Rural SNAP Participants and Food Insecurity: How Can Communities Leverage Resources to Meet the Growing Food Insecurity Status of Rural and Low-Income Residents?

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
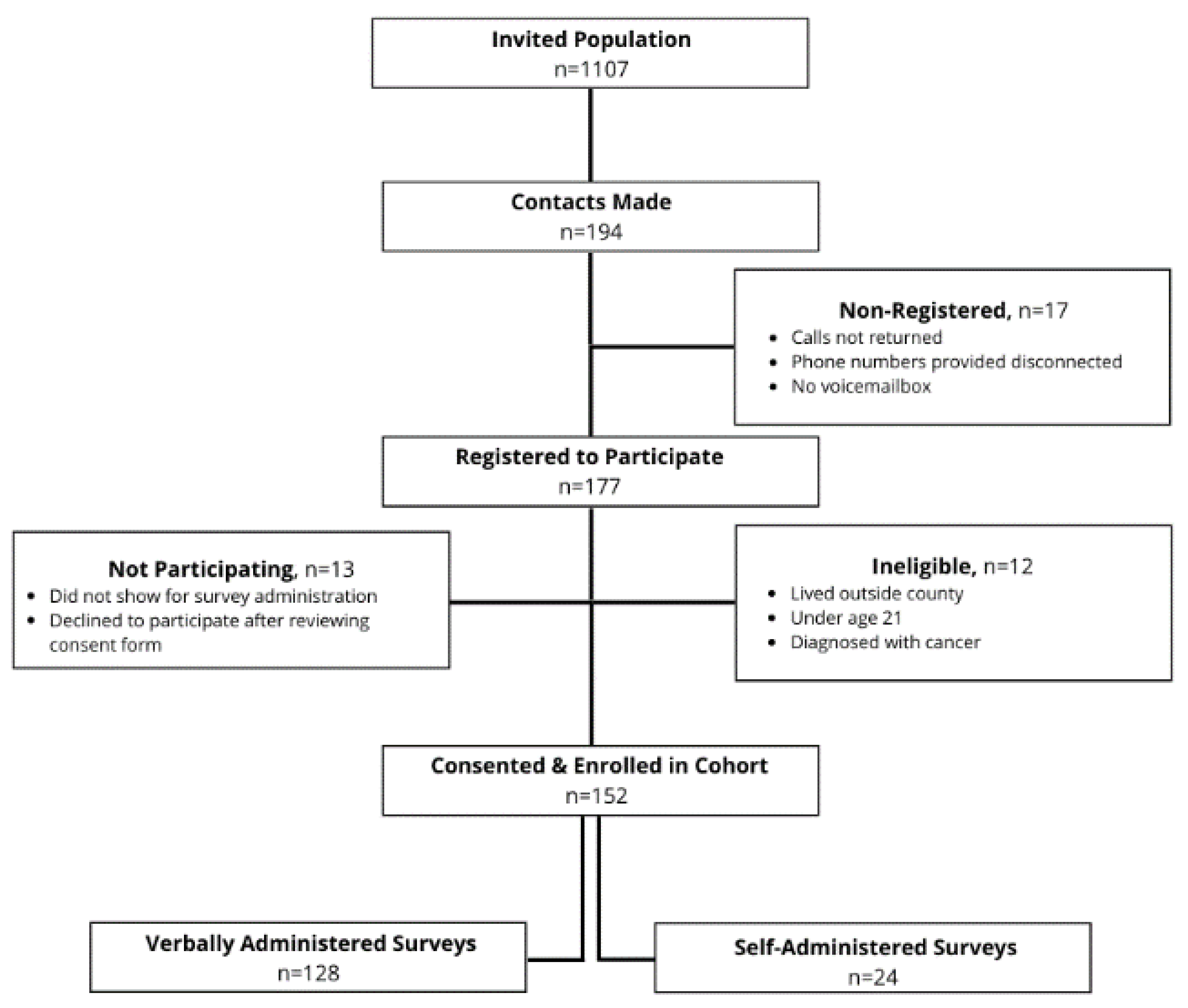
2.1. Baseline Survey Administration
2.2. Measures
2.2.1. Independent Variables
2.2.2. Dependent Variables
2.2.3. Covariates
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Shopping Practices
3.3. Fruit and Vegetable Intakes
3.4. SNAP and Food Insecurity
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Befort, C.A.; Nazir, N.; Perri, M.G. Prevalence of Obesity among Adults from Rural and Urban Areas of the United States: Findings from NHANES (2005–2008). J. Rural Health 2012, 28, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bethea, T.N.; Lopez, R.P.; Cozier, Y.C.; White, L.F.; McClean, M.D. The Relationship Between Rural Status, Individual Characteristics, and Self-Rated Health in the Behavioral Risk Factor Surveillance System. J. Rural Health 2012, 28, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monnat, S.M.; Pickett, C.B. Rural/Urban differences in self-rated health: Examining the roles of county size and metropolitan adjacency. Health Place 2011, 17, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, N.; Johnson, N.E.; Morton, L.W. Spatial Patterns of Rural Mortality. In Critical Issues in Rural Health; Blackwell Pub: Ames, IA, USA, 2004. [Google Scholar]
- Ormond, B.A.Z.; Stephen, Z.; Lhila, A. Rural/Urban Differences in Health Care Are Not Uniform Across States. In Assessing the New Federalism; The Urban Institute: Washington, DC, USA, 2000. [Google Scholar]
- Zahnd, W.E. Health Literacy Skills in Rural and Urban Populations. Am. J. Health Behav. 2009, 33, 550–557. [Google Scholar] [CrossRef]
- Matthews, K.A. Health-Related Behaviors by Urban-Rural County Classification—United States, 2013. MMWR Surveill. Summ. 2017, 66, 1–8. [Google Scholar] [CrossRef]
- Dean, W.R.; Sharkey, J.R. Rural and Urban Differences in the Associations between Characteristics of the Community Food Environment and Fruit and Vegetable Intake. J. Nutr. Educ. Behav. 2011, 43, 426–433. [Google Scholar] [CrossRef] [Green Version]
