeios: London, UK, 2018. [Google Scholar] [CrossRef]
- Di Fede, O.; Panzarella, V.; Mauceri, R.; Fusco, V.; Bedogni, A.; Lo Muzio, L.; Board, S.O.; Campisi, G. The dental management of patients at risk of medication-related osteonecrosis of the jaw: New paradigm of primary prevention. Biomed. Res. Int. 2018, 2018, 1–10. [Google Scholar] [CrossRef]
- Campisi, G.; Fedele, S.; Fusco, V.; Pizzo, G.; Di Fede, O.; Bedogni, A. Epidemiology, clinical manifestations, risk reduction and treatment strategies of jaw osteonecrosis in cancer patients exposed to antiresorptive agents. Future Oncol. 2014, 10, 257–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fung, P.; Bedogni, G.; Bedogni, A.; Petrie, A.; Porter, S.; Campisi, G.; Bagan, J.; Fusco, V.; Saia, G.; Acham, S.; et al. Time to onset of bisphosphonate-related osteonecrosis of the jaws: A multicentre retrospective cohort study. Oral Dis. 2017, 477–483. [Google Scholar] [CrossRef]
- Fusco, V.; Santini, D.; Armento, G.; Tonini, G.; Campisi, G. Osteonecrosis of jaw beyond antiresorptive (bone-targeted) agents: New horizons in oncology. Expert Opin. Drug Saf. 2016, 15, 925–935. [Google Scholar] [CrossRef] [Green Version]
- Bedogni, A.; Fedele, S.; Bedogni, G.; Scoletta, M.; Favia, G.; Colella, G.; Agrillo, A.; Bettini, G.; Di Fede, O.; Oteri, G.; et al. Staging of osteonecrosis of the jaw requires computed tomography for accurate definition of the extent of bony disease. Br. J. Oral Maxillofac. Surg. 2014, 52, 603–608. [Google Scholar] [CrossRef]
- Nicolatou-Galitis, O.; Kouri, M.; Papadopoulou, E.; Vardas, E.; Galiti, D.; Epstein, J.B.; Elad, S.; Campisi, G.; Tsoukalas, N.; Bektas-Kayhan, K.; et al. Osteonecrosis of the jaw related to non-antiresorptive medications: A systematic review. Support. Care Cancer 2019, 27, 383–394. [Google Scholar] [CrossRef] [Green Version]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American association of oral and maxillofacial surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef]
- Nicolatou-Galitis, O.; Papadopoulou, E.; Vardas, E.; Kouri, M.; Galiti, D.; Galitis, E.; Alexiou, K.E.; Tsiklakis, K.; Ardavanis, A.; Razis, E.; et al. Alveolar bone histological necrosis observed prior to extractions in patients, who received bone-targeting agents. Oral Dis. 2020, 26, 955–966. [Google Scholar] [CrossRef] [PubMed]
