Immersive Virtual Reality Applications in Schizophrenia Spectrum Therapy: A Systematic Review

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
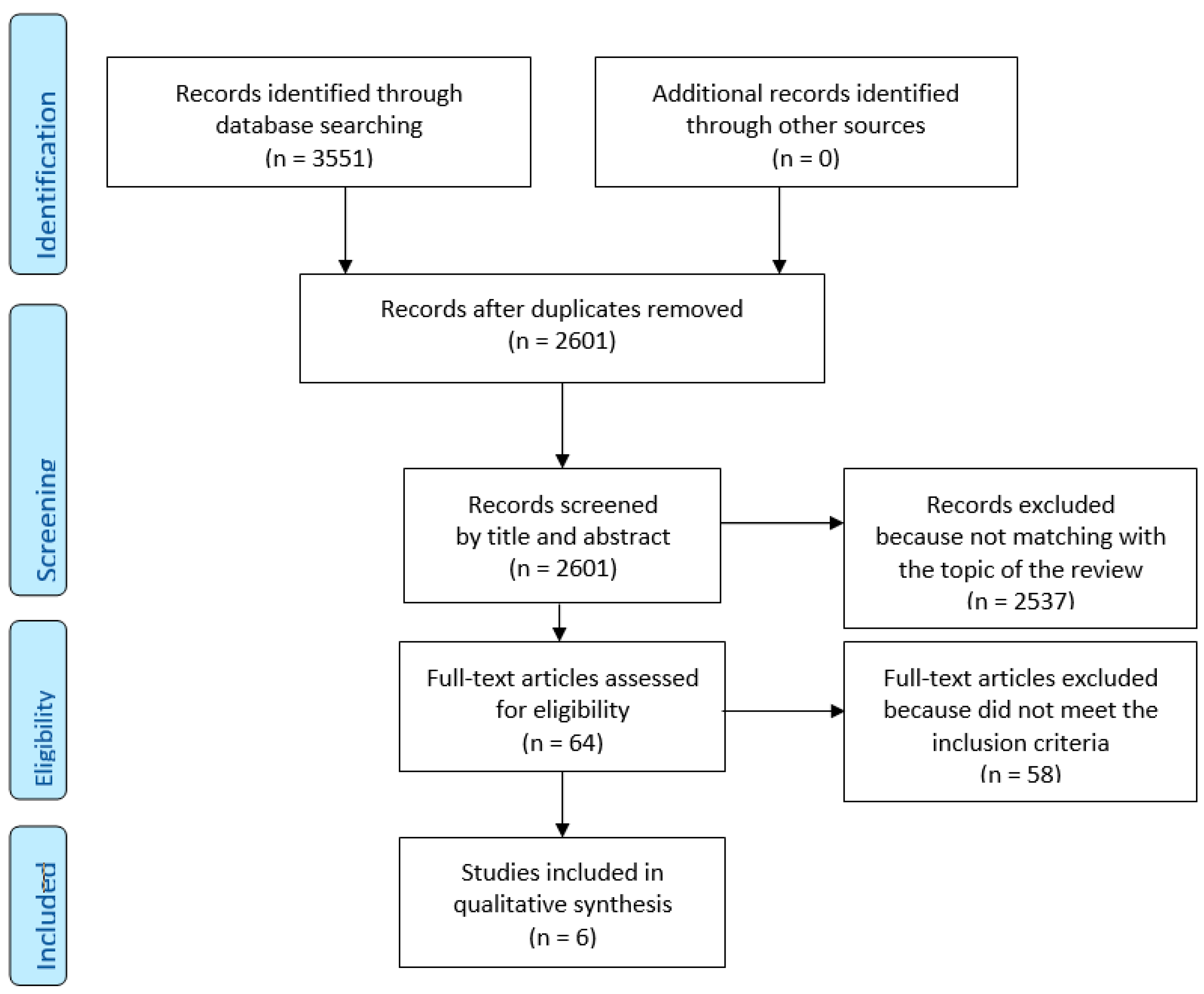
2.1. Search Strategy
2.2. Eligibility Criteria
- (1)
- Participants: patients with schizophrenia spectrum disorders.
