Clearing the Smoke Screen: Smoking, Alcohol Consumption, and Stress Management Techniques among Canadian Long-Term Care Workers

Abstract
:1. Introduction
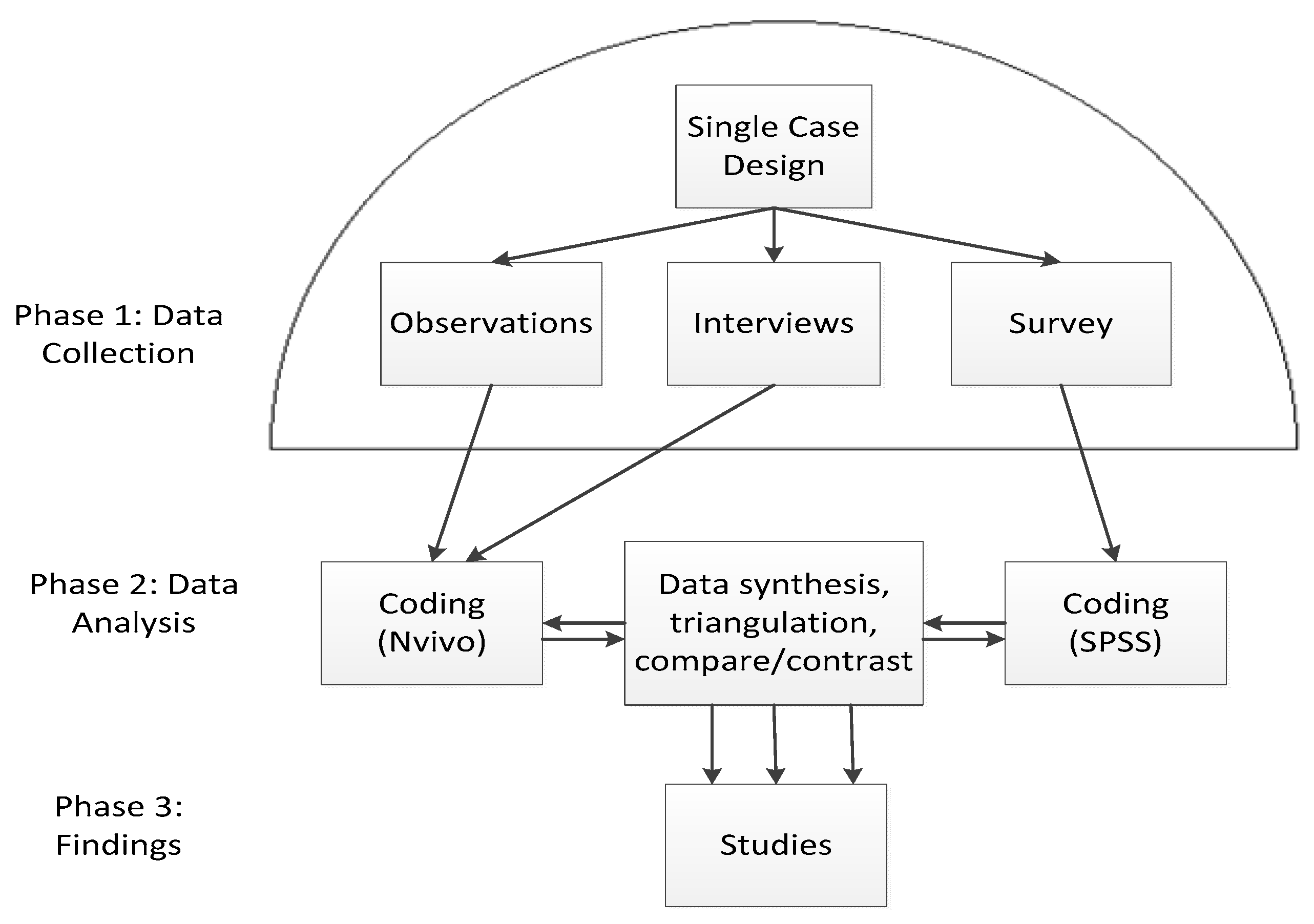
2. Materials and Methods
3. Results
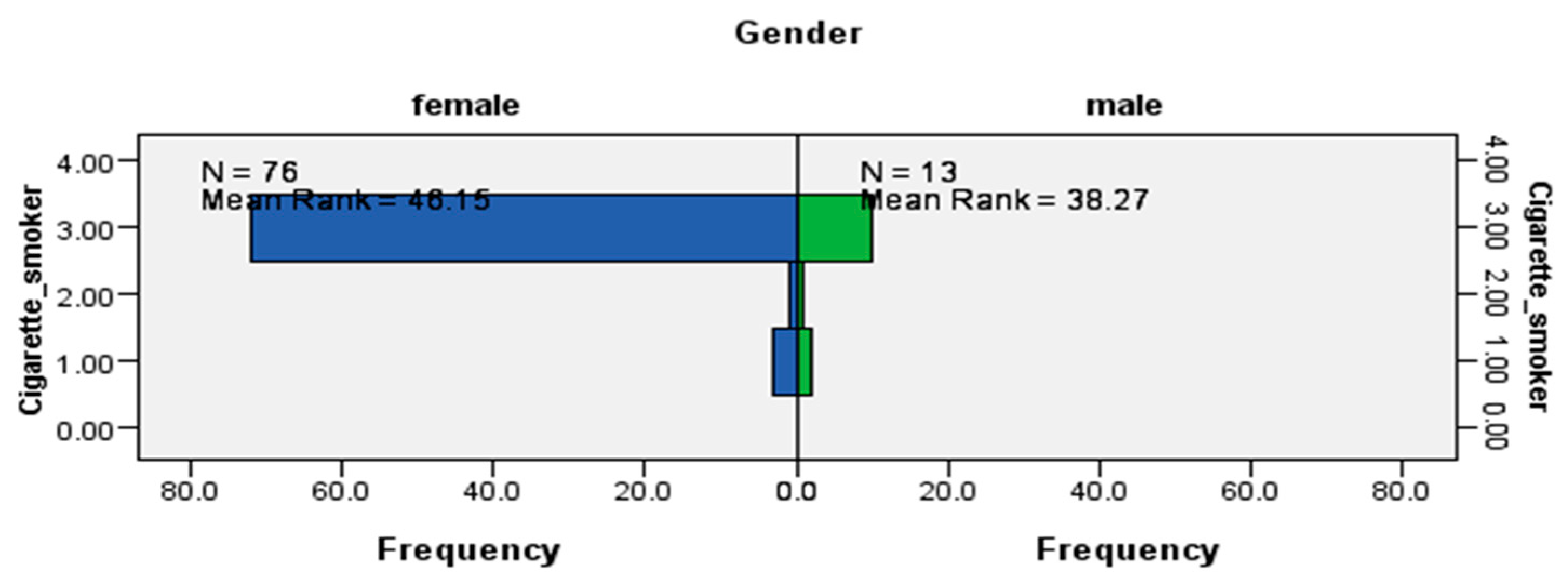
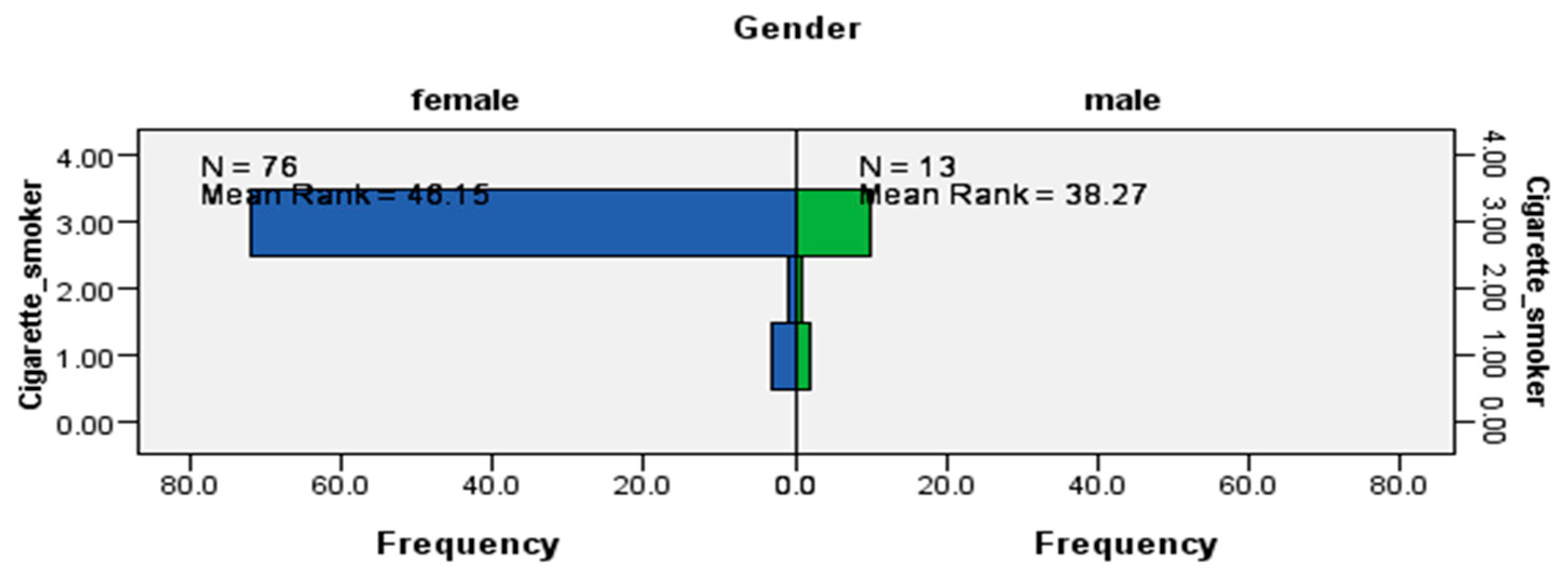