- Schiodt, M.; Otto, S.; Fedele, S.; Bedogni, A.; Nicolatou-Galitis, O.; Guggenberger, R.; Herlofson, B.B.; Ristow, O.; Kofod, T. Workshop of European task force on medication-related osteonecrosis of the jaw—Current challenges. Oral Dis. 2019, 25, 1815–1821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campisi, G.; Bedogni, A.; Fusco, V. Raccomandazioni Clinico-Terapeutiche Sull’osteonecrosi Delle Ossa Mascellari (ONJ) Farmaco-Relata e Sua Prevenzione; Palermo University Press: Palermo, Italy, 2020. [Google Scholar] [CrossRef]
- Saad, F.; Brown, J.E.; Van Poznak, C.; Ibrahim, T.; Stemmer, S.M.; Stopeck, A.T.; Diel, I.J.; Takahashi, S.; Shore, N.; Henry, D.H.; et al. Incidence, risk factors, and outcomes of osteonecrosis of the jaw: Integrated analysis from three blinded active-controlled phase III trials in cancer patients with bone metastases. Ann. Oncol. 2012, 23, 1341–1347. [Google Scholar] [CrossRef]
- Bagan, J.; Peydró, A.; Calvo, J.; Leopoldo, M.; Jiménez, Y.; Bagan, L. Medication-related osteonecrosis of the jaw associated with bisphosphonates and denosumab in osteoporosis. Oral Dis. 2016, 22, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Troeltzsch, M.; Woodlock, T.; Kriegelstein, S.; Steiner, T.; Messlinger, K.; Troeltzsch, M. Physiology and pharmacology of nonbisphosphonate drugs implicated in osteonecrosis of the jaw. J. Can. Dent. Assoc. 2012, 78, c85. [Google Scholar]
- Hamadeh, I.S.; Ngwa, B.A.; Gong, Y. Drug induced osteonecrosis of the jaw. Cancer Treat. Rev. 2015, 41, 455–464. [Google Scholar] [CrossRef]
- Campisi, G.; Mauceri, R.; Bertoldo, F.; Fusco, V.; Bedogni, A.; Campisi, G.; Mauceri, R.; Bertoldo, F.; Fusco Vittorio, B.A. Simplifying the Dental/Periodontal Management of Patients with Metabolic Bone Fragility Receiving Treatment with Denosumab; Qeios: London, UK, 2020. [Google Scholar] [CrossRef]
- Campisi, G. Global Change and the Dentistry. A Wish from Italy and DoctOral App for the New Open Dental Journal “POJ Dental and Oral Care”. POJ Dent. Oral Care 2017, 1, 1–2. [Google Scholar] [CrossRef]
- The Council of the European Eunion. Directives—Council Directive 2013/59/Euratom. Off. J. Eur. Union 2014, L 13/1, 1–73. [Google Scholar]
- Fedele, S.; Bedogni, G.; Scoletta, M.; Favia, G.; Colella, G.; Agrillo, A.; Bettini, G.; Di Fede, O.; Oteri, G.; Fusco, V.; et al. Up to a quarter of patients with osteonecrosis of the jaw associated with antiresorptive agents remain undiagnosed. Br. J. Oral Maxillofac. Surg. 2015, 53, 13–17. [Google Scholar] [CrossRef]