- (2)
- Intervention: any kind of VR-based intervention performed through immersive virtual reality (VR), carried out with HMD (head-mounted display).
- (3)
- Comparison: therapy as usual (TAU), not VR based, or other types of VR interventions.
- (4)
- Outcomes: We considered the outcomes social skills and cognition, cognitive deficit, persecutory delusions and paranoia, and auditory verbal hallucinations (AVH).
- (5)
- Study design: clinical trials.
2.3. Data Extraction
2.4. Risk of Bias Assessment
3. Results
3.1. Characteristics of the Included Studies
3.1.1. Delusions and Paranoia
3.1.2. Auditory Verbal Hallucinations
3.1.3. Cognitive Deficits
3.1.4. Social Skills
4. Discussions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sung, R.C.; Ritchie, J.L.; Robinson, G.; Day, P.; Corney, J.; Lim, T. Automated design process modelling and analysis using immersive virtual reality. Comput. Des. 2009, 41, 1082–1094. [Google Scholar] [CrossRef]
- Radianti, J.; Majchrzak, T.A.; Fromm, J.; Wohlgenannt, I. A systematic review of immersive virtual reality applications for higher education: Design elements, lessons learned, and research agenda. Comput. Educ. 2020, 147, 103778. [Google Scholar] [CrossRef]
- Allcoat, D.; Von Mühlenen, A. Learning in virtual reality: Effects on performance, emotion and engagement. Res. Learn. Technol. 2018, 26, 26. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Yu, F.; Shi, D.; Shi, J.; Tian, Z.; Yang, J.; Wang, X.; Jiang, Q. Application of virtual reality technology in clinical medicine. Am. J. Transl. Res. 2017, 9, 3867–3880. [Google Scholar]
- Riva, G.; Mantovani, F.; Gaggioli, A. Presence and rehabilitation: Toward second-generation virtual reality applications in neuropsychology. J. Neuroeng. Rehabil. 2004, 1, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizzo, A.A.; Schultheis, M.; Kerns, K.A.; Mateer, C. Analysis of assets for virtual reality applications in neuropsychology. Neuropsychol. Rehabil. 2004, 14, 207–239. [Google Scholar] [CrossRef]
- Aida, J.; Chau, B.; Dunn, J. Immersive virtual reality in traumatic brain injury rehabilitation: A literature review. Neurorehabilitation 2018, 42, 441–448. [Google Scholar] [CrossRef]
- Dockx, K.; Bekkers, E.M.; Bergh, V.V.D.; Ginis, P.; Rochester, L.; Hausdorff, J.M.; Mirelman, A.; Nieuwboer, A. Virtual reality for rehabilitation in Parkinson’s disease. Cochrane Database Syst. Rev. 2016, 2016, 12. [Google Scholar] [CrossRef]
- Pourmand, A.; Davis, S.; Marchak, A.; Whiteside, T.; Sikka, N. Virtual reality as a clinical tool for pain management. Curr. Pain Headache Rep. 2018, 22, 53. [Google Scholar] [CrossRef]
- Gregg, L.; Tarrier, N. Virtual reality in mental health. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 343–354. [Google Scholar] [CrossRef]
- Krijn, M.; Emmelkamp, P.M.; Ólafsson, R.P.; Biemond, R. Virtual reality exposure therapy of anxiety disorders: A review. Clin. Psychol. Rev. 2004, 24, 259–281. [Google Scholar] [CrossRef] [PubMed]
- Pull, C.B. Current status of virtual reality exposure therapy in anxiety disorders: Editorial review. Curr. Opin. Psychiatry 2005, 18, 7–14. [Google Scholar] [PubMed]
- Emmelkamp, P.M.; Krijn, M.; Hulsbosch, A.; De Vries, S.; Schuemie, M.J.; Van Der Mast, C. Virtual reality treatment versus exposure in vivo: A comparative evaluation in acrophobia. Behav. Res. Ther. 2002, 40, 509–516. [Google Scholar] [CrossRef]
- Freeman, D. Studying and treating schizophrenia using virtual reality: A new paradigm. Schizophr. Bull. 2007, 34, 605–610. [Google Scholar] [CrossRef]