- Trivedi, T.; Liu, J.; Probst, J.C.; Merchant, A.T.; Jhones, S.; Martin, A.B. Obesity and obesity-related behaviors among rural and urban adults in the USA. Rural Remote Health 2015, 15, 3267. [Google Scholar]
- Coleman-Jensen, A. Household Food Security in the United States in 2016. In Economic Research Report Number 237; United States Department of Agriculture: Washington, DC, USA, 2017. [Google Scholar]
- Jackson, J.E.; Doescher, M.P.; Jerant, A.F.; Hart, L.G. A National Study of Obesity Prevalence and Trends by Type of Rural County. J. Rural Health 2005, 21, 140–148. [Google Scholar] [CrossRef]
- Hamer, S.P.H. 2017 Census of Agriculture United States Summary and State Data. In Geographic Area Series; United States Department of Agriculture: Washington, DC, USA, 2019; pp. 1–820. [Google Scholar]
- Median Household Income of Principal Farm Operators by Source and Sales Class. 2018. Available online: https://www.ers.usda.gov/data-products/chart-gallery/gallery/chart-detail/?chartId=58426 (accessed on 27 November 2019).
- Smith, C.; Morton, L.W. Rural Food Deserts: Low-Income Perspectives on Food Access in Minnesota and Iowa. J. Nutr. Educ. Behav. 2009, 41, 176–187. [Google Scholar] [CrossRef]
- Scott, J.; Dardas, L.; Sloane, R.; Wigington, T.; Noonan, D.; Simmons, L.A. Understanding Social Determinants of Cardiometabolic Disease Risk in Rural Women. J. Community Health 2019, 45, 1–9. [Google Scholar] [CrossRef]
- United States Department of Agriculture. Trends in Supplemental Nutrition Assistance Program Participation Rates: Fiscal Year 2010 to Fiscal Year 2017—Final Report. Available online: https://fns-prod.azureedge.net/sites/default/files/resource-files/Trends2010-2017.pdf (accessed on 7 April 2020).
- Harnack, L.; Valluri, S.; French, S.A. Importance of the Supplemental Nutrition Assistance Program in Rural America. Am. J. Public Health 2019, 109, 1641–1645. [Google Scholar] [CrossRef] [PubMed]
- Rural Poverty & Well-Being. Available online: https://www.ers.usda.gov/topics/rural-economy-population/rural-poverty-well-being/ (accessed on 8 June 2020).