- Chiandussi, S.; Biasotto, M.; Dore, F.; Cavalli, F.; Cova, M.A.; Di Lenarda, R. Clinical and diagnostic imaging of bisphosphonate-associated osteonecrosis of the jaws. Dentomaxillofac. Radiol. 2006, 35, 236–243. [Google Scholar] [CrossRef]
- Mallya, S.M.; Tetradis, S. Imaging of Radiation- and Medication-Related Osteonecrosis. Radiol. Clin. N. Am. 2018, 56, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, G.; Kalyoussef, E.; Blitz-Goldstein, M.; Guerrero, J.; Ghesani, N.; Quek, S.Y.P. Identifying MRONJ-affected bone with digital fusion of functional imaging (FI) and cone-beam computed tomography (CBCT): Case reports and hypothesis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, e106–e116. [Google Scholar] [CrossRef] [PubMed]
- Reid, I.R.; Bolland, M.J.; Grey, A.B. Is bisphosphonate-associated osteonecrosis of the jaw caused by soft tissue toxicity? Bone 2007, 41, 318–320. [Google Scholar] [CrossRef] [PubMed]
- Soares, A.L.; Simon, S.; Gebrim, L.H.; Nazário, A.C.P.; Lazaretti-Castro, M. Prevalence and risk factors of medication-related osteonecrosis of the jaw in osteoporotic and breast cancer patients: A cross-sectional study. Support. Care Cancer 2020, 28, 2265–2271. [Google Scholar] [CrossRef] [PubMed]
- Nicolatou-Galitis, O.; Schiødt, M.; Mendes, R.A.; Ripamonti, C.; Hope, S.; Drudge-Coates, L.; Niepel, D.; Van den Wyngaert, T. Medication-related osteonecrosis of the jaw: Definition and best practice for prevention, diagnosis, and treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 117–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giovannacci, I.; Meleti, M.; Manfredi, M.; Mortellaro, C.; Greco Lucchina, A.; Bonanini, M.; Vescovi, P. Medication-Related Osteonecrosis of the Jaw Around Dental Implants: Implant Surgery-Triggered or Implant Presence-Triggered Osteonecrosis? J. Craniofac. Surg. 2016, 27, 697–701. [Google Scholar] [CrossRef]
- Fedele, S.; Porter, S.R.; D’Aiuto, F.; Aljohani, S.; Vescovi, P.; Manfredi, M.; Arduino, P.G.; Broccoletti, R.; Musciotto, A.; Di Fede, O.; et al. Nonexposed variant of bisphosphonate-associated osteonecrosis of the jaw: A case series. Am. J. Med. 2010, 123, 1060–1064. [Google Scholar] [CrossRef] [Green Version]
- Ruggiero, S.L. Bisphosphonate-related osteonecrosis of the jaw (BRONJ): Initial discovery and subsequent development. J. Oral Maxillofac. Surg. 2009, 67, 13–18. [Google Scholar] [CrossRef]