- Freeman, D.; Bradley, J.; Antley, A.; Bourke, E.; DeWeever, N.; Evans, N.; Černis, E.; Sheaves, B.; Waite, F.; Dunn, G.; et al. Virtual reality in the treatment of persecutory delusions: Randomised controlled experimental study testing how to reduce delusional conviction. Br. J. Psychiatry 2016, 209, 62–67. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Vives, M.V.; Slater, M. From presence to consciousness through virtual reality. Nat. Rev. Neurosci. 2005, 6, 332–339. [Google Scholar] [CrossRef]
- Slater, M.; Rovira, A.; Southern, R.; Swapp, D.; Zhang, J.J.; Campbell, C.; Levine, M. Bystander responses to a violent incident in an immersive virtual environment. PLoS ONE 2013, 8, e52766. [Google Scholar] [CrossRef] [Green Version]
- Nichols, S.; Haldane, C.; Wilson, J.R.; Sharples, S. Measurement of presence and its consequences in virtual environments. Int. J. Hum. Comput. Stud. 2000, 52, 471–491. [Google Scholar] [CrossRef]
- Meehan, M.; Insko, B.; Whitton, M.; Brooks, F.P., Jr. Physiological measures of presence in stressful virtual environments. ACM Trans. Graph. 2002, 21, 645–652. [Google Scholar] [CrossRef] [Green Version]
- Veling, W.; Moritz, S.; Van Der Gaag, M. Brave new worlds—Review and update on virtual reality assessment and treatment in psychosis. Schizophr. Bull. 2014, 40, 1194–1197. [Google Scholar] [CrossRef] [Green Version]
- Valmaggia, L.; Latif, L.; Kempton, M.J.; Rus-Calafell, M.; Kemptom, M.J.; Maria, R.-C. Virtual reality in the psychological treatment for mental health problems: An systematic review of recent evidence. Psychiatry Res. Neuroimaging 2016, 236, 189–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rus-Calafell, M.; Garety, P.; Sason, E.; Craig, T.J.K.; Valmaggia, L. Virtual reality in the assessment and treatment of psychosis: A systematic review of its utility, acceptability and effectiveness. Psychol. Med. 2017, 48, 362–391. [Google Scholar] [CrossRef] [PubMed]
- Park, M.J.; Kim, D.J.; Lee, U.; Na, E.J.; Jeon, H.J. A literature overview of virtual reality (vr) in treatment of psychiatric disorders: Recent advances and limitations. Front. Psychol. 2019, 10, 505. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, U.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Pot-Kolder, R.; Geraets, C.N.W.; Veling, W.; Van Beilen, M.; Staring, A.B.; Gijsman, H.J.; Delespaul, P.A.E.G.; Van Der Gaag, M. Virtual-reality-based cognitive behavioural therapy versus waiting list control for paranoid ideation and social avoidance in patients with psychotic disorders: A single-blind randomised controlled trial. Lancet Psychiatry 2018, 5, 217–226. [Google Scholar] [CrossRef]
- Freeman, D.; Garety, P.A.; Kuipers, E.; Fowler, D.; Bebbington, P. A cognitive model of persecutory delusions. Br. J. Clin. Psychol. 2002, 41, 331–347. [Google Scholar] [CrossRef]
- Du Sert, O.P.; Potvin, S.; Lipp, O.; Dellazizzo, L.; Laurelli, M.; Breton, R.; LaLonde, P.; Phraxayavong, K.; O’Connor, K.; Pelletier, J.-F.; et al. Virtual reality therapy for refractory auditory verbal hallucinations in schizophrenia: A pilot clinical trial. Schizophr. Res. 2018, 197, 176–181. [Google Scholar] [CrossRef]
- Leff, J.; Williams, G.; Huckvale, M.A.; Arbuthnot, M.; Leff, A.P. Computer-assisted therapy for medication-resistant auditory hallucinations: Proof-of-concept study. Br. J. Psychiatry 2013, 202, 428–433. [Google Scholar] [CrossRef] [Green Version]
- Diemer, J.; Alpers, G.W.; Peperkorn, H.M.; Shiban, Y.; Mühlberger, A. The impact of perception and presence on emotional reactions: A review of research in virtual reality. Front. Psychol. 2015, 6, 26. [Google Scholar] [CrossRef] [Green Version]
- Trémeau, F. A review of emotion deficits in schizophrenia. Dialog. Clin. Neurosci. 2006, 8, 59–70. [Google Scholar]