- Food Research & Action Center. Rural Hunger in America: Supplemental Nutrition Assistance Program. 2018. Available online: https://frac.org/wp-content/uploads/rural-hunger-in-america-snap-get-the-facts.pdf (accessed on 7 April 2020).
- Food and Nutrition Service. Trends in Supplemental Nutrition Assistance Program Participation Rates: Fiscal Year 2010 to Fiscal Year 2017. 2019. Available online: https://www.fns.usda.gov/snap/trends-supplemental-nutrition-assistance-program-participation-rates-fiscal-year-2010 (accessed on 8 June 2020).
- Gunderson, C.; Dewey, A.; Englehard, E.; Strayer, M.; Lapinski, L.; Odeen, B.; Hartman, C. Map the Meal Gap 2020; Feeding America: Chicago, IL, USA, 2020. [Google Scholar]
- Mabli, J.; Ohls, J. Supplemental Nutrition Assistance Program Participation Is Associated with an Increase in Household Food Security in a National Evaluation. J. Nutr. 2014, 145, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Wallace, H.S.; Franck, K.L.; Sweet, C.L. Community Coalitions for Change and the Policy, Systems, and Environment Model: A Community-Based Participatory Approach to Addressing Obesity in Rural Tennessee. Prev. Chronic Dis. 2019, 16, E120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kegler, M.C.; Honeycutt, S.; Davis, M.; Dauria, E.; Berg, C.; Dove, C.; Gamble, A.; Hawkins, J. Policy, Systems, and Environmental Change in the Mississippi Delta. Health Educ. Behav. 2015, 42, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Barnidge, E.; Baker, E.A.; Estlund, A.; Motton, F.; Hipp, P.R.; Brownson, R.C. A Participatory Regional Partnership Approach to Promote Nutrition and Physical Activity Through Environmental and Policy Change in Rural Missouri. Prev. Chronic Dis. 2015, 12, E92. [Google Scholar] [CrossRef] [Green Version]
- Morland, K.; Evenson, K.R. Obesity prevalence and the local food environment. Health Place 2009, 15, 491–495. [Google Scholar] [CrossRef] [Green Version]
- Krukowski, R.A.; West, D.S.; Harvey-Berino, J.; Prewitt, T.E. Neighborhood Impact on Healthy Food Availability and Pricing in Food Stores. J. Community Health 2010, 35, 315–320. [Google Scholar] [CrossRef] [Green Version]
- Dwyer-Lindgren, L.; Bertozzi-Villa, A.; Stubbs, R.W.; Morozoff, C.; MacKenbach, J.P.; Van Lenthe, F.J.; Mokdad, A.H.; Murray, C.J.L. Inequalities in Life Expectancy Among US Counties, 1980 to 2014: Temporal Trends and Key Drivers. JAMA Intern. Med. 2017, 177, 1003–1011. [Google Scholar] [CrossRef] [Green Version]
- Lichter, D.T. Emerging Patterns of Population Redistribution and Migration in Appalachia; Citeseer: Princeton, NJ, USA, 2005. [Google Scholar]
- Social Vulnerability Index; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020.
- QuickFacts: Martin County, Kentucky. Available online: https://www.census.gov/quickfacts/martincountykentucky (accessed on 7 April 2020).
- Feeding America. Food Insecurity in Martin County. Map the Meal Gap 2016. Available online: https://map.feedingamerica.org/county/2016/overall/kentucky/county/martin (accessed on 7 April 2020).
- SNAP Participation Map. 2019. Available online: https://frac.org/snap-county-map/snap-counties.html (accessed on 8 June 2020).
- NIH National Cancer Institute Division of Cancer Control & Population Sciences. Scoring the All-Day Screener. Available online: https://epi.grants.cancer.gov/diet/screeners/fruitveg/scoring/allday.html (accessed on 27 November 2019).
- Thompson, F.E.; Subar, A.F.; Smith, A.F.; Midthune, D.; Radimer, K.L.; Kahle, L.L.; Kipnis, V. Fruit and Vegetable Assessment. J. Am. Diet. Assoc. 2002, 102, 1764–1772. [Google Scholar] [CrossRef]
- American Time Use Survey. Eating & Health Module 2014–2016 Questionnaire. 2017. Available online: https://www.bls.gov/tus/ehmquestionnaire1416.pdf (accessed on 27 November 2019).