- Colella, G.; Campisi, G.; Fusco, V. American Association of Oral and Maxillofacial Surgeons Position Paper: Bisphosphonate-Related Osteonecrosis of the Jaws—2009 Update: The Need to Refine the BRONJ Definition. J. Oral Maxillofac. Surg. 2009, 67, 2698–2699. [Google Scholar] [CrossRef]
- Khosla, S.; Burr, D.; Cauley, J.; Dempster, D.W.; Ebeling, P.R.; Felsenberg, D.; Gagel, R.F.; Gilsanz, V.; Guise, T.; Koka, S.; et al. Bisphosphonate-Associated Osteonecrosis of the Jaw: Report of a Task Force of the American Society for Bone and Mineral Research. J. Bone Miner. 2007, 22. [Google Scholar] [CrossRef] [Green Version]
- De Boissieu, P.; Kanagaratnam, L.; Abou Taam, M.; Roux, M.P.; Dramé, M.; Trenque, T. Notoriety bias in a database of spontaneous reports: The example of osteonecrosis of the jaw under bisphosphonate therapy in the French national pharmacovigilance database. Pharmacoepidemiol. Drug Saf. 2014, 23, 989–992. [Google Scholar] [CrossRef] [PubMed]
- De Boissieu, P.; Trenque, T. Adjuvant denosumab in early breast-cancer. Lancet Oncol. 2020, 21, e123. [Google Scholar] [CrossRef]
- De Boissieu, P.; Kanagaratnam, L.; Mahmoudi, R.; Morel, A.; Dramé, M.; Trenque, T. Adjudication of osteonecrosis of the jaw in phase III randomized controlled trials of denosumab: A systematic review. Eur. J. Clin. Pharmacol. 2017, 73, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Hellstein, J.W.; Adler, R.A.; Edwards, B.; Jacobsen, P.L.; Kalmar, J.R.; Koka, S.; Migliorati, C.A.; Ristic, H. Managing the care of patients receiving antiresorptive therapy for prevention and treatment of osteoporosis: Executive summary of recommendations from the American Dental Association Council on Scientific Affairs. J. Am. Dent. Assoc. 2011, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bedogni, A.; Blandamura, S.; Lokmic, Z.; Palumbo, C.; Ragazzo, M.; Ferrari, F.; Tregnaghi, A.; Pietrogrande, F.; Procopio, O.; Saia, G.; et al. Bisphosphonate-associated jawbone osteonecrosis: A correlation between imaging techniques and histopathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 105, 358–364. [Google Scholar] [CrossRef]
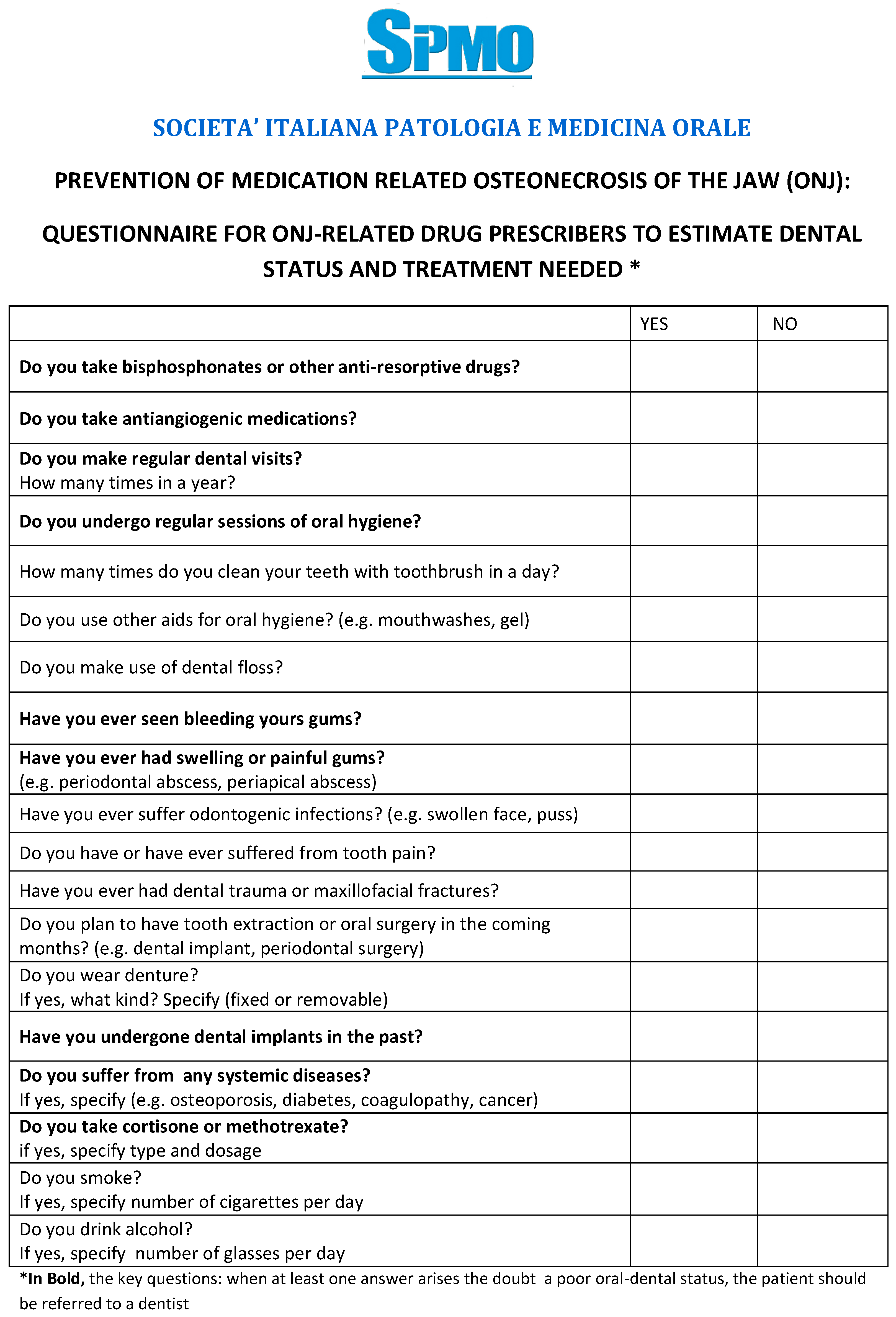
- SIPMO. Questionario per la Prevenzione Dell’osteonecrosi Delle Ossa Mascellari—SIPMO n.d. Available online: https://www.sipmo.it/questionario-per-la-prevenzione-dellosteonecrosi-delle-ossa-mascellari/ (accessed on 12 June 2020).