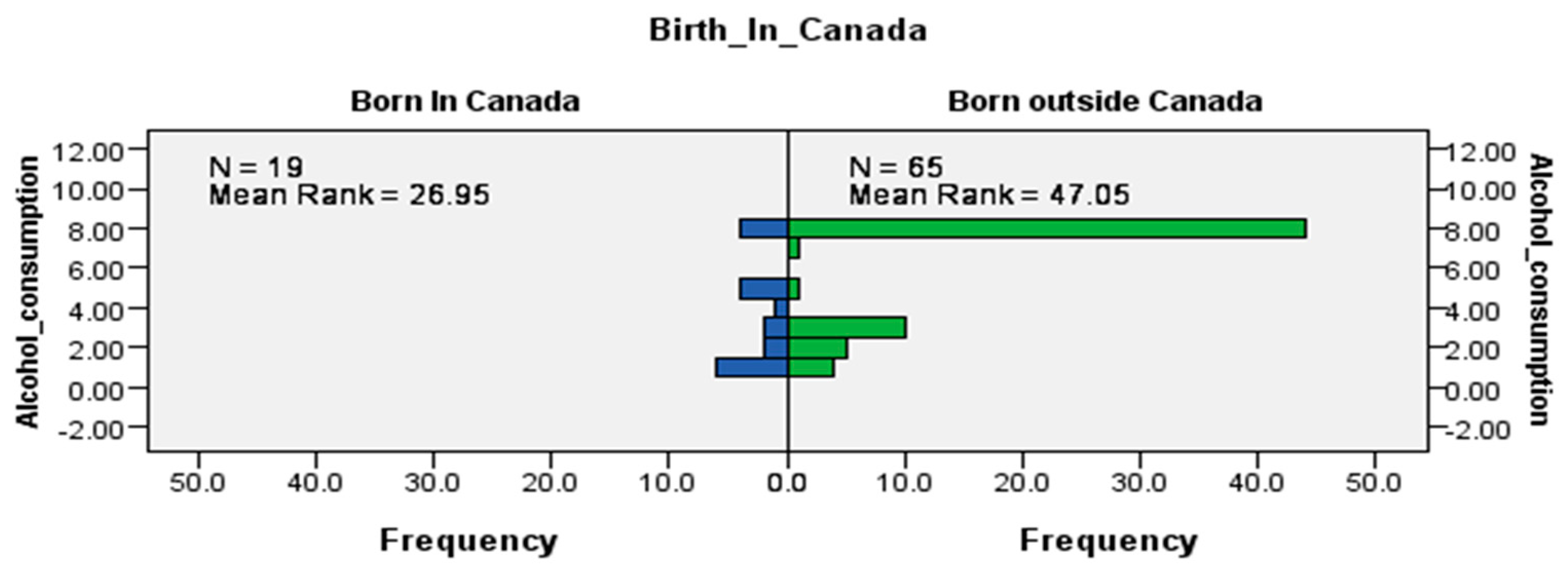
3.1. Smoking and Alcohol Consumption
3.2. Coping, Defense, and Stress Management Techniques
Individual Methods of Coping and Defense
3.3. Drawing on Social Support from Family, Friends, and the Community
Group Dynamics in Coping and Defense
4. Discussion
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Risk Factor and Disease or Injury Cause, by Age and Sex: Global Burden of Disease—Americas; World Health Organization: Geneva, Switzerland, 2004; Available online: http://www.who.int/healthinfo/global_burden_disease/risk_factors/en/index.htm (accessed on 2 June 2020).
- Oberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Prüss-Ustün, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2010. [Google Scholar] [CrossRef]
- Takala, J. Introductory Report: Decent Work—Safe Work. In Proceedings of the XVII World Congress on Safety and Health at Work, Orlando, FL, USA, 18–22 September 2005; International Labour Organization: Geneva, Switzerland, 2005. Available online: http://www.ilo.org/public/libdoc/ilo/2005/105B09_281_engl (accessed on 2 June 2020).
- Fathallah, N.; Maurel-Donnarel, E.; Baumstarck-Barrau, K.; Lehucher-Michel, M.P. Three-year follow-up of attitudes and smoking behaviour among hospital nurses following enactment of France’s national smoke-free workplace law. Int. J. Nurs. Stud. 2012, 49, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Baliunas, D.; Brochu, S.; Fischer, B.; Gnam, W.; Patra, J.; Popova, S.; Sarnocinska-Hart, A.; Taylor, B. The Costs of Substance Abuse in Canada; Canadian Centre on Substance Abuse: Ottawa, ON, Canada, 2006; Available online: https://ccsa.ca/sites/default/files/2019-05/ccsa-011332-2006.pdf (accessed on 2 June 2020).
- Yin, P.; Jiang, C.Q.; Cheng, K.K.; Lam, T.H.; Miller, M.R.; Zhang, W.S.; Thomas, G.N.; Adab, P. Passive smoking exposure and risk of COPD among adults in China: The Guangzhou Biobank Cohort Study. Lancet 2007, 370, 751–757. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009; Available online: http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf (accessed on 2 June 2020).
- World Health Organization (WHO). Guidelines for Implementation of the WHO Framework Convention on Tobacco Control; World Health Organization: Geneva, Switzerland, 2009; Available online: http://libdoc.who.int/publications/2009/9789241598224_eng.pdf (accessed on 2 June 2020).
- World Health Organization (WHO). WHO Report on the Global Tobacco Epidemic, 2009: Implementing Smoke-Free Environments; World Health Organization: Geneva, Switzerland, 2009; Available online: http://www.who.int/tobacco/mpower/2009/en/index.html (accessed on 2 June 2020).
- Government of Canada, Conference Board. The Costs of Tobacco Use in Canada, 2012. 2017. Available online: https://www.canada.ca/content/dam/hc-sc/documents/services/publications/healthy-living/costs-tobacco-use-canada-2012/Costs-of-Tobacco-Use-in-Canada-2012-eng.pdf (accessed on 2 June 2020).
- World Health Organization (WHO). Global Status Report on Alcohol; World Health Organization: Geneva, Switzerland, 2004; Available online: https://www.who.int/substance_abuse/publications/global_status_report_2004_overview.pdf (accessed on 2 June 2020).
- Butt, P.; Gliksman, L.; Beirness, D.; Paradis, C.; Stockwell, T. Alcohol and Health in Canada: A Summary of Evidence and Guidelines for Low-Risk Drinking; Canadian Centre on Substance Abuse: Ottawa, ON, Canada, 2011; Available online: https://ccsa.ca/sites/default/files/2019-04/2011-Summary-of-Evidence-and-Guidelines-for-Low-Risk%20Drinking-en.pdf (accessed on 31 July 2019).
- World Health Organization (WHO). Global Strategy to Reduce the Harmful Use of Alcohol; World Health Organization: Geneva, Switzerland, 2010; Available online: https://www.who.int/substance_abuse/activities/gsrhua/en/ (accessed on 2 June 2020).