- Khoury, B.; LeComte, T. Emotion Regulation and Schizophrenia. Int. J. Cogn. Ther. 2012, 5, 67–76. [Google Scholar] [CrossRef]
- Craig, T.J.; Rus-Calafell, M.; Ward, T.; Leff, J.P.; Huckvale, M.; Howarth, E.; Emsley, R.; Garety, P.A. AVATAR therapy for auditory verbal hallucinations in people with psychosis: A single-blind, randomised controlled trial. Lancet Psychiatry 2018, 5, 31–40. [Google Scholar] [CrossRef] [Green Version]
- La Paglia, F.; La Cascia, C.; Rizzo, R.; Sideli, L.; Francomano, A.; La Barbera, D. Cognitive rehabilitation of schizophrenia through NeuroVr training. Stud. Health Technol. Inform. 2013, 191, 158–162. [Google Scholar]
- La Paglia, F.; La Cascia, C.; Rizzo, R.; Sanna, M.; Cangialosi, F.; Sideli, L.; Francomano, A.; Riva, G.; La Barbera, D. Virtual reality environments to rehabilitation attention deficits in schizophrenic patients. Annu. Rev. CyberTherapy Telemed. 2016, 14, 143–148. Available online: https://iris.unipa.it/retrieve/handle/10447/206419/356410/ARCTT%202016.pdf.pdf (accessed on 8 May 2019).
- Park, K.-M.; Ku, J.; Choi, S.-H.; Jang, H.-J.; Park, J.-Y.; Kim, S.I.; Kim, J.-J. A virtual reality application in role-plays of social skills training for schizophrenia: A randomized, controlled trial. Psychiatry Res. 2011, 189, 166–172. [Google Scholar] [CrossRef]
- Freeman, D.; Yu, L.-M.; Kabir, T.; Martin, J.; Craven, M.P.; Leal, J.; Lambe, S.; Brown, S.; Morrison, A.; Chapman, K.; et al. Automated virtual reality (VR) cognitive therapy for patients with psychosis: Study protocol for a single-blind parallel group randomised controlled trial (gameChange). BMJ Open 2019, 9, e031606. [Google Scholar] [CrossRef] [Green Version]
- Freeman, D.; Lister, R.; Waite, F.; Yu, L.-M.; Slater, M.; Dunn, G.; Clark, D.M. Automated psychological therapy using virtual reality (VR) for patients with persecutory delusions: Study protocol for a single-blind parallel-group randomised controlled trial (THRIVE). Trials 2019, 20, 87. [Google Scholar] [CrossRef] [Green Version]
- Nijman, S.A.; Veling, W.; Greaves-Lord, K.; Vermeer, R.R.; Vos, M.; Zandee, C.E.R.; Zandstra, D.C.; Geraets, C.N.W.; Pijnenborg, G.H.M. Dynamic Interactive Social Cognition Training in Virtual Reality (DiSCoVR) for social cognition and social functioning in people with a psychotic disorder: Study protocol for a multicenter randomized controlled trial. BMC Psychiatry 2019, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Moccia, A.; Ortano, R.; Fusco, C.; Di Nunzio, M. Cognitive training in virtual reality vs. cogpack in patients with schizophrenia: Study proposal. Minerva Psichiatr. 2020, 61, 5–9. [Google Scholar] [CrossRef]
- Alptekin, K.; Kartelli, F.; Berger, M.; Hoşgelen, E.I.; Erinç, S.; Yerlikaya, D.; Özbek, Y.; Ercegil, G.; Yener, G.; Kılınç, O.; et al. S111. A real environment based virtual reality application to improve physical health of patients with schizophrenia. Schizophr. Bull. 2020, 46, S76–S77. [Google Scholar] [CrossRef]
- Hoşgelen, E.I.; Kartelli, F.; Berger, M.; Erinç, S.; Yerlikaya, D.; Özbek, Y.; Yener, G.; Akdede, B.B.; Alptekin, K. T128. A real environment based virtual reality psychosocial treatment may help patients with schizophrenia to increase social functioning: A preliminary study. Schizophr. Bull. 2020, 46, S315–S316. [Google Scholar] [CrossRef]