- Vescovi, P.; Campisi, G.; Fusco, V.; Mergoni, G.; Manfredi, M.; Merigo, E.; Solazzo, L.; Gabriele, M.; Gaeta, G.M.; Favia, G.; et al. Surgery-triggered and non surgery-triggered Bisphosphonate-related Osteonecrosis of the Jaws (BRONJ): A retrospective analysis of 567 cases in an Italian multicenter study. Oral Oncol. 2011, 47, 191–194. [Google Scholar] [CrossRef]
- Escobedo, M.F.; Cobo, J.L.; Junquera, S.; Milla, J.; Olay, S.; Junquera, L.M. Medication-related osteonecrosis of the jaw. Implant presence-triggered osteonecrosis: Case series and literature review. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 40–48. [Google Scholar] [CrossRef]
- Granate-Marques, A.; Polis-Yanes, C.; Seminario-Amez, M.; Jané-Salas, E.; López-López, J. Medication-related osteonecrosis of the jaw associated with implant and regenerative treatments: Systematic review. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e195–e203. [Google Scholar] [CrossRef]
- Walter, C.; Al-Nawas, B.; Wolff, T.; Schiegnitz, E.; Grötz, K.A. Dental implants in patients treated with antiresorptive medication—a systematic literature review. Int. J. Implant Dent. 2016, 2. [Google Scholar] [CrossRef] [Green Version]
- DeFRA. DeFRA79 Algorithm n.d. Available online: https://defra-osteoporosi.it/ (accessed on 8 June 2020).
- McClung, M.; Harris, S.T.; Miller, P.D.; Bauer, D.C.; Davison, K.S.; Dian, L.; Hanley, D.A.; Kendler, D.L.; Yuen, C.K.; Lewiecki, E.M. Bisphosphonate Therapy for Osteoporosis: Benefits, Risks, and Drug Holiday; Elsevier Inc.: Amsterdam, The Netherlands, 2013; Volume 126. [Google Scholar] [CrossRef]
- De Oliveira, C.C.; Brizeno, L.A.C.; de Sousa, F.B.; Mota, M.R.L.; Alves, A.P.N.N. Osteonecrosis of the jaw induced by receptor activator of nuclear factor-kappa B ligand (Denosumab)—Review. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e431–e439. [Google Scholar] [CrossRef]
- Adams, A.L.; Adams, J.L.; Raebel, M.A.; Tang, B.T.; Kuntz, J.L.; Vijayadeva, V.; McGlynn, E.A.; Gozansky, W.S. Bisphosphonate Drug Holiday and Fracture Risk: A Population-Based Cohort Study. J. Bone Miner. Res. 2018, 33, 1252–1259. [Google Scholar] [CrossRef]
- Raje, N.; Terpos, E.; Willenbacher, W.; Shimizu, K.; García-Sanz, R.; Durie, B.; Legieć, W.; Krejčí, M.; Laribi, K.; Zhu, L.; et al. Denosumab versus zoledronic acid in bone disease treatment of newly diagnosed multiple myeloma: An international, double-blind, double-dummy, randomised, controlled, phase 3 study. Lancet Oncol. 2018, 19, 370–381. [Google Scholar] [CrossRef]
- Bindon, B.; Adams, W.; Balasubramanian, N.; Sandhu, J.; Camacho, P. Osteoporotic fractures during bisphosphonate drug holiday. Endocr. Pract. 2018, 24, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Anagnostis, P.; Paschou, S.A.; Mintziori, G.; Ceausu, I.; Depypere, H.; Lambrinoudaki, I.; Mueck, A.; Pérez-López, F.R.; Rees, M.; Senturk, L.M.; et al. Drug holidays from bisphosphonates and denosumab in postmenopausal osteoporosis: EMAS position statement. Maturitas 2017, 101, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziebart, T.; Pabst, A.; Klein, M.O.; Kämmerer, P.; Gauss, L.; Brüllmann, D.; Al-Nawas, B.; Walter, C. Bisphosphonates: Restrictions for vasculogenesis and angiogenesis: Inhibition of cell function of endothelial progenitor cells and mature endothelial cells in vitro. Clin. Oral Investig. 2011, 15, 105–111. [Google Scholar] [CrossRef]
- Soares, M.Q.S.; Van Dessel, J.; Jacobs, R.; da Silva Santos, P.S.; Cestari, T.M.; Garlet, G.P.; Duarte, M.A.; Imada, T.S.; Lambrichts, I.; Rubira-Bullen, I.R. Zoledronic Acid Induces Site-Specific Structural Changes and Decreases Vascular Area in the Alveolar Bone. J. Oral Maxillofac. Surg. 2018, 76, 1893–1901. [Google Scholar] [CrossRef] [Green Version]