- World Health Organization (WHO). Global Status Report on Alcohol and Health; World Health Organization: Geneva, Switzerland, 2018; Available online: https://www.who.int/substance_abuse/publications/global_alcohol_report/en/ (accessed on 2 June 2020).
- Health Canada. Alcohol. Available online: https://www.canada.ca/en/health-canada/services/health-concerns/alcohol-health-concerns.html (accessed on 31 July 2019).
- Health Canada. Problematic Alcohol Use. 2018. Available online: https://www.canada.ca/en/health-canada/services/substance-use/problematic-alcohol-use.html (accessed on 31 July 2019).
- Glanz, K.; Rimer, B.; Visawanath, K. (Eds.) Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2018. [Google Scholar]
- Mensch, B.S.; Kandel, D.B. Do job conditions influence the use of drugs? J. Health Soc. Behav. 1988, 29, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Azagba, S.; Sharaf, M.F. The effect of job stress on smoking and alcohol consumption. Health Econ. Rev. 2011, 15, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wills, T.A. Stress and Coping in Early Adolescence: Relationships to Substance Use in Urban School Samples. Health Psychol. 1986, 5, 503–529. [Google Scholar] [CrossRef] [PubMed]
- Wills, T.A.; Clearly, S.D. Stress-coping model for alcohol-tobacco interactions in adolescence. In Alcohol and Tobacco: From Basic Science to Clinical Practice; Fertig, J.B., Allen, J.P., Eds.; National Institutes of Health, National Institute on Alcohol Abuse and Alcoholism: Bethesda, MD, USA, 1995; pp. 107–128. [Google Scholar]
- Conway, T.L.; Vickers, R.R., Jr.; Ward, H.W.; Rahe, R.H. Occupational stress and variation in cigarette, coffee, and alcohol consumption. J. Health Soc. Behav. 1981, 22, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Beh, L.S.; Loo, L.H. ; Loo, L.H. Job stress and coping mechanisms among nursing staff in public health services. Int. J. Acad. Res. Bus. Soc. Sci. 2012, 2, 131–176. [Google Scholar]
- Bourgeault, I.L. Sociological perspectives on health and health care. Staying Alive: Critical Perspectives on Health, Illness and Health Care, 2nd ed.; Bryant, T., Raphael, D., Rioux, M., Eds.; Canadian Scholars Press: Toronto, ON, Canada, 2010; pp. 41–63. [Google Scholar]
- Biggs, L. Rethinking the History of Midwifery in Canada. Reconceiving Midwifery; Bourgeault, I.L., Benoit, C., Davis-Floyd, R., Eds.; McGill-Queen’s University Press: Montreal, QC, Canada, 2004; pp. 17–45. [Google Scholar]
- Dei, G.J.S. S. Critical Perspectives in Anti-racism: An Introduction. Can. Rev. Sociol. Anthropol. 1996, 33, 247–267. [Google Scholar] [CrossRef]
- Galabuzi, G.E. Canada’s Economic Apartheid: The Social Exclusion of Racialized Groups in the New Century; Canadian Scholars’ Press: Toronto, ON, Canada, 2006. [Google Scholar]
- Jones, T. Shades of Brown: The Law of Skin Color. Duke Law J. 2000, 49, 1487–1557. [Google Scholar] [CrossRef] [Green Version]
- National Collaborating Centre for Indigenous Health. Anti-Idegenous Racism in Canada. 2020. Available online: https://www.nccih.ca/419/Aboriginal_Racism_in_Canada.nccah (accessed on 10 July 2020).
- Ontario Human Rights Commission Racial Discrimination, Race and Racism (Fact Sheet). 2020. Available online: http://www.ohrc.on.ca/en/racial-discrimination-race-and-racism-fact-sheet (accessed on 6 July 2020).