- Ogden, C.L. Obesity and socioeconomic status in adults: United States, 2005–2008. NCHS Data Br. 2010, 50, 1. [Google Scholar]
- Levine, J.A. Poverty and obesity in the U.S. Diabetes 2011, 60, 2667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregory, C. Supplemental Nutrition Assistance Program (SNAP) Participation Leads to Modest Changes in Diet Quality; SNAP: Clinton, TN, USA, 2013. [Google Scholar]
- Ratcliffe, C.; McKernan, S.-M.; Zhang, S. How Much Does the Supplemental Nutrition Assistance Program Reduce Food Insecurity? Am. J. Agric. Econ. 2011, 93, 1082–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kendall, M.; Broyles, S.T.; Freightman, J.; Cater, M.; Holston, D. Opportunities and Challenges Addressing Access to Healthy Food in Five Rural Louisiana Food Stores. Prev. Chronic Dis. 2019, 16, 16. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Sharpe, P.A.; Bell, B.A.; Liu, J.; White, K.; Liese, A.D. Food Acquisition and Shopping Patterns among Residents of Low-Income and Low-Access Communities in South Carolina. J. Acad. Nutr. Diet. 2018, 118, 1844–1854. [Google Scholar] [CrossRef]
- Sohi, I.; Bell, B.A.; Liu, J.; Battersby, S.E.; Liese, A.D. Differences in food environment perceptions and spatial attributes of food shopping between residents of low and high food access areas. J. Nutr. Educ. Behav. 2014, 46, 241–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appalachian Regional Commission. The Appalachian Region. Available online: https://www.arc.gov/appalachian_region/TheAppalachianRegion.asp (accessed on 8 June 2020).
- Pollard, K.; Jacobsen, L.A. The Appalachian Region: A Data Overview from the 2013–2017 American Community Survey. In Chartbook; Appalachian Regional Commission: Washington, DC, USA, 2019. [Google Scholar]
- Nguyen, B.T.; Shuval, K.; Bertmann, F.; Yaroch, A.L. The Supplemental Nutrition Assistance Program, Food Insecurity, Dietary Quality, and Obesity among US Adults. Am. J. Public Health 2015, 105, 1453–1459. [Google Scholar] [CrossRef] [PubMed]
- Defosset, A.R.; Kwan, A.; Rizik-Baer, D.; Gutierrez, L.; Gase, L.N.; Kuo, T. Implementing a Healthy Food Distribution Program: A Supply Chain Strategy to Increase Fruit and Vegetable Access in Underserved Areas. Prev. Chronic Dis. 2018, 15, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, A.E.; Jennings, R.; Smiley, A.W.; Medina, J.L.; Sharma, S.; Rutledge, R.; Stigler, M.H.; Hoelscher, D. Introduction of farm stands in low-income communities increases fruit and vegetable among community residents. Health Place 2012, 18, 1137–1143. [Google Scholar] [CrossRef]
- Gans, K.; Risica, P.M.; Keita, A.D.; Dionne, L.; Mello, J.; Stowers, K.C.; Papandonatos, G.D.; Whittaker, S.; Gorham, G. Multilevel approaches to increase fruit and vegetable intake in low-income housing communities: Final results of the ‘Live Well, Viva Bien’ cluster-randomized trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 80. [Google Scholar] [CrossRef] [Green Version]
- Dunn, C.G. Feeding low-income children during the Covid-19 pandemic. N. Engl. J. Med. 2020, 382, e40. [Google Scholar] [CrossRef]
- Feeding America. The Impact of the Coronavirus on Food Insecurity. Available online: https://www.feedingamerica.org/sites/default/files/2020-04/Brief_Impact%20of%20Covid%20on%20Food%20Insecurity%204.22%20%28002%29.pdf (accessed on 8 June 2020).