- Gao, S.Y.; Zheng, G.S.; Wang, L.; Liang, Y.J.; Zhang, S.E.; Lao, X.M.; Li, K.; Liao, G.Q. Zoledronate suppressed angiogenesis and osteogenesis by inhibiting osteoclasts formation and secretion of PDGF-BB. PLoS ONE 2017, 12, e0179248. [Google Scholar] [CrossRef]
- Manfredi, M.; Mergoni, G.; Goldoni, M.; Salvagni, S.; Merigo, E.; Meleti, M.; Vescovi, P. A 5-year retrospective longitudinal study on the incidence and the risk factors of osteonecrosis of the jaws in patients treated with zoledronic acid for bone metastases from solid tumors. Med. Oral Patol. Oral Cir. Bucal 2017, 22, e342–e348. [Google Scholar] [CrossRef] [Green Version]
- Malan, J.; Ettinger, K.; Naumann, E.; Beirne, O.R. The relationship of denosumab pharmacology and osteonecrosis of the jaws. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 671–676. [Google Scholar] [CrossRef]
- Higuchi, T.; Soga, Y.; Muro, M.; Kajizono, M.; Kitamura, Y.; Sendo, T.; Sasaki, A. Replacing zoledronic acid with denosumab is a risk factor for developing osteonecrosis of the jaw. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 547–551. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Risk Factor | ||
|---|---|---|
| Drug-Related | Systemic | Local |
| Product (Antiresorptive/antiangiogenic drug) Route of administration (po, sc, iv, im) Cumulative dosage Duration of treatments Supportive care (e.g., chemotherapy, steroids, thalidomide) | Underlying disease (solid tumors, multiple myeloma, osteoporosis) Comorbidity (e.g., diabetes, rheumatoid arthritis, hypocalcemia, hyperparathyroidism) Lifestyle (e.g., smoking) | Dental/periodontal infection Peri-implantitis Oral surgeries (e.g., dental extractions) Unfitting removable dentures Anatomical conditions (e.g., torus, exostosis, pronounced mylohyoid ridge) |
| Drug Suspensions in Cancer Patients | ||
| Active Pharmaceutical Ingredient | Last Administrations before Surgical Procedure | Resume Treatment |
| Bisphosphonates | At least 1 week before | At least 4–6 weeks after surgical procedures |
| Denosumab (Xgeva®) | At least 3 weeks before | |
| Bevacizumab | At least 5–8 weeks before | |
| Sunitinib | At least 1 week before | |
| Drug Suspensions in Osteometabolic Patients | ||
| Active Pharmaceutical Ingredient | Last Administrations before Surgical Procedure | Resume Treatment |
| Bisphosphonates * | At least 1 week before | At least 4–6 weeks after surgical procedures |
| Denosumab (Prolia®) | No suspension ** | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campisi, G.; Mauceri, R.; Bertoldo, F.; Bettini, G.; Biasotto, M.; Colella, G.; Consolo, U.; Di Fede, O.; Favia, G.; Fusco, V.; et al. Medication-Related Osteonecrosis of Jaws (MRONJ) Prevention and Diagnosis: Italian Consensus Update 2020. Int. J. Environ. Res. Public Health 2020, 17, 5998. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165998
Campisi G, Mauceri R, Bertoldo F, Bettini G, Biasotto M, Colella G, Consolo U, Di Fede O, Favia G, Fusco V, et al. Medication-Related Osteonecrosis of Jaws (MRONJ) Prevention and Diagnosis: Italian Consensus Update 2020. International Journal of Environmental Research and Public Health. 2020; 17(16):5998. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165998
Chicago/Turabian StyleCampisi, Giuseppina, Rodolfo Mauceri, Francesco Bertoldo, Giordana Bettini, Matteo Biasotto, Giuseppe Colella, Ugo Consolo, Olga Di Fede, Gianfranco Favia, Vittorio Fusco, and et al. 2020. "Medication-Related Osteonecrosis of Jaws (MRONJ) Prevention and Diagnosis: Italian Consensus Update 2020" International Journal of Environmental Research and Public Health 17, no. 16: 5998. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17165998