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Syed, I. In Biomedicine, Thin Is Still In: Obesity Surveillance Among Racialized, (Im)migrant, and Female Bodies. Societies 2019, 9, 59. [Google Scholar] [CrossRef] [Green Version]
- Syed, I. Theorizing Precarization and Racialization as Social Determinants of Health: A Case Study Investigating Work in Long Term Residential Care. Ph.D. Thesis, York University, Toronto, ON, Canada, 2019. [Google Scholar]
- Syed, I. Chronic Illness among Immigrant Workers in Canada: An Overview of Existing Knowledge. In Working Bodies: Chronic Illness in the Canadian Workplace; Stone, S.D., Crooks, V.A., Owen, M., Eds.; McGill-Queen’s University Press: Montreal, QC, Canada, 2014; pp. 161–176. [Google Scholar]
- Syed, I.; Ahmad, F. A Scoping Literature Review of Work-Related Musculoskeletal Disorders among South Asian Immigrant Women in Canada. J. Glob. Health 2016, 6, 28–34. [Google Scholar]
- Syed, I.U.B. Labour Exploitation and Health Inequities among Market Migrants: A Political Economy Perspective. J. Int. Migr. Integr. 2015, 17, 449–465. [Google Scholar] [CrossRef]
- Syed, I.; Daly, T.; Armstrong, P.; Lowndes, R.; Chadoin, M.; Naidoo, V. How Do Work Hierarchies and Strict Divisions of Labour Impact Care Workers’ Experiences of Health and Safety? Case Studies of Long Term Care in Toronto. J. Nurs. Home Res. Sci. 2016, 2, 41–49. [Google Scholar] [PubMed]
- Syed, I.U. Diet, physical activity, and emotional health: What works, what doesn’t, and why we need integrated solutions for total worker health. BMC Public Health. 2020, 20, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikkonen, J.; Raphael, D. Social Determinants of Health: The Canadian Facts. 2010. Available online: http://www.thecanadianfacts.org/the_canadian_facts.pdf (accessed on 2 June 2020).
- Yin, R.K. Case Study Research Design and Methods, 5th ed.; Sage: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Langton, N.; Robbins, S.P.; Judge, T. Organizational Behavior: Concepts, Controversies, Applications, Eighth Canadian Edition; Pearson Canada Inc.: Don Mills, ON, Canada, 2019. [Google Scholar]
- Lee, M.P.; Hudson, H.; Richards, R.; Chang, C.C.; Chosewood, L.C.; Schill, A.L. Fundamentals of Total Worker Health® Approaches: Essential Elements for Advancing Worker Safety, Health, and Well-Being; Department of Health and Human Services: Cincinnati, OH, USA; Centers for Disease Control and Prevention (CDC): Atlanta, GA, USA; National Institute for Occupational Safety and Health (NIOSH): Washington, DC, USA, 2016. [Google Scholar]
- McLellan, R.K. Total worker health: A promising approach to a safer and healthier workforce. Ann. Intern. Med. 2016, 165, 294–295. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, G.; Barbeau, E. Steps to a Healthier U.S. Workforce: Integrating Occupational Health and Safety and Worksite Health Promotion: State of the Science. 2012 NIOSH Research Compendium. The NIOSH Total Worker Health Program: Seminal Research Papers. Presented at the Steps to a Healthier U.S. Workforce Symposium. Available online: http://www.cdc.gov/niosh/docs/2012-146/pdfs/2012-146.pdf (accessed on 2 June 2020).