- Miller, W. Community Adaptations to an Impending Food Desert in Rural Appalachia, USA. Rural Remote Health 2016, 16, 3901. [Google Scholar] [PubMed]
- Fleischhacker, S.E. Strengthening national nutrition research: Rationale and options for a new coordinated federal research effort and authority. Am. J. Clin. Nutr. 2020, 179. [Google Scholar] [CrossRef]
- SNAP COVID-19 Waivers. Available online: https://www.fns.usda.gov/programs/fns-disaster-assistance/fns-response-covid-19/snap-covid-19-waivers (accessed on 8 July 2020).
- Kinsey, E.W.; Kinsey, D.; Rundle, A.G. COVID-19 and Food Insecurity: An Uneven Patchwork of Responses. J. Hered. 2020, 97, 332–335. [Google Scholar] [CrossRef] [PubMed]
- Farley, K.W.; Bush, C.B. Using Relationships as Resources in Social Impact Investing: Examining a Local Food Movement in Appalachia. J. Appalach. Stud. 2016, 22, 224. [Google Scholar] [CrossRef]
- Glanz, K.; Sallis, J.F.; Saelens, B.E.; Frank, L.D. Nutrition Environment Measures Survey in Stores (NEMS-S) Development and Evaluation. Am. J. Prev. Med. 2007, 32, 282–289. [Google Scholar] [CrossRef]
- Thomson, J.L.; Goodman, M.H.; Landry, A.S. Measurement of Nutrition Environments in Grocery Stores, Convenience Stores, and Restaurants in the Lower Mississippi Delta. Prev. Chronic Dis. 2020, 17, 17. [Google Scholar] [CrossRef] [Green Version]
- Barnidge, E.; Hipp, P.R.; Estlund, A.; Duggan, K.; Barnhart, K.J.; Brownson, R.C. Association between community garden participation and fruit and vegetable consumption in rural Missouri. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 128. [Google Scholar] [CrossRef] [Green Version]
- Gamburzew, A.; Darcel, N.; Gazan, R.; Dubois, C.; Maillot, M.; Tomé, D.; Raffin, S.; Darmon, N. In-Store marketing of inexpensive foods with good nutritional quality in disadvantaged neighborhoods: Increased awareness, understanding, and purchasing. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 104. [Google Scholar] [CrossRef]
- Paek, H.-J.; Oh, H.J.; Jung, Y.; Thompson, T.; Alaimo, K.; Risley, J.; Mayfield, K. Assessment of a Healthy Corner Store Program (FIT Store) in Low-Income, Urban, and Ethnically Diverse Neighborhoods in Michigan. Fam. Community Health 2014, 37, 86–99. [Google Scholar] [CrossRef]
- Ball, K.; Abbott, G.; Wilson, M.; Chisholm, M.; Sahlqvist, S. How to get a nation walking: Reach, retention, participant characteristics and program implications of Heart Foundation Walking, a nationwide Australian community-based walking program. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 161. [Google Scholar] [CrossRef] [Green Version]
- Rejeski, W.J.; Ambrosius, W.T.; Burdette, J.H.; Walkup, M.P.; Marsh, A.P. Community Weight Loss to Combat Obesity and Disability in At-Risk Older Adults. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2017, 72, 1547–1553. [Google Scholar] [CrossRef] [PubMed]
- Lenstra, N.; Carlos, J. Public Libraries and Walkable Neighborhoods. Int. J. Environ. Res. Public Health 2019, 16, 1780. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Demographic Characteristic | Among All Participants % (n) | Among Martin County Population % 1 |
|---|---|---|
| Age (mean, in years) 2 | 56 (22–84) | |
| Gender | ||
| Male | 34.9 (53) | 55.3 |
| Female | 65.1 (99) | 44.7 |
| Race | ||
| White | 98.7 (150) | 91.4 |
| Non-white | 1.3 (2) | 8.5 |
| Education | ||
| Less than high school 2 | 43.4 (66) | |
| High school graduate | 36.2 (55) | 72.8 |
| Post-high school | 20.4 (31) | 8.5 |
| Household Income 3 | ||
| <USD 20,000 | 60.4 (90) | USD $35,000 (median) |