- Caponnetto, P.; Milazzo, M. Cyber health psychology: The use of new technologies at the service of psychologycal well being and health empowerment. Health Psychol. Res. 2019, 7, 8559. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Authors | Year | Title | Target | Country | Study Design | Total Sample | Patient’s Diagnosis | DSM | Type of VR-Therapy | Number of Sessions | Duration of Each Session | Duration of Treatment | Principal Outcome Assessment | Principal Findings |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| du Sert, O. P.; Potvin, S.; Lipp, O.; Dellazizzo, L.; Laurelli, M.; Breton, R.; Lalonde, P.; Phraxayavong, K.; O’Connor, K.; Pelletier, J.-F.; Boukhalfi, T.; Renaud, P.; Dumais, A. | 2018 | Virtual reality therapy for refractory auditory verbal hallucinations in schizophrenia: A pilot clinical trial | Auditory verbal hallucinations | Canada | randomised controlled trial | 15 | schizophrenia or schizoaffective disorder | DSM-5 | AVATAR therapy | 1 avatar creation session + 6 sessions | 45 min | 7 weeks | PSYRATS BAVQ-R PANSS QLESQ-SF | VRT produced significant improvements in auditory verbal hallucinations severity, depressive symptoms and quality of life that remained table at the 3-month follow-up period. |
| Freeman, D.; Bradley, J.; Antley, A.; Bourke, E.; DeWeever, N.; Evans, N.; Černis, E.; Sheaves, B.; Waite, F.; Dunn, G.; Slater, M.; Clark, D. M. | 2016 | Virtual reality in the treatment of persecutory delusions: Randomised controlled experimental study testing how to reduce delusional conviction | Delusions and paranoia | UK | randomized controlled trial | 30 | psycosis with persecutory delusions | not specified | VR-CBT and VR-exposure | 1 | 30 min | 1 day | PANSS PSYRATS BDI BAI SBQ-PB | Cognitive therapy using virtual reality could prove highly effective in treating delusions. In comparison with exposure, virtual reality cognitive therapy led to large reductions in delusional conviction (reduction 22.0%, and real-world distress (reduction 19.6%,). |
| La Paglia F.; La Cascia C.; Rizzo R.; Sanna M.; Cangialosi F.; Sideli L.; Francomano A.; Riva G.; La Barbera D. | 2016 | Virtual reality environments to rehabilitation attention deficits in schizophrenic patients | Cognitive deficits | Italy | clinical trial | 15 | schizophrenia | DSM-5 | VR-training | 10 | 90 min | 10 weeks | MMSE FAB TMT-A, TMT-B, TMT B-A ToL Memory Battery WCST | Both VR training and IPT were associated with improved performance. VR training was additionally related with better cognitive functioning (MMSE), and with improved planning (TOL), and sustained attention (TMT-A). |
| La Paglia, F.; La Cascia, C.; Rizzo, R.; Sideli, L.; Francomano, A.; La Barbera, D. | 2013 | Cognitive Rehabilitation of Schizophrenia Through Neurovr Training. | Cognitive deficits | Italy | clinical trial | 12 | schizophrenia | DSM IV-TR | VR-training | 10 | 90 min | 10 weeks | MMSE ToL FAB TMT-B execution time, error number | VR may improve cognitive functioning in psycotic patients. |
| Park, K.-M.; Ku, J.; Choi, S.-H.; Jang, H.-J.; Park, J.-Y.; Kim, S. I.; Kim, J.-J. | 2011 | A virtual reality application in role-plays of social A randomized, controlled trial | Social skills | Korea | randomized controlled trial | 91 | schizophrenia | DSM-IV | SST-VR | 10 | 90 min | 5 weeks | SBS | SST-VR group improved more in conversational skills and assertiveness. |
| Pot-Kolder, Roos M. C. A.; Geraets, Chris N. W.; Veling, Wim; van Beilen, Marije; Staring, Anton B. P.; Gijsman, Harm J.; Delespaul, Philippe A. E. G.; van der Gaag, Mark; | 2018 | Virtual-reality-based cognitive behavioural therapy versus waiting list control for paranoid ideation and social avoidance in patients with psychotic disorders: A single-blind randomised controlled trial | Delusions and paranoia | Holland | randomised controlled trial | 116 | psychotic disorder and paranoid ideation | DSM-IV | VR-CBT | 16 | 60 min | 8-12 weeks | ESM (structured diary) via PsyMate electronic