- Pronk, N. Total Worker Health®: An Emerging Innovation in Workplace Health and Well-Being. ACSM’s Health Fit. J. 2020, 24, 42. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Frequency | % | |
|---|---|---|---|
| Sex | Female | 35 | 83.3% |
| Male | 7 | 16.7% | |
| Employment Type | Full Time | 32 | 76.2% |
| Part Time | 10 | 23.8% | |
| Race/VM Status | Non-VM, non-racialized, White | 12 | 28.6% |
| VM, racialized | 30 | 71.4% | |
| Job Title/Role | Trainee | 3 | 7.1% |
| Allied Health | 7 | 16.7% | |
| Nurse | 9 | 21.4% | |
| Manager | 4 | 9.5% | |
| Support Staff | 6 | 14.3% | |
| Ancillary | 6 | 14.3% | |
| Personal Support Worker (PSW) | 7 | 16.7% | |
| Characteristic | Frequency | % | |
|---|---|---|---|
| Sex | Female | 76 | 83.5% |
| Male | 14 | 15.4% | |
| No response/omitted | 1 | 1.1% | |
| Birth/Immigration Status | Born in Canada | 19 | 20.9% |
| Born outside Canada, i.e., Immigrant | 66 | 72.5% | |
| No responses/omitted | 6 | 6.6% | |
| Race/VM Status | Non-VM, non-racialized | 11 | 12.1% |
| VM, racialized | 78 | 85.7% | |
| No response/omitted | 2 | 2.2% | |
| Smoking Status | Smoker | 7 | 7.7% |
| Non-smoker | 83 | 91.2% | |
| No response/omitted | 1 | 1.1% | |
| Alcohol Consumption | Yes | 39 | 43.40% |
| No | 51 | 56.7% | |
| No response/omitted | 1 | 1.1% | |
| Smoking Status | Frequency | % |
|---|---|---|
| Daily | 5 | 5.6% |
| Occasionally | 2 | 2.2% |
| Not at all, i.e., non-Smoker | 83 | 92.2% |
| Total | 90 | 100.0% |
| Alcohol Consumption | Frequency | % |
|---|---|---|
| Less than once a month | 11 | 12.2% |
| Once a month | 7 | 7.8% |
| 2 to 3 times a month | 13 | 14.4% |
| Once a week | 1 | 1.1% |
| 2 to 3 times a week | 6 | 6.7% |
| 4 to 6 times a week | 0 | 0.0% |
| Every day | 1 | 1.1% |
| Not at all | 51 | 56.7% |
| Total | 90 | 100.0% |
| Alcohol Consumption | Sex | |||||
|---|---|---|---|---|---|---|
| n = 90 | n = 76 | n = 13 | ||||
| Response | Frequency | % | Female | % | Male | % |
| Less than once a month | 11 | 12.2% | 9 | 81.8% | 2 | 18.2% |
| Once a month | 7 | 7.8% | 5 | 71.4% | 1 | 14.3% |
| 2 to 3 times a month | 13 | 14.4% | 11 | 84.6% | 2 | 15.4% |
| Once a week | 1 | 1.1% | 0 | 0% | 1 | 100% |
| 2 to 3 times a week | 6 | 6.7% | 4 | 66.7% | 2 | 33.3% |
| 4 to 6 times a week | 0 | 0% | 0 | 0% | 0 | 0% |
| Every day | 1 | 1.1% | 1 | 100% | 0 | 0% |
| Not at all | 51 | 56.7% | 46 | 90.2% | 5 | 9.8% |
| Total | 90 | 100% | 76 | 84.4% | 13 | 14.4% |
| Alcohol Consumption | VM Status | |||||
|---|---|---|---|---|---|---|
| n = 90 | n = 77 | n = 11 | ||||
| Response | Frequency | % | VM | % | Non-VM | % |
| Less than once a month | 11 | 12.2% | 9 | 81.8% | 1 | 9.1% |
| Once a month | 7 | 7.8% | 7 | 100% | 0 | 0% |
| 2 to 3 times a month | 13 | 14.4% | 10 | 76.9% | 3 | 23.1% |
| Once a week | 1 | 1.1% | 0 | 1 | 100% | |
| 2 to 3 times a week | 6 | 6.7% | 4 | 66.7% | 2 | 33.3% |
| 4 to 6 times a week | 0 | 0% | 0 | 0% | 0 | 0% |
| Every day | 1 | 1.1% | 1 | 100% | 0 | 0% |
| Not at all | 51 | 56.7% | 46 | 90.2% | 4 | 7.8% |
| Total | 90 | 100% | 77 | 85.6% | 11 | 12.2% |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Syed, I.U. Clearing the Smoke Screen: Smoking, Alcohol Consumption, and Stress Management Techniques among Canadian Long-Term Care Workers. Int. J. Environ. Res. Public Health 2020, 17, 6027. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176027
Syed IU. Clearing the Smoke Screen: Smoking, Alcohol Consumption, and Stress Management Techniques among Canadian Long-Term Care Workers. International Journal of Environmental Research and Public Health. 2020; 17(17):6027. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176027
Chicago/Turabian StyleSyed, Iffath Unissa. 2020. "Clearing the Smoke Screen: Smoking, Alcohol Consumption, and Stress Management Techniques among Canadian Long-Term Care Workers" International Journal of Environmental Research and Public Health 17, no. 17: 6027. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176027