| ≥USD 20,000 | 39.6 (59) | |
| Martin County Residency 2,3 | ||
| <20 years | 17.2 (26) | |
| ≥20 years | 82.8 (125) | |
| SNAP Participation 4 | ||
| Yes | 39.5 (60) | 30.7 |
| No | 60.5 (92) |
| Shopping Practice | SNAP | |||
|---|---|---|---|---|
| All % (n) | Participant % (n) | Non-Participant % (n) | p-Value | |
| N | 152 | 60 | 92 | |
| Are you the person who usually does the grocery shopping in your household? | ||||
| Yes | 70.4 (107) | 71.7 (43) | 69.6 (64) | 0.85 |
| No | 12.5 (19) | 13.3 (8) | 12 (11) | |
| I split it with other household members | 17.1 (26) | 15.0 (9) | 18.5 (17) | |
| Where do you get most of your groceries? | ||||
| Grocery store | 80.3 (122) | 83.3 (50) | 78.3 (72) | 0.44 |
| Super center | 20.4 (31) | 18.3 (11) | 21.7 (20) | 0.61 |
| Discount store | 0.7 (1) | 0.0 (0) | 1.1 (1) | 1.00 |
| What is the primary reason you shop there? | ||||
| Price | 42.1 (64) | 50.0 (30) | 37.0 (34) | 0.11 |
| Location | 40.8 (62) | 38.3 (23) | 42.4 (39) | 0.62 |
| Quality | 7.9 (12) | 3.3 (2) | 10.9 (10) | 0.13 |
| Variety | 9.2 (14) | 8.3 (5) | 9.8 (9) | 0.76 |
| Are you aware of the farmers’ market in your community? | ||||
| Yes | 82.9 (126) | 75.0 (45) | 88.0 (81) | 0.05 |
| No | 17.1 (26) | 25.0 (15) | 12.0 (11) | |
| Do you regularly shop at the farmers’ market in your community? | ||||
| Yes | 21.2 (32) | 16.9 (10) | 23.9 (22) | 0.41 |
| No | 78.8 (119) | 83.1 (49) | 76.1 (70) | |
| Which of the following statements best describes the amount of food eaten in your household in the last 30 days? | ||||
| Enough food | 70.9 (107) | 58.3 (35) | 79.1 (72) | <0.01 |
| Not enough food | 29.1 (44) | 41.7 (25) | 20.9 (19) | |
| Gender | SNAP | |||
|---|---|---|---|---|
| Participant | Non-Participant | |||
| Mean FV Servings | 95% CI | Mean FV Servings | 95% CI | |
| Male | 2.77 | (1.99–3.85) | 4.45 | (3.43–5.76) |
| Female | 3.94 | (3.12–4.99) | 2.97 | (2.45–3.60) |
| Characteristic | SNAP Participant vs. Non-Participant | |
|---|---|---|
| Odds Ratio | 95% CI | |
| Food Insecurity | ||
| Female | 3.136 | (1.288–7.636) |
| Male | 2.000 | (0.578–6.920) |
| Overall | 2.707 | (1.317–5.563) |
| Not Enough FV | ||
| Female | 1.366 | (0.595–3.131) |
| Male | 1.659 | (0.542–5.080) |
| Overall | 1.475 | (0.761–2.859) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
DeWitt, E.; Gillespie, R.; Norman-Burgdolf, H.; Cardarelli, K.M.; Slone, S.; Gustafson, A. Rural SNAP Participants and Food Insecurity: How Can Communities Leverage Resources to Meet the Growing Food Insecurity Status of Rural and Low-Income Residents? Int. J. Environ. Res. Public Health 2020, 17, 6037. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176037
DeWitt E, Gillespie R, Norman-Burgdolf H, Cardarelli KM, Slone S, Gustafson A. Rural SNAP Participants and Food Insecurity: How Can Communities Leverage Resources to Meet the Growing Food Insecurity Status of Rural and Low-Income Residents? International Journal of Environmental Research and Public Health. 2020; 17(17):6037. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176037
Chicago/Turabian StyleDeWitt, Emily, Rachel Gillespie, Heather Norman-Burgdolf, Kathryn M. Cardarelli, Stacey Slone, and Alison Gustafson. 2020. "Rural SNAP Participants and Food Insecurity: How Can Communities Leverage Resources to Meet the Growing Food Insecurity Status of Rural and Low-Income Residents?" International Journal of Environmental Research and Public Health 17, no. 17: 6037. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176037