device | A large reduction was noted in momentary paranoia in the VR-CBT group, whereas a slight increase was noted in the control group; A significantly larger decrease in momentary anxiety was noted in the VR-CBT group than in the control These result remained significant at follow-up. Treatment effects on paranoid ideation were significant: at the post-treatment and follow-up assessments, levels of ideas of persecution and social reference were lower in the VR-CBT group than in the ontrol group. The VR-CBT group had improvements in self-stigmatisation and social functioning at follow-up whereas the control group did not. |
| Type of VR Intervention | Description |
|---|---|
| VR training | Training consisting of a series of 3D-VR scenarios reproducing daily life and related challenges, to training and improve cognitive skills of schizophrenic subjects. |
| VR SST | Virtual reality social skill training (VR SST), consist of a VR version of classic SST intervention, thought conversation training and role-plays focused on interpersonal communication. It aimed at enhancing verbal, non-verbal skills and social cognition, detecting and correcting the errors committed by the patient on multiple communication levels. |
| VR Avatar therapy | The therapy involves a three-way conversation between therapist, patient and a VR digital simulation (avatar) of one of his hallucinated voices, made by patients himself as a representation of the entity to which he attributes his auditory hallucinations. The therapist’s voice is transformed through speech transformation software to coincide with the vocal characteristics attributed by the patient to the entity. |
| VR CBT (cognitive behavior therapy) | Use of techniques of cognitive behavioral psychotherapy (CBT) for the treatment of delusional disorders and paranoia, taking advantage of the immersive environment offered by VR, that allows a controlled exposure to social situation. |
| VR exposure | Therapy based on controlled exposure in a virtual reality environment to a situation or a stimulus that usually causes anxiety and fear in the subject, in order to induce a progressive desensitization towards it. |
| Randomization process | Deviations from intended interventions | Missing outcome data | Measurement of the outcome | Selection of the reported result | Overall | ||||
| Du Sert et al. (2018) |  |  |  |  |  |  | |||
| Freeman et al. (2016) |  |  |  |  |  |  | |||
| La Paglia et al. (2013) |  |  |  |  |  |  | Legend: | ||
| La Paglia et al. (2016) |  |  |  |  |  |  |  | Low risk | |
| Park et al. (2011) |  |  |  |  |  |  |  | Some concerns | |
| Pot-Kolder et al. (2018) |  |  |  |  |  |  |  | High risk |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bisso, E.; Signorelli, M.S.; Milazzo, M.; Maglia, M.; Polosa, R.; Aguglia, E.; Caponnetto, P. Immersive Virtual Reality Applications in Schizophrenia Spectrum Therapy: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 6111. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176111
Bisso E, Signorelli MS, Milazzo M, Maglia M, Polosa R, Aguglia E, Caponnetto P. Immersive Virtual Reality Applications in Schizophrenia Spectrum Therapy: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(17):6111. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176111
Chicago/Turabian StyleBisso, Emanuele, Maria Salvina Signorelli, Michele Milazzo, Marilena Maglia, Riccardo Polosa, Eugenio Aguglia, and Pasquale Caponnetto. 2020. "Immersive Virtual Reality Applications in Schizophrenia Spectrum Therapy: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 17: 6111